
Comparative Study of Anticipatory Postural Adjustments between Normal and Cervical Myelopathy Patients

 , , and
, , and
Abstract
1. Introduction
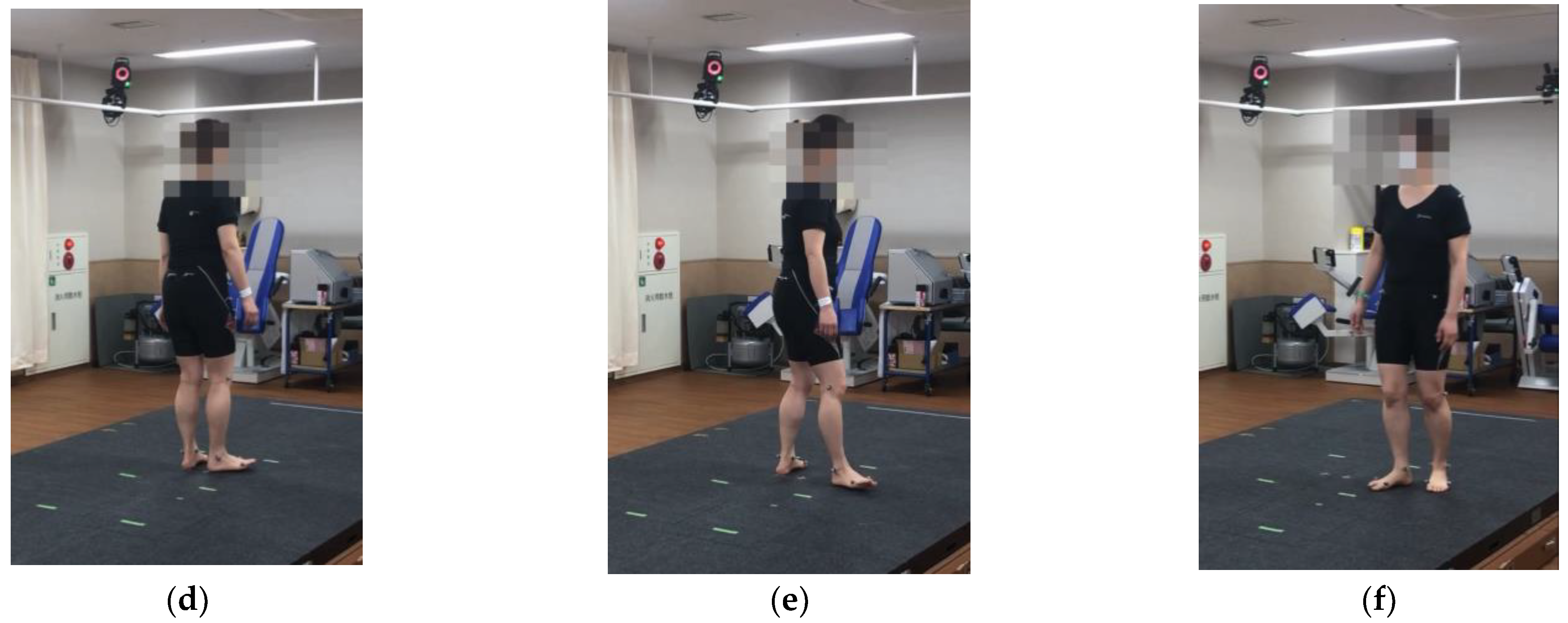
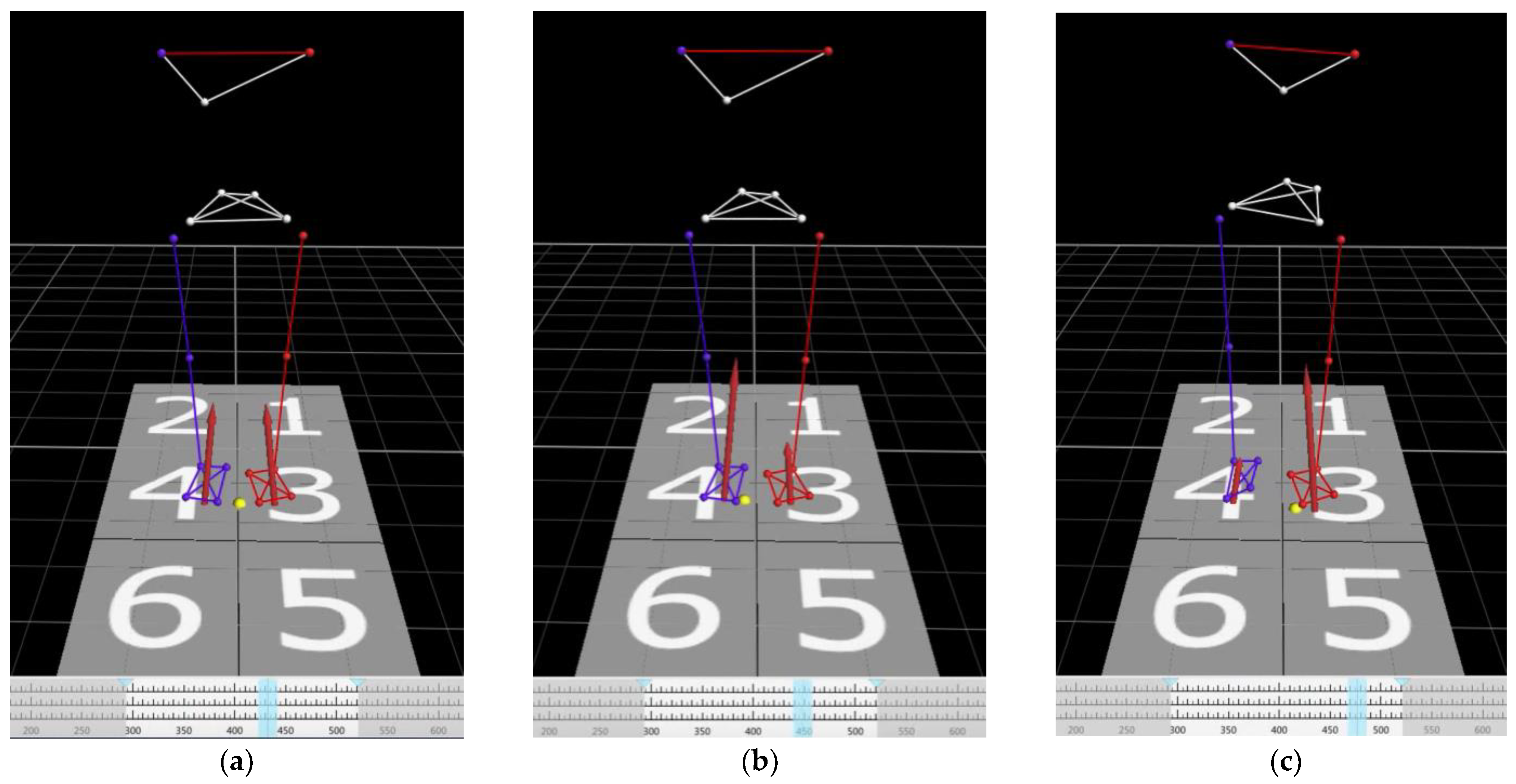
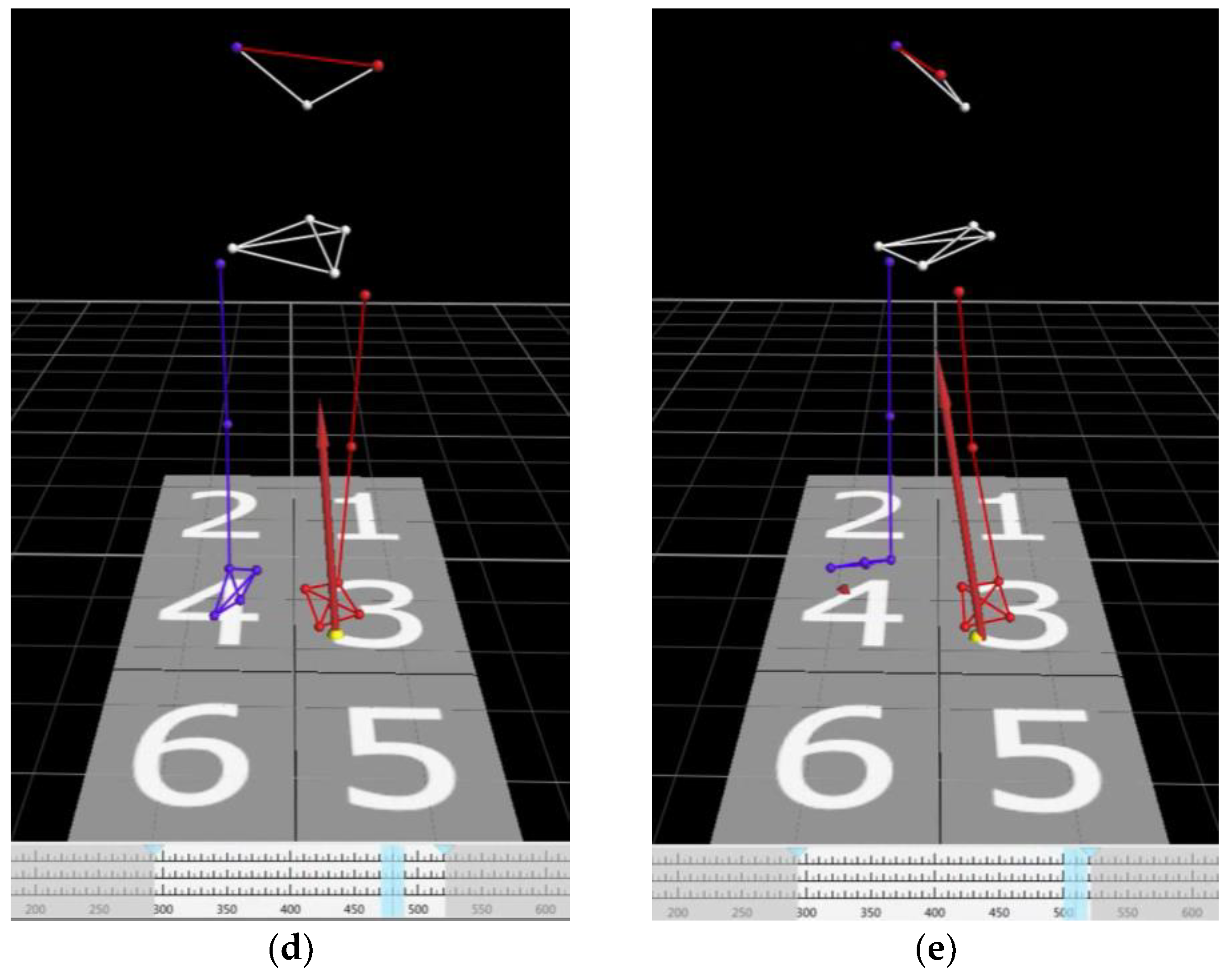
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kimura, A.; Seichi, A.; Takeshita, K.; Inoue, H.; Kato, T.; Yoshii, T.; Furuya, T.; Koda, M.; Takeuchi, K.; Matsunaga, S.; et al. Fall-related deterioration of subjective symptoms in patients with cervical myelopathy. Spine 2017, 42, E398–E403. [Google Scholar] [CrossRef] [PubMed]
- National Spinal Cord Injury Statistical Center. Available online: https://www.nscisc.uab.edu/Public_Pages/Database (accessed on 22 February 2023).
- Spivak, J.; Weis, M.; Cotler, J.; Call, M. Cervical spine injuries in patients 65 and older. Spine 1994, 19, 2302–2306. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.J.; Kanekar, N.; Aruin, A.S. The role of anticipatory postural adjustments in compensatory control of posture: 1. Electromyographic analysis. J. Electromyogr. Kinesiol. 2010, 20, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.J.; Kanekar, N.; Aruin, A.S. The role of anticipatory postural adjustments in compensatory control of posture: 2. Biomechanical analysis. J. Electromyogr. Kinesiol. 2010, 20, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Aruin, A.S. Enhancing anticipatory postural adjustments: A novel approach to balance rehabilitation. J. Nov. Physiother. 2016, 6, e144. [Google Scholar] [CrossRef] [PubMed]
- Kanekar, N.; Aruin, A.S. The effect of aging on anticipatory postural control. Exp. Brain Res. 2014, 232, 1127–1136. [Google Scholar] [CrossRef] [PubMed]
- Kimijanová, J.; Bzdúšková, D.; Hirjaková, Z.; Hlavačka, F. Age-related changes of the anticipatory postural adjustments during gait initiation preceded by vibration of lower leg muscles. Front. Hum. Neurosci. 2021, 15, 771446. [Google Scholar] [CrossRef]
- Rogers, M.W.; Hilliard, M.J.; Martinez, K.M.; Zhang, Y.; Simuni, T.; Mille, M.L. Perturbations of ground support alter posture and locomotion coupling during step initiation in Parkinson’s disease. Exp. Brain Res. 2011, 208, 557–567. [Google Scholar] [CrossRef]
- Sousa, A.; Silva, A.; Santos, R. Ankle anticipatory postural adjustments during gait initiation in healthy and post-stroke subjects. Clin. Biomech. 2015, 30, 960–965. [Google Scholar] [CrossRef]
- Chang, W.-H.; Tang, P.-F.; Wang, Y.-H.; Lin, K.-H.; Chiu, M.-J.; Chen, S.-H.A. Role of the premotor cortex in leg selection and anticipatory postural adjustments associated with a rapid stepping task in patients with stroke. Gait Posture 2010, 32, 487–493. [Google Scholar] [CrossRef]
- Garcez, D.R.; da Silva Almeida, G.C.; Silva, C.F.O.; de Souza Nascimento, T.; de Athayde Costa E Silva, A.; Kleiner, A.F.R.; da Silva Souza, G.; Yamada, E.S.; Callegari, B. Postural adjustments impairments in elderly people with chronic low back pain. Sci. Rep. 2021, 11, 4783. [Google Scholar] [CrossRef]
- Tateuchi, H.; Ichihara, N.; Shinya, M.; Oda, S. Anticipatory postural adjustments during lateral step motion in patients with hip osteoarthritis. J. Appl. Biomech. 2011, 27, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Viton, J.M.; Atlani, L.; Mesure, S.; Massion, J.; Franceschi, J.P.; Delarque, A.; Bardot, A. Reorganization of equilibrium and movement control strategies after total knee arthroplasty. J. Rehabil. Med. 2002, 34, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Lyon, I.N.; Day, B.L. Control of frontal plane body motion in human stepping. Exp. Brain Res. 1997, 115, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.gov-online.go.jp/eng/publicity/book/hlj/html/202102/202102_09_en.html (accessed on 10 January 2023).
- Nakashima, H.; Tetreault, L.A.; Nagoshi, N.; Nouri, A.; Kopjar, B.; Arnold, P.M.; Bartels, R.; Defino, H.; Kale, S.; Zhou, Q.; et al. Does age affect surgical outcomes in patients with degenerative cervical myelopathy? Results from the prospective multicenter AOSpine International study on 479 patients. J. Neurol. Neurosurg. Psychiatry 2016, 87, 734–740. [Google Scholar] [CrossRef]
- Isogai, N.; Nagoshi, N.; Iwanami, A.; Kono, H.; Kobayashi, Y.; Tsuji, T.; Fujita, N.; Yagi, M.; Watanabe, K.; Kitamura, K.; et al. Surgical Treatment of Cervical Spondylotic Myelopathy in the Elderly: Outcomes in Patients Aged 80 Years or Older. Spine 2018, 43, E1430–E1436. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, M.; Chiba, K.; Toyama, Y. Surgical treatment of ossification of the posterior longitudinal ligament and its outcomes: Posterior surgery by laminoplasty. Spine 2012, 37, E303–E308. [Google Scholar] [CrossRef]
- Matsunaga, S.; Sakou, T. OPLL: Disease entity, incidence, literature search and prognosis. In OPLL: Ossification of the Posterior Longitudinal Ligament, 2nd ed.; Yoneobu, K., Nakamura, K., Toyama, Y., Eds.; Springer: Tokyo, Japan, 2006; pp. 11–17. [Google Scholar]
- Fujimori, T.; Watabe, T.; Iwamoto, Y.; Hamada, S.; Iwasaki, M.; Oda, T. Prevalence, concomitance, and distribution of ossification of the spinal ligaments: Results of whole spine CT scans in 1500 Japanese Patients. Spine 2016, 41, 1668–1676. [Google Scholar] [CrossRef]
- Kawaguchi, Y.; Nakano, M.; Yasuda, T.; Seki, S.; Hori, T.; Kimura, T. Ossification of the posterior longitudinal ligament in not only the cervical spine, but also other spinal regions. Spine 2013, 38, E1477–E1482. [Google Scholar] [CrossRef]
- Onishi, E.; Sakamoto, A.; Murata, S.; Matsushita, M. Risk factors for acute cervical spinal cord injury associated with ossification of the posterior longitudinal ligament. Spine 2012, 37, 660–666. [Google Scholar] [CrossRef]
- Gélat, T.; Coudrat, L.; Ferrel-Chapus, C.; Vernazza-Martin, S. The duration of emotional image exposure does not impact anticipatory postural adjustments during gait initiation. Brain Sci. 2018, 8, 195. [Google Scholar] [CrossRef] [PubMed]
- Michel, V.; Do, M.C. Are stance ankle plantar flexor muscles necessary to generate propulsive force during human gait initiation? Neurosci. Lett. 2002, 325, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Hirabayashi, K.; Miyakawa, J.; Satomi, K.; Maruyama, K.; Wakano, K. Operative results and postoperative progression of ossification among patients with ossification of cervical posterior longitudinal ligament. Spine 1981, 6, 354–364. [Google Scholar] [CrossRef] [PubMed]
- Nurick, S. The pathogenesis of the spinal cord disorder associated with cervical spondylosis. Brain 1972, 95, 87–100. [Google Scholar] [CrossRef]
- Kadoya, S. Grading and scoring system for neurological function in degenerative cervical spine disease―Neurosurgical Cervical Spine Scale. Neurol. Med. Chir. 1992, 32, 40–41. [Google Scholar] [CrossRef]
- Herdman, J.; Linzbach, M.; Krzan, M.; Dvorák, J.; Bock, W.J. The European Myelopathy Score. In Advances in Neurosurgery 22; Bauer, B., Brock, M., Klinger, M., Eds.; Springer: Berlin/Heidelberg, Germany, 1994; pp. 266–268. [Google Scholar]
- Casey, A.T.; Bland, J.M.; Crockard, H.A. Development of a functional scoring system for rheumatoid arthritis patients with cervical myelopathy. Ann. Rheum. Dis. 1996, 55, 901–906. [Google Scholar] [CrossRef]
- Dalitz, K.; Vitzthum, H.E. Evaluation of five scoring systems for cervical spondylogenic myelopathy. Spine J. 2009, 19, e41–e46. [Google Scholar] [CrossRef]
- Kimura, A.; Takeshita, K.; Inoue, H.; Inose, H.; Yoshii, T.; Maekawa, A.; Endo, K.; Miyamoto, T.; Furuya, T.; Nakamura, A.; et al. The 5-question Geriatric Locomotive Function Scale predicts postoperative fall risk in patients undergoing surgery for degenerative cervical myelopathy. J. Orthop. Sci. 2021, 26, 779–785. [Google Scholar] [CrossRef]
- Aruin, A.S.; Kanekar, N.; Jadghane, S. Training-related enhancement of anticipatory postural adjustments in older adults. In Proceedings of the 7th International Posture Symposium, Smolenice Castle, Bratislava, Slovakia, 6–9 September 2015; Hlavacka, F., Lobotkova, J., Eds.; Institute of Normal and Pathological Physiology, SAS: Stockholm, Sweden, 2015. [Google Scholar]
- Jagdhane, S.; Kanekar, N.; Aruin, A.S. The effect of a four-week balance training program on anticipatory postural adjustments in older adults: A pilot feasibility study. Curr. Aging Sci. 2016, 9, 295–300. [Google Scholar] [CrossRef]
- Li, Z.; Yu, Q.; Luo, H.; Liang, W.; Li, X.; Ge, L.; Zhang, S.; Li, L.; Wang, C. The Effect of Virtual Reality Training on Anticipatory Postural Adjustments in Patients with Chronic Nonspecific Low Back Pain: A Preliminary Study. Neural Plast. 2021, 27, 9975862. [Google Scholar] [CrossRef]
- Duarte, M.B.; da Costa Moraes, A.A.; Ferreira, E.V.; da Silva Almeida, G.C.; da Rocha Santos, E.G.; Pinto, G.H.L.; de Oliveira, P.R.; Amorim, C.F.; Dos Santos Cabral, A.; Saunier, G.; et al. Validity and reliability of a smartphone-based assessment for anticipatory and compensatory postural adjustments during predictable perturbations. Gait Posture 2022, 96, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Onuma, R.; Hoshi, F.; Yamasaki, H.R.; Sakai, T.; Jinno, T. New quantitative evaluation of anticipatory postural adjustments using a smartphone in patients with Parkinson’s disease. Physiother. Theory Pract. 2022, 1–6. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Score | ||
|---|---|---|---|
| Motor dysfunction | |||
| Upper extremity | |||
| unable to eat with chopstick, spoon, or fork, and/or unable to fasten button of any size | 0 | ||
| able to eat with spoon, or fork but not with chopsticks | 1 | ||
| either eating with chopsticks or writing is possible but inadequate, and/or large button can be fastened | 2 | ||
| either eating with chopsticks or writing is clumsy but practical, and/or cuff button can be fastened | 3 | ||
| normal | 4 | ||
| Lower extremity | |||
| unable to stand and walk by any means | 0 | ||
| unable to walk without a cane or other support on a level | 1 | ||
| able to walk independently on a level, but needs support on stairs | 2 | ||
| capable of fast but clumsy walking | 3 | ||
| normal | 4 | ||
| Sensory dysfunction | |||
| Upper extremity | |||
| apparent sensory disturbance | 0 | ||
| minimal sensory disturbance | 1 | ||
| normal | 2 | ||
| Lower extremity | |||
| apparent sensory disturbance | 0 | ||
| minimal sensory disturbance | 1 | ||
| normal | 2 | ||
| Trunk | |||
| apparent sensory disturbance | 0 | ||
| minimal sensory disturbance | 1 | ||
| normal | 2 | ||
| Bladder dysfunction | |||
| complete retention | 0 | ||
| severe impairment (sense of retention, or dribbling) | 1 | ||
| mild impairment (pollakiuria, or urinary hesitancy) | 2 | ||
| normal | 3 | ||
| Cervical Myelopathy | Normal | p-Value | |||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| APA phase (sec) | 0.47 | 0.11 | 0.39 | 0.08 | <0.05 |
| Step time (sec) | 0.32 | 0.08 | 0.35 | 0.08 | 0.30 |
| Turning time (sec) | 2.27 | 0.51 | 1.83 | 0.29 | <0.01 |
| Step length (mm) | 305.18 | 72.00 | 361.04 | 81.90 | 0.06 |
| % Step length (%) | 18.94 | 4.03 | 22.37 | 5.52 | 0.06 |
| APA Phase | Step Time | Turning Time | Step Length | % Step Length | |
|---|---|---|---|---|---|
| JOA U/E motor dysfunction | −0.03 (p = 0.92) | −0.18 (p = 0.52) | −0.32 (p = 0.24) | 0.13 (p = 0.65) | 0.12 (p = 0.67) |
| JOA L/E motor dysfunction | 0.17 (p = 0.55) | 0.21 (p = 0.45) | −0.35 (p = 0.20) | * 0.68 (p < 0.01) | * 0.68 (p < 0.01) |
| JOA U/E sensory dysfunction | 0.02 (p = 0.94) | 0.17 (p = 0.55) | −0.32 (p = 0.35) | 0.38 (p = 0.16) | 0.37 (p = 0.16) |
| JOA trunk sensory dysfunction | 0.19 (p = 0.50) | −0.12 (p = 0.66) | 0.18 (p = 0.51) | 0.00 (p = 0.99) | −0.1 (p = 0.74) |
| JOA L/E sensory dysfunction | 0.15 (p = 0.59) | 0.15 (p = 0.60) | −0.10 (p = 0.73) | 0.38 (p = 0.17) | 0.33 (p = 0.24) |
| JOA bladder dysfunction | 0.07 (p = 0.80) | 0.33 (p = 0.23) | 0.00 (p = 0.98) | 0.11 (p = 0.70) | 0.12 (p = 0.66) |
| JOA total | 0.11 (p = 0.69) | 0.12 (p = 0.66) | −0.27 (p = 0.34) | 0.45 (p = 0.09) | 0.40 (p = 0.14) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Funao, H.; Igawa, T.; Matsuzawa, M.; Isogai, N.; Ishii, K. Comparative Study of Anticipatory Postural Adjustments between Normal and Cervical Myelopathy Patients. J. Clin. Med. 2023, 12, 3584. https://doi.org/10.3390/jcm12103584
Funao H, Igawa T, Matsuzawa M, Isogai N, Ishii K. Comparative Study of Anticipatory Postural Adjustments between Normal and Cervical Myelopathy Patients. Journal of Clinical Medicine. 2023; 12(10):3584. https://doi.org/10.3390/jcm12103584
Chicago/Turabian StyleFunao, Haruki, Tatsuya Igawa, Masaru Matsuzawa, Norihiro Isogai, and Ken Ishii. 2023. "Comparative Study of Anticipatory Postural Adjustments between Normal and Cervical Myelopathy Patients" Journal of Clinical Medicine 12, no. 10: 3584. https://doi.org/10.3390/jcm12103584
APA StyleFunao, H., Igawa, T., Matsuzawa, M., Isogai, N., & Ishii, K. (2023). Comparative Study of Anticipatory Postural Adjustments between Normal and Cervical Myelopathy Patients. Journal of Clinical Medicine, 12(10), 3584. https://doi.org/10.3390/jcm12103584