
Comparative Effect of Two Types of Physical Exercise for the Improvement of Exercise Capacity, Diastolic Function, Endothelial Function and Arterial Stiffness in Participants with Heart Failure with Preserved Ejection Fraction (ExIC-FEp Study): Protocol for a Randomized Controlled Trial

 ,
, 
 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Setting
2.3. Participants
2.4. Randomization
2.5. Intervention
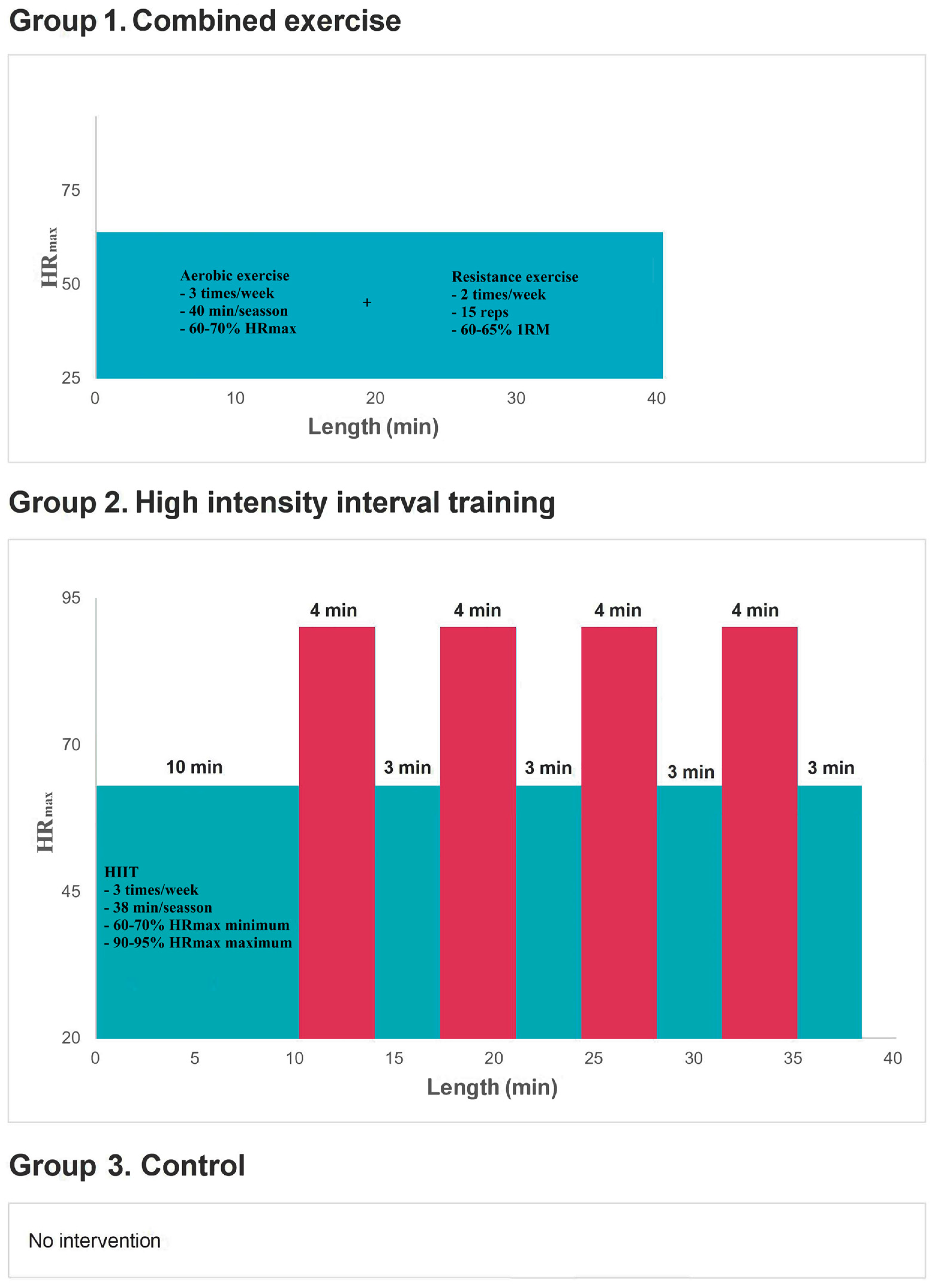
2.5.1. Training Interventions
2.5.2. Control Group (Group 3)
2.5.3. Duration of the Intervention
2.6. Criteria for Nonadherence and Prolongation of Training
2.7. Outcomes
2.7.1. Primary Outcomes
- −
- Gas analyzer (K5 COSMED): VO2max, ventilation slope/carbon dioxide production (VE/VCO2) per minute, and ventilatory threshold (VT).
- −
- Workload measured in watts.
- −
- Average exercise time in minutes.
- −
- HRmax by Polar H10 heart rate monitor.
- −
- A 6-min walking test, in a 30-m corridor, to be performed by walking from one side to the other along this stretch of corridor, which will be delimited by cone-type indicators. These signs will be placed 29 m from each other, leaving 0.5 m at each end for the subject to turn. The test will be performed accompanied by the examiner. The primary test outcome is the final distance walked.
- −
- Using Sonosite SII Doppler ultrasound (Sonosite Inc., Bothell, WA, USA), the following will be measured: E velocity (m/s), A velocity (m/s), E/A ratio, e’ velocity (m/s), E/e’ ratio, ejection fraction percentage, left ventricular volume index, end-diastolic volume, left ventricular mass, left atrial diameter, isovolume relaxation time, deceleration time (m/s) and left atrial volume index.
- −
- Carotid intima-media thickness (cIMT): by ultrasound with the Sonosite SII device (Sonosite Inc., Bothell, WA, USA).
- −
- Pulse wave velocity (PWv) and central augmentation index (cAIx) using the Mobil-O-Graph PWA (I.E.M. GmbH, Stolberg, Germany).
- −
- Validated 12-item health questionnaire (SF-12).
- −
- Validated Minnesota Living with Heart Failure Questionnaire (MLWHFQ).
2.7.2. Covariables
- −
- Age.
- −
- Sex.
- −
- Socioeconomic level: using the Spanish Society of Epidemiology scale. Participants will report their educational level and employment status, and an index will be calculated considering both.
- −
- Comorbidities (hypertension, diabetes, smoking, alcohol consumption).
- −
- Pharmacological treatment.
- −
- Weight: mean of two weight measurements (Seca® 861 scale), with the participant barefoot and lightly wrapped.
- −
- Height: mean of two measurements with a wall-mounted measuring rod (Seca® 222), with the participant barefoot, in an upright position and with his/her sagittal midline coinciding with the measuring rod.
- −
- Body mass index: body mass index will be calculated by the formula weight (kg)/height2 (m2).
- −
- Waist circumference: mean of two measurements of waist circumference with a flexible tape measure at the midpoint between the last rib and the iliac crest at the end of a normal exhalation.
- −
- Body fat percentage: mean of two measurements from an 8-electrode electrical bioimpedance model Tanita® BC-418 MA (Tanita Corp., Tokyo, Japan).
- −
- Densitometry (DXA) (model GE-Lunar DXA): densitometry will be performed to estimate fat mass, lean mass and bone mineral density.
- −
- Blood pressure: mean of two blood pressure determinations separated by a 5-min interval. The first measurement is obtained after a rest of at least 5 min. The subject is seated in a quiet environment, with the right arm semi-flexed at heart level. Blood pressure will be measured with the Omron® M5-I monitor (Omron Healthcare UK Ltd., Milton Keynes, UK) and cuffs of three sizes according to arm circumference.
- −
- The manual grip strength will be determined with the TKK 5401 Grip-D dynamometer (Takey®, Tokyo, Japan).
- −
- Forced vital capacity (FVC).
- −
- Forced expiratory volume in the first second (FEV1).
- −
- FEV1/FVC ratio.
- −
- Glucose, total cholesterol, triglycerides, HDL cholesterol, LDL cholesterol, apolipoproteins A1 and B, insulin and ultrasensitive C-reactive protein. The determinations will be made on a Roche Diagnostics® Cobas 8000 system, and the insulin determination will be made on the Abbott® Architect platform.
- −
- N-terminal pro-B-type natriuretic peptide (NT-proBNP). Plasma concentrations of NTproBMP will be determined by enzyme-linked immunosorbent assay (ELISA) (R & D Systems, Minneapolis, MN, USA).
- −
- HbA1c will be determined by high-performance liquid chromatography on an ADAMS A1c HA-8180 V analyzer from A. Menarini Diagnostics®, a method certified by the National Glycohemoglobin Standard Glycohemoglobin Standardization Program (NGSP) and the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC).
- −
- Accelerometry: Physical activity will be objectively measured using AX6 accelerometers (Axivity) for nine consecutive days (including nights).
- −
- Podometry measured by using the Xiaomi MI Band 3 smart bracelet. This device will also be used to provide information during the study on sleep time and sedentary time.
- −
- Validated 14-item Mediterranean diet adherence questionnaire (MEDAS-14).
2.8. Ethical Considerations
2.9. Sample Size Calculation
2.10. Statistical Analysis
2.11. Participation of Subjects with HFpEF in Research
3. Results
4. Discussion
4.1. HFpEF and Exercise Capacity
4.2. HFpEF and Diastolic Function
4.3. HFpEF and Endothelial Function
4.4. HFpEF and Arterial Stiffness
4.5. HFpEF and QoL
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heidenreich, P.A.; Albert, N.M.; Allen, L.A.; Bluemke, D.A.; Butler, J.; Fonarow, G.G.; Ikonomidis, J.S.; Khavjou, O.; Konstam, M.A.; Maddox, T.M.; et al. Forecasting the impact of heart failure in the United States: A policy statement from the American Heart Association. Circ. Heart Fail. 2013, 6, 606–619. [Google Scholar] [CrossRef]
- Senni, M.; Paulus, W.J.; Gavazzi, A.; Fraser, A.G.; Diez, J.; Solomon, S.D.; Smiseth, O.A.; Guazzi, M.; Lam, C.S.; Maggioni, A.P.; et al. New strategies for heart failure with preserved ejection fraction: The importance of targeted therapies for heart failure phenotypes. Eur. Heart J. 2014, 35, 2797–2815. [Google Scholar] [CrossRef]
- Kapłon-Cieślicka, A.; Kupczyńska, K.; Dobrowolski, P.; Michalski, B.; Jaguszewski, M.J.; Banasiak, W.; Burchardt, P.; Chrzanowski, Ł.; Darocha, S.; Domienik-Karłowicz, J.; et al. On the search for the right definition of heart failure with preserved ejection fraction. Cardiol. J. 2020, 27, 449–468. [Google Scholar] [CrossRef]
- Sato, T.; Yoshihisa, A.; Kanno, Y.; Suzuki, S.; Yamaki, T.; Sugimoto, K.; Kunii, H.; Nakazato, K.; Suzuki, H.; Saitoh, S.I.; et al. Cardiopulmonary exercise testing as prognostic indicators: Comparisons among heart failure patients with reduced, mid-range and preserved ejection fraction. Eur. J. Prev. Cardiol. 2017, 24, 1979–1987. [Google Scholar] [CrossRef]
- Glezeva, N.; and Baugh, J.A. Role of inflammation in the pathogenesis of heart failure with preserved ejection fraction and its potential as a therapeutic target. Heart Fail. Rev. 2014, 19, 681–694. [Google Scholar] [CrossRef]
- Ather, S.; Chan, W.; Bozkurt, B.; Aguilar, D.; Ramasubbu, K.; Zachariah, A.A.; Wehrens, X.H.; Deswal, A. Impact of noncardiac comorbidities on morbidity and mortality in a predominantly male population with heart failure and preserved versus reduced ejection fraction. J. Am. Coll. Cardiol. 2012, 59, 998–1005. [Google Scholar] [CrossRef]
- Pandey, A.; Darden, D.; Berry, J.D. Low fitness in midlife: A novel therapeutic target for heart failure with preserved ejection fraction prevention. Prog. Cardiovasc. Dis. 2015, 58, 87–93. [Google Scholar] [CrossRef]
- Pandey, A.; Berry, J.D.; Lavie, C.J. Cardiometabolic disease leading to heart failure: Better fat and fit than lean and lazy. Curr. Heart Fail. Rep. 2015, 12, 302–308. [Google Scholar] [CrossRef]
- Leggio, M.; Fusco, A.; Armeni, M.; D’Emidio, S.; Severi, P.; Calvaruso, S.; Limongelli, G.; Sgorbini, L.; Bendini, M.G.; Mazza, A. Pulmonary hypertension and exercise training: A synopsis on the more recent evidences. Ann. Med. 2018, 50, 226–233. [Google Scholar] [CrossRef]
- Leggio, M.; Fusco, A.; Limongelli, G.; Sgorbini, L. Exercise training in patients with pulmonary and systemic hypertension: A unique therapy for two different diseases. Eur. J. Intern. Med. 2018, 47, 17–24. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, 1757–1780. [Google Scholar] [CrossRef]
- McMurray, J.J.; Adamopoulos, S.; Anker, S.D.; Auricchio, A.; Böhm, M.; Dickstein, K.; Falk, V.; Filippatos, G.; Fonseca, C.; Gomez-Sanchez, M.A. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Eur. Heart J. 2012, 33, 1787–1847. [Google Scholar]
- Chan, E.; Giallauria, F.; Vigorito, C.; Smart, N.A. Exercise training in heart failure patients with preserved ejection fraction: A systematic review and meta-analysis. Monaldi Arch. Chest Dis. 2016, 86, 759. [Google Scholar] [CrossRef]
- Dieberg, G.; Ismail, H.; Giallauria, F.; Smart, N.A. Clinical outcomes and cardiovascular responses to exercise training in heart failure patients with preserved ejection fraction: A systematic review and meta-analysis. J. Appl. Physiol. 2015, 119, 726–733. [Google Scholar] [CrossRef]
- Fukuta, H. Effects of Exercise Training on Cardiac Function in Heart Failure with Preserved Ejection Fraction. Card. Fail. Rev. 2020, 6, e27. [Google Scholar] [CrossRef]
- Fukuta, H.; Goto, T.; Wakami, K.; Kamiya, T.; Ohte, N. Effects of exercise training on cardiac function, exercise capacity, and quality of life in heart failure with preserved ejection fraction: A meta-analysis of randomized controlled trials. Heart Fail. Rev. 2019, 24, 535–547. [Google Scholar] [CrossRef]
- Leggio, M.; Fusco, A.; Loreti, C.; Limongelli, G.; Bendini, M.G.; Mazza, A.; Coraci, D.; Padua, L. Effects of exercise training in heart failure with preserved ejection fraction: An updated systematic literature review. Heart Fail. Rev. 2020, 25, 703–711. [Google Scholar] [CrossRef]
- Pandey, A.; Garg, S.; Matulevicius, S.A.; Shah, A.M.; Garg, J.; Drazner, M.H.; Berry, J.D. Exercise training in patients with heart failure and preserved ejection fraction: Meta-analysis of randomized control trials. Circ. Heart Fail. 2015, 8, 33–40. [Google Scholar] [CrossRef]
- Schmidt, C.; Moreira-Gonçalves, D.; Santos, M.; Leite-Moreira, A.; Oliveira, J. Physical activity and exercise training in heart failure with preserved ejection fraction: Gathering evidence from clinical and pre-clinical studies. Heart Fail. Rev. 2020, 27, 573–586. [Google Scholar] [CrossRef]
- Taylor, R.S.; Davies, E.J.; Dalal, H.M.; Davis, R.; Doherty, P.; Cooper, C.; Holland, D.J.; Jolly, K.; Smart, N.A. Effects of exercise training for heart failure with preserved ejection fraction: A systematic review and meta-analysis of comparative studies. Int. J. Cardiol. 2012, 162, 6–13. [Google Scholar] [CrossRef]
- Tucker, W.J.; Nelson, M.D.; Beaudry, R.I.; Halle, M.; Sarma, S.; Kitzman, D.W.; La Gerche, A.; Haykowsky, M.J. Impact of exercise training on peak oxygen uptake and its determinants in heart failure with preserved ejection fraction. Cardiac. Fail. Rev. 2016, 2, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Angadi, S.S.; Mookadam, F.; Lee, C.D.; Tucker, W.J.; Haykowsky, M.J.; Gaesser, G.A. High-intensity interval training vs. moderate-intensity continuous exercise training in heart failure with preserved ejection fraction: A pilot study. J. Appl. Physiol. 2015, 119, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Donelli da Silveira, A.; Beust de Lima, J.; da Silva Piardi, D.; Dos Santos Macedo, D.; Zanini, M.; Nery, R.; Laukkanen, J.A.; Stein, R. High-intensity interval training is effective and superior to moderate continuous training in patients with heart failure with preserved ejection fraction: A randomized clinical trial. Eur. J. Prev. Cardiol. 2020, 27, 1733–1743. [Google Scholar] [CrossRef] [PubMed]
- Edelmann, F.; Gelbrich, G.; Düngen, H.D.; Fröhling, S.; Wachter, R.; Stahrenberg, R.; Binder, L.; Töpper, A.; Lashki, D.J.; Schwarz, S.; et al. Exercise Training Improves Exercise Capacity and Diastolic Function in Patients with Heart Failure with Preserved Ejection Fraction Results of the Ex-DHF (Exercise training in Diastolic Heart Failure) Pilot Study. J. Am. Coll. Cardiol. 2011, 58, 1780–1791. [Google Scholar] [CrossRef] [PubMed]
- Gary, R.A.; Sueta, C.A.; Dougherty, M.; Rosenberg, B.; Cheek, D.; Preisser, J.; Neelon, V.; McMurray, R. Home-based exercise improves functional performance and quality of life in women with diastolic heart failure. Heart Lung 2004, 33, 210–218. [Google Scholar] [CrossRef]
- Haykowsky, M.J.; Brubaker, P.H.; Stewart, K.P.; Morgan, T.M.; Eggebeen, J.; Kitzman, D.W. Effect of Endurance Training on the Determinants of Peak Exercise Oxygen Consumption in Elderly Patients with Stable Compensated Heart Failure and Preserved Ejection Fraction. J. Am. Coll. Cardiol. 2012, 60, 120–128. [Google Scholar] [CrossRef]
- Kitzman, D.W.; Brubaker, P.H.; Morgan, T.M.; Stewart, K.P.; Little, W.C. Exercise Training in Older Patients with Heart Failure and Preserved Ejection Fraction: A Randomized, Controlled, Single-Blind Trial. Circ. Heart Fail. 2010, 3, 659–667. [Google Scholar] [CrossRef]
- Kitzman, D.W.; Brubaker, P.H.; Herrington, D.M.; Morgan, T.M.; Stewart, K.P.; Hundley, W.G.; Abdelhamed, A.; Haykowsky, M.J. Effect of Endurance Exercise Training on Endothelial Function and Arterial Stiffness in Older Patients with Heart Failure and Preserved Ejection Fraction: A Randomized, Controlled, Single-Blind Trial. J. Am. Coll. Cardiol. 2013, 62, 584–592. [Google Scholar] [CrossRef]
- Kitzman, D.W.; Brubaker, P.; Morgan, T.; Haykowsky, M.; Hundley, G.; Kraus, W.E.; Eggebeen, J.; Nicklas, B.J. Effect of Caloric Restriction or Aerobic Exercise Training on Peak Oxygen Consumption and Quality of Life in Obese Older Patients with Heart Failure with Preserved Ejection Fraction: A Randomized Clinical Trial. JAMA 2016, 315, 36–46. [Google Scholar] [CrossRef]
- Maldonado-Martín, S.; Brubaker, P.H.; Eggebeen, J.; Stewart, K.P.; Kitzman, D.W. Association between six-minute walk distance and objective variables of functional capacity after exercise training in elderly heart failure patients with preserved ejection fraction: A randomized exercise trial. Arch. Phys. Med. Rehabil. 2017, 98, 600–603. [Google Scholar] [CrossRef]
- 31 Mueller, S.; Winzer, E.B.; Duvinage, A.; Gevaert, A.B.; Edelmann, F.; Haller, B.; Pieske-Kraigher, E.; Beckers, P.; Bobenko, A.; Hommel, J.; et al. Effect of High-Intensity Interval Training, Moderate Continuous Training, or Guideline-Based Physical Activity Advice on Peak Oxygen Consumption in Patients with Heart Failure with Preserved Ejection Fraction: A Randomized Clinical Trial. JAMA 2021, 325, 542–551. [Google Scholar] [CrossRef]
- Smart, N.A.; Haluska, B.; Jeffriess, L.; Leung, D. Exercise Training in Heart Failure with Preserved Systolic Function: A Randomized Controlled Trial of the Effects on Cardiac Function and Functional Capacity. Congest. Heart Fail. 2012, 18, 295–301. [Google Scholar] [CrossRef]
- Cavero-Redondo, I.; Martínez-García, I.; Saz-Lara, A.; Garcia-Klepzig, J.L.; Álvarez-Bueno, C.; Martínez-Vizcaino, V. Comparative effect of different physical exercise training on exercise capacity and cardiac function in heart failure with preserved ejection fraction: A network meta-analysis. ExIC-FEp Study. Eur. J. Cardiovasc. Nurs. 2023, zvad018. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 74, e177–e232. [Google Scholar] [CrossRef]
- Asrar Ul Haq, M.; Goh, C.Y.; Levinger, I.; Wong, C.; Hare, D.L. Clinical utility of exercise training in heart failure with reduced and preserved ejection fraction. Clin. Med. Insights Cardiol. 2015, 9, CMC-S21372. [Google Scholar]
- Borlaug, B.A.; Olson, T.P.; Lam, C.S.; Flood, K.S.; Lerman, A.; Johnson, B.D.; Redfield, M.M. Global cardiovascular reserve dysfunction in heart failure with preserved ejection fraction. J. Am. Coll. Cardiol. 2010, 56, 845–854. [Google Scholar] [CrossRef]
- Akiyama, E.; Sugiyama, S.; Matsuzawa, Y.; Konishi, M.; Suzuki, H.; Nozaki, T.; Ohba, K.; Matsubara, J.; Maeda, H.; Horibata, Y.; et al. Incremental prognostic significance of peripheral endothelial dysfunction in patients with heart failure with normal left ventricular ejection fraction. J. Am. Coll. Cardiol. 2012, 60, 1778–1786. [Google Scholar] [CrossRef]
- Ter Maaten, J.M.; Damman, K.; Verhaar, M.C.; Paulus, W.J.; Duncker, D.J.; Cheng, C.; Van Heerebeek, L.; Hillege, H.L.; Lam, C.S.; Navis, G.; et al. Connecting heart failure with preserved ejection fraction and renal dysfunction: The role of endothelial dysfunction and inflammation. Eur. J. Heart Fail. 2016, 18, 588–598. [Google Scholar] [CrossRef]
- Weber, T.; and Chirinos, J.A. Pulsatile arterial haemodynamics in heart failure. Eur. Heart J. 2018, 39, 3847–3854. [Google Scholar] [CrossRef]
- Saz-Lara, A.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Notario-Pacheco, B.; Reina-Gutiérrez, S.; Sequí-Domínguez, I.; Ruiz, J.R.; Martínez-Vizcaíno, V. What type of physical exercise should be recommended for improving arterial stiffness on adult population? A network meta-analysis. Eur. J. Cardiovasc. Nurs. 2021, 20, 696–716. [Google Scholar] [CrossRef] [PubMed]
- Reddy, Y.N.V.; Rikhi, A.; Obokata, M.; Shah, S.J.; Lewis, G.D.; AbouEzzedine, O.F.; Dunlay, S.; McNulty, S.; Chakraborty, H.; Stevenson, L.W.; et al. Quality of life in heart failure with preserved ejection fraction: Importance of obesity, functional capacity, and physical inactivity. Eur. J. Heart Fail. 2020, 22, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Moradi, M.; Daneshi, F.; Behzadmehr, R.; Rafiemanesh, H.; Bouya, S.; Raeisi, M. Quality of life of chronic heart failure patients: A systematic review and meta-analysis. Heart Fail. Rev. 2020, 25, 993–1006. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.C.; Yang, N.I.; Wang, C.H.; Cherng, W.J.; Chou, S.L.; Pan, T.L.; Wang, J.S. Aerobic interval training elicits different hemodynamic adaptations between heart failure patients with preserved and reduced ejection fraction. Am. J. Phys. Med. Rehabil. 2016, 95, 15–27. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| 1. HFpEF (diagnosis according to ESC 2021 criteria): a. Signs and symptoms of HF. b. LVEF ≥ 50%. c. Objective evidence of cardiac structural and/or functional abnormalities consistent with the presence of left ventricular diastolic dysfunction/elevated left ventricular filling pressures, including elevated natriuretic peptide. 2. Sedentary men and women (structured exercise < 2 × 30 min/week). 3. Age ≥ 40 years. 4. Written informed consent. 5. Clinically stable for ≥6 weeks. 6. Optimal medical treatment for ≥6 weeks. | 1. Noncardiac causes of HF symptoms: -Significant valvular or coronary artery disease. -Uncontrolled hypertension or arrhythmias. -Primary cardiomyopathies. 2. Significant pulmonary disease (FEV1 < 50% predicted, GOLD III-IV). 3. Exercise disability or conditions that may interfere with exercise intervention. 4. Myocardial infarction within the last 3 months. 5. Signs of ischemia during maximal cardiopulmonary stress test. 6. Comorbidity (renal failure, cancer, cognitive impariment) that may influence prognosis at 1 year. 7. Participation in another clinical trial. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavero-Redondo, I.; Saz-Lara, A.; Martínez-García, I.; Bizzozero-Peroni, B.; Díaz-Goñi, V.; Díez-Fernández, A.; Moreno-Herráiz, N.; Pascual-Morena, C. Comparative Effect of Two Types of Physical Exercise for the Improvement of Exercise Capacity, Diastolic Function, Endothelial Function and Arterial Stiffness in Participants with Heart Failure with Preserved Ejection Fraction (ExIC-FEp Study): Protocol for a Randomized Controlled Trial. J. Clin. Med. 2023, 12, 3535. https://doi.org/10.3390/jcm12103535
Cavero-Redondo I, Saz-Lara A, Martínez-García I, Bizzozero-Peroni B, Díaz-Goñi V, Díez-Fernández A, Moreno-Herráiz N, Pascual-Morena C. Comparative Effect of Two Types of Physical Exercise for the Improvement of Exercise Capacity, Diastolic Function, Endothelial Function and Arterial Stiffness in Participants with Heart Failure with Preserved Ejection Fraction (ExIC-FEp Study): Protocol for a Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(10):3535. https://doi.org/10.3390/jcm12103535
Chicago/Turabian StyleCavero-Redondo, Iván, Alicia Saz-Lara, Irene Martínez-García, Bruno Bizzozero-Peroni, Valentina Díaz-Goñi, Ana Díez-Fernández, Nerea Moreno-Herráiz, and Carlos Pascual-Morena. 2023. "Comparative Effect of Two Types of Physical Exercise for the Improvement of Exercise Capacity, Diastolic Function, Endothelial Function and Arterial Stiffness in Participants with Heart Failure with Preserved Ejection Fraction (ExIC-FEp Study): Protocol for a Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 10: 3535. https://doi.org/10.3390/jcm12103535
APA StyleCavero-Redondo, I., Saz-Lara, A., Martínez-García, I., Bizzozero-Peroni, B., Díaz-Goñi, V., Díez-Fernández, A., Moreno-Herráiz, N., & Pascual-Morena, C. (2023). Comparative Effect of Two Types of Physical Exercise for the Improvement of Exercise Capacity, Diastolic Function, Endothelial Function and Arterial Stiffness in Participants with Heart Failure with Preserved Ejection Fraction (ExIC-FEp Study): Protocol for a Randomized Controlled Trial. Journal of Clinical Medicine, 12(10), 3535. https://doi.org/10.3390/jcm12103535