
Comparison of Remimazolam-Flumazenil versus Propofol for Rigid Bronchoscopy: A Prospective Randomized Controlled Trial

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Patient Enrollment and Exclusion Criteria
2.3. Randomization and Blinding
2.4. Anesthesia Method Selection
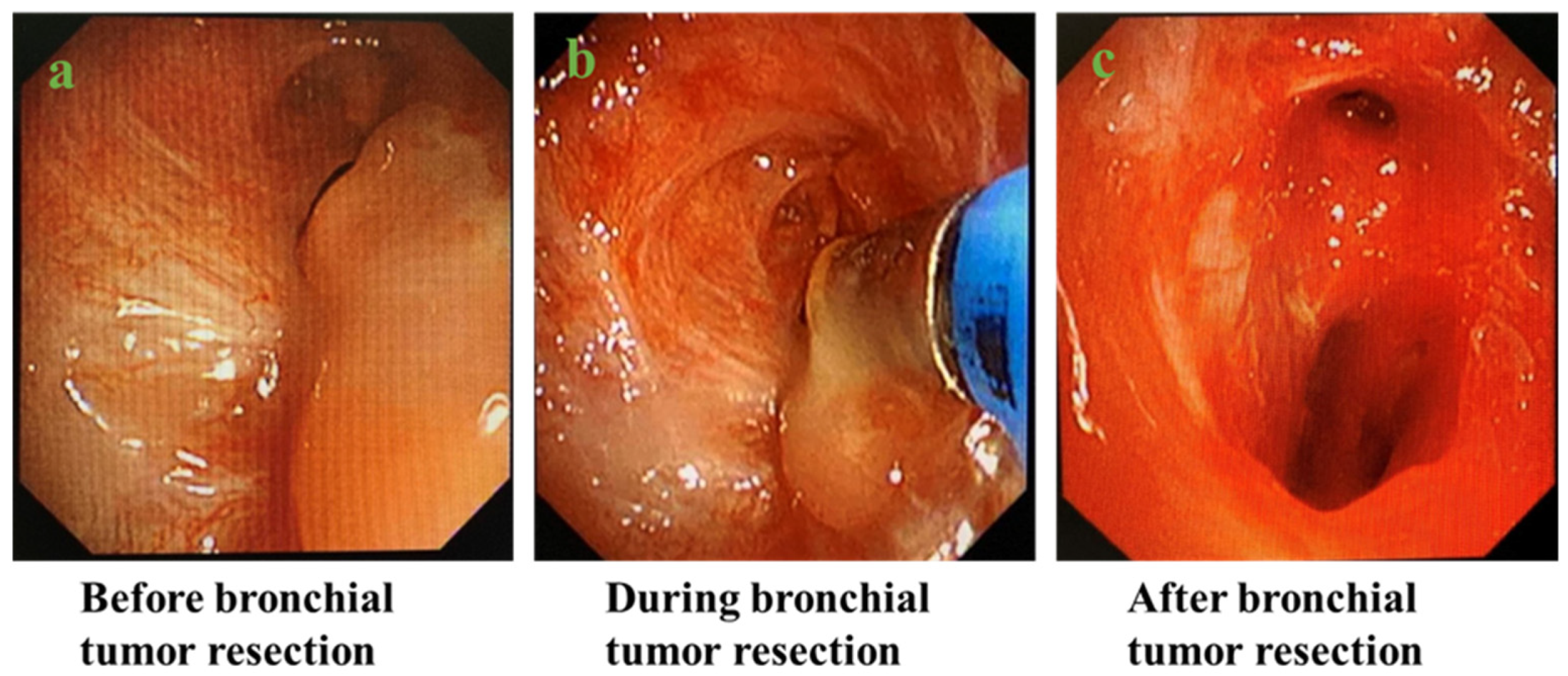
2.5. Operative Process
2.6. Data Collection
2.7. Statistical Analysis
2.8. Ethics
3. Results
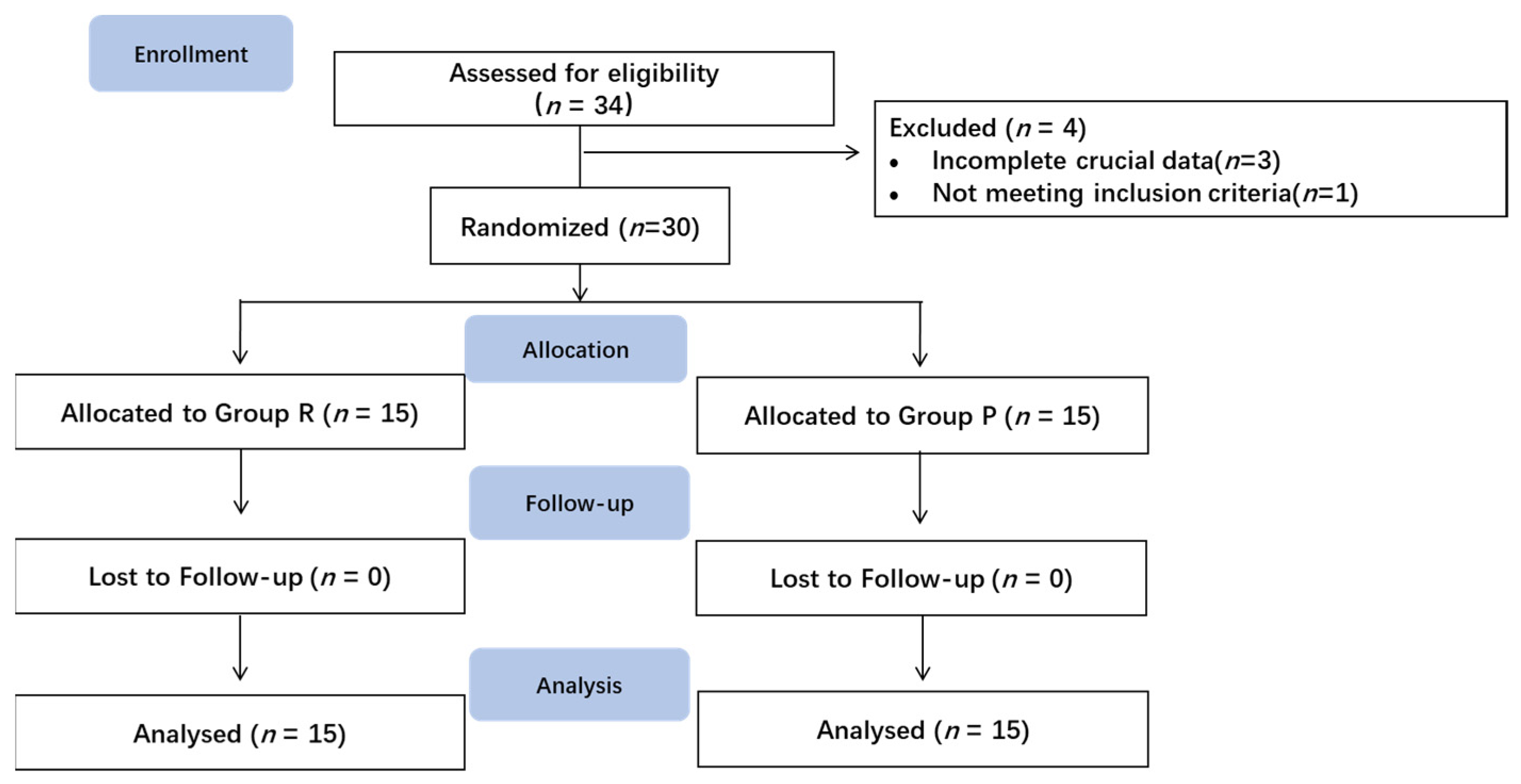
3.1. Participants
3.2. Demographic and Clinical Characteristics
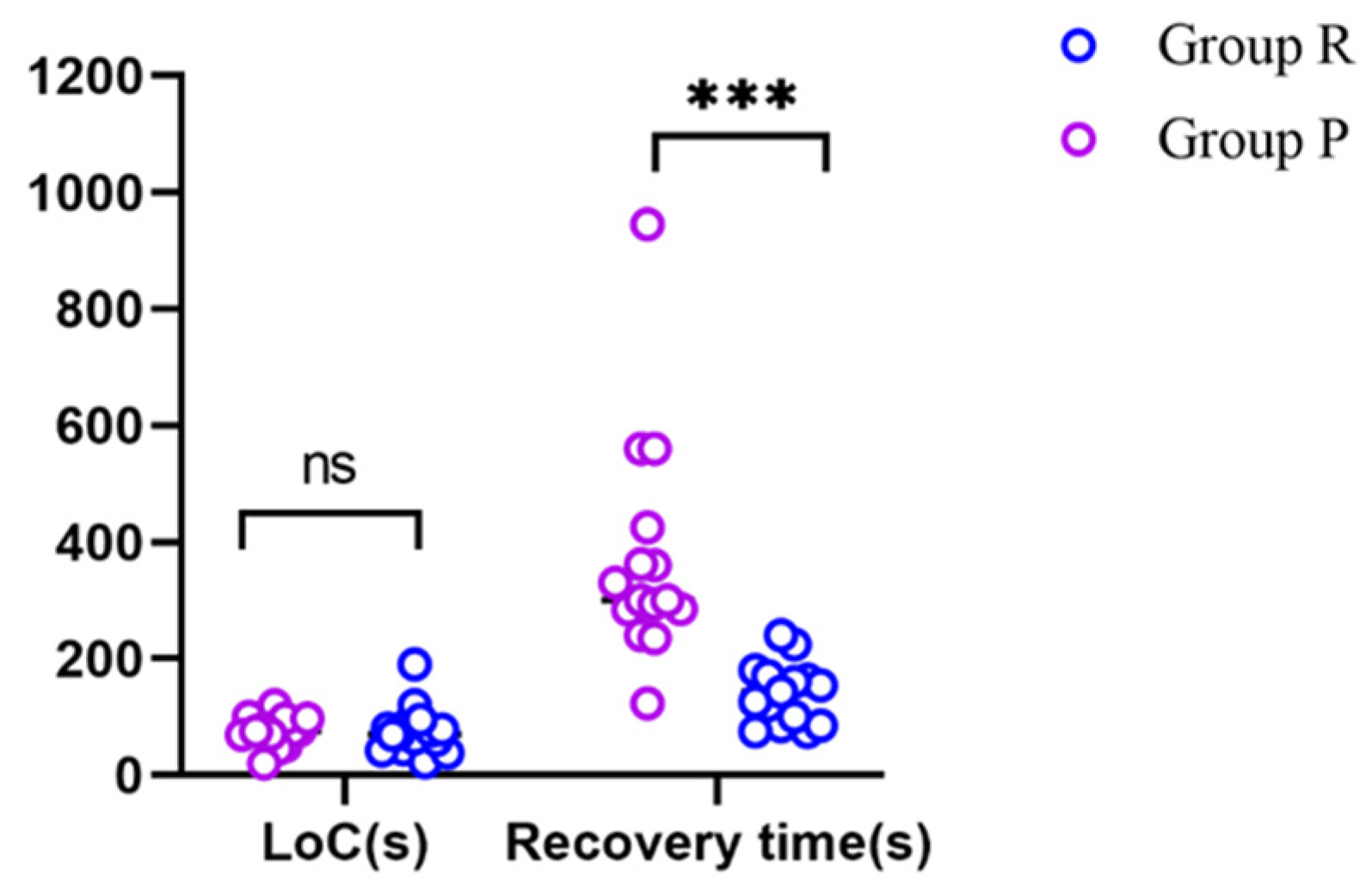
3.3. LoC and Recovery Time
3.4. Parameters during and after Anesthesia
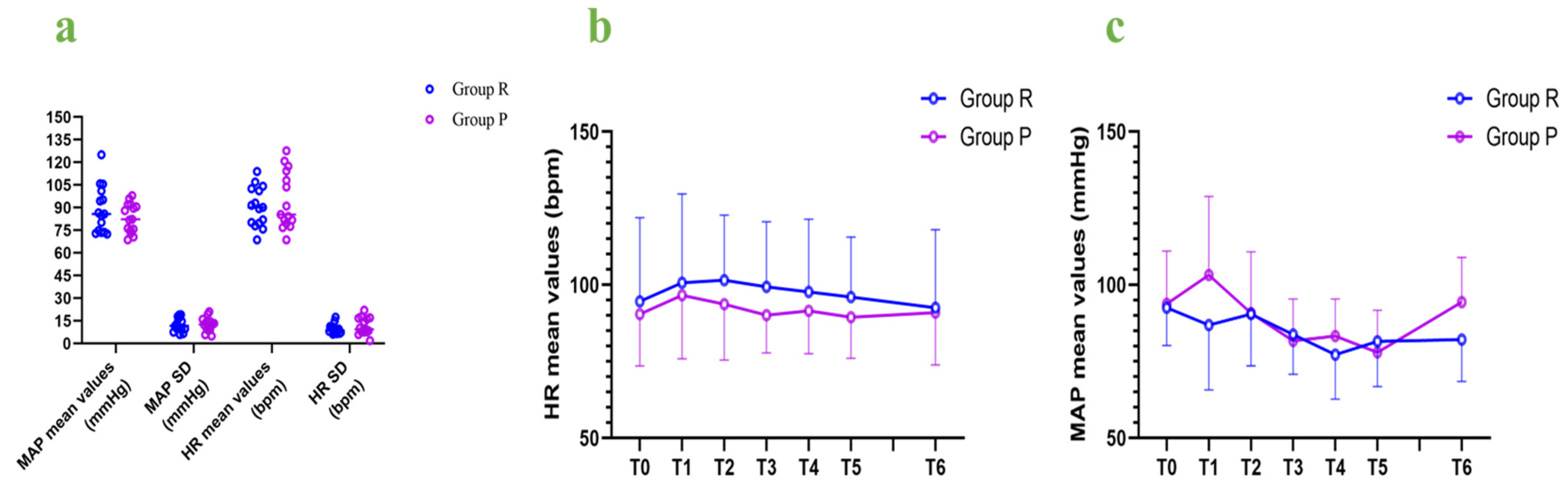
3.5. Hemodynamic Fluctuations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Minto, C.F.; Schnider, T.W. Contributions of PK/PD modeling to intravenous anesthesia. Clin. Pharmacol. Ther. 2008, 84, 27–38. [Google Scholar] [CrossRef]
- Sneyd, J.R.; Rigby-Jones, A.E. Remimazolam for anaesthesia or sedation. Curr. Opin. Anaesthesiol. 2020, 33, 506–511. [Google Scholar] [CrossRef]
- Morimoto, Y. Efficacy and Safety Profile of Remimazolam for Sedation in Adults Undergoing Short Surgical Procedures. Ther. Clin. Risk Manag. 2022, 18, 95–100. [Google Scholar] [CrossRef]
- Antonik, L.J.; Goldwater, D.R.; Kilpatrick, G.J.; Tilbrook, G.S.; Borkett, K.M. A placebo- and midazolam-controlled phase I single ascending-dose study evaluating the safety, pharmacokinetics, and pharmacodynamics of remimazolam (CNS 7056): Part I. Safety, efficacy, and basic pharmacokinetics. Anesth. Analg. 2012, 115, 274–283. [Google Scholar] [CrossRef]
- Mao, Y.; Guo, J.; Yuan, J.; Zhao, E.; Yang, J. Quality of Recovery After General Anesthesia with Remimazolam in Patients’ Undergoing Urologic Surgery: A Randomized Controlled Trial Comparing Remimazolam with Propofol. Drug Des. Dev. Ther. 2022, 16, 1199–1209. [Google Scholar] [CrossRef]
- Lee, B.; Kim, M.H.; Kong, H.J.; Shin, H.J.; Yang, S.; Kim, N.Y.; Chae, D. Effects of Remimazolam vs. Sevoflurane Anesthesia on Intraoperative Hemodynamics in Patients with Gastric Cancer Undergoing Robotic Gastrectomy: A Propensity Score-Matched Analysis. J. Clin. Med. 2022, 11, 2643. [Google Scholar] [CrossRef]
- Liu, T.; Lai, T.; Chen, J.; Lu, Y.; He, F.; Chen, Y.; Xie, Y. Effect of remimazolam induction on hemodynamics in patients undergoing valve replacement surgery: A randomized, double-blind, controlled trial. Pharmacol. Res. Perspect. 2021, 9, e00851. [Google Scholar] [CrossRef]
- Guo, J.; Qian, Y.; Zhang, X.; Han, S.; Shi, Q.; Xu, J. Remimazolam tosilate compared with propofol for gastrointestinal endoscopy in elderly patients: A prospective, randomized and controlled study. BMC Anesthesiol. 2022, 22, 180. [Google Scholar] [CrossRef]
- Stohr, T.; Colin, P.J.; Ossig, J.; Pesic, M.; Borkett, K.; Winkle, P.; Struys, M.; Schippers, F. Pharmacokinetic properties of remimazolam in subjects with hepatic or renal impairment. Br. J. Anaesth. 2021, 127, 415–423. [Google Scholar] [CrossRef]
- Wesolowski, A.M.; Zaccagnino, M.P.; Malapero, R.J.; Kaye, A.D.; Urman, R.D. Remimazolam: Pharmacologic Considerations and Clinical Role in Anesthesiology. Pharmacotherapy 2016, 36, 1021–1027. [Google Scholar] [CrossRef]
- Kilpatrick, G.J. Remimazolam: Non-Clinical and Clinical Profile of a New Sedative/Anesthetic Agent. Front. Pharmacol. 2021, 12, 690875. [Google Scholar] [CrossRef]
- Aya, D.; Hoshi, T.; Yamaguchi, H. Predicting the amount of flumazenil needed to antagonize remimazolam. Eur. J. Gastroenterol. Hepatol. 2021, 33, 1335–1336. [Google Scholar] [CrossRef]
- Chen, X.; Sang, N.; Song, K.; Zhong, W.; Wang, H.; Jiang, J.; Huang, Y.; Hu, P. Psychomotor Recovery Following Remimazolam-induced Sedation and the Effectiveness of Flumazenil as an Antidote. Clin. Ther. 2020, 42, 614–624. [Google Scholar] [CrossRef]
- Doi, M.; Morita, K.; Takeda, J.; Sakamoto, A.; Yamakage, M.; Suzuki, T. Efficacy and safety of remimazolam versus propofol for general anesthesia: A multicenter, single-blind, randomized, parallel-group, phase IIb/III trial. J. Anesth. 2020, 34, 543–553. [Google Scholar] [CrossRef]
- Sheng, X.Y.; Liang, Y.; Yang, X.Y.; Li, L.E.; Ye, X.; Zhao, X.; Cui, Y.M. Safety, pharmacokinetic and pharmacodynamic properties of single ascending dose and continuous infusion of remimazolam besylate in healthy Chinese volunteers. Eur. J. Clin. Pharmacol. 2020, 76, 383–391. [Google Scholar] [CrossRef]
- Oka, S.; Satomi, H.; Sekino, R.; Taguchi, K.; Kajiwara, M.; Oi, Y.; Kobayashi, R. Sedation outcomes for remimazolam, a new benzodiazepine. J. Oral Sci. 2021, 63, 209–211. [Google Scholar] [CrossRef]
- Park, I.; Cho, M.; Nam, S.W.; Hwang, J.W.; Do, S.H.; Na, H.S. Total intravenous anesthesia induced and maintained by a combination of remimazolam and remifentanil without a neuromuscular blocking agent: A prospective, observational pilot study. BMC Anesthesiol. 2022, 22, 237. [Google Scholar] [CrossRef]
- Kim, K.M.; Bang, J.Y.; Lee, J.M.; Yang, H.S.; Choi, B.M.; Noh, G.J. Effect-site concentration of remimazolam at loss and recovery of responsiveness during general anesthesia: A simulation study. Anesth. Pain Med. 2022, 17, 262–270. [Google Scholar] [CrossRef]
- Schuttler, J.; Eisenried, A.; Lerch, M.; Fechner, J.; Jeleazcov, C.; Ihmsen, H. Pharmacokinetics and Pharmacodynamics of Remimazolam (CNS 7056) after Continuous Infusion in Healthy Male Volunteers: Part I. Pharmacokinetics and Clinical Pharmacodynamics. Anesthesiology 2020, 132, 636–651. [Google Scholar] [CrossRef]
- Oh, J.; Park, S.Y.; Lee, S.Y.; Song, J.Y.; Lee, G.Y.; Park, J.H.; Joe, H.B. Determination of the 95% effective dose of remimazolam to achieve loss of consciousness during anesthesia induction in different age groups. Korean J. Anesthesiol. 2022, 75, 510–517. [Google Scholar] [CrossRef]
- Dai, G.; Pei, L.; Duan, F.; Liao, M.; Zhang, Y.; Zhu, M.; Zhao, Z.; Zhang, X. Safety and efficacy of remimazolam compared with propofol in induction of general anesthesia. Minerva Anestesiol. 2021, 87, 1073–1079. [Google Scholar] [CrossRef]
- Sneyd, J.R.; Absalom, A.R.; Barends, C.R.M.; Jones, J.B. Hypotension during propofol sedation for colonoscopy: A retrospective exploratory analysis and meta-analysis. Br. J. Anaesth. 2022, 128, 610–622. [Google Scholar] [CrossRef]
- Yao, Y.; Guan, J.; Liu, L.; Fu, B.; Chen, L.; Zheng, X. Discharge readiness after remimazolam versus propofol for colonoscopy: A randomised, double-blind trial. Eur. J. Anaesthesiol. 2022, 39, 911–917. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, X.; Zhang, Q.; Wang, Z.; Zhu, S. Application effects of remimazolam and propofol on elderly patients undergoing hip replacement. BMC Anesthesiol. 2022, 22, 118. [Google Scholar] [CrossRef]
- Sneyd, J.R.; Gambus, P.L.; Rigby-Jones, A.E. Current status of perioperative hypnotics, role of benzodiazepines, and the case for remimazolam: A narrative review. Br. J. Anaesth. 2021, 127, 41–55. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group R (n = 15) | Group P (n = 15) | p-Value | |
|---|---|---|---|
| Age | 61.13 ± 8.62 | 60.13 ± 7.24 | 0.733 a |
| Sex, male/female | 12/3 | 15/0 | 0.224 b |
| BMI | 20.08 ± 3.81 | 21.73 ± 2.89 | 0.194 a |
| ASA physical status II/III/IV | 7/7/1 | 11/4/0 | 0.187 c |
| Smoking history, n (%) | 10 (66.7) | 9 (60.0) | 1.000 b |
| PONS ≥ 1 n (%) | 5 (33.3) | 2 (13.3) | 0.203 b |
| Group R (n = 15) | Group P (n = 15) | p-Value | |
|---|---|---|---|
| Loss of consciousness (s) | 76 ± 40 | 75 ± 25 | 0.952 a |
| MAP mean value (mmHg) | 83.29 ± 9.66 | 88.79 ± 15.54 | 0.255 a |
| MAP SD (mmHg) | 12.42 ± 4.48 | 12.69 ± 4.53 | 0.869 a |
| Heart rate mean value (bpm) | 94.58 ± 18.89 | 90.46 ± 13.14 | 0.825 a |
| Heart rate SD (bpm) | 11.46 ± 5.54 | 9.57 ± 3.22 | 0.262 a |
| Hypotension (n (%)) | 6 (40.0) | 5 (33.3) | 1.000 b |
| Bradycardia (n (%)) | 0 (0.0) | 1 (6.7) | 1.000 b |
| Stress times | 11 | 13 | 0.272 a |
| Average dose of remimazolam or propofol (mg) | 59.06 ± 16.89 | 263.33 ± 100.80 | NS |
| Average dose of remifentanil (ug) | 382.73 ± 196.12 | 365.60 ± 212.95 | 0.820 a |
| Number of patients using vasoactive drugs (n (%)) | 6 (40.0) | 2 (13.3) | 0.215 b |
| Ephedrine (n (%)) | 1 (6.7) | 2 (13.3) | 1.000 b |
| Dopamine (n (%)) | 2 (13.3) | 0 (0.0) | 0.483 b |
| Metaraminol (n (%)) | 2 (13.3) | 0 (0.0) | 0.483 b |
| Phenylephrine (n (%)) | 1 (6.7) | 0 (0.0) | 1.000 b |
| Beta blockers (n (%)) | 2 (13.3) | 1 (6.7) | 0.550 b |
| Duration of operation (min) | 36.67 ± 19.85 | 44.40 ± 22.72 | 0.424 a |
| Recovery time (s) | 140 ± 52 | 374 ± 195 | 0.000 a * |
| Duration of anesthesia (min) | 41.47 ± 19.31 | 49.60 ± 22.86 | 0.424 a |
| Observer’s Assessment of Alertness/Sedation (OAA/S) Scale | |||
| - 3 (n (%)) | 1 (6.7) | 1 (6.7) | 1.0 c |
| - 4 (n (%)) | 1 (6.7) | 1 (6.7) | |
| - 5 (n (%)) | 13 (86.7) | 13 (86.7) | |
| POD (n (%)) | 0 (0.0) | 1 (6.7) | 1.000 b |
| PONV (n (%)) | 0 (0.0) | 0 (0.0) | NS |
| Modified Brice Questionnaire (n (%)) | 0 (0.0) | 0 (0.0) | NS |
| Cough (n (%)) | 8 (53.3) | 8 (53.3) | 1.000 b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, Y.; Chen, M.; Gu, F.; Chen, J.; Zhang, W.; Huang, Z.; Zhu, D.; Song, J.; Fang, J.; Yu, W.; et al. Comparison of Remimazolam-Flumazenil versus Propofol for Rigid Bronchoscopy: A Prospective Randomized Controlled Trial. J. Clin. Med. 2023, 12, 257. https://doi.org/10.3390/jcm12010257
Pan Y, Chen M, Gu F, Chen J, Zhang W, Huang Z, Zhu D, Song J, Fang J, Yu W, et al. Comparison of Remimazolam-Flumazenil versus Propofol for Rigid Bronchoscopy: A Prospective Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(1):257. https://doi.org/10.3390/jcm12010257
Chicago/Turabian StylePan, Yafei, Mo Chen, Fulei Gu, Jinyan Chen, Wen Zhang, Zhangxiang Huang, Dapeng Zhu, Jia Song, Jun Fang, Weifeng Yu, and et al. 2023. "Comparison of Remimazolam-Flumazenil versus Propofol for Rigid Bronchoscopy: A Prospective Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 1: 257. https://doi.org/10.3390/jcm12010257
APA StylePan, Y., Chen, M., Gu, F., Chen, J., Zhang, W., Huang, Z., Zhu, D., Song, J., Fang, J., Yu, W., & Xie, K. (2023). Comparison of Remimazolam-Flumazenil versus Propofol for Rigid Bronchoscopy: A Prospective Randomized Controlled Trial. Journal of Clinical Medicine, 12(1), 257. https://doi.org/10.3390/jcm12010257