

Oxygen–Ozone Therapy in Cervicobrachial Pain: A Real-Life Experience
 , , , , , , ,
, , , , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Experimental Protocol
2.3. Local Infiltration
2.4. Inclusion and Exclusion Criteria
2.5. Endpoints
2.6. Statistical Analyses
3. Results
3.1. Patients’ Basic Characteristics
3.2. Pain and Quality of Life
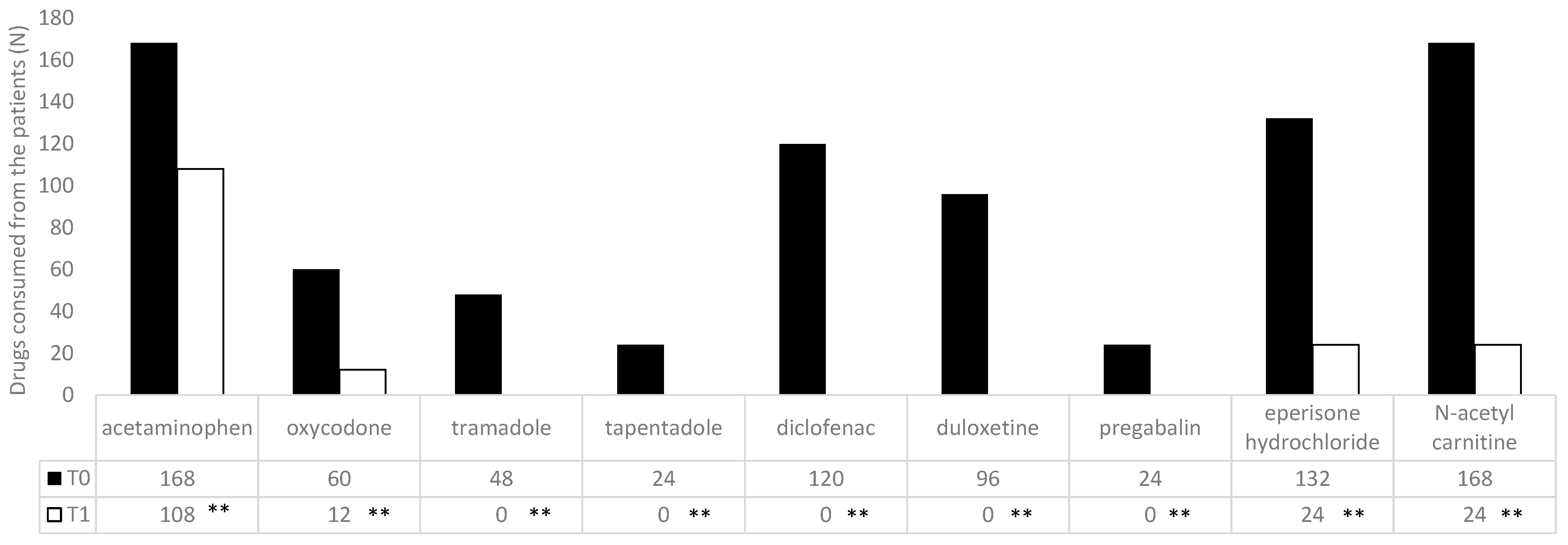
3.3. O2–O3 Treatment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kazeminasab, S.; Nejadghaderi, S.A.; Amiri, P.; Pourfathi, H.; Araj-Khodaei, M.; Sullman, M.J.M.; Kolahi, A.-A.; Safiri, S. Neck pain: Global epidemiology, trends and risk factors. BMC Musculoskelet. Disord. 2022, 23, 1–13. [Google Scholar] [CrossRef]
- Skelly, A.C.; Chou, R.; Dettori, J.R.; Turner, J.A.; Friedly, J.L.; Rundell, S.D.; Fu, R.; Brodt, E.D.; Wasson, N.; Kantner, S.; et al. Noninvasive Nonpharmacological Treatment for Chronic Pain: A Systematic Review Update. In Comparative Effectiveness Review, No. 227; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2020. [Google Scholar]
- Khan, S.A.; Seyam, O.; Smith, N.L.; Reid, I.; Gandhi, J.; Jiang, W. Clinical utility of ozone therapy for musculoskeletal disorders. Med. Gas Res. 2018, 8, 103–110. [Google Scholar] [CrossRef]
- Stoker, G. The Surgical Uses of Ozone. Lancet 1916, 188, 712. [Google Scholar] [CrossRef]
- Özcan, Ç.; Polat, Ö.; Çelik, H.; Uçar, B.Y. The Effect of Paravertebral Ozone Injection in the Treatment of Low Back Pain. Pain Pract. 2019, 19, 821–825. [Google Scholar] [CrossRef] [PubMed]
- Kadir, K.; Syam, Y.; Yusuf, S.; Zainuddin, M. Ozone Therapy on Reduction of Bacterial Colonies and Acceleration of Diabetic Foot Ulcer Healing. Home Healthc. Now 2020, 38, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Peralta, C.; Xaus, C.; Bartrons, R.; Leon, O.S.; Gelpi, E.; Rosello-Catafau, J. Effect of Ozone Treatment on Reactive Oxygen Species and Adenosine Production During Hepatic Ischemia-Reperfusion. Free Rad. Res. 2000, 33, 595–605. [Google Scholar] [CrossRef]
- Sagai, M.; Bocci, V. Mechanisms of Action Involved in Ozone Therapy: Is Healing Induced via a Mild Oxidative Stress? Med. Gas Res. 2011, 1, 29. [Google Scholar] [CrossRef]
- Clavo, B.; Pérez, J.L.; López, L.; Suárez, G.; Lloret, M.; Rodríguez, V.; Macías, D.; Santana, M.; Morera, J.; Fiuza, D.; et al. Effect of Ozone Therapy on Muscle Oxygenation. J. Altern. Complement. Med. 2003, 9, 251–256. [Google Scholar] [CrossRef]
- Clavo, B.; Pérez, J.L.; López, L.; Suárez, G.; Lloret, M.; Rodríguez, V.; Macías, D.; Santana, M.; Hernández, M.A.; Martín-Oliva, R.; et al. Ozone Therapy for Tumor Oxygenation: A Pilot Study. eCAM 2004, 1, 93–98. [Google Scholar] [CrossRef]
- Calderón Guzmá, D.; Islas, J.L.H.; Mejía, G.B.; del Angel, D.S.; García, E.H.; Olguín, H.J. Effect of nutritional status and ozone exposure on Na+/K+ ATPpase and lipid peroxidation in rat brain. Proc. West. Pharmacol. Soc. 2005, 48, 118–121. [Google Scholar]
- Barragán-Mejía, M.G.; Castilla-Serna, L.; Calderón-Guzmán, D.; Hernández-Islas, J.; Labra-Ruiz, N.A.; Rodríguez-Pérez, R.; Angel, D.S.-D. Effect of Nutritional Status and Ozone Exposure on Rat Brain Serotonin. Arch. Med. Res. 2002, 33, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Khor, T.O.; Xu, C.; Shen, G.; Jeong, W.S.; Yu, S.; Kong, A.N. Activation of Nrf2-antioxidant signaling attenuates NFkappaB inflammatory response and elicits apoptosis. Biochem. Pharmacol. 2008, 76, 1485–1489. [Google Scholar] [CrossRef] [PubMed]
- Mourkioti, F.; Kratsios, P.; Luedde, T.; Song, Y.-H.; Delafontaine, P.; Adami, R.; Parente, V.; Bottinelli, R.; Pasparakis, M.; Rosenthal, N. Targeted ablation of IKK2 improves skeletal muscle strength, maintains mass, and promotes regeneration. J. Clin. Investig. 2006, 116, 2945–2954. [Google Scholar] [CrossRef] [PubMed]
- Ulusoy, G.R.; Bilge, A.; Öztürk, Ö. Comparison of corticosteroid injection and ozone injection for relief of pain in chronic lateral epicondylitis. Acta Orthop. Belg. 2019, 85, 317–324. [Google Scholar] [PubMed]
- Martinelli, M.; Giovannangeli, F.; Venditto, T.; Travagli, V. The use of oxygen ozone therapy in the treatment of cervicobrachial pain: Case series study. J. Biol. Regul. Homeost. Agents 2020, 34, 47–55. [Google Scholar]
- Thong, I.S.K.; Jensen, M.P.; Miró, J.; Tan, G. The validity of pain intensity measures: What do the NRS, VAS, VRS, and FPS-R measure? Scand. J. Pain 2018, 18, 99–107. [Google Scholar] [CrossRef]
- VanDenKerkhof, E.G.; Stitt, L.; Clark, A.J.; Gordon, A.; Lynch, M.; Morley-Forster, P.K.; Nathan, H.J.; Smyth, C.; Toth, C.; Ware, M.A.; et al. Sensitivity of the DN4 in Screening for Neuropathic Pain Syndromes. Clin. J. Pain 2018, 34, 30–36. [Google Scholar] [CrossRef]
- Lin, S.H.; Wu, C.C.; Hung, C.J. Use dn4-t questionnaire to rule out non-neuropathic pain. J. Chin. Med. Assoc. 2020, 83, 510. [Google Scholar] [CrossRef]
- Ware, J.E.; Gandek, B. Overview of the SF-36 Health Survey and the International Quality of Life Assessment (IQOLA) Project. J. Clin. Epidemiol. 1998, 51, 903–912. [Google Scholar] [CrossRef]
- Gallelli, L.; Ferreri, G.; Colosimo, M.; Pirritano, D.; Flocco, M.A.; Pelaia, G.; De Sarro, G.B. Adverse drug reactions to antibiotics observed in two pulmonology divisions of Catanzaro, Italy: A six-year retrospective study. Pharmacol. Res. 2002, 46, 395–400. [Google Scholar] [CrossRef]
- Gallelli, L.; Ferreri, G.; Colosimo, M.; Pirritano, D.; Flocco, M.A.; Pelaia, G.; De Sarro, G.B. Retrospective analysis of adverse drug reactions to bronchodilators observed in two pulmonary divisions of Catanzaro, Italy. Pharmacol. Res. 2003, 47, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Bonetti, M.; Cotticelli, B.; Albertini, F.; Brayda-Bruno, M.; Valdenassi, L.; Richelmi, P. Percutaneous Paravertebral Ozone Therapy. Rivista Neuroradiologia 2002, 15, 415–419. [Google Scholar] [CrossRef]
- Bocci, V.A. Scientific and medical aspects of ozone therapy. State of the art. Riv. Ital. Di Ossigeno-Ozonoterapia 2006, 5, 93–104. [Google Scholar] [CrossRef]
- Zeng, J.; Lei, L.; Zeng, Q.; Yao, Y.; Wu, Y.; Li, Q.; Gao, L.; Du, H.; Xie, Y.; Huang, J. Ozone therapy attenuates NF-ΚB–mediated local inflammatory response and activation of th17 cells in treatment for psoriasis. Int. J. Biol. Sci. 2020, 16, 1833–1845. [Google Scholar] [CrossRef]
- Alexandre, A.; Corò, L.; Azuelos, A.; Buric, J.; Salgado, H.; Murga, M.; Marin, F.; Giocoli, H. Intradiscal injection of oxygen-ozone gas mixture for the treatment of cervical disc herniations. Acta Neurochir. Suppl. 2005, 92, 79–82. [Google Scholar] [PubMed]
- Raeissadat, S.A.; Rayegani, S.M.; Sadeghi, F.; Rahimi-Dehgolan, S. Comparison of ozone and lidocaine injection efficacy vs dry needling in myofascial pain syndrome patients. J. Pain Res. 2018, 11, 1273. [Google Scholar] [CrossRef]
- Beyaz, S.G.; Sayhan, H. Six-Month Results of Cervical Intradiscal Oxygen-Ozone Mixture Therapy on Patients with Neck Pain: Preliminary Findings. Pain Physician 2018, 21, E449–E456. [Google Scholar]
- Caterina, P.; Di Paolo, A.; Giofrè, C.; Caglioti, C.; Leuzzi, G.; Siniscalchi, A.; De Sarro, G.; Gallelli, L. Pharmacokinetic drug-drug interaction and their implication in clinical management. J. Res. Med. Sci. 2013, 18, 601. [Google Scholar]
- Gallelli, L.; Siniscalchi, A.; Palleria, C.; Mumoli, L.; Staltari, O.; Squillace, A.; Maida, F.; Russo, E.; Gratteri, S.; De Sarro, G.; et al. Adverse Drug Reactions Related to Drug Administration in Hospitalized Patients. Curr. Drug Saf. 2017, 12, 171–177. [Google Scholar] [CrossRef]
- Madrid Declaration on Ozone Therapy, 3rd ed.; Official Document of ISCO3; Faculdade do Centro Oeste Paulista: Madrid, Spain, March 2020.




{kind=link}
{kind=link}
{kind=link}
| Men (N: 240) | % | Women (N: 300) | % | Delta Percentage of Men vs. Women (%) | p | |
|---|---|---|---|---|---|---|
| Years | ||||||
| 18–64 | 132 | 55 | 216 | 72 | −17.00 | <0.05 |
| >65 | 108 | 45 | 84 | 28 | 17.00 | <0.05 |
| BMI kg/m2 | ||||||
| <24 | 84 | 35 | 84 | 28 | 7.00 | |
| 25–30 | 84 | 35 | 84 | 28 | 7.00 | |
| >30 | 72 | 30 | 132 | 44 | −14 | <0.05 |
| Comorbidity | ||||||
| Anxiety/depression | 0 | 0 | 60 | 20 | −20.0 | <0.01 |
| Arthritis | 0 | 0 | 36 | 12 | −12.0 | <0.05 |
| Benign prostatic hyperplasia | 26 | 10.8 | 0 | 0 | 10.8 | <0.05 |
| Blood hypertension | 96 | 40 | 108 | 36 | 4.0 | |
| Bowel inflammatory diseases | 12 | 5 | 0 | 0 | 5.0 | |
| Chronic obstructive pulmonary disease | 12 | 5 | 24 | 8 | −3.0 | |
| Gastroesophageal reflux diseases | 36 | 15 | 12 | 4 | 11.0 | <0.05 |
| Heart disease | 24 | 10 | 12 | 4 | 6.0 | |
| Hypercholesterolemia | 36 | 15 | 84 | 28 | −13.0 | <0.05 |
| Obesity | 72 | 30 | 84 | 28 | 2.0 | |
| Obstructive sleep apnea | 12 | 5 | 24 | 8 | −3.0 | |
| Osteoarthritis | 72 | 30 | 0 | 0 | 30.0 | <0.01 |
| Osteoporosis | 0 | 0 | 12 | 4 | −4.0 | |
| Sjogren syndrome | 0 | 0 | 24 | 8 | −8.0 | |
| Thyroiditis | 0 | 0 | 48 | 16 | −16.0 | <0.05 |
| Type 2 diabetes | 96 | 40 | 36 | 12 | 28.0 | <0.01 |
| Drug use | ||||||
| Analgesics | 168 | 70 | 192 | 64 | 6.0 | |
| Anti-inflammatory drugs | 63 | 25 | 108 | 36 | −9.8 | |
| Immunosuppressants | 12 | 5 | 24 | 8 | −3.0 | |
| Antidepressants | 48 | 20 | 60 | 20 | 0.0 | |
| Antiepileptics | 12 | 5 | 12 | 4 | 1.0 | |
| Muscle relaxants | 64 | 25 | 108 | 36 | −9.3 | |
| Nutraceuticals | 36 | 15 | 156 | 52 | −37.0 | <0.01 |
| <65 Years (N: 348) | % | ≥65 Years (N: 192) | % | Delta Percentage of Young vs. Old (%) | p | |
|---|---|---|---|---|---|---|
| Men | 132 | 37.9 | 108 | 56.25 | −18.3 | 0.02 |
| Women | 216 | 62.1 | 84 | 43.75 | 18.3 | 0.02 |
| Mean age | 54.3 ± 7.2 | 73.6 ± 7.6 | ||||
| BMI kg/m2 | ||||||
| <24 | 60 | 17.2 | 36 | 18.75 | −1.5 | |
| 25–30 | 36 | 10.3 | 60 | 31.25 | −20.9 | 0.009 |
| >30 | 12 | 3.45 | 96 | 50 | −46.6 | 0.001 |
| Comorbidity | ||||||
| Anxiety/depression | 60 | 17.2 | 0 | 0 | 17.24 | 0.03 |
| Arthritis | 36 | 10.3 | 0 | 0 | 10.34 | |
| Benign prostatic hyperplasia | 12 | 3.45 | 12 | 6.25 | −2.80 | |
| Blood hypertension | 120 | 34.5 | 84 | 43.75 | −9.27 | |
| Bowel inflammatory diseases | 0 | 0 | 12 | 6.25 | −6.25 | |
| Chronic obstructive pulmonary disease | 24 | 6.9 | 12 | 6.25 | 0.65 | |
| Gastroesophageal reflux diseases | 36 | 10.3 | 36 | 18.75 | −8.41 | |
| Heart disease | 0 | 0 | 12 | 6.25 | −6.25 | |
| Hypercholesterolemia | 84 | 24.1 | 36 | 18.75 | 5.39 | |
| Obesity | 108 | 31 | 96 | 50 | −18.97 | 0.02 |
| Obstructive sleep apnea | 36 | 10.3 | 0 | 0 | 10.34 | |
| Osteoarthritis | 24 | 6.9 | 48 | 25 | −18.10 | 0.02 |
| Osteoporosis | 12 | 3.45 | 0 | 0 | 3.45 | |
| Sjogren syndrome | 24 | 6.9 | 0 | 0 | 6.90 | |
| Thyroiditis | 24 | 6.9 | 24 | 12.5 | −5.60 | |
| Type 2 diabetes | 24 | 6.9 | 108 | 56.25 | −49.35 | 0.001 |
| Drug use | ||||||
| Analgesics | 192 | 55.2 | 168 | 87.5 | −32.33 | 0.009 |
| Anti-inflammatory drugs | 111 | 31.9 | 60 | 31.25 | 0.65 | |
| Immunosuppressants | 36 | 10.3 | 0 | 0 | 10.34 | 0.049 |
| Antidepressants | 72 | 20.7 | 36 | 18.75 | 1.94 | |
| Antiepileptics | 24 | 6.9 | 0 | 0 | 6.90 | |
| Muscle relaxants | 156 | 44.8 | 15 | 7.8125 | 37.02 | 0.001 |
| Nutraceuticals | 156 | 44.8 | 36 | 18.75 | 26.08 | 0.009 |
| Item | T0 | T1 | T2 |
|---|---|---|---|
| Burning | 0.76 ± 0.43 | 0.62 ± 0.49 ** | 0.62 ± 0.49 |
| Painful cold | 0.70 ± 0.46 | 0.59 ± 0.50 ** | 0.59 ± 0.50 |
| Electric shocks | 0.19 ± 0.40 | 0.16 ± 0.37 ** | 0.16 ± 0.37 |
| Pain and symptoms | |||
| Tingling | 0.83 ± 0.38 | 0.65 ± 0.48 ** | 0.65 ± 0.48 |
| Pins and needles | 0.05 ± 0.23 | 0.05 ± 0.23 ** | 0.05 ± 0.23 |
| Numbness | 0.89 ± 0.31 | 0.54 ± 0.51 ** | 0.54 ± 0.51 |
| Itching | 0.65 ± 0.48 | 0.19 ± 0.40 ** | 0.21 ± 0.43 |
| Pain located in an area | |||
| Hypoesthesia to touch | 0.62 ± 0.49 | 0.46 ± 0.51 ** | 0.46 ± 0.51 |
| Hypoesthesia to prick | 0.22 ± 0.42 | 0.19 ± 0.40 ** | 0.19 ± 0.40 |
| Pain caused or increased | |||
| Brushing | 0.89 ± 0.31 | 0.59 ± 0.50 ** | 0.59 ± 0.50 |
| T0 | T1 | T2 | |
|---|---|---|---|
| Physical functioning | 65 ± 18.6 | 92 ± 7.5 ** | 91 ± 8.8 |
| Limitations due to physical health | 2.1 ± 1.8 | 75.7 ± 14.3 ** | 73 ± 15.6 |
| Limitations due to emotional problems | 1.2 ± 0.9 | 97.6 ± 4.3 ** | 96.9 ± 4.9 |
| Energy/fatigue | 45 ± 8.2 | 65.3 ± 13.2 ** | 63.4 ± 14.5 |
| Emotional well-being | 68 ± 9.7 | 68.1 ± 11.3 ** | 66.7 ± 11.4 |
| Social functioning | 37.3 ± 3.8 | 75.2 ± 16.5 ** | 73.6 ± 15.2 |
| Pain | 22.7 ± 3.2 | 77.5 ± 12.4 ** | 72.1 ± 16.5 |
| General health | 35.1 ± 5.2 | 66.2 ± 12.4 ** | 64.3 ± 10.3 |
| Health change | 25.3 ± 6.1 | 92.8 ± 6.5 ** | 91.6 ± 7.1 |
| Men | Women | |||||
|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | |
| Analgesics | 168 | 108 ** | 108 | 192 | 96 ** | 96 |
| Anti-inflammatory drugs | 60 | 0 ** | 12 ** | 108 | 36 ** | 48 ** |
| Immunosuppressants | 12 | 12 | 12 | 24 | 12 ** | 12 |
| Antidepressants | 48 | 12 ** | 12 | 60 | 24 ** | 24 |
| Antiepileptics | 12 | 0 ** | 0 | 12 | 0 ** | 0 |
| Muscle relaxants | 60 | 12 ** | 12 | 108 | 24 ** | 24 |
| Nutrients | 36 | 0 ** | 0 | 156 | 24 ** | 24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rania, V.; Marcianò, G.; Casarella, A.; Vocca, C.; Palleria, C.; Calabria, E.; Spaziano, G.; Citraro, R.; De Sarro, G.; Monea, F.; et al. Oxygen–Ozone Therapy in Cervicobrachial Pain: A Real-Life Experience. J. Clin. Med. 2023, 12, 248. https://doi.org/10.3390/jcm12010248
Rania V, Marcianò G, Casarella A, Vocca C, Palleria C, Calabria E, Spaziano G, Citraro R, De Sarro G, Monea F, et al. Oxygen–Ozone Therapy in Cervicobrachial Pain: A Real-Life Experience. Journal of Clinical Medicine. 2023; 12(1):248. https://doi.org/10.3390/jcm12010248
Chicago/Turabian StyleRania, Vincenzo, Gianmarco Marcianò, Alessandro Casarella, Cristina Vocca, Caterina Palleria, Elena Calabria, Giuseppe Spaziano, Rita Citraro, Giovambattista De Sarro, Francesco Monea, and et al. 2023. "Oxygen–Ozone Therapy in Cervicobrachial Pain: A Real-Life Experience" Journal of Clinical Medicine 12, no. 1: 248. https://doi.org/10.3390/jcm12010248
APA StyleRania, V., Marcianò, G., Casarella, A., Vocca, C., Palleria, C., Calabria, E., Spaziano, G., Citraro, R., De Sarro, G., Monea, F., & Gallelli, L. (2023). Oxygen–Ozone Therapy in Cervicobrachial Pain: A Real-Life Experience. Journal of Clinical Medicine, 12(1), 248. https://doi.org/10.3390/jcm12010248