
Lactate Dehydrogenase/Albumin To-Urea Ratio: A Novel Prognostic Maker for Fatal Clinical Complications in Patients with COVID-19 Infection

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
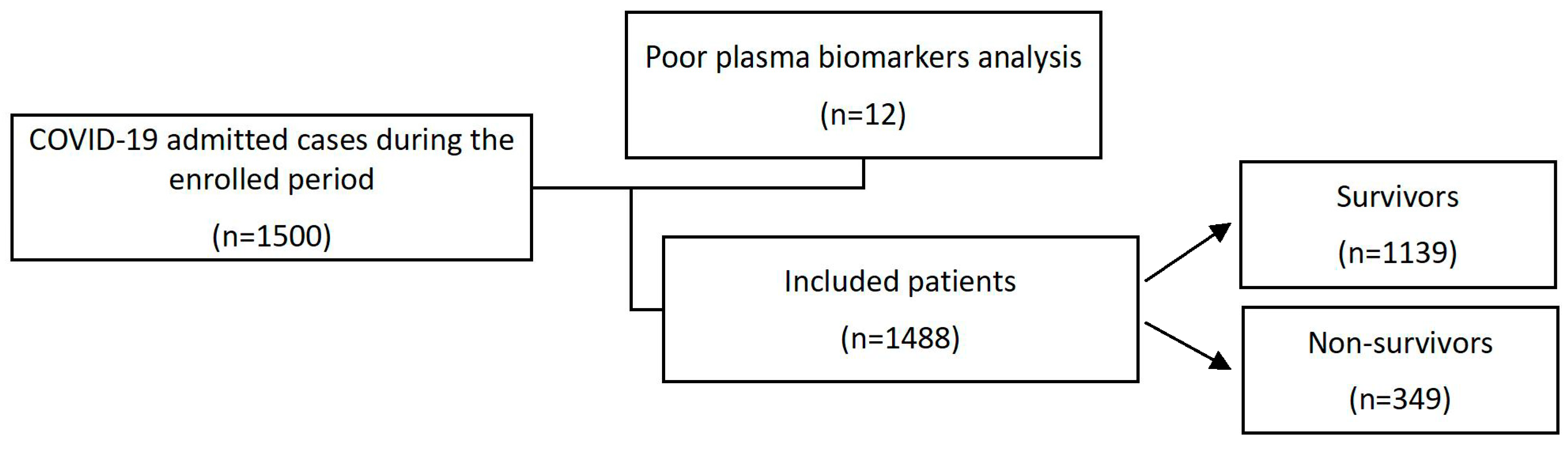
2.1. Study Design and Participants
2.2. General Assessments
2.3. Laboratory Procedures
2.4. Sample Size and Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Haematology Results
3.3. Organ Function Tests
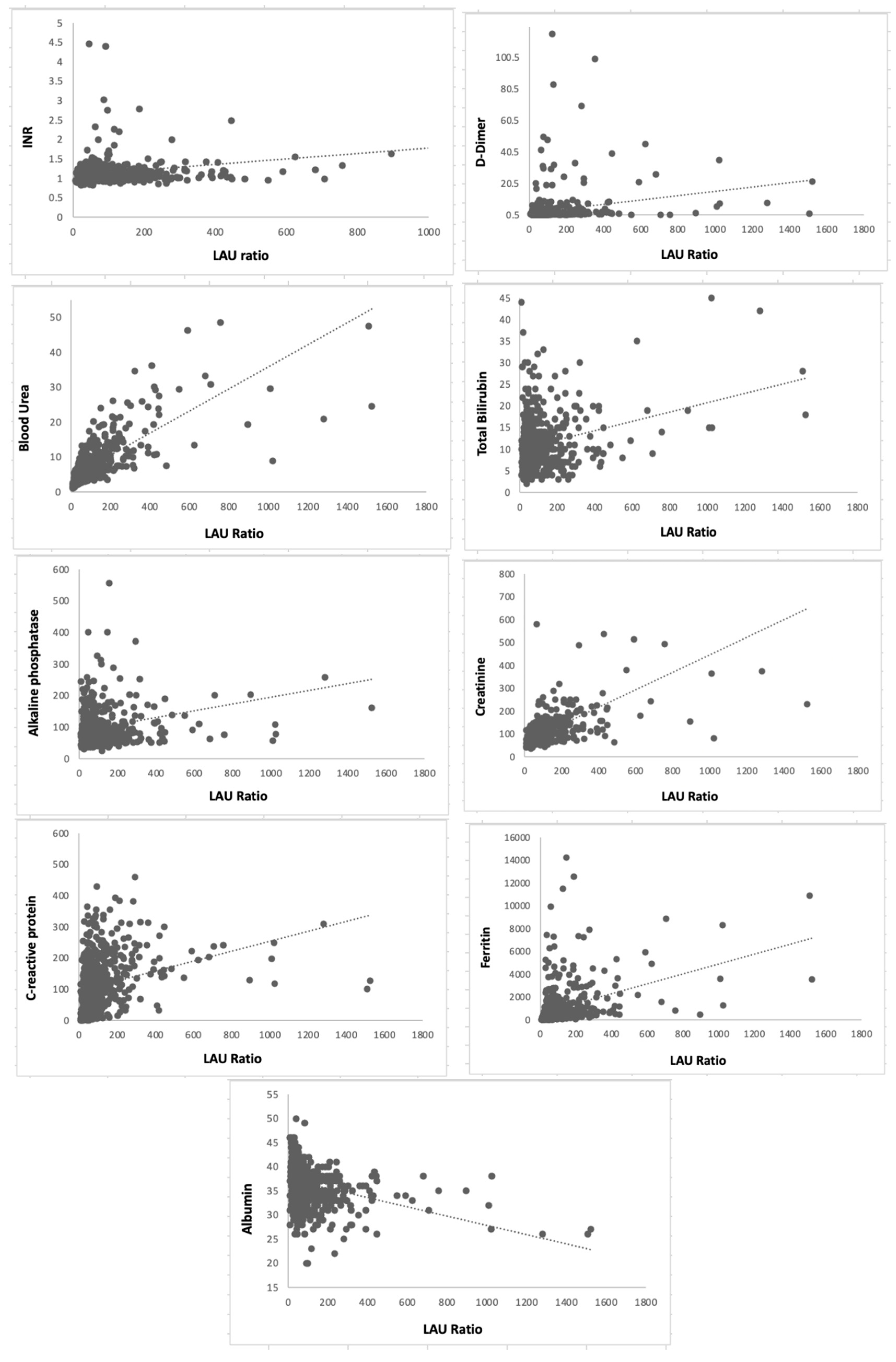
3.4. Correlation Studies
3.5. Analysis of the Area under Receiver Operating Characteristic (AUROC)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cavanagh, D. A Review of Coronaviruses and Toroviruses. In Coronaviruses with Special Emphasis on First Insights Concerning SARS; Springer Science & Business Media: Berlin, Germany, 2005; pp. 1–232. [Google Scholar]
- Yang, Y.; Peng, F.; Wang, R.; Guan, K.; Jiang, T.; Xu, G.; Sun, J.; Chang, C. The Deadly Coronaviruses: The 2003 SARS Pandemic and the 2020 Novel Coronavirus Epidemic in China. J. Autoimmun. 2020, 109, 102434. [Google Scholar] [CrossRef]
- Mackay, I.M.; Arden, K.E. MERS Coronavirus: Diagnostics, Epidemiology and Transmission. Virol. J. 2015, 12, 222. [Google Scholar] [CrossRef]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2020, 19, 141–154. [Google Scholar] [CrossRef]
- Zhu, Z.; Lian, X.; Su, X.; Wu, W.; Marraro, G.A.; Zeng, Y. From SARS and MERS to COVID-19: A Brief Summary and Comparison of Severe Acute Respiratory Infections Caused by Three Highly Pathogenic Human Coronaviruses. Respir. Res. 2020, 21, 224. [Google Scholar] [CrossRef]
- England Summary|Coronavirus (COVID-19) in the UK. Available online: https://coronavirus.data.gov.uk (accessed on 26 November 2022).
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The Clinical and Chest CT Features Associated with Severe and Critical COVID-19 Pneumonia. Investig. Radiol. 2020, 55, 327–331. [Google Scholar] [CrossRef]
- Schröder, I. COVID-19: A Risk Assessment Perspective. ACS Chem. Health Saf. 2020, 27, 160–169. [Google Scholar] [CrossRef]
- Marwah, M.; Shokr, H.; Demitry, A.; Wang, K.; Ahmad, S.; Marwah, S.; Wandroo, F. SARS-2 COVID-19-Induced Immunity Response, a New Prognostic Marker for the Pregnant Population Correlates Inversely with Neonatal Apgar Score. Infection 2022, 1, 3. [Google Scholar] [CrossRef]
- Agbuduwe, C.; Basu, S. Haematological Manifestations of COVID-19: From Cytopenia to Coagulopathy. Eur. J. Haematol. 2020, 105, 540–546. [Google Scholar] [CrossRef]
- Henry, B.M.; de Oliveira, M.H.S.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, Biochemical and Immune Biomarker Abnormalities Associated with Severe Illness and Mortality in Coronavirus Disease 2019 (COVID-19): A Meta-Analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef]
- Yin, M.; Si, L.; Qin, W.; Li, C.; Zhang, J.; Yang, H.; Han, H.; Zhang, F.; Ding, S.; Zhou, M.; et al. Predictive Value of Serum Albumin Level for the Prognosis of Severe Sepsis Without Exogenous Human Albumin Administration: A Prospective Cohort Study. J. Intensive Care Med. 2018, 33, 687–694. [Google Scholar] [CrossRef]
- Higashikawa, T.; Okuro, M.; Ishigami, K.; Mae, K.; Sangen, R.; Mizuno, T.; Usuda, D.; Saito, A.; Kasamaki, Y.; Fukuda, A.; et al. Procalcitonin and Albumin as Prognostic Biomarkers in Elderly Patients with a Risk of Bacterial Infection. J. Int. Med. Res. 2018, 46, 2606–2614. [Google Scholar] [CrossRef]
- Xu, Y.; Yang, H.; Wang, J.; Li, X.; Xue, C.; Niu, C.; Liao, P. Serum Albumin Levels Are a Predictor of COVID-19 Patient Prognosis: Evidence from a Single Cohort in Chongqing, China. Int. J. Gen. Med. 2021, 14, 2785. [Google Scholar] [CrossRef]
- Zein, J.G.; Lee, G.L.; Tawk, M.; Dabaja, M.; Kinasewitz, G.T. Prognostic Significance of Elevated Serum Lactate Dehydrogenase (LDH) in Patients with Severe Sepsis. Chest 2004, 126, 873S. [Google Scholar] [CrossRef]
- Fanali, G.; di Masi, A.; Trezza, V.; Marino, M.; Fasano, M.; Ascenzi, P. Human Serum Albumin: From Bench to Bedside. Mol. Aspects Med. 2012, 33, 209–290. [Google Scholar] [CrossRef]
- Erez, A.; Shental, O.; Tchebiner, J.Z.; Laufer-Perl, M.; Wasserman, A.; Sella, T.; Guzner-Gur, H. Diagnostic and Prognostic Value of Very High Serum Lactate Dehydrogenase in Admitted Medical Patients. Isr. Med. Assoc. J. 2014, 16, 5. [Google Scholar]
- Brancaccio, P.; Lippi, G.; Maffulli, N. Biochemical Markers of Muscular Damage. Clin. Chem. Lab. Med. 2010, 48, 757–767. [Google Scholar] [CrossRef]
- Jialal, I.; Sokoll, L.J. Clinical Utility of Lactate Dehydrogenase. Am. J. Clin. Pathol. 2015, 143, 158–159. [Google Scholar] [CrossRef]
- Jeon, S.Y.; Ryu, S.; Oh, S.K.; Park, J.S.; You, Y.H.; Jeong, W.J.; Cho, Y.C.; Ahn, H.J.; Kang, C.S. Lactate Dehydrogenase to Albumin Ratio as a Prognostic Factor for Patients with Severe Infection Requiring Intensive Care. Medicine 2021, 100, e27538. [Google Scholar] [CrossRef]
- Alizadeh, N.; Tabatabaei, F.; Azimi, A.; Faraji, N.; Akbarpour, S.; Dianatkhah, M.; Moghaddas, A. Lactate Dehydrogenase to Albumin Ratio as a Predictive Factor of COVID-19 Patients’ Outcome; a Cross-Sectional Study. Arch. Acad. Emerg. Med. 2022, 10, e63. [Google Scholar] [CrossRef]
- Liu, Y.-M.; Xie, J.; Chen, M.-M.; Zhang, X.; Cheng, X.; Li, H.; Zhou, F.; Qin, J.-J.; Lei, F.; Chen, Z.; et al. Kidney Function Indicators Predict Adverse Outcomes of COVID-19. Med 2021, 2, 38–48.e2. [Google Scholar] [CrossRef]
- Alirezaei, T.; Hooshmand, S.; Irilouzadian, R.; Hajimoradi, B.; Montazeri, S.; Shayegh, A. The Role of Blood Urea Nitrogen to Serum Albumin Ratio in the Prediction of Severity and 30-Day Mortality in Patients with COVID-19. Health Sci. Rep. 2022, 5, e606. [Google Scholar] [CrossRef] [PubMed]
- Shokr, H.; Gherghel, D. European Society of Cardiology/European Society of Hypertension versus the American College of Cardiology/American Heart Association Guidelines on the Cut-off Values for Early Hypertension: A Microvascular Perspective. Sci. Rep. 2021, 11, 3473. [Google Scholar] [CrossRef] [PubMed]
- Fällmar, D.; Rostami, E.; Kumlien, E.; Ashton, N.J.; Jackmann, S.; Pavel, R.; Blennow, K.; Hultström, M.; Lipcsey, M.; Frithiof, R.; et al. The Extent of Neuroradiological Findings in COVID-19 Shows Correlation with Blood Biomarkers, Glasgow Coma Scale Score and Days in Intensive Care. J. Neuroradiol. 2021, 49, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Shokr, H.; Dias, I.H.K.; Gherghel, D. Oxysterols and Retinal Microvascular Dysfunction as Early Risk Markers for Cardiovascular Disease in Normal, Ageing Individuals. Antioxidants 2021, 10, 1756. [Google Scholar] [CrossRef]
- 14.9 Million Excess Deaths Associated with the COVID-19 Pandemic in 2020 and 2021. Available online: https://www.who.int/news/item/05-05-2022-14.9-million-excess-deaths-were-associated-with-the-covid-19-pandemic-in-2020-and-2021 (accessed on 11 May 2022).
- Robba, C.; Battaglini, D.; Pelosi, P.; Rocco, P.R.M. Multiple Organ Dysfunction in SARS-CoV-2: MODS-CoV-2. Expert Rev. Respir. Med. 2020, 14, 865–868. [Google Scholar] [CrossRef]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk Stratification of Patients Admitted to Hospital with COVID-19 Using the ISARIC WHO Clinical Characterisation Protocol: Development and Validation of the 4C Mortality Score. BMJ 2020, 370, 22. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Liu, Y.; Du, X.; Chen, J.; Jin, Y.; Peng, L.; Wang, H.H.X.; Luo, M.; Chen, L.; Zhao, Y. Neutrophil-to-Lymphocyte Ratio as an Independent Risk Factor for Mortality in Hospitalized Patients with COVID-19. J. Infect. 2020, 81, e6–e12. [Google Scholar] [CrossRef]
- Channappanavar, R.; Perlman, S. Pathogenic Human Coronavirus Infections: Causes and Consequences of Cytokine Storm and Immunopathology. Semin. Immunopathol. 2017, 39, 529–539. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Alfaraj, S.H.; Al-Tawfiq, J.A.; Assiri, A.Y.; Alzahrani, N.A.; Alanazi, A.A.; Memish, Z.A. Clinical Predictors of Mortality of Middle East Respiratory Syndrome Coronavirus (MERS-CoV) Infection: A Cohort Study. Travel Med. Infect. Dis. 2019, 29, 48–50. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Ansar, W.; Ghosh, S. Inflammation and Inflammatory Diseases, Markers, and Mediators: Role of CRP in Some Inflammatory Diseases. In Biology of C Reactive Protein in Health and Disease; Springer: New Delhi, India, 2016; pp. 67–107. [Google Scholar] [CrossRef]
- Indalao, I.L.; Sawabuchi, T.; Takahashi, E.; Kido, H. IL-1b Is a Key Cytokine That Induces Trypsin Upregulation in the Influenza Virus-Cytokine-Trypsin Cycle. Arch. Virol. 2017, 162, 201–211. [Google Scholar] [CrossRef]
- Miglietta, F.; Faneschi, M.L.; Lobreglio, G.; Palumbo, C.; Rizzo, A.; Cucurachi, M.; Portaccio, G.; Guerra, F.; Pizzolante, M. Procalcitonin, C-Reactive Protein and Serum Lactate Dehydrogenase in the Diagnosis of Bacterial Sepsis, SIRS and Systemic Candidiasis. Infez. Med. 2015, 23, 230–237. [Google Scholar]
- Aday, U.; Böyük, A.; Akkoç, H. The Prognostic Significance of Serum Lactate Dehydrogenase-to-Albumin Ratio in Colorectal Cancer. Ann. Surg. Treat. Res. 2020, 99, 161. [Google Scholar] [CrossRef]
- Laham, F.R.; Trott, A.A.; Bennett, B.L.; Kozinetz, C.A.; Jewell, A.M.; Garofalo, R.P.; Piedra, P.A. LDH Concentration in Nasal-Wash Fluid as a Biochemical Predictor of Bronchiolitis Severity. Pediatrics 2010, 125, e225–e233. [Google Scholar] [CrossRef]
- Arnau-Barrés, I.; Güerri-Fernández, R.; Luque, S.; Sorli, L.; Vázquez, O.; Miralles, R. Serum Albumin Is a Strong Predictor of Sepsis Outcome in Elderly Patients. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 743–746. [Google Scholar] [CrossRef]
- Xing, Y.; Xiao, Y.; Zhang, Y.; Mo, P.; Xing, Y.; Xiao, Y.; Deng, L.; Zhao, Q.; Wang, H.; Xiong, Y.; et al. Clinical Characteristics of Refractory Coronavirus Disease 2019 in Wuhan, China. Clin. Infect. Dis. 2021, 73, e4208–e4213. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| GP (A) Survivors (1139) | GP (B) Non-Survivors (349) | p-Value | |
|---|---|---|---|
| Age (year) | 58.66 (18.90) | 75.87 (13.43) | 0.0001 * |
| RR (12–18 bpm) | 19.24 (5.53) | 21.05 (6.24) | <0.001 * |
| SBP (mmHg) | 121 (13.78) | 126.4 (14.3) | 0.76 |
| DBP (mmHg) | 73.01 (16.199) | 71.08 (14.15) | 0.06 |
| MAP (mmHg) | 91 (12.45) | 92.4 (11.37) | 0.37 |
| HR (60–100 bpm) | 81.84 (20.68) | 83.50 (21.03) | 0.19 |
| BMI (18.5–24.9 Kg/m2) | 22.5 (4.6) | 23.1 (5.7) | 0.23 |
| GCS | 9.60 (7.0) | 10.20 (6.23) | 0.16 |
| GP (A) Survivors (1139) | GP (B) Non-Survivors (349) | p-Value | |
|---|---|---|---|
| HB-A1c (<42 mmol/mol) | 52.22 (19.46) | 50.75 (16.38) | 0.530 |
| T-CHOL (<5 mmol/L) | 4.88 (3.48) | 4.39 (0.99) | 0.329 |
| WBCs (4–11 × 109/L) | 8.004 (7.33) | 9.00 (10.1) | 0.095 |
| Hb (115–160 g/L) | 131.72 (21.47) | 122.81 (24.52) | 0.0001 * |
| MCV (80–100 fL) | 86.08 (7.82) | 90.01 (8.80) | 0.0001 * |
| PLT (150–450 × 109/L) | 255.85 (106.17) | 232.49 (104.83) | 0.0001 |
| Neut (1.7–7.5 × 109/L) | 5.92 (4.47) | 6.82 (4.37) | 0.0013 * |
| Lymph (1–4 × 109/L) | 1.32 (1.042) | 1.51 (8.58) | 0.695 |
| Mono (0.2 * 80 × 109/L) | 0.6161 (1.722) | 0.596 (0.44) | 0.839 |
| Eos (>0.5 × 109/L) | 0.058 (0.13) | 0.059 (0.30) | 0.877 |
| Baso (>0.1 × 109/L) | 0.024 (0.023) | 0.025 (0.032) | 0.859 |
| Neut/Lymph | 6.173 (6.095) | 9.52 (9.66) | <0.0001 * |
| LDH/ALB X Urea | 36.51 (92.64) | 81.63 (168.70) | <0.0001 * |
| GP (A) Survivors (1139) | GP (B) Non-Survivors (349) | p-Value | |
|---|---|---|---|
| INR (0.9–1.2) | 1.12 (0.29) | 1.25 (0.69) | 0.003 * |
| D-dimer (0.22–0.46 FEU µg/mL) | 2.96 (9.48) | 4.98 (11.92) | 0.029 * |
| Urea (2.5–7.8 mmol/L) | 6.90 (5.70) | 11.43 (7.74) | 0.0001 * |
| Albumin (35–50 g/L) | 38.37 (11.66) | 33.52 (4.92) | 0.0001 * |
| Bilirubin (<21 µmol/L) | 10.56 (10.98) | 13.11 (15.30) | 0.005 * |
| ALP (30–130 IU/L) | 95.13 (59.73) | 117.13 (128.61) | 0.003 * |
| ALT (4–36 U/L) | 40.77 (48.69) | 43.90 (80.85) | 0.510 |
| CRE (45–110 µmol/L) | 102.43 (9795) | 130.91 (77.09) | 0.0001 * |
| CRP (<1 mg/L) | 84.53 (82.43) | 118.56 (91.51) | 0.0001 * |
| FER (41–400 μg/L) | 854.92 (1324.32) | 1180.42 (1818.14) | 0.021 * |
| LDH (140–280 U/L) | 442.18 (259.71) | 507.349 (341.38) | 0.032 * |
| cTnI (<14 ng/L) | 207.37 (2256.01) | 219.96 (1038.96) | 0.938 |
| 25-OHD (25–40 ng/mL) | 43.53 (31.05) | 46.65 (41.97) | 0.253 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shokr, H.; Marwah, M.K.; Siddiqi, H.; Wandroo, F.; Sanchez-Aranguren, L.; Ahmad, S.; Wang, K.; Marwah, S. Lactate Dehydrogenase/Albumin To-Urea Ratio: A Novel Prognostic Maker for Fatal Clinical Complications in Patients with COVID-19 Infection. J. Clin. Med. 2023, 12, 19. https://doi.org/10.3390/jcm12010019
Shokr H, Marwah MK, Siddiqi H, Wandroo F, Sanchez-Aranguren L, Ahmad S, Wang K, Marwah S. Lactate Dehydrogenase/Albumin To-Urea Ratio: A Novel Prognostic Maker for Fatal Clinical Complications in Patients with COVID-19 Infection. Journal of Clinical Medicine. 2023; 12(1):19. https://doi.org/10.3390/jcm12010019
Chicago/Turabian StyleShokr, Hala, Mandeep Kaur Marwah, Hisam Siddiqi, Farooq Wandroo, Lissette Sanchez-Aranguren, Shakil Ahmad, Keqing Wang, and Sukhjinder Marwah. 2023. "Lactate Dehydrogenase/Albumin To-Urea Ratio: A Novel Prognostic Maker for Fatal Clinical Complications in Patients with COVID-19 Infection" Journal of Clinical Medicine 12, no. 1: 19. https://doi.org/10.3390/jcm12010019
APA StyleShokr, H., Marwah, M. K., Siddiqi, H., Wandroo, F., Sanchez-Aranguren, L., Ahmad, S., Wang, K., & Marwah, S. (2023). Lactate Dehydrogenase/Albumin To-Urea Ratio: A Novel Prognostic Maker for Fatal Clinical Complications in Patients with COVID-19 Infection. Journal of Clinical Medicine, 12(1), 19. https://doi.org/10.3390/jcm12010019