
Does Hysteroscopic Dissection of Partial Uterine Septum Represent a Risk Factor for Placental Abnormalities in Subsequent Pregnancy Compared with Controls Undergoing Other Hysteroscopic Surgery? Results from a Large Case–Control Analysis

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karadag, B.; Dilbaz, B.; Demir, B.; Ozgurluk, I.; Kocak, M.; Karasu, Y.; Gulsah Sahin, E.; Dilbaz, S. Reproductive performance after hysteroscopic metroplasty in infertile women: Complete versus partial uterine septum. Clin. Exp. Obs. Gynecol. 2016, 43, 584–587. [Google Scholar] [CrossRef]
- Mollo, A.; De Franciscis, P.; Colacurci, N.; Cobellis, L.; Perino, A.; Venezia, R.; Alviggi, C.; De Placido, G. Hysteroscopic resection of the septum improves the pregnancy rate of women with unexplained infertility: A prospective controlled trial. Fertil. Steril. 2009, 91, 2628–2631. [Google Scholar] [CrossRef] [PubMed]
- Paradisi, R.; Barzanti, R.; Natali, F.; Battaglia, C.; Venturoli, S. Metroplasty in a large population of women with septate uterus. J. Minim. Invasive Gynecol. 2011, 18, 449–454. [Google Scholar] [CrossRef]
- Tonguc, E.A.; Var, T.; Batioglu, S. Hysteroscopic metroplasty in patients with a uterine septum and otherwise unexplained infertility. Int. J. Gynaecol. Obs. 2011, 113, 128–130. [Google Scholar] [CrossRef]
- Valle, R.F.; Ekpo, G.E. Hysteroscopic metroplasty for the septate uterus: Review and meta-analysis. J. Minim. Invasive Gynecol. 2013, 20, 22–42. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; An, J.; Su, Y.; Liu, C.; Lin, S.; Zhang, J.; Xie, X. Reproductive outcome of a complete septate uterus after hysteroscopic metroplasty. J. Int. Med. Res. 2020, 48, 300060519893836. [Google Scholar] [CrossRef] [PubMed]
- Ban-Frangez, H.; Tomazevic, T.; Virant-Klun, I.; Verdenik, I.; Ribic-Pucelj, M.; Bokal, E.V. The outcome of singleton pregnancies after IVF/ICSI in women before and after hysteroscopic resection of a uterine septum compared to normal controls. Eur. J. Obs. Gynecol. Reprod. Biol. 2009, 146, 184–187. [Google Scholar] [CrossRef]
- Chen, H.; Sun, P.; Zhang, N.; Lv, S.; Cao, Y.; Yan, L. Effects of Septum Resection for Secondary Infertility on Subsequent Reproductive Outcomes of in vitro Fertilization-Intracytoplasmic Sperm Injection. Front. Med. 2022, 9, 765827. [Google Scholar] [CrossRef]
- Tomazevic, T.; Ban-Frangez, H.; Virant-Klun, I.; Verdenik, I.; Pozlep, B.; Vrtacnik-Bokal, E. Septate, subseptate and arcuate uterus decrease pregnancy and live birth rates in IVF/ICSI. Reprod. Biomed. Online 2010, 21, 700–705. [Google Scholar] [CrossRef]
- Scoccia, B.; Demir, H.; Elter, K.; Scommegna, A. Successful medical management of post-hysteroscopic metroplasty bleeding with intravenous estrogen therapy: A report of two cases and review of the literature. J. Minim. Invasive Gynecol. 2009, 16, 639–642. [Google Scholar] [CrossRef]
- Lee, E.B.; Park, J.; Lim, H.K.; Kim, Y.I.; Jin, Y.; Lee, K.H. Complications of fluid overload during hysteroscopic surgery: Cardiomyopathy and epistaxis-A case report. Anesth. Pain Med. 2020, 15, 61–65. [Google Scholar] [CrossRef] [PubMed]
- De Franciscis, P.; Riemma, G.; Schiattarella, A.; Cobellis, L.; Colacurci, N.; Vitale, S.G.; Cianci, A.; Lohmeyer, F.M.; La Verde, M. Impact of Hysteroscopic Metroplasty on Reproductive Outcomes of Women with a Dysmorphic Uterus and Recurrent Miscarriages: A Systematic Review and Meta-Analysis. J. Gynecol. Obs. Hum. Reprod. 2020, 49, 101763. [Google Scholar] [CrossRef] [PubMed]
- Vigoureux, S.; Fernandez, H.; Capmas, P.; Levaillant, J.M.; Legendre, G. Assessment of Abdominal Ultrasound Guidance in Hysteroscopic Metroplasty. J. Minim. Invasive Gynecol. 2016, 23, 78–83. [Google Scholar] [CrossRef]
- Jansa, V.; Lagana, A.S.; Ferrari, F.; Ghezzi, F.; Burnik Papler, T.; Vrtacnik Bokal, E.; Ban Frangez, H. Uterine rupture in pregnancy after hysteroscopic septum resection: A 20-year retrospective analysis. Minim. Invasive Ther. Allied Technol. 2022, 31, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Agostini, A.; De Guibert, F.; Salari, K.; Crochet, P.; Bretelle, F.; Gamerre, M. Adverse obstetric outcomes at term after hysteroscopic metroplasty. J. Minim. Invasive Gynecol. 2009, 16, 454–457. [Google Scholar] [CrossRef]
- Miklavcic, J.; Lagana, A.S.; Premru Srsen, T.; Korosec, S.; Ban Frangez, H. Effect of hysteroscopic septum resection on preterm delivery rate in singleton pregnancies. Minim Invasive Ther. Allied Technol. 2021, 30, 377–383. [Google Scholar] [CrossRef]
- Moffat, R.; Bergsma, N.; Sartorius, G.; Raggi, A.; Guth, U.; De Geyter, C. Does prior hysteroscopy affect pregnancy outcome in primigravid infertile women? Am. J. Obs. Gynecol. 2014, 211, 130.e1–130.e6. [Google Scholar] [CrossRef]
- Shah, P.S.; Zao, J.; Knowledge Synthesis Group of Determinants of preterm. Induced termination of pregnancy and low birthweight and preterm birth: A systematic review and meta-analyses. BJOG 2009, 116, 1425–1442. [Google Scholar] [CrossRef]
- Baldwin, H.J.; Patterson, J.A.; Nippita, T.A.; Torvaldsen, S.; Ibiebele, I.; Simpson, J.M.; Ford, J.B. Antecedents of Abnormally Invasive Placenta in Primiparous Women: Risk Associated With Gynecologic Procedures. Obs. Gynecol. 2018, 131, 227–233. [Google Scholar] [CrossRef]
- Zhang, L.P.; Wang, M.; Shang, X.; Zhang, Q.; Yang, B.J.; Xu, Y.; Li, J.H.; Feng, L.M. The incidence of placenta related disease after the hysteroscopic adhesiolysis in patients with intrauterine adhesions. Taiwan J. Obs. Gynecol. 2020, 59, 575–579. [Google Scholar] [CrossRef]
- Mathiesen, E.; Hohenwalter, M.; Basir, Z.; Peterson, E. Placenta increta after hysteroscopic myomectomy. Obs. Gynecol. 2013, 122, 478–481. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Matsuzaki, S.; Matsuzaki, S.; Kakigano, A.; Kumasawa, K.; Ueda, Y.; Endo, M.; Kimura, T. Placenta accreta following hysteroscopic myomectomy. Clin. Case Rep. 2016, 4, 541–544. [Google Scholar] [CrossRef] [PubMed]
- Kenda Suster, N.; Gergolet, M. Does hysteroscopic metroplasty for septate uterus represent a risk factor for adverse outcome during pregnancy and labor? Gynecol. Surg. 2016, 13, 37–41. [Google Scholar] [CrossRef][Green Version]
- Feinberg, E.C.; Levens, E.D.; DeCherney, A.H. Infertility surgery is dead: Only the obituary remains? Fertil. Steril. 2008, 89, 232–236. [Google Scholar] [CrossRef]
- Cochrane, E.; Pando, C.; Kirschen, G.W.; Soucier, D.; Fuchs, A.; Garry, D.J. Assisted reproductive technologies (ART) and placental abnormalities. J. Perinat. Med. 2020, 48, 825–828. [Google Scholar] [CrossRef] [PubMed]
- Karami, M.; Jenabi, E.; Fereidooni, B. The association of placenta previa and assisted reproductive techniques: A meta-analysis. J. Matern. Fetal Neonatal Med. 2018, 31, 1940–1947. [Google Scholar] [CrossRef] [PubMed]
- Qin, J.; Liu, X.; Sheng, X.; Wang, H.; Gao, S. Assisted reproductive technology and the risk of pregnancy-related complications and adverse pregnancy outcomes in singleton pregnancies: A meta-analysis of cohort studies. Fertil. Steril. 2016, 105, 73–85.e6. [Google Scholar] [CrossRef]
- Jenabi, E.; Salimi, Z.; Ayubi, E.; Bashirian, S.; Salehi, A.M. The environmental risk factors prior to conception associated with placental abruption: An umbrella review. Syst. Rev. 2022, 11, 55. [Google Scholar] [CrossRef]
- Pavalagantharajah, S.; Villani, L.A.; D’Souza, R. Vasa previa and associated risk factors: A systematic review and meta-analysis. Am. J. Obs. Gynecol. MFM 2020, 2, 100117. [Google Scholar] [CrossRef]
- Fitzpatrick, K.E.; Sellers, S.; Spark, P.; Kurinczuk, J.J.; Brocklehurst, P.; Knight, M. Incidence and risk factors for placenta accreta/increta/percreta in the UK: A national case-control study. PLoS ONE 2012, 7, e52893. [Google Scholar] [CrossRef]
- Kyozuka, H.; Yamaguchi, A.; Suzuki, D.; Fujimori, K.; Hosoya, M.; Yasumura, S.; Yokoyama, T.; Sato, A.; Hashimoto, K.; Japan, E.; et al. Risk factors for placenta accreta spectrum: Findings from the Japan environment and Children’s study. BMC Pregnancy Childbirth 2019, 19, 447. [Google Scholar] [CrossRef]
- Perlman, N.C.; Carusi, D.A. Retained placenta after vaginal delivery: Risk factors and management. Int. J. Womens Health 2019, 11, 527–534. [Google Scholar] [CrossRef]
- Vitale, S.G.; Parry, J.P.; Carugno, J.; Cholkeri-Singh, A.; Della Corte, L.; Cianci, S.; Schiattarella, A.; Riemma, G.; De Franciscis, P. Surgical and Reproductive Outcomes after Hysteroscopic Removal of Retained Products of Conception: A Systematic Review and Meta-analysis. J. Minim. Invasive Gynecol. 2021, 28, 204–217. [Google Scholar] [CrossRef]
- Chan, Y.Y.; Jayaprakasan, K.; Tan, A.; Thornton, J.G.; Coomarasamy, A.; Raine-Fenning, N.J. Reproductive outcomes in women with congenital uterine anomalies: A systematic review. Ultrasound Obs. Gynecol 2011, 38, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.A.; Kim, H.S.; Kim, Y.H. Reproductive, Obstetric and Neonatal Outcomes in Women with Congenital Uterine Anomalies: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 4797. [Google Scholar] [CrossRef] [PubMed]
- Noventa, M.; Spagnol, G.; Marchetti, M.; Saccardi, C.; Bonaldo, G.; Lagana, A.S.; Cavallin, F.; Andrisani, A.; Ambrosini, G.; Vitale, S.G.; et al. Uterine Septum with or without Hysteroscopic Metroplasty: Impact on Fertility and Obstetrical Outcomes-A Systematic Review and Meta-Analysis of Observational Research. J. Clin. Med. 2022, 11, 3290. [Google Scholar] [CrossRef] [PubMed]
- Venetis, C.A.; Papadopoulos, S.P.; Campo, R.; Gordts, S.; Tarlatzis, B.C.; Grimbizis, G.F. Clinical implications of congenital uterine anomalies: A meta-analysis of comparative studies. Reprod. Biomed. Online 2014, 29, 665–683. [Google Scholar] [CrossRef]
- Rikken, J.F.W.; Kowalik, C.R.; Emanuel, M.H.; Bongers, M.Y.; Spinder, T.; Jansen, F.W.; Mulders, A.; Padmehr, R.; Clark, T.J.; van Vliet, H.A.; et al. Septum resection versus expectant management in women with a septate uterus: An international multicentre open-label randomized controlled trial. Hum. Reprod. 2021, 36, 1260–1267. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| HSD | without HSD | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|
| Conception | ||||||||
| Natural (A) | IVF/ICSI (B) | Natural (C) | IVF/ICSI (D) | AC | BD | AB | CD | |
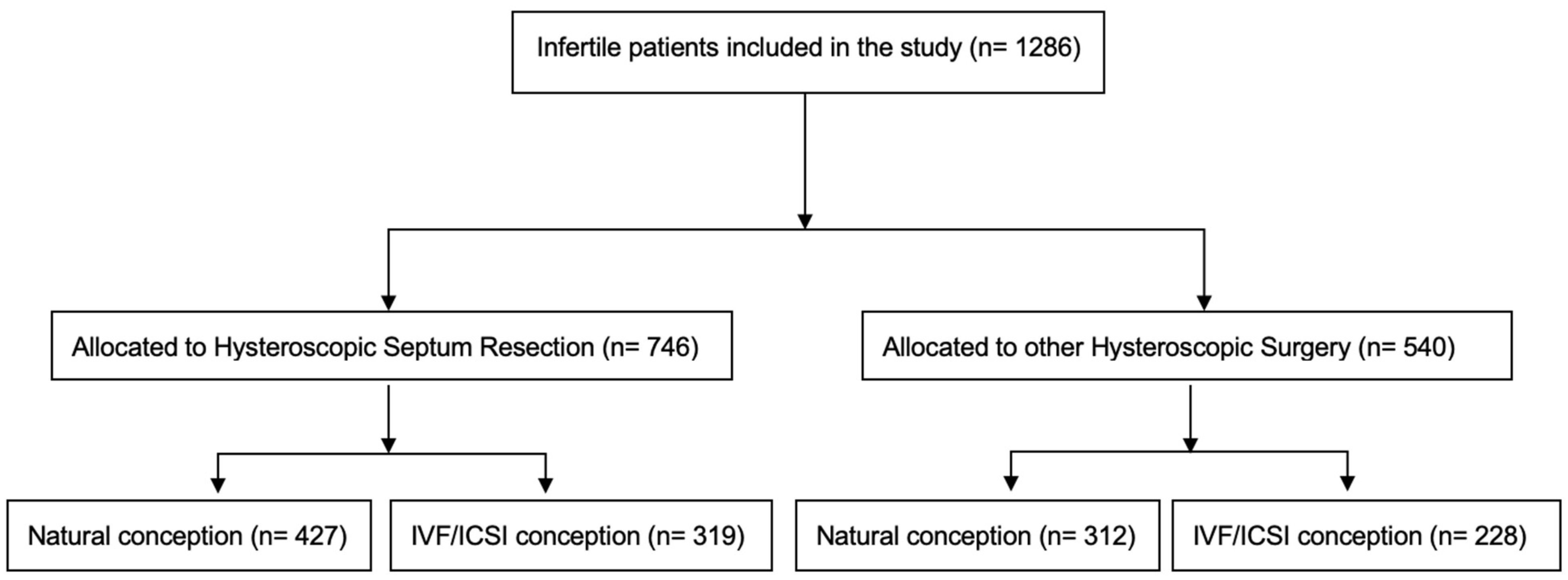
| Number of patients | 427 | 319 | 312 | 228 | ||||
| Mean age (mean years ± SD) | 30.84 ± 4.21 | 31.72 ± 4.39 | 30.68 ± 4.12 | 31.71 ± 3.70 | 1 | 1 | 0.024 * | 0.028 * |
| Primary vs. secondary infertility (%) | 285 vs. 142 (66.7% vs. 33.3%) | 225 vs. 94 (70.5% vs. 29.5%) | 210 vs. 102 (67.3% vs. 32.7%) | 165 vs. 63 (72.4% vs. 27.6%) | 0.872 | 0.640 | 0.271 | 0.207 |
| Previous early pregnancy losses cases (mean ± SD) | 0.438 ± 0.789 | 0.376 ± 0.720 | 0.311 ± 0.706 | 0.211 ± 0.522 | 0.016 * | 0.008 * | 1 | 0.788 |
| Previous ectopic pregnancies cases (mean ± SD) | 0.021 ± 0.144 | 0.056 ± 0.302 | 0.003 ± 0.057 | 0.039 ± 0.195 | 0.152 | 1 | 0.448 | 0.008 * |
| HSD | without HSD | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|
| Conception | ||||||||
| Natural (A) | IVF/ICSI (B) | Natural (C) | IVF/ICSI (D) | AC | BD | AB | CD | |
| Placental abruption | 8 (1.9%) | 2 (0.6%) | 4 (1.3%) | 2 (0.9%) | 0.7697 | 1 | 0.2020 | 1 |
| Placenta previa | 5 (1.2%) | 4 (1.3%) | 2 (0.6%) | 7 (3.1%) | 0.7050 | 0.2149 | 1 | 0.0401 * |
| Adherent placenta | 9 (2.1%) | 14 (4.4%) | 6 (1.9%) | 7 (3.1%) | 1 | 0.5034 | 0.0878 | 0.4083 |
| Incomplete placenta | 19 (4.4%) | 17 (5.3%) | 12 (3.8%) | 11 (4.8%) | 0.7151 | 0.8463 | 0.6074 | 0.6675 |
| Placental calcification | 14 (3.3%) | 9 (2.8%) | 10 (3.2%) | 4 (1.8%) | 1 | 0.5722 | 0.8318 | 0.4132 |
| Placental infarction | 4 (0.9%) | 5 (1.6%) | 1 (0.3%) | 1 (0.4%) | 0.4034 | 0.4086 | 0.5078 | 1 |
| PAS | 2 (0.5%) | 0 (0.0%) | 1 (0.3%) | 0 (0.0%) | 1 | 1 | 0.5098 | 1 |
| Vasa previa | 0 (0.0%) | 1 (0.3%) | 0 (0.0%) | 1 (0.4%) | 1 | 1 | 0.4276 | 0.4222 |
| Preeclampsia | 11 (2.5%) | 12 (3.7%) | 8 (2.6%) | 8 (3.5%) | 0.593 | 0.534 | 0.237 | 0.347 |
| No placental defect | 370 (86.7%) | 267 (83.7%) | 280 (89.7%) | 196 (86.0%) | 0.2104 | 0.5478 | 0.2949 | 0.1812 |
| HSD | without HSD | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|
| Conception | ||||||||
| Natural (A) | IVF/ICSI (B) | Natural (C) | IVF/ICSI (D) | AC | BD | AB | CD | |
| Mean gestation age (weeks ± SD) | 38.78 ± 2.451 | 38.34 ± 2.776 | 38.98 ± 1.847 | 38.38 ± 2.760 | 1 | 1 | 0.091 | 0.029 * |
| Birth weight (g ± SD) | 3256 ± 601 | 3219 ± 678 | 3352 ± 530 | 3241 ± 684 | 0.237 | 1 | 1 | 0.243 |
| APGAR after 1 min | 8.76 ± 1.011 | 8.70 ± 1.292 | 8.80 ± 1.026 | 8.75 ± 1.131 | 1 | 1 | 1 | 1 |
| APGAR after 5 min | 9.07 ± 0.854 | 9.04 ± 0.951 | 9.12 ± 0.859 | 9.09 ± 0.925 | 1 | 1 | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hajšek, P.; Riemma, G.; Korošec, S.; Laganà, A.S.; Chiantera, V.; Mikuš, M.; Ban Frangež, H. Does Hysteroscopic Dissection of Partial Uterine Septum Represent a Risk Factor for Placental Abnormalities in Subsequent Pregnancy Compared with Controls Undergoing Other Hysteroscopic Surgery? Results from a Large Case–Control Analysis. J. Clin. Med. 2023, 12, 177. https://doi.org/10.3390/jcm12010177
Hajšek P, Riemma G, Korošec S, Laganà AS, Chiantera V, Mikuš M, Ban Frangež H. Does Hysteroscopic Dissection of Partial Uterine Septum Represent a Risk Factor for Placental Abnormalities in Subsequent Pregnancy Compared with Controls Undergoing Other Hysteroscopic Surgery? Results from a Large Case–Control Analysis. Journal of Clinical Medicine. 2023; 12(1):177. https://doi.org/10.3390/jcm12010177
Chicago/Turabian StyleHajšek, Pia, Gaetano Riemma, Sara Korošec, Antonio Simone Laganà, Vito Chiantera, Mislav Mikuš, and Helena Ban Frangež. 2023. "Does Hysteroscopic Dissection of Partial Uterine Septum Represent a Risk Factor for Placental Abnormalities in Subsequent Pregnancy Compared with Controls Undergoing Other Hysteroscopic Surgery? Results from a Large Case–Control Analysis" Journal of Clinical Medicine 12, no. 1: 177. https://doi.org/10.3390/jcm12010177
APA StyleHajšek, P., Riemma, G., Korošec, S., Laganà, A. S., Chiantera, V., Mikuš, M., & Ban Frangež, H. (2023). Does Hysteroscopic Dissection of Partial Uterine Septum Represent a Risk Factor for Placental Abnormalities in Subsequent Pregnancy Compared with Controls Undergoing Other Hysteroscopic Surgery? Results from a Large Case–Control Analysis. Journal of Clinical Medicine, 12(1), 177. https://doi.org/10.3390/jcm12010177