
Effect of PCSK9 Inhibitors on Hemostasis in Patients with Isolated Hypercholesterolemia


Abstract
:1. Introduction
2. Materials and Methods
Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thim, T.; Hagensen, M.K.; Bentzon, J.F.; Falk, E. From vulnerable plaque to atherothrombosis. J. Intern. Med. 2008, 263, 506–516. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.B. Overview of hemostatic factors involved in atherosclerotic cardiovascular disease. Lipids 2005, 40, 1215–1220. [Google Scholar] [CrossRef] [PubMed]
- Kher, N.; Marsh, J.D. Pathobiology of atherosclerosis-a brief review. Semin. Thromb. Hemost. 2004, 30, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Paciullo, F.; Momi, S.; Gresele, P. PCSK9 in Haemostasis and Thrombosis: Possible Pleiotropic Effects of PCSK9 Inhibitors in Cardiovascular Prevention. Thromb. Haemost. 2019, 119, 359–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obermayer, G.; Afonyushkin, T.; Binder, C.J. Oxidized low-density lipoprotein in inflammation-driven thrombosis. J. Thromb. Haemost. 2018, 3, 418–428. [Google Scholar] [CrossRef] [Green Version]
- Ouweneel, A.B.; Van Eck, M. Lipoproteins as modulators of atherothrombosis: From endothelial function to primary and secondary coagulation. Vascul. Pharmacol. 2016, 82, 1–10. [Google Scholar] [CrossRef]
- Urban, D.; Pöss, J.; Böhm, M.; Laufs, U. Targeting the proprotein convertase subtilisin/kexin type 9 for the treatment of dyslipidemia and atherosclerosis. J. Am. Coll. Cardiol. 2013, 62, 1401–1408. [Google Scholar] [CrossRef] [Green Version]
- Pęczek, P.; Leśniewski, M.; Mazurek, T.; Szarpak, L.; Filipiak, K.J.; Gąsecka, A. Antiplatelet Effects of PCSK9 Inhibitors in Primary Hypercholesterolemia. Life 2021, 11, 466. [Google Scholar] [CrossRef]
- Martinelli, N.; Girelli, D.; Lunghi, B.; Pinotti, M.; Marchetti, G.; Malerba, G.; Pignatti, P.F.; Corrocher, R.; Olivieri, O.; Bernardi, F. Polymorphisms at LDLR locus may be associated with coronary artery disease through modulation of coagulation factor VIII activity and independently from lipid profile. Blood 2010, 116, 5688–5697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badimon, L.; Vilahur, G. Thrombosis formation on atherosclerotic lesions and plaque rupture. J. Intern. Med. 2014, 276, 618–632. [Google Scholar] [CrossRef]
- Tang, W.; Schwienbacher, C.; Lopez, L.M.; Ben-Shlomo, Y.; Oudot-Mellakh, T.; Johnson, A.D.; Samani, N.J.; Basu, S.; Gögele, M.; Davies, G.; et al. Genetic associations for activated partial thromboplastin time and prothrombin time, their gene expression profiles, and risk of coronary artery disease. Am. J. Hum. Genet. 2012, 91, 152–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Zhu, C.G.; Xu, R.X.; Li, S.; Guo, Y.L.; Sun, J.; Li, J.J. Relation of circulating PCSK9 concentration to fibrinogen in patients with stable coronary artery disease. J. Clin. Lipidol. 2014, 8, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Tosi, F.; Micaglio, R.; Sandri, M.; Castagna, A.; Minguzzi, D.; Stefanoni, F.; Chiariello, C.; Franzese, I.; Luciani, G.B.; Faggian, G.; et al. Increased plasma thrombin potential is associated with stable coronary artery disease: An angiographically-controlled study. Thromb. Res. 2017, 155, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart disease and stroke statistics--2012 update: A report from the American Heart Association. Circulation 2012, 125, e2–e220. [Google Scholar] [PubMed]
- Dahlbäck, B. Blood coagulation. Lancet 2000, 355, 1627–1632. [Google Scholar] [CrossRef]
- Puccini, M.; Landmesser, U.; Rauch, U. Pleiotropic Effects of PCSK9: Focus on Thrombosis and Haemostasis. Metabolism 2022, 12, 226. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; Harrington, R.A.; et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N. Engl. J. Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef]
- Basiak, M.; Kosowski, M.; Cyrnek, M.; Bułdak, Ł.; Maligłówka, M.; Machnik, G.; Okopień, B. Pleiotropic Effects of PCSK-9 Inhibitors. Int. J. Mol. Sci. 2021, 22, 3144. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Peng, J.; Liu, M.M.; Jin, J.L.; Cao, Y.X.; Guo, Y.L.; Wu, N.Q.; Zhu, C.G.; Dong, Q.; Sun, J.; Xu, R.X.; et al. Association of circulating PCSK9 concentration with cardiovascular metabolic markers and outcomes in stable coronary artery disease patients with or without diabetes: A prospective, observational cohort study. Cardiovasc. Diabetol. 2020, 19, 167. [Google Scholar] [CrossRef] [PubMed]
- Krysiak, R.; Okopień, B.; Herman, Z. Effects of HMG-CoA reductase inhibitors on coagulation and fibrinolysis processes. Drugs 2003, 63, 1821–1854. [Google Scholar] [CrossRef] [PubMed]
- Okopień, B.; Haberka, M.; Madej, A.; Belowski, D.; Labuzek, K.; Krysiak, R.; Zieliński, M.; Basiak, M.; Herman, Z.S. Extralipid effects of micronized fenofibrate in dyslipidemic patients. Pharmacol. Rep. 2006, 58, 729–735. [Google Scholar] [PubMed]
- O’Donoghue, M.L.; Fazio, S.; Giugliano, R.P.; Stroes, E.S.G.; Kanevsky, E.; Gouni-Berthold, I.; Im, K.; Pineda, A.L.; Wasserman, S.M.; Češka, R.; et al. Lipoprotein(a), PCSK9 Inhibition, and Cardiovascular Risk. Circulation 2019, 139, 1483–1492. [Google Scholar] [CrossRef]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bittner, V.A.; Diaz, R.; Goodman, S.G.; Kim, Y.U.; Jukema, J.W.; Pordy, R.; Roe, M.T.; et al. Peripheral Artery Disease and Venous Thromboembolic Events After Acute Coronary Syndrome: Role of Lipoprotein(a) and Modification by Alirocumab: Prespecified Analysis of the ODYSSEY OUTCOMES Randomized Clinical Trial. Circulation 2020, 141, 1608–1617. [Google Scholar] [CrossRef]
- Kaufman, R.J.; Pipe, S.W.; Tagliavacca, L.; Swaroop, M.; Moussalli, M. Biosynthesis, assembly and secretion of coagulation factor VIII. Blood Coagul. Fibrinolysis 1997, 8, 3–14. [Google Scholar]
- Siegler, J.E.; Samai, A.; Albright, K.C.; Boehme, A.K.; Martin-Schild, S. Factoring in Factor VIII with Acute Ischemic Stroke. Clin. Appl. Thromb. Hemost. 2015, 21, 597–602. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.X.; Liu, H.H.; Sun, D.; Jin, J.L.; Xu, R.X.; Guo, Y.L.; Wu, N.Q.; Zhu, C.G.; Li, S.; Zhang, Y.; et al. The different relations of PCSK9 and Lp(a) to the presence and severity of atherosclerotic lesions in patients with familial hypercholesterolemia. Atherosclerosis 2018, 277, 7–14. [Google Scholar] [CrossRef]
- Dwivedi, D.J.; Grin, P.M.; Khan, M.; Prat, A.; Zhou, J.; Fox-Robichaud, A.E.; Seidah, N.G.; Liaw, P.C. Differential Expression of PCSK9 Modulates Infection, Inflammation, and Coagulation in a Murine Model of Sepsis. Shock 2016, 46, 672–680. [Google Scholar] [CrossRef]
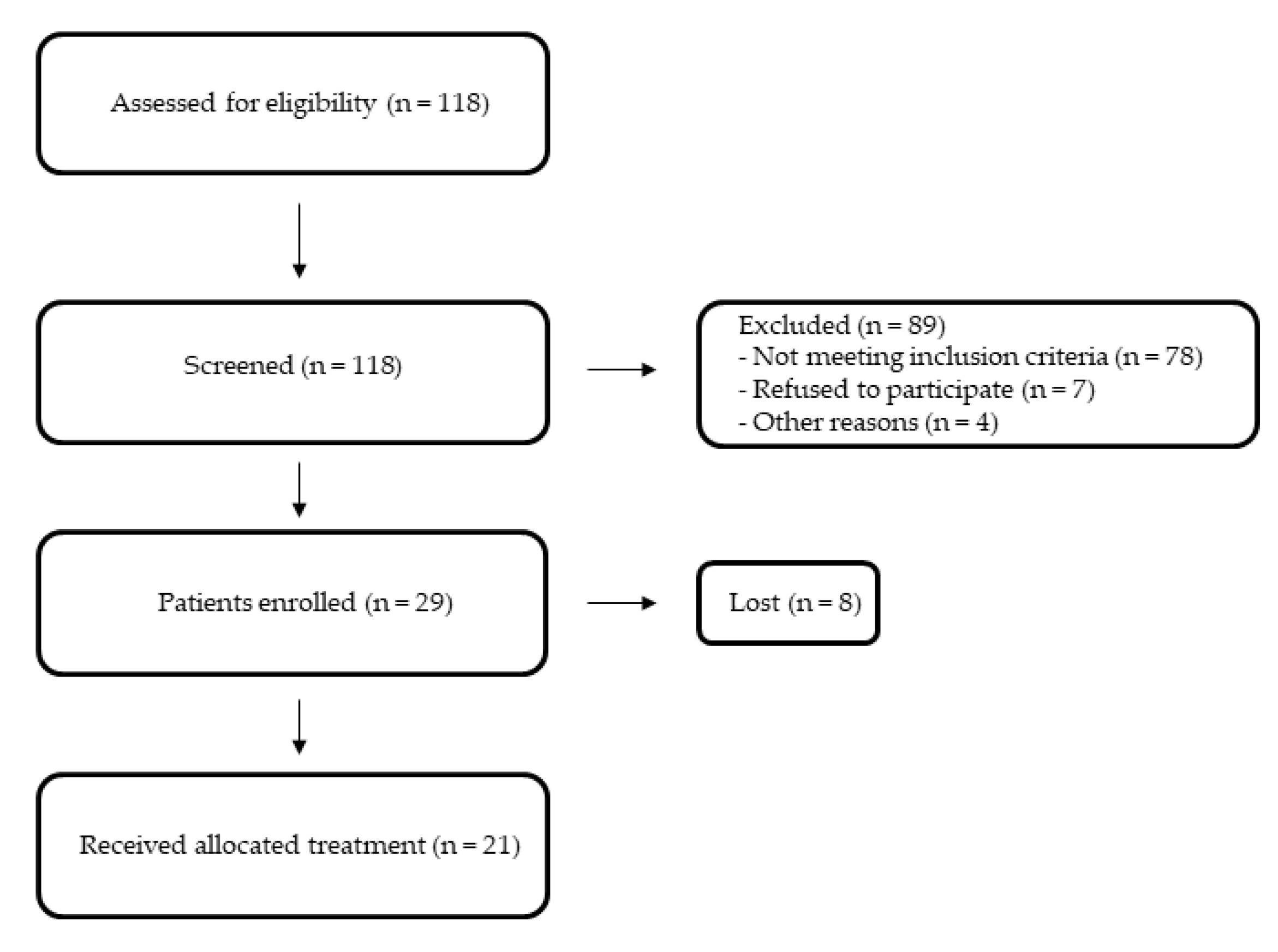

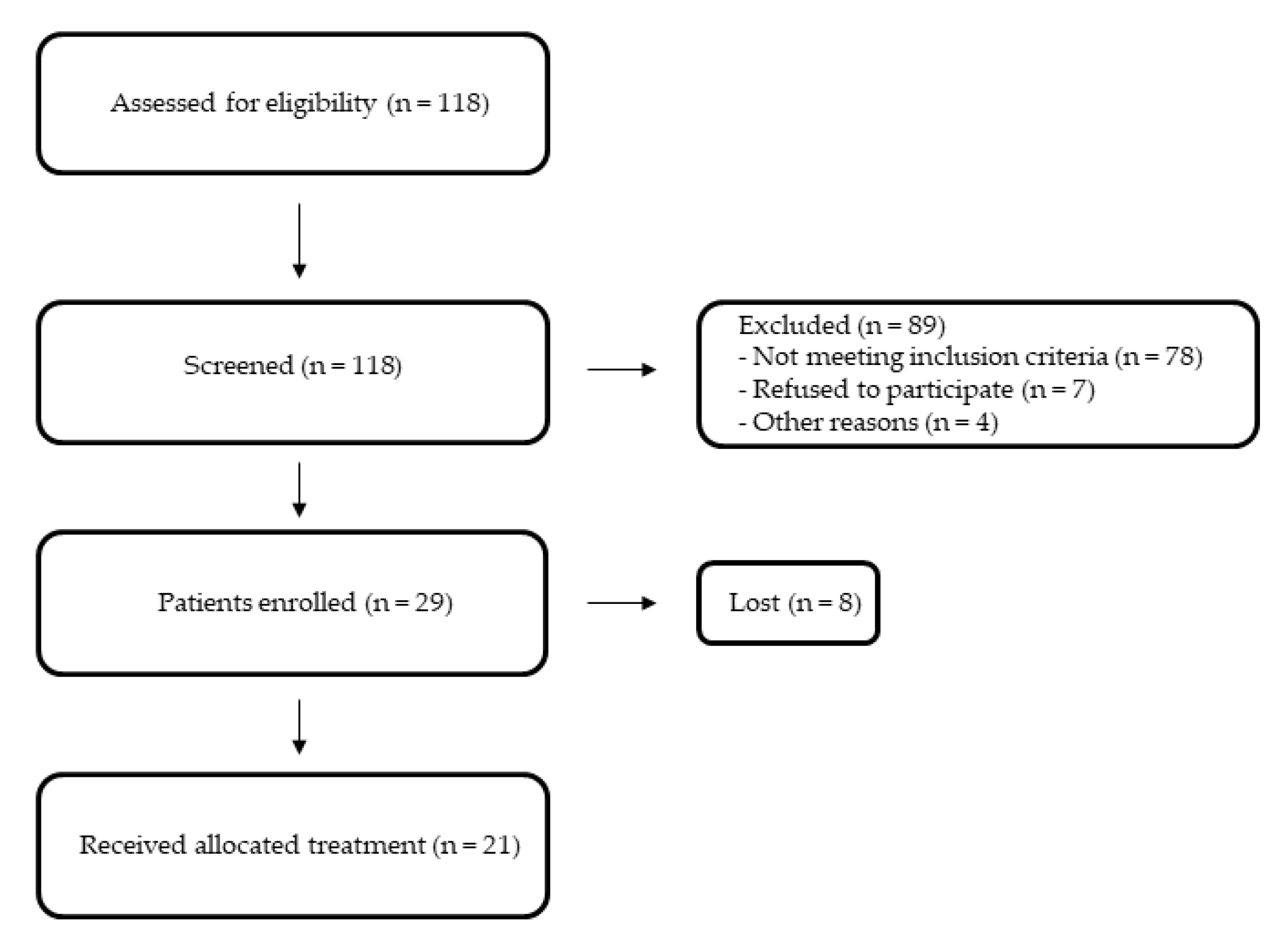{kind=link}
| Control Group | Study Group before Treatment | |
|---|---|---|
| Number of patients | 19 | 21 |
| Age, years | 45 ± 5 | 47 ± 6 |
| Women, % | 37 | 35 |
| BMI | 27.2 ± 2.7 | 28.1 ± 2.2 |
| WHO guidelines on physical activity, % | 84 | 81 |
| Smokers, % | 26 | 27 |
| Alcohol abuse | No | No |
| Systolic blood pressure, mmHg | 132 ± 6 | 134 ± 5 |
| Diastolic blood pressure, mmHg | 84 ± 4 | 83 ± 4 |
| INR | 0.84 ± 0.05 | 0.85 ± 0.06 |
| Total cholesterol, mg/dL | 160.2 ± 10.6 | 249.7 ± 12.9 |
| LDL cholesterol, mg/dL | 96.4 ± 8.7 | 181.0 ± 10.6 |
| HDL cholesterol, mg/dL | 48.1 ± 4.3 | 46.2 ± 4.2 |
| Triglycerides, mg/dL | 119.2 ± 9.6 | 121.6 ± 11.2 |
| Fasting glucose, mg/dL | 91 ± 4 | 92 ± 5 |
| Prothrombin time, s | 13.4 ± 1.3 | 14.2 ± 1.2 |
| Partial thromboplastin time, s | 31.1 ± 1.4 | 32.1 ± 1.7 |
| Fibrinogen, g/L | 3.2 ± 0.2 | 3.6 ± 0.5 |
| Factor VII activity, % | 141.3 ± 15.2 | 143.8 ± 16.7 |
| Von Willebrand factor, IU/dL | 116.1 ± 17.2 | 118.1 ± 16.0 |
| PAI-1 antigen, ng/mL | 72.3 ± 15.2 | 74.9 ± 13.9 |
| Variable | Control Group (Λ%) | Study Group (Λ%) | |
|---|---|---|---|
| Total cholesterol, mg/dL | Baseline After 90 days | 160.2 ± 10.6 157.1 ± 10.2 (−2) | 249.7 ± 12.9 152.4 ± 10.2 (−39) ***,### |
| LDL cholesterol, mg/dL | Baseline After 90 days | 96.4 ± 8.7 95.3 ± 8.1 (−1) | 181.0 ± 10.6 108.3 ± 8.4 (−40) ***,### |
| HDL cholesterol, mg/dL | Baseline After 90 days | 48.1 ± 4.3 49.1 ± 4.2 (2) | 46.2 ± 4.2 48.2 ± 4.3 (4) |
| Triglycerides, mg/dL | Baseline After 90 days | 119.2 ± 9.6 119.8 ± 10.2 (1) | 121.6 ± 11.2 109.2 ± 9.4 (−10) |
| Fasting glucose, mg/dL | Baseline After 90 days | 91 ± 4 92 ± 5 (1) | 92 ± 5 90 ± 4 (−2) |
| Prothrombin time, s | Baseline After 90 days | 13.4 ± 1.3 13.8 ± 1.4 (3) | 14.2 ± 1.2 16.4 ± 0.7 (15) |
| Partial thromboplastin time, s | Baseline After 90 days | 31.1 ± 1.4 31.8 ± 1.6 (2) | 32.1 ± 1.7 36.6 ± 1.4 (14) |
| Fibrinogen, g/L | Baseline After 90 days | 3.2 ± 0.2 3.5 ± 0.3 (9) | 3.6 ± 0.5 2.9 ± 0.4 (−20) **,# |
| Factor VII activity, % | Baseline After 90 days | 141.3 ± 15.2 142.2 ± 15.3 (1) | 143.8 ± 16.7 114.5 ± 14.1 (−20) **,## |
| Von Willebrand factor, IU/dL | Baseline After 90 days | 116.1 ± 17.2 120.2 ± 13.2 (4) | 118.1 ± 16.0 96.8 ± 11.4 (−18) # |
| PAI-1 antigen, ng/mL | Baseline After 90 days | 72.3 ± 15.2 74.4 ± 12.8 (3) | 74.9 ± 13.9 52.8 ± 9.1 (−30) ***,### |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basiak, M.; Hachula, M.; Kosowski, M.; Okopien, B. Effect of PCSK9 Inhibitors on Hemostasis in Patients with Isolated Hypercholesterolemia. J. Clin. Med. 2022, 11, 2542. https://doi.org/10.3390/jcm11092542
Basiak M, Hachula M, Kosowski M, Okopien B. Effect of PCSK9 Inhibitors on Hemostasis in Patients with Isolated Hypercholesterolemia. Journal of Clinical Medicine. 2022; 11(9):2542. https://doi.org/10.3390/jcm11092542
Chicago/Turabian StyleBasiak, Marcin, Marcin Hachula, Michal Kosowski, and Boguslaw Okopien. 2022. "Effect of PCSK9 Inhibitors on Hemostasis in Patients with Isolated Hypercholesterolemia" Journal of Clinical Medicine 11, no. 9: 2542. https://doi.org/10.3390/jcm11092542
APA StyleBasiak, M., Hachula, M., Kosowski, M., & Okopien, B. (2022). Effect of PCSK9 Inhibitors on Hemostasis in Patients with Isolated Hypercholesterolemia. Journal of Clinical Medicine, 11(9), 2542. https://doi.org/10.3390/jcm11092542