
Initial Experience with Left Bundle Branch Area Pacing with Conventional Stylet-Driven Extendable Screw-In Leads and New Pre-Shaped Delivery Sheaths

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
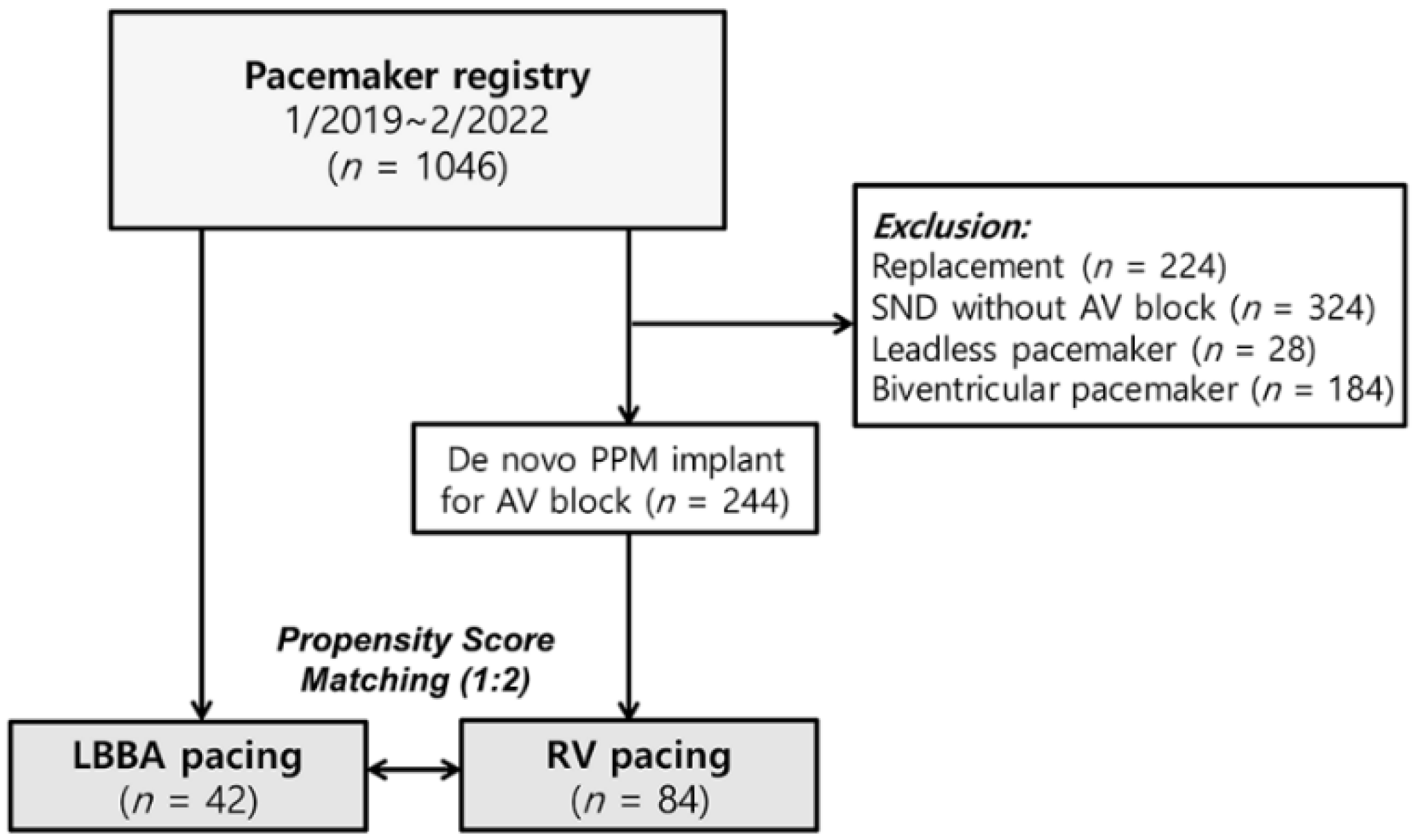
2.1. Patient Population
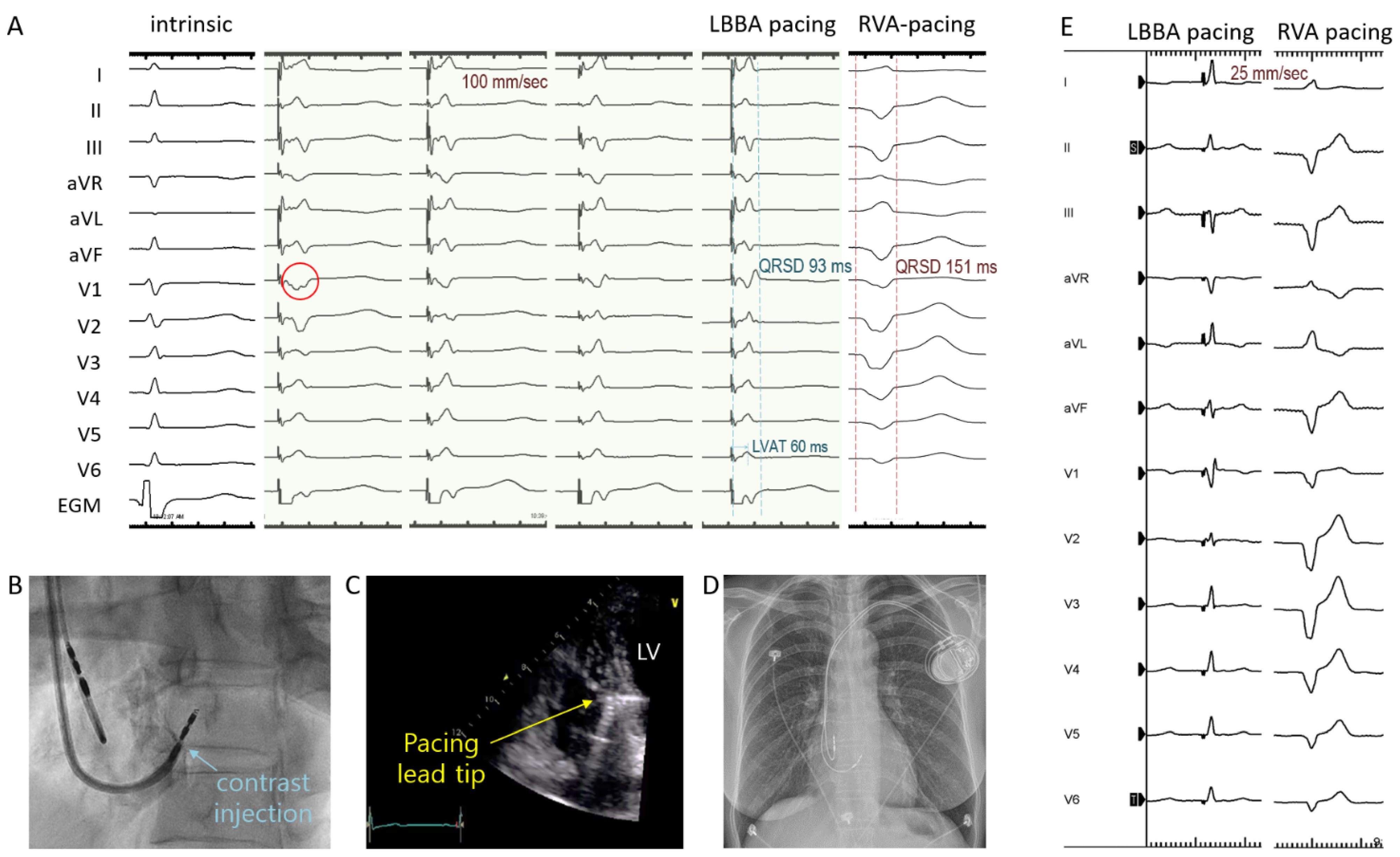
2.2. LBBAp Procedures
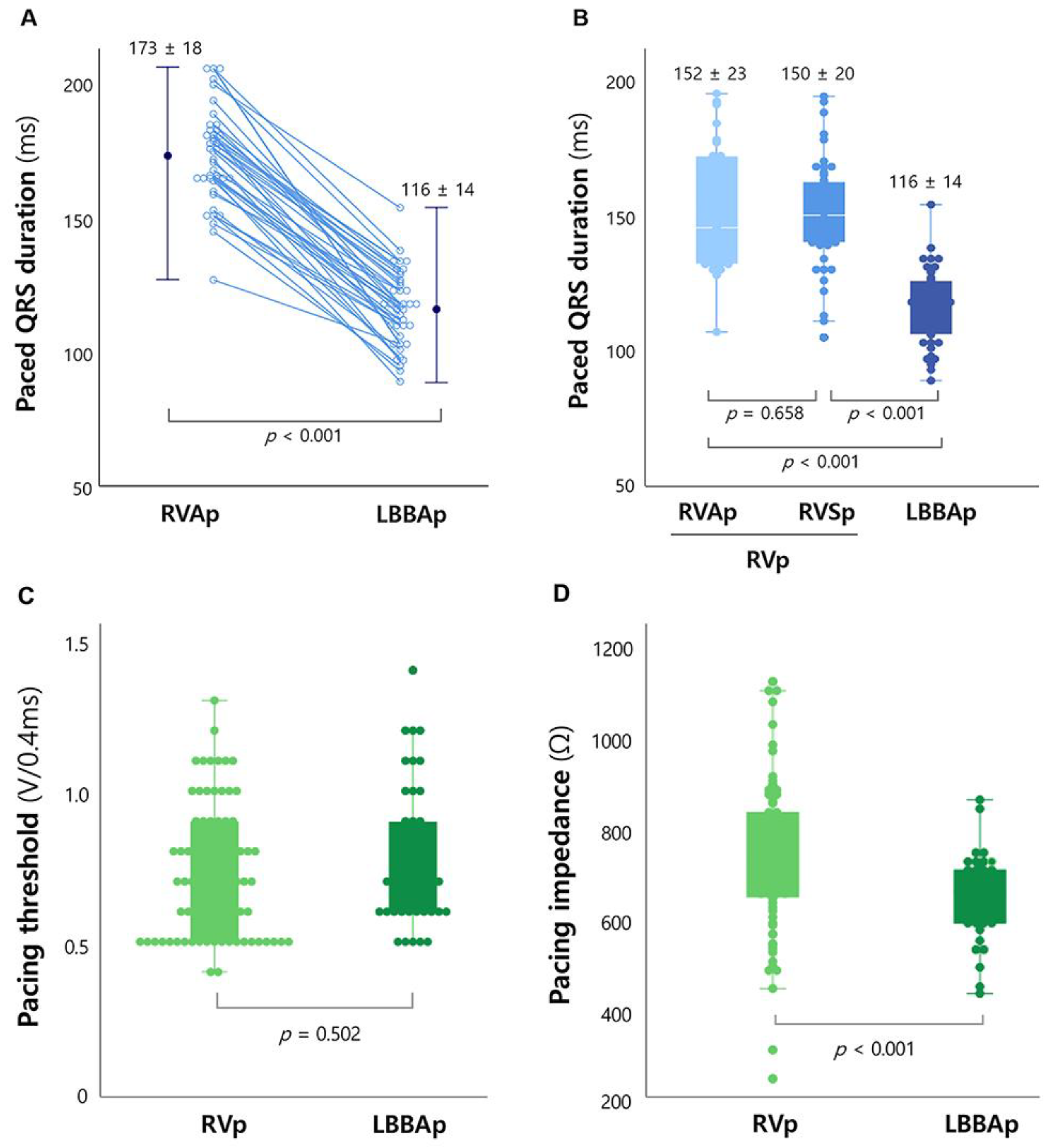
2.3. Measurement of Paced-QRS Duration and Pacing-Related Variables
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
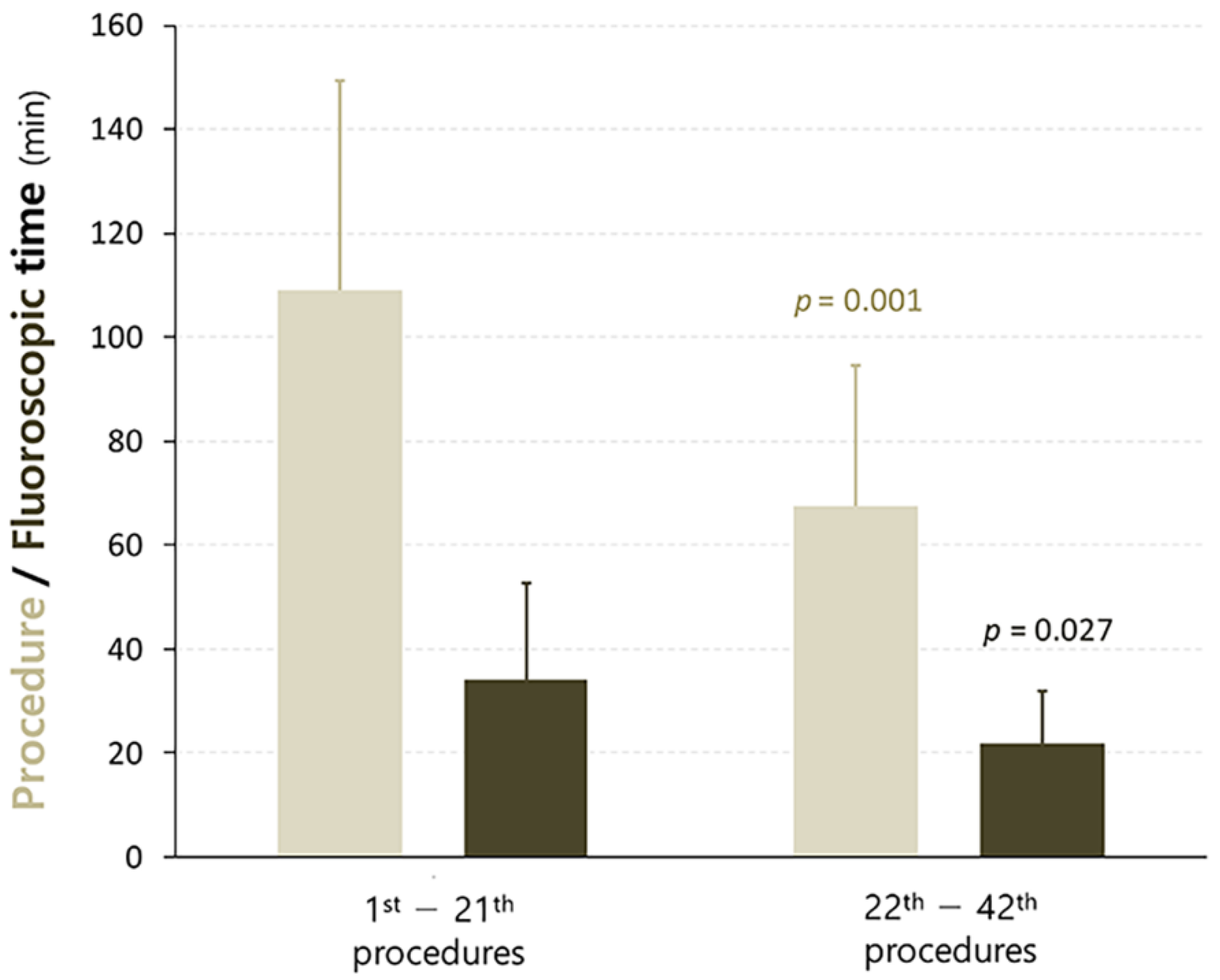
3.2. Acute Procedural and Short-Term Follow-Up Outcomes in the LBBAp Group
3.3. Comparison of Acute Outcomes between the LBBAp and RVp Groups
4. Discussion
4.1. Main Findings
4.2. Efficacy and Safety of LBBAp Using SDES Leads and New Fixed Curve Delivery Sheath
4.3. Efficacy of Physiological Pacing Using the New Implant Approach
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cho, S.W.; Gwag, H.B.; Hwang, J.K.; Chun, K.J.; Park, K.M.; On, Y.K.; Kim, J.S.; Park, S.J. Clinical features, predictors, and long-term prognosis of pacing-induced cardiomyopathy. Eur. J. Heart Fail. 2019, 21, 643–651. [Google Scholar] [CrossRef]
- Wilkoff, B.L.; Cook, J.R.; Epstein, A.E.; Greene, H.L.; Hallstrom, A.P.; Hsia, H.; Kutalek, S.P.; Sharma, A. Dual-chamber pacing or ventricular backup pacing in patients with an implantable defibrillator: The Dual Chamber and VVI Implantable Defibrillator (DAVID) Trial. JAMA 2002, 288, 3115–3123. [Google Scholar]
- Kusumoto, F.M.; Schoenfeld, M.H.; Barrett, C.; Edgerton, J.R.; Ellenbogen, K.A.; Gold, M.R.; Goldschlager, N.F.; Hamilton, R.M.; Joglar, J.A.; Kim, R.J.; et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients with Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2019, 140, e382–e482. [Google Scholar]
- Bhatt, A.G.; Musat, D.L.; Milstein, N.; Pimienta, J.; Flynn, L.; Sichrovsky, T.; Preminger, M.W.; Mittal, S. The Efficacy of His Bundle Pacing: Lessons Learned from Implementation for the First Time at an Experienced Electrophysiology Center. JACC Clin. Electrophysiol. 2018, 4, 1397–1406. [Google Scholar] [CrossRef]
- Lustgarten, D.L.; Sharma, P.S.; Vijayaraman, P. Troubleshooting and programming considerations for His bundle pacing. Heart Rhythm 2019, 16, 654–662. [Google Scholar] [CrossRef]
- Huang, W.; Su, L.; Wu, S.; Xu, L.; Xiao, F.; Zhou, X.; Ellenbogen, K.A. A Novel Pacing Strategy with Low and Stable Output: Pacing the Left Bundle Branch Immediately beyond the Conduction Block. Can. J. Cardiol. 2017, 33, 1736.e1–1736.e3. [Google Scholar] [CrossRef]
- Padala, S.K.; Master, V.M.; Terricabras, M.; Chiocchini, A.; Garg, A.; Kron, J.; Shepard, R.; Kalahasty, G.; Azizi, Z.; Tsang, B.; et al. Initial Experience, Safety, and Feasibility of Left Bundle Branch Area Pacing: A Multicenter Prospective Study. JACC Clin. Electrophysiol. 2020, 6, 1773–1782. [Google Scholar] [CrossRef]
- Qian, Z.; Qiu, Y.; Wang, Y.; Jiang, Z.; Wu, H.; Hou, X.; Zou, J. Lead performance and clinical outcomes of patients with permanent His-Purkinje system pacing: A single-centre experience. Europace 2020, 22, ii45–ii53. [Google Scholar] [CrossRef]
- Su, L.; Wang, S.; Wu, S.; Xu, L.; Huang, Z.; Chen, X.; Zheng, R.; Jiang, L.; Ellenbogen, K.A.; Whinnett, Z.I.; et al. Long-Term Safety and Feasibility of Left Bundle Branch Pacing in a Large Single-Center Study. Circ. Arrhythm. Electrophysiol. 2021, 14, e009261. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Ponnusamy, S.; Cano, Ó.; Sharma, P.S.; Naperkowski, A.; Subsposh, F.A.; Moskal, P.; Bednarek, A.; Dal Forno, A.R.; Young, W.; et al. Left Bundle Branch Area Pacing for Cardiac Resynchronization Therapy: Results from the International LBBAP Collaborative Study Group. JACC Clin. Electrophysiol. 2021, 7, 135–147. [Google Scholar] [CrossRef]
- Wang, J.; Liang, Y.; Wang, W.; Chen, X.; Bai, J.; Chen, H.; Su, Y.; Chen, R.; Ge, J. Left bundle branch area pacing is superior to right ventricular septum pacing concerning depolarization-repolarization reserve. J. Cardiovasc. Electrophysiol. 2020, 31, 313–322. [Google Scholar] [CrossRef]
- Padala, S.K.; Ellenbogen, K.A. Left bundle branch pacing is the best approach to physiological pacing. Heart Rhythm O2 2020, 1, 59–67. [Google Scholar] [CrossRef]
- Gillis, K.; O’Neill, L.; Wielandts, J.Y.; Hilfiker, G.; Vlase, A.; Knecht, S.; Duytschaever, M.; Tavernier, R.; le Polain de Waroux, J.B. Left bundle branch area pacing guided by continuous uninterrupted monitoring of unipolar pacing characteristics. J. Cardiovasc. Electrophysiol. 2022, 33, 299–307. [Google Scholar] [CrossRef]
- De Pooter, J.; Calle, S.; Timmermans, F.; Van Heuverswyn, F. Left bundle branch area pacing using stylet-driven pacing leads with a new delivery sheath: A comparison with lumen-less leads. J. Cardiovasc. Electrophysiol. 2021, 32, 439–448. [Google Scholar] [CrossRef]
- le Polain de Waroux, J.B.; Wielandts, J.Y.; Gillis, K.; Hilfiker, G.; Sorgente, A.; Capulzini, L.; Geerts, B.; Knecht, S.; Duytschaever, M.; Tavernier, R. Repositioning and extraction of stylet-driven pacing leads with extendable helix used for left bundle branch area pacing. J. Cardiovasc. Electrophysiol. 2021, 32, 1464–1466. [Google Scholar] [CrossRef]
- Huang, W.; Chen, X.; Su, L.; Wu, S.; Xia, X.; Vijayaraman, P. A beginner’s guide to permanent left bundle branch pacing. Heart Rhythm 2019, 16, 1791–1796. [Google Scholar] [CrossRef] [Green Version]
- Jiang, H.; Hou, X.; Qian, Z.; Wang, Y.; Tang, L.; Qiu, Y.; Jiang, Z.; Chen, X.; Li, K.; Zou, J. A novel 9-partition method using fluoroscopic images for guiding left bundle branch pacing. Heart Rhythm 2020, 17, 1759–1767. [Google Scholar] [CrossRef]
- Zanon, F.; Marcantoni, L.; Pastore, G.; Baracca, E. Left bundle branch pacing by standard stylet-driven lead: Preliminary experience of two case reports. HeartRhythm Case Rep. 2020, 6, 614–617. [Google Scholar] [CrossRef]
- Curila, K.; Jurak, P.; Jastrzebski, M.; Prinzen, F.; Waldauf, P.; Halamek, J.; Vernooy, K.; Smisek, R.; Karch, J.; Plesinger, F.; et al. Left bundle branch pacing compared to left ventricular septal myocardial pacing increases interventricular dyssynchrony but accelerates left ventricular lateral wall depolarization. Heart Rhythm 2021, 18, 1281–1289. [Google Scholar] [CrossRef]
- Heckman, L.I.B.; Luermans, J.; Curila, K.; Van Stipdonk, A.M.W.; Westra, S.; Smisek, R.; Prinzen, F.W.; Vernooy, K. Comparing Ventricular Synchrony in Left Bundle Branch and Left Ventricular Septal Pacing in Pacemaker Patients. J. Clin. Med. 2021, 10, 822. [Google Scholar] [CrossRef]
- Arnold, A.D.; Whinnett, Z.I.; Vijayaraman, P. His-Purkinje Conduction System Pacing: State of the Art in 2020. Arrhythm. Electrophysiol. Rev. 2020, 9, 136–145. [Google Scholar]
- Zingarini, G.; Notaristefano, F.; Spighi, L.; Bagliani, G.; Cavallini, C. Permanent His bundle pacing using a new tridimensional delivery sheath and a standard active fixation pacing lead: The telescopic technique. J. Cardiovasc. Electrophysiol. 2021, 32, 449–457. [Google Scholar] [CrossRef]
- Elizari, M.V. The normal variants in the left bundle branch system. J. Electrocardiol. 2017, 50, 389–399. [Google Scholar] [CrossRef]
- Kim, J.H.; Kang, K.W.; Chin, J.Y.; Kim, T.S.; Park, J.H.; Choi, Y.J. Major determinant of the occurrence of pacing-induced cardiomyopathy in complete atrioventricular block: A multicentre, retrospective analysis over a 15-year period in South Korea. BMJ Open 2018, 8, e019048. [Google Scholar] [CrossRef]
- Ng, A.C.; Allman, C.; Vidaic, J.; Tie, H.; Hopkins, A.P.; Leung, D.Y. Long-term impact of right ventricular septal versus apical pacing on left ventricular synchrony and function in patients with second- or third-degree heart block. Am. J. Cardiol. 2009, 103, 1096–1101. [Google Scholar] [CrossRef]
- Stambler, B.S.; Ellenbogen, K.; Zhang, X.; Porter, T.R.; Xie, F.; Malik, R.; Small, R.; Burke, M.; Kaplan, A.; Nair, L.; et al. Right ventricular outflow versus apical pacing in pacemaker patients with congestive heart failure and atrial fibrillation. J. Cardiovasc. Electrophysiol. 2003, 14, 1180–1186. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LBBA Pacing (n = 42) | Non-LBBA Pacing (n = 84) | p Value | |
|---|---|---|---|
| Demographics | |||
| Age (years) | 71 ± 16 | 69 ± 15 | 0.232 |
| Male | 22 (52) | 45 (54) | 0.900 |
| Height | 2.54 ± 0.29 | 2.58 ± 0.33 | 0.475 |
| BSA (m2) | 1.62 ± 0.17 | 1.65 ± 0.19 | 0.504 |
| Medical history | |||
| Diabetes mellitus | 15 (36) | 30 (36) | 1.000 |
| Hypertension | 20 (48) | 43 (51) | 0.705 |
| Heart failure | 10 (24) | 9 (11) | 0.053 |
| Myocardial infarction | 1 (2) | 0 (0) | 0.333 |
| Previous surgery/intervention | 6 (14) | 11 (13) | 0.854 |
| Chronic kidney disease | 5 (12) | 5 (6) | 0.244 |
| Echo- and Electrocardiographic variables | |||
| LVEF (%) | 62 ± 9 | 63 ± 7 | 0.436 |
| LVEDD (mm) | 52 ± 6 | 51 ± 5 | 0.932 |
| AF/AFL | 9 (21) | 13 (16) | 0.407 |
| Pacemaker-related variables | |||
| Indication of pacing | AVB, 38 (90) | AVB, 84 (100) | |
| SSS, 4 (10) | SSS, 0 (0) | ||
| Pacing location | LBBA, 42 (100) | RV apex, 31 (37) | |
| RV septum *, 53 (63) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byeon, K.; Kim, H.R.; Park, S.-J.; Park, Y.J.; Choi, J.-H.; Kim, J.Y.; Park, K.-M.; On, Y.K.; Kim, J.S. Initial Experience with Left Bundle Branch Area Pacing with Conventional Stylet-Driven Extendable Screw-In Leads and New Pre-Shaped Delivery Sheaths. J. Clin. Med. 2022, 11, 2483. https://doi.org/10.3390/jcm11092483
Byeon K, Kim HR, Park S-J, Park YJ, Choi J-H, Kim JY, Park K-M, On YK, Kim JS. Initial Experience with Left Bundle Branch Area Pacing with Conventional Stylet-Driven Extendable Screw-In Leads and New Pre-Shaped Delivery Sheaths. Journal of Clinical Medicine. 2022; 11(9):2483. https://doi.org/10.3390/jcm11092483
Chicago/Turabian StyleByeon, Kyeongmin, Hye Ree Kim, Seung-Jung Park, Young Jun Park, Ji-Hoon Choi, Ju Youn Kim, Kyoung-Min Park, Young Keun On, and June Soo Kim. 2022. "Initial Experience with Left Bundle Branch Area Pacing with Conventional Stylet-Driven Extendable Screw-In Leads and New Pre-Shaped Delivery Sheaths" Journal of Clinical Medicine 11, no. 9: 2483. https://doi.org/10.3390/jcm11092483
APA StyleByeon, K., Kim, H. R., Park, S.-J., Park, Y. J., Choi, J.-H., Kim, J. Y., Park, K.-M., On, Y. K., & Kim, J. S. (2022). Initial Experience with Left Bundle Branch Area Pacing with Conventional Stylet-Driven Extendable Screw-In Leads and New Pre-Shaped Delivery Sheaths. Journal of Clinical Medicine, 11(9), 2483. https://doi.org/10.3390/jcm11092483