
Three Clinical Clusters Identified through Hierarchical Cluster Analysis Using Initial Laboratory Findings in Korean Patients with Systemic Lupus Erythematosus

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
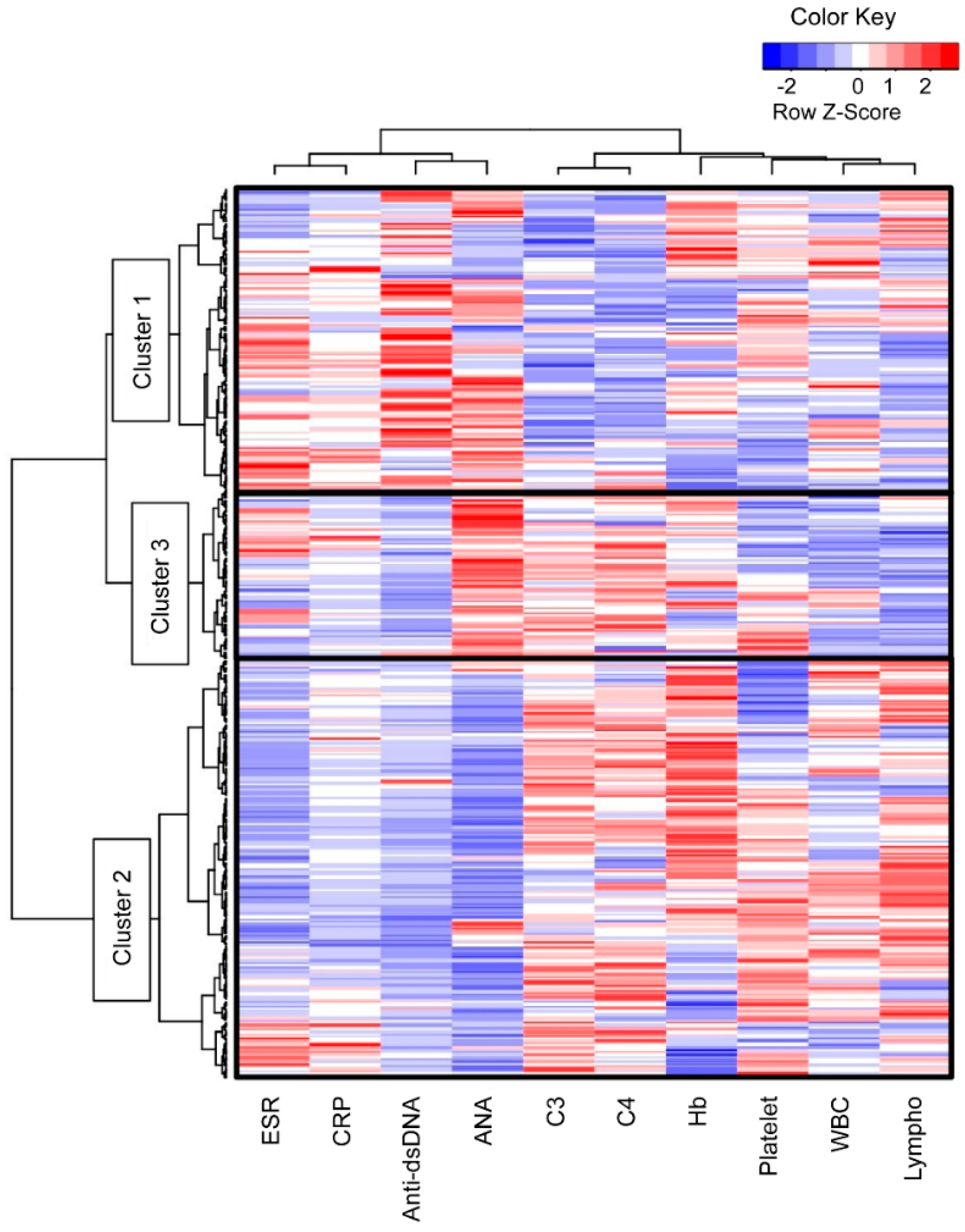
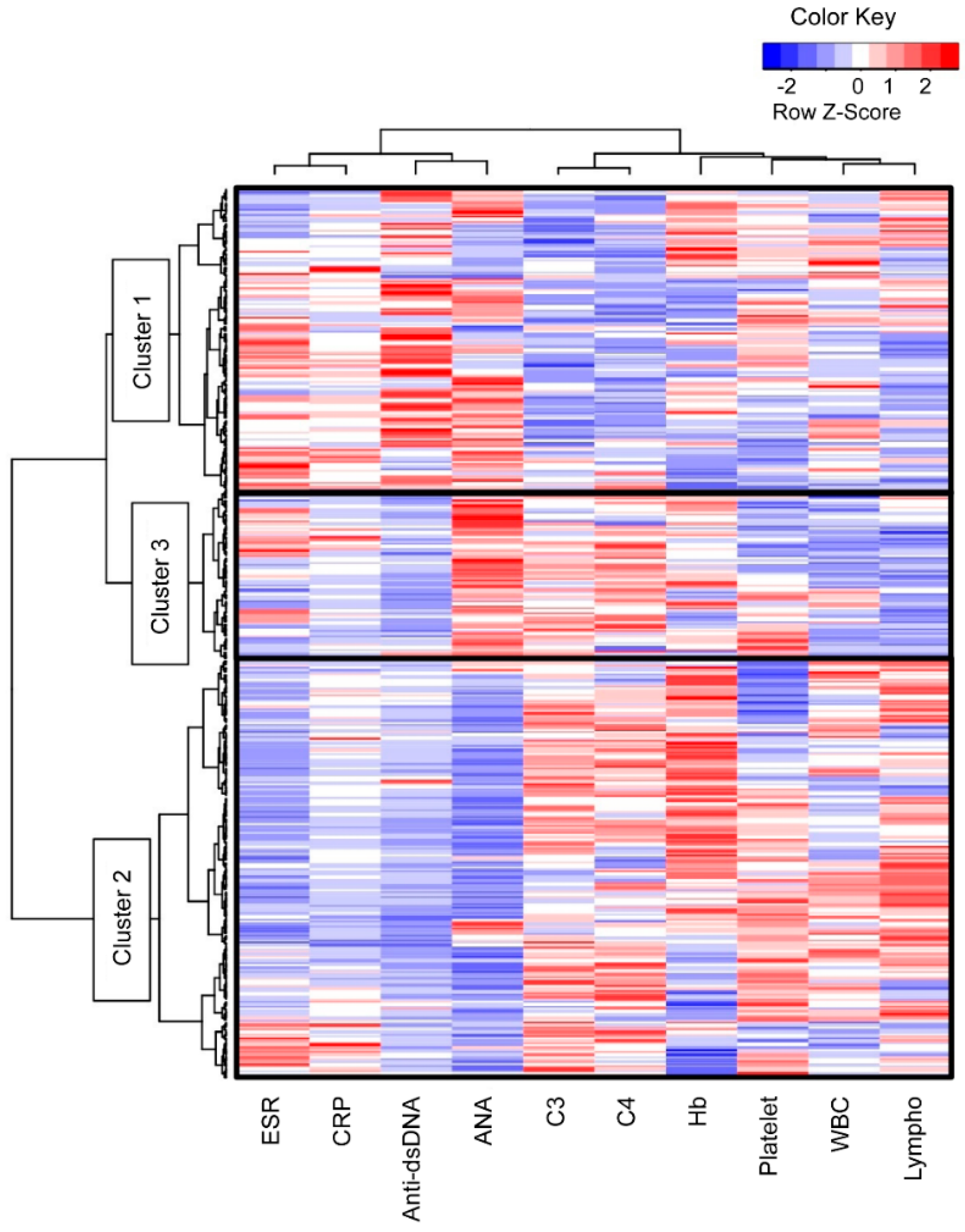
3.1. Three Clusters with Different Characteristics Were Identified among the Patients with SLE
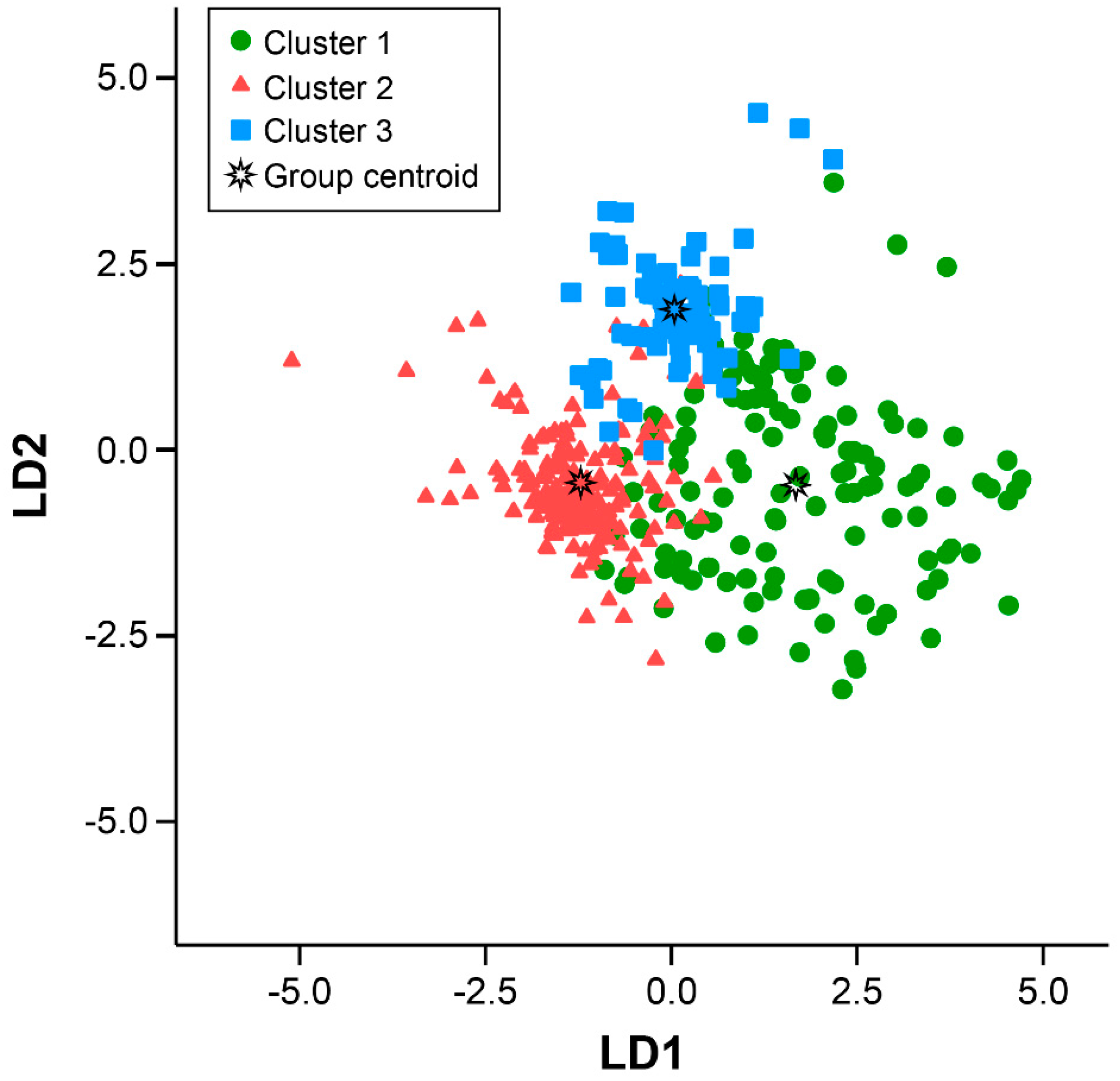
3.2. Three Clusters Were Separated with Significant Statistical Power
3.3. Each Cluster Showed Different Manifestations during Follow-Up
3.4. Mortality and Renal Damage within 171 Months were Not Different between the Clusters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lisnevskaia, L.; Murphy, G.; Isenberg, D. Systemic lupus erythematosus. Lancet 2014, 384, 1878–1888. [Google Scholar] [CrossRef]
- Kamen, D.L.; Zollars, E.S. Corticosteroids in lupus nephritis and central nervous system lupus. Rheum. Dis. Clin. N. Am. 2016, 42, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Tarr, T.; Papp, G.; Nagy, N.; Cserép, E.; Zeher, M. Chronic high-dose glucocorticoid therapy triggers the development of chronic organ damage and worsens disease outcome in systemic lupus erythematosus. Clin. Rheumatol. 2017, 36, 327–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moghaddam, B.; Marozoff, S.; Li, L.; Sayre, E.C.; Zubieta, J.A. All-cause and Cause-specific Mortality in Systemic Lupus Erythematosus: A Population-based Study. Rheumatology 2021, 61, 367–376. [Google Scholar] [CrossRef]
- Tselios, K.; Gladman, D.D.; Sheane, B.J.; Su, J.; Urowitz, M. All-cause, cause-specific and age-specific standardised mortality ratios of patients with systemic lupus erythematosus in Ontario, Canada over 43 years (1971–2013). Ann. Rheum. Dis. 2019, 78, 802–806. [Google Scholar] [CrossRef] [PubMed]
- Legge, A.; Doucette, S.; Hanly, J.G. Predictors of organ damage progression and effect on health-related quality of life in systemic lupus erythematosus. J. Rheumatol. 2016, 43, 1050–1056. [Google Scholar] [CrossRef]
- Alarcón, G.S.; McGwin, G., Jr.; Bastian, H.M.; Roseman, J.; Lisse, J.; Fessler, B.J.; Friedman, A.W.; Reveille, J.D. Systemic lupus erythematosus in three ethnic groups. VII [correction of VIII]. Predictors of early mortality in the LUMINA cohort. LUMINA Study Group. Arthritis Rheum. 2001, 45, 191–202. [Google Scholar] [CrossRef]
- Pimentel-Quiroz, V.R.; Ugarte-Gil, M.F.; Harvey, G.; Wojdyla, D.; Pons-Estel, G.; Quintana, R.; Esposto, A.; García, M.A.; Catoggio, L.J.; Cardiel, M.H.; et al. Factors predictive of serious infections over time in systemic lupus erythematosus patients: Data from a multi-ethnic, multi-national, Latin American lupus cohort. Lupus 2019, 28, 1101–1110. [Google Scholar] [CrossRef] [PubMed]
- McMahon, M.; Skaggs, B. Pathogenesis and treatment of atherosclerosis in lupus. Rheum. Dis. Clin. N. Am. 2014, 40, 475–495. [Google Scholar] [CrossRef]
- Thanou, A.; Jupe, E.; Purushothaman, M.; Niewold, T.B.; Munroe, M.E. Clinical disease activity and flare in SLE: Current concepts and novel biomarkers. J. Autoimmun. 2021, 119, 102615. [Google Scholar] [CrossRef] [PubMed]
- Ceccarelli, F.; Perricone, C.; Massaro, L.; Cipriano, E.; Alessandri, C.; Spinelli, F.R.; Valesini, G.; Conti, F. Assessment of disease activity in systemic lupus erythematosus: Lights and shadows. Autoimmun. Rev. 2015, 14, 601–608. [Google Scholar] [CrossRef]
- Castrejón, I.; Tani, C.; Jolly, M.; Huang, A.; Mosca, M. Indices to assess patients with systemic lupus erythematosus in clinical trials, long-term observational studies, and clinical care. Clin. Exp. Rheumatol. 2014, 32, S85–S95. [Google Scholar]
- Romero-Diaz, J.; Isenberg, D.; Ramsey-Goldman, R. Measures of adult systemic lupus erythematosus: Updated version of British Isles Lupus Assessment Group (BILAG 2004), European Consensus Lupus Activity Measurements (ECLAM), Systemic Lupus Activity Measure, Revised (SLAM-R), Systemic Lupus Activity Questionnaire for Population Studies (SLAQ), Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K), and Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index (SDI). Arthritis Care Res. 2011, 63 (Suppl. 11), S37–S46. [Google Scholar]
- Yu, J.; Zeng, T.; Wu, Y.; Tian, Y.; Tan, L.; Duan, X.; Wu, Q.; Li, H.; Yu, L. Neutrophil-to-C3 ratio and neutrophil-to-lymphocyte ratio were associated with disease activity in patients with systemic lupus erythematosus. J. Clin. Lab. Anal. 2019, 33, e22633. [Google Scholar] [CrossRef] [PubMed]
- Linnik, M.D.; Hu, J.Z.; Heilbrunn, K.R.; Strand, V.; Hurley, F.L.; Joh, T. Relationship between anti-double-stranded DNA antibodies and exacerbation of renal disease in patients with systemic lupus erythematosus. Arthritis Rheum. 2005, 52, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Gladman, D.D.; Goldsmith, C.H.; Urowitz, M.B.; Bacon, P.; Fortin, P.; Ginzler, E.; Gordon, C.; Hanly, J.G.; Isenberg, D.; Petri, M.; et al. The Systemic Lupus International Collaborating Clinics/American College of Rheumatology (SLICC/ACR) Damage Index for Systemic Lupus Erythematosus International Comparison. J. Rheumatol. 2000, 27, 373–376. [Google Scholar]
- Touma, Z.; Hoskin, B.; Atkinson, C.; Bell, D.; Massey, O.; Lofland, J.H.; Berry, P.; Karyekar, C.S.; Costenbader, K.H. Systemic lupus erythematosus symptom clusters and their association with patient-reported outcomes and treatment: Analysis of real-world data. Arthritis Care Res. 2020. [CrossRef]
- Lu, Z.; Li, W.; Tang, Y.; Da, Z.; Li, X. Lymphocyte subset clustering analysis in treatment-naive patients with systemic lupus erythematosus. Clin. Rheumatol. 2021, 40, 1835–1842. [Google Scholar] [CrossRef] [PubMed]
- Ahn, G.Y.; Lee, J.; Won, S.; Ha, E.; Kim, H.; Nam, B.; Kim, J.S.; Kang, J.; Kim, J.; Song, G.G.; et al. Identifying damage clusters in patients with systemic lupus erythematosus. Int. J. Rheum. Dis. 2020, 23, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Petri, M.; Orbai, A.-M.; Alarcón, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O.; et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef]
- Chan, E.K.L.; von Mühlen, C.A.; Fritzler, M.J.; Damoiseaux, J.; Infantino, M.; Klotz, W.; Satoh, M.; Musset, L.; García-De La Torre, I.; Carballo, O.G.; et al. The International Consensus on ANA Patterns (ICAP) in 2021-The 6th Workshop and Current Perspectives. J. Appl. Lab. Med. 2022, 7, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Uribe, A.G.; Vila, L.M.; McGwin, G., Jr.; Sanchez, M.L.; Reveille, J.D.; Alarcon, G.S. The Systemic Lupus Activity Measure-revised, the Mexican Systemic Lupus Erythematosus Disease Activity Index (SLEDAI), and a modified SLEDAI-2K are adequate instruments to measure disease activity in systemic lupus erythematosus. J. Rheumatol. 2004, 31, 1934–1940. [Google Scholar]
- Cheadle, C.; Vawter, M.P.; Freed, W.J.; Becker, K.G. Analysis of microarray data using Z score transformation. J. Mol. Diagn. 2003, 5, 73–81. [Google Scholar] [CrossRef] [Green Version]
- Murtagh, F.; Legendre, P. Ward’s hierarchical agglomerative clustering method: Which algorithms implement ward’s criterion? J. Classific. 2014, 31, 274–295. [Google Scholar] [CrossRef] [Green Version]
- Cervera, R.; Doria, A.; Amoura, Z.; Khamashta, M.; Schneider, M.; Guillemin, F.; Maurel, F.; Garofano, A.; Roset, M.; Perna, A.; et al. Patterns of systemic lupus erythematosus expression in Europe. Autoimmun. Rev. 2014, 13, 621–629. [Google Scholar] [CrossRef]
- To, C.H.; Mok, C.C.; Tang, S.S.K.; Ying, S.K.Y.; Wong, R.W.K.; Lau, C.S. Prognostically distinct clinical patterns of systemic lupus erythematosus identified by cluster analysis. Lupus 2009, 18, 1267–1275. [Google Scholar] [CrossRef] [PubMed]
- Pego-Reigosa, J.M.; Lois, A.; Rúa-Figueroa, Í.; Galindo, M.; Calvo-Alén, J.; de Uña-Álvarez, J.; Barreiro, V.B.; Ruan, J.I.; Olivé, A.; Rodríguez-Gómez, M.; et al. Relationship between damage clustering and mortality in systemic lupus erythematosus in early and late stages of the disease: Cluster analyses in a large cohort from the Spanish Society of Rheumatology Lupus Registry. Rheumatology 2016, 55, 1243–1250. [Google Scholar] [CrossRef] [Green Version]
- Enocsson, H.; Sjöwall, C.; Wirestam, L.; Dahle, C.; Kastbom, A.; Rönnelid, J.; Wetterö, J.; Skogh, T. Four anti-dsDNA antibody assays in relation to systemic lupus erythematosus disease specificity and activity. J. Rheumatol. 2015, 42, 817–825. [Google Scholar] [CrossRef]
- Biesen, R.; Rose, T.; Hoyer, B.F.; Alexander, T.; Hiepe, F. Autoantibodies, complement and type I interferon as biomarkers for personalized medicine in SLE. Lupus 2016, 25, 823–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soliman, S.; Mohan, C. Lupus nephritis biomarkers. Clin. Immunol. 2017, 185, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Cervera, R. Systemic lupus erythematosus in Europe at the change of the millennium: Lessons from the “Euro-Lupus Project”. Autoimmun. Rev. 2006, 5, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Hepburn, A.L.; Narat, S.; Mason, J.C. The management of peripheral blood cytopenias in systemic lupus erythematosus. Rheumatology 2010, 49, 2243–2254. [Google Scholar] [CrossRef] [Green Version]
- García-Valladares, I.; Atisha-Fregoso, Y.; Richaud-Patin, Y.; Jakez-Ocampo, J.; Soto-Vega, E.; Elías-López, D.; Carrillo-Maravilla, E.; Cabiedes, J.; Ruiz-Argüelles, A.; Llorente, L. Diminished expression of complement regulatory proteins (CD55 and CD59) in lymphocytes from systemic lupus erythematosus patients with lymphopenia. Lupus 2006, 15, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Ogbu, E.A.; Chandrakasan, S.; Rouster-Stevens, K.; Greenbaum, L.A.; Sanz, I.; Gillespie, S.E.; Marion, C.; Okeson, K.; Prahalad, S. Impact of autoimmune cytopenias on severity of childhood-onset systemic lupus erythematosus: A single-center retrospective cohort study. Lupus 2021, 30, 109–117. [Google Scholar] [CrossRef]
- Kurien, B.T.; Scofield, R.H. Autoantibody determination in the diagnosis of systemic lupus erythematosus. Scand. J. Immunol. 2006, 64, 227–235. [Google Scholar] [CrossRef]
- Pisetsky, D.S. Antinuclear antibodies in rheumatic disease: A proposal for a function-based classification. Scand. J. Immunol. 2012, 76, 223–228. [Google Scholar] [CrossRef]
- Solomon, D.H.; Kavanaugh, A.J.; Schur, P.H. Evidence-based guidelines for the use of immunologic tests: Antinuclear antibody testing. Arthritis Rheum. 2002, 47, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, C.; Kokkonen, H.; Johansson, M.; Hallmans, G.; Wadell, G.; Rantapää-Dahlqvist, S. Autoantibodies predate the onset of systemic lupus erythematosus in northern Sweden. Arthritis Res. Ther. 2011, 13, R30. [Google Scholar] [CrossRef] [Green Version]
- Almeida-Brasil, C.C.; Hanly, J.G.; Urowitz, M.; Clarke, A.E.; Ruiz-Irastorza, G.; Gordon, C.; Ramsey-Goldman, R.; Petri, M.; Ginzler, E.M.; Wallace, D.J.; et al. Flares after hydroxychloroquine reduction or discontinuation: Results from the Systemic Lupus International Collaborating Clinics (SLICC) inception cohort. Ann. Rheum. Dis. 2022, 81, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Pakchotanon, R.; Gladman, D.D.; Su, J.; Urowitz, M.B. More Consistent Antimalarial Intake in First 5 Years of Disease Is Associated with Better Prognosis in Patients with Systemic Lupus Erythematosus. J. Rheumatol. 2018, 45, 90–94. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Cluster 1 | Cluster 2 | Cluster 3 | p-Value a | ||||
|---|---|---|---|---|---|---|---|
| (n = 131) | (n = 183) | (n = 75) | Overall | 1 vs. 2 | 1 vs. 3 | 2 vs. 3 | |
| Diagnostic age, years | 31.2 ± 13.2 | 35.6 ± 12.6 | 36.8 ± 12.3 | <0.001 | 0.044 | <0.001 | 0.752 |
| Male: female, n (%) | 10 (7.6):121 (92.4) | 15 (8.2):168 (91.8) | 4 (5.3):71 (94.7) | 0.819 | 1.000 | 0.775 | 0.601 |
| Duration, month b | 117.8 ± 48.5 | 126.0 ± 40.6 | 138.4 ± 146.8 | 0.169 | 0.608 | 0.144 | 0.455 |
| WBC count,/µL | 5623.9 ± 3157.4 | 6111.9 ± 2304.6 | 4673.1 ± 1877.5 | <0.001 | 0.219 | 0.029 | <0.001 |
| Lymphocyte count,/µL | 1214.3 ± 628.1 | 1765.5 ± 683.0 | 1171.2 ± 395.7 | <0.001 | <0.001 | 0.881 | <0.001 |
| Hemoglobin,/µL | 11.5 ± 1.8 | 12.5 ± 1.6 | 12.3 ± 1.1 | <0.001 | <0.001 | 0.001 | 0.581 |
| Platelet count, ×103/µL | 208.1 ± 76.7 | 238.9 ± 88 | 225.7 ± 66.7 | 0.004 | 0.003 | 0.288 | 0.452 |
| ESR, mm/h | 30.4 ± 26.5 | 16.8 ± 17.9 | 26.7 ± 20.1 | <0.001 | <0.001 | 0.454 | 0.003 |
| CRP, mg/dL | 1.1 ± 3 | 0.5 ± 1.8 | 0.7 ± 2 | 0.097 | 0.078 | 0.554 | 0.756 |
| Complement 3, mg/dL | 71.8 ± 29.4 | 112.7 ± 27.3 | 110.5 ± 21.7 | <0.001 | <0.001 | <0.001 | 0.820 |
| Complement 4, mg/dL | 13 ± 7.5 | 25 ± 9.7 | 27.5 ± 8.6 | <0.001 | <0.001 | <0.001 | 0.100 |
| Anti-dsDNA antibody, IU/mL | 47.8 ± 38.5 | 7.2 ± 10.3 | 7.5 ± 6.8 | <0.001 | <0.001 | <0.001 | 0.996 |
| ANA titer | 1715.1 ± 1135.3 | 463.8 ± 641.6 | 2474.7 ± 731.5 | <0.001 | <0.001 | <0.001 | <0.001 |
| Homogenous (AC-1), n (%) | 46 (35.4) | 64 (35) | 11 (14.7) | 0.002 | 1.000 | 0.001 | 0.001 |
| Nucleolar (AC-8,9,10), n (%) | 0 (0) | 15 (8.2) | 1 (1.3) | <0.001 | <0.001 | 0.366 | 0.045 |
| Speckled (AC-4,5), n (%) | 58 (44.6) | 56 (30.6) | 54 (72) | <0.001 | 0.012 | <0.001 | <0.001 |
| Cytoplasmic (AC-15 to AC-23), n (%) | 3 (2.3) | 22 (12) | 1 (1.3) | <0.001 | 0.001 | 1.000 | 0.004 |
| Mixed, n (%) | 21 (16.2) | 26 (14.2) | 8 (10.7) | 0.575 | 0.634 | 0.306 | 0.545 |
| Parameters | LD1 | LD2 | LD3 |
|---|---|---|---|
| White blood cell count | 0.001 | 0.001 | 0.000 |
| Erythrocyte sedimentation rate | 0.013 | −0.040 | −0.014 |
| Complement 3 | 0.085 | 0.138 | 0.115 |
| Complement 4 | 0.000 | 0.086 | 0.174 |
| Anti-dsDNA Ab | 0.103 | 0.041 | 0.028 |
| Anti-nuclear antibody level | 0.002 | 0.000 | 0.003 |
| Constant | −10.259 | −11.298 | −14.753 |
| Cluster 1 | Cluster 2 | Cluster 3 | p-Value a | ||||
|---|---|---|---|---|---|---|---|
| (n = 131) | (n = 183) | (n = 75) | Overall | 1 vs. 2 | 1 vs. 3 | 2 vs. 3 | |
| Number of CMs, n (%) | 1.4 ± 1.3 | 0.9 ± 0.9 | 0.8 ± 1 | <0.001 | <0.001 | 0.002 | 0.901 |
| Number of CMs of ≥ 2, n (%) | 49 (37.7) | 41 (22.4) | 16 (21.3) | 0.006 | 0.004 | 0.019 | 1.000 |
| Oral ulcer, n (%) | 18 (13.7) | 43 (23.5) | 15 (20) | 0.095 | 0.042 | 0.244 | 0.624 |
| Malar rash, n (%) | 35 (26.7) | 27 (14.8) | 8 (10.7) | 0.006 | 0.010 | 0.007 | 0.430 |
| Alopecia, n (%) | 35 (26.9) | 19 (10.4) | 12 (16) | 0.001 | <0.001 | 0.085 | 0.212 |
| Arthritis, n (%) | 42 (32.1) | 52 (28.4) | 16 (21.3) | 0.263 | 0.533 | 0.110 | 0.278 |
| Renal disease, n (%) | 46 (35.1) | 24 (13.1) | 12 (16) | <0.001 | <0.001 | 0.004 | 0.556 |
| Serositis, n (%) | 2 (1.5) | 0 (0.0) | 0 (0) | 0.150 | 0.173 | 0.535 | NA |
| SLEDAI score * | 7.2 ± 4.9 | 3.0 ± 3.2 | 2.4 ± 2.7 | <0.001 | <0.001 | <0.001 | 0.548 |
| SLICC/ACR damage index | 0.4 ± 0.9 | 0.4 ± 1.0 | 0.4 ± 0.9 | 0.993 | 0.992 | 0.999 | 0.998 |
| Hydroxychloroquine use, n (%) | 81 (61.8) | 138 (75.4) | 57 (76) | 0.021 | 0.013 | 0.045 | 1.000 |
| Current glucocorticoid use, n (%) | 120 (91.6) | 159 (86.9) | 65 (86.7) | 0.385 | 0.208 | 0.339 | 1.000 |
| Total glucocorticoid dose, mg | 8465.9 ± 10,962 | 5306.0 ± 8645.4 | 5611.1 ± 6466.9 | 0.008 | 0.008 | 0.080 | 0.968 |
| Mean glucocorticoid dose, mg | 67.1 ± 76 | 37.8 ± 54.1 | 51.5 ± 82.3 | 0.001 | 0.001 | 0.254 | 0.305 |
| Azathioprine use, n (%) | 35 (26.7) | 22 (12) | 14 (18.7) | 0.004 | 0.001 | 0.235 | 0.170 |
| Cyclophosphamide use, n (%) | 19 (14.5) | 4 (2.2) | 3 (4) | <0.001 | <0.001 | 0.019 | 0.418 |
| MMF use, n (%) | 17 (13) | 12 (6.6) | 5 (6.7) | 0.127 | 0.074 | 0.240 | 1.000 |
| Methotrexate use, n (%) | 14 (10.7) | 31 (16.9) | 13 (17.3) | 0.243 | 0.142 | 0.200 | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, J.-Y.; Lee, H.-Y.; Lee, E.; Kim, H.-A.; Yoon, D.; Suh, C.-H. Three Clinical Clusters Identified through Hierarchical Cluster Analysis Using Initial Laboratory Findings in Korean Patients with Systemic Lupus Erythematosus. J. Clin. Med. 2022, 11, 2406. https://doi.org/10.3390/jcm11092406
Jung J-Y, Lee H-Y, Lee E, Kim H-A, Yoon D, Suh C-H. Three Clinical Clusters Identified through Hierarchical Cluster Analysis Using Initial Laboratory Findings in Korean Patients with Systemic Lupus Erythematosus. Journal of Clinical Medicine. 2022; 11(9):2406. https://doi.org/10.3390/jcm11092406
Chicago/Turabian StyleJung, Ju-Yang, Hyun-Young Lee, Eunyoung Lee, Hyoun-Ah Kim, Dukyong Yoon, and Chang-Hee Suh. 2022. "Three Clinical Clusters Identified through Hierarchical Cluster Analysis Using Initial Laboratory Findings in Korean Patients with Systemic Lupus Erythematosus" Journal of Clinical Medicine 11, no. 9: 2406. https://doi.org/10.3390/jcm11092406
APA StyleJung, J.-Y., Lee, H.-Y., Lee, E., Kim, H.-A., Yoon, D., & Suh, C.-H. (2022). Three Clinical Clusters Identified through Hierarchical Cluster Analysis Using Initial Laboratory Findings in Korean Patients with Systemic Lupus Erythematosus. Journal of Clinical Medicine, 11(9), 2406. https://doi.org/10.3390/jcm11092406