
Predictors of Submaximal Exercise Test Attainment in Adults Reporting Long COVID Symptoms



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study and Cohort Description
2.2. Participant Characteristics
- ○
- Demographics: age, sex.
- ○
- Anthropometrics: body mass index (BMI, Kg/m2).
- ○
- Days since COVID-19 illness, and whether a participant was hospitalized or not due to COVID-19 (at least one overnight stay).
- ○
- Cardiopulmonary disease prior to COVID-19 (chronic respiratory disease, chronic heart disease, or hypertension: yes or no).
- ○
- Current medications: antihypertensives, beta blockers (yes or no).
- ○
- Smoking status: never smoked versus former/current smoker.
- ○
- Resting seated systolic (SBP), diastolic (DBP) blood pressure and HR were measured prior to CPET with an oscillometric brachial blood pressure measurement device (Connex® Vital Signs Monitor, Welch Allyn Inc., Skaneateles Falls, NY, USA).
- ○
- Long COVID symptomatology. Participants were asked if following COVID-19 illness they had ongoing symptoms (yes or no) of: shortness of breath, cough, throat pain, chest tightness, chest pain, heart palpitations, headache, loss of smell, loss of taste, brain fog, sleeping problems, dizziness, muscular weakness, muscular pain, or joint pain.
- ○
- Participants were also administered the 11-item Chalder Fatigue Scale (CFQ), a self-rating scale developed to measure the severity of physical and mental fatigue [21]. We employed the Likert scoring system, with an overall scale range from 0 (minimum) to 33 (maximum fatigue).
2.3. CPET Protocol
- ○
- Test duration (seconds).
- ○
- Peak HR achieved (beats per minute, bpm).
- ○
- Peak work rate (WR, Watts).
- ○
- Peak oxygen consumption (VO2peak), average during last 30 s of exercise, per Kg (mL/Kg/min).
- ○
- ○
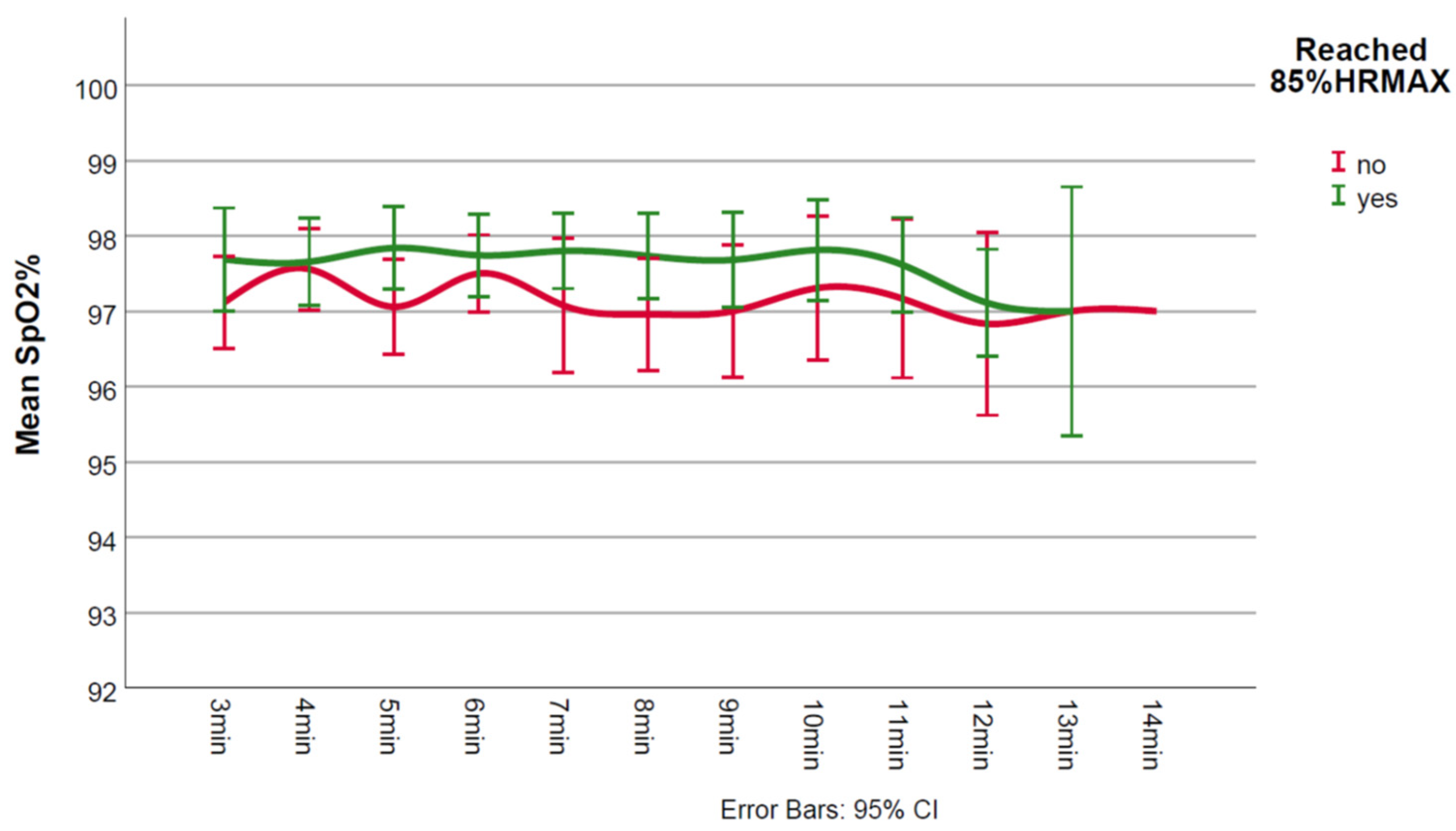
- Lowest SpO2% value.
- ○
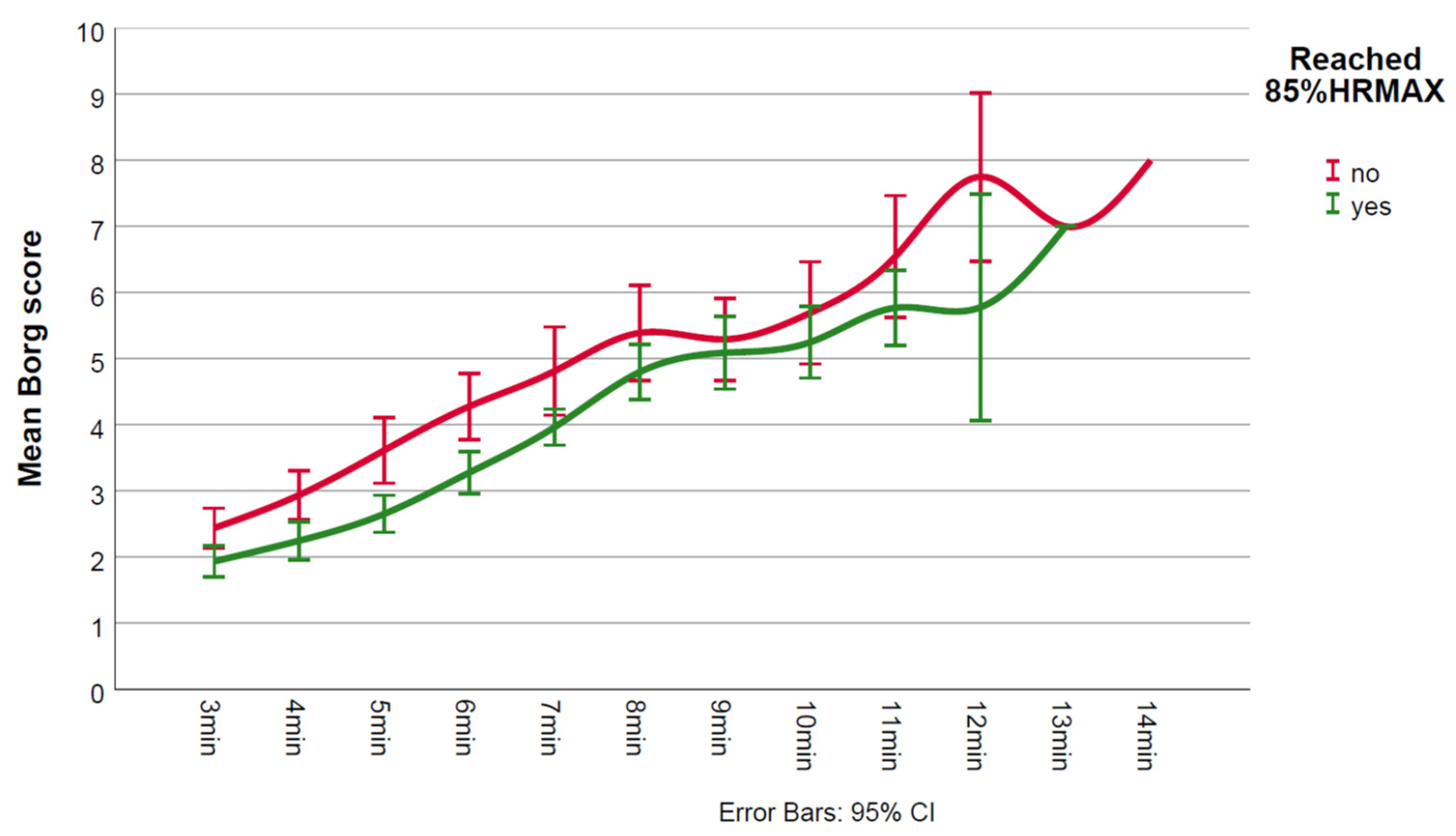
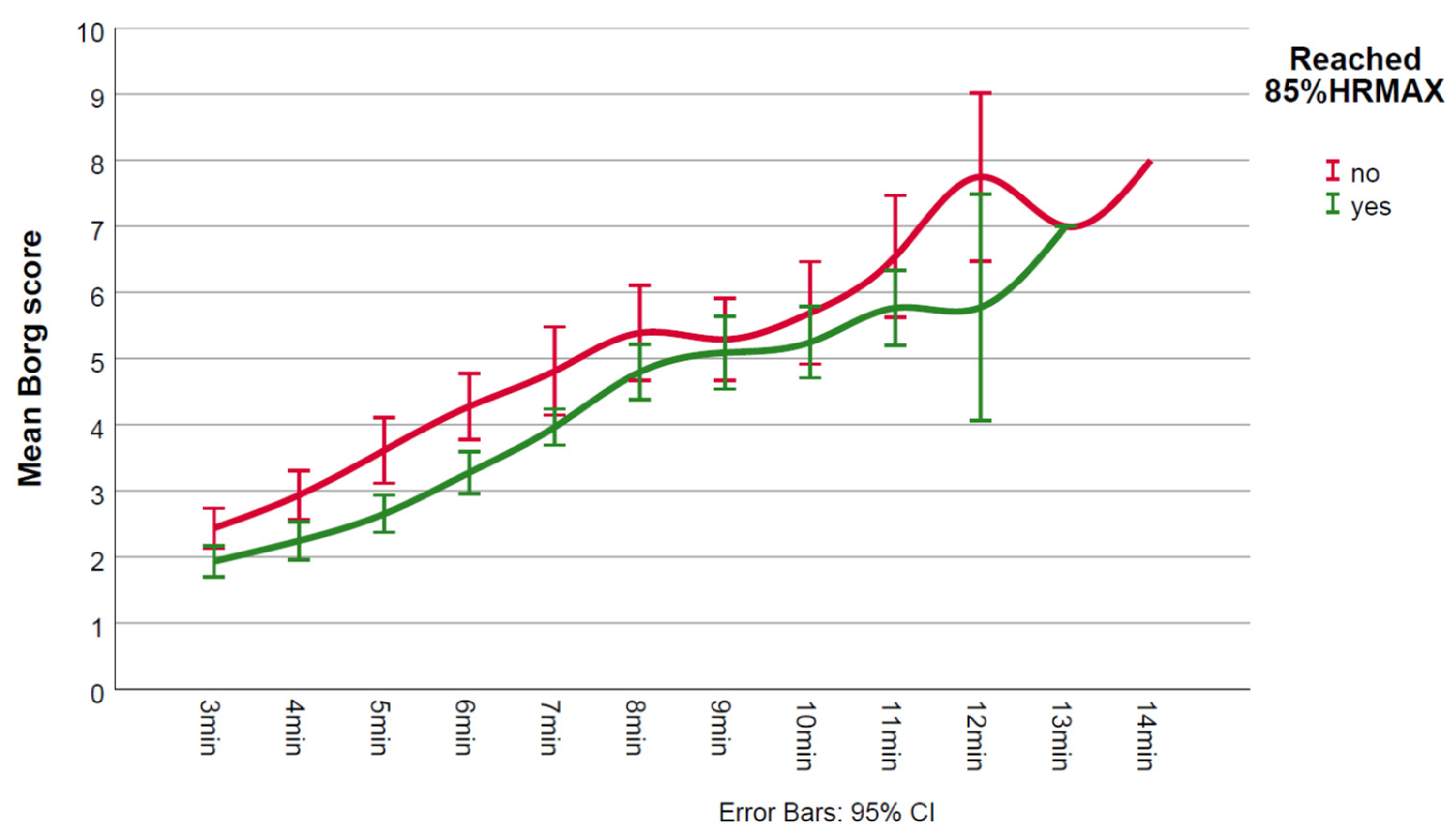
- Maximum Borg score.
2.4. Statistical Analyses
2.5. Ethical Approval
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Odds Ratio | 95% Confidence Interval for Odds Ratio | p | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Age | 0.861 | 0.776 | 0.955 | 0.005 |
| Days post-COVID-19 | 1.006 | 1.001 | 1.010 | 0.014 |
| Hospitalized | 0.119 | 0.017 | 0.816 | 0.030 |
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [PubMed]
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 5 February 2022).
- WHO. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus, 6 October 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 5 February 2022).
- Taquet, M.; Dercon, Q.; Luciano, S.; Geddes, J.R.; Husain, M.; Harrison, P.J. Incidence, co-occurrence, and evolution of long-COVID features: A 6-month retrospective cohort study of 273,618 survivors of COVID-19. PLoS Med. 2021, 18, e1003773. [Google Scholar] [CrossRef] [PubMed]
- Jennings, G.; Monaghan, A.; Xue, F.; Mockler, D.; Romero-Ortuno, R. A Systematic Review of Persistent Symptoms and Residual Abnormal Functioning following Acute COVID-19: Ongoing Symptomatic Phase vs. Post-COVID-19 Syndrome. J. Clin. Med. 2021, 10, 5913. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-de-Las-Penas, C.; Palacios-Cena, D.; Gomez-Mayordomo, V.; Palacios-Cena, M.; Rodriguez-Jimenez, J.; de-la-Llave-Rincon, A.I.; Velasco-Arribas, M.; Fuensalida-Novo, S.; Ambite-Quesada, S.; Guijarro, C.; et al. Fatigue and Dyspnoea as Main Persistent Post-COVID-19 Symptoms in Previously Hospitalized Patients: Related Functional Limitations and Disability. Respiration 2022, 101, 132–141. [Google Scholar] [CrossRef]
- Tleyjeh, I.M.; Saddik, B.; Ramakrishnan, R.K.; AlSwaidan, N.; AlAnazi, A.; Alhazmi, D.; Aloufi, A.; AlSumait, F.; Berbari, E.F.; Halwani, R. Long term predictors of breathlessness, exercise intolerance, chronic fatigue and well-being in hospitalized patients with COVID-19: A cohort study with 4 months median follow-up. J. Infect. Public Health 2022, 15, 21–28. [Google Scholar] [CrossRef]
- Jahn, K.; Sava, M.; Sommer, G.; Schumann, D.M.; Bassetti, S.; Siegemund, M.; Battegay, M.; Stolz, D.; Tamm, M.; Khanna, N.; et al. Exercise capacity impairment after COVID-19 pneumonia is mainly caused by deconditioning. Eur. Respir. J. 2022, 59, 2101136. [Google Scholar] [CrossRef]
- Rinaldo, R.F.; Mondoni, M.; Parazzini, E.M.; Pitari, F.; Brambilla, E.; Luraschi, S.; Balbi, M.; Sferrazza Papa, G.F.; Sotgiu, G.; Guazzi, M.; et al. Deconditioning as main mechanism of impaired exercise response in COVID-19 survivors. Eur. Respir. J. 2021, 58, 2100870. [Google Scholar] [CrossRef]
- Clavario, P.; De Marzo, V.; Lotti, R.; Barbara, C.; Porcile, A.; Russo, C.; Beccaria, F.; Bonavia, M.; Bottaro, L.C.; Caltabellotta, M.; et al. Assessment of functional capacity with cardiopulmonary exercise testing in non-severe COVID-19 patients at three months follow-up. medRxiv 2020. medRxiv:2020.11.15.20231985. [Google Scholar]
- Ferreira, E.V.M.; Oliveira, R.K.F. Mechanisms of exercise intolerance after COVID-19: New perspectives beyond physical deconditioning. J. Bras. Pneumol. 2021, 47, e20210406. [Google Scholar]
- Albouaini, K.; Egred, M.; Alahmar, A.; Wright, D.J. Cardiopulmonary exercise testing and its application. Heart 2007, 93, 1285–1292. [Google Scholar] [CrossRef] [PubMed]
- Glaab, T.; Taube, C. Practical guide to cardiopulmonary exercise testing in adults. Respir. Res. 2022, 23, 9. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, R.J.; Balady, G.J.; Bricker, J.T.; Chaitman, B.R.; Fletcher, G.F.; Froelicher, V.F.; Mark, D.B.; McCallister, B.D.; Mooss, A.N.; O’Reilly, M.G.; et al. ACC/AHA 2002 guideline update for exercise testing: Summary article: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). Circulation 2002, 106, 1883–1892. [Google Scholar] [PubMed]
- Brubaker, P.H.; Kitzman, D.W. Chronotropic incompetence: Causes, consequences, and management. Circulation 2011, 123, 1010–1020. [Google Scholar] [CrossRef] [Green Version]
- Naeije, R.; Caravita, S. CPET for Long COVID-19. JACC Heart Fail. 2022, 10, 214–215. [Google Scholar] [CrossRef]
- Liguori, G.; ACSM. ACSM’s Guidelines for Exercise Testing and Prescription, 11th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2020. [Google Scholar]
- Thompson, P.D.; Arena, R.; Riebe, D.; Pescatello, L.S.; American College of Sports Medicine. ACSM’s new preparticipation health screening recommendations from ACSM’s guidelines for exercise testing and prescription, ninth edition. Curr. Sports Med. Rep. 2013, 12, 215–217. [Google Scholar] [CrossRef]
- Monaghan, A.; Jennings, G.; Xue, F.; Byrne, L.; Duggan, E.; Romero-Ortuno, R. Orthostatic Intolerance in Adults Reporting Long COVID Symptoms Was Not Associated with Postural Orthostatic Tachycardia Syndrome. Front. Physiol. 2022, 13, 833650. [Google Scholar] [CrossRef]
- Cella, M.; Chalder, T. Measuring fatigue in clinical and community settings. J. Psychosom. Res. 2010, 69, 17–22. [Google Scholar] [CrossRef]
- Mihalick, V.L.; Canada, J.M.; Arena, R.; Abbate, A.; Kirkman, D.L. Cardiopulmonary exercise testing during the COVID-19 pandemic. Prog. Cardiovasc. Dis. 2021, 67, 35–39. [Google Scholar] [CrossRef]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef] [Green Version]
- Burdon, J.G.; Juniper, E.F.; Killian, K.J.; Hargreave, F.E.; Campbell, E.J. The perception of breathlessness in asthma. Am. Rev. Respir. Dis. 1982, 126, 825–828. [Google Scholar] [PubMed]
- Weatherald, J.; Philipenko, B.; Montani, D.; Laveneziana, P. Ventilatory efficiency in pulmonary vascular diseases. Eur. Respir. Rev. 2021, 30, 200214. [Google Scholar] [CrossRef] [PubMed]
- Crisafulli, E.; Dorelli, G.; Sartori, G.; Dalle Carbonare, L. Exercise ventilatory inefficiency may be a relevant CPET-feature in COVID-19 survivors. Int. J. Cardiol. 2021, 343, 200. [Google Scholar] [CrossRef] [PubMed]
- NICE, COVID-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19 NICE Guideline [NG188]. Available online: https://www.nice.org.uk/guidance/ng188 (accessed on 18 April 2022).
- Palmer, S.; Cunniffe, N.; Donnelly, R. COVID-19 hospitalization rates rise exponentially with age, inversely proportional to thymic T-cell production. J. R. Soc. Interface 2021, 18, 20200982. [Google Scholar] [CrossRef]
- Cheval, B.; Sieber, S.; Maltagliati, S.; Millet, G.P.; Formanek, T.; Chalabaev, A.; Cullati, S.; Boisgontier, M.P. Muscle strength is associated with COVID-19 hospitalization in adults 50 years of age or older. J. Cachexia Sarcopenia Muscle 2021, 12, 1136–1143. [Google Scholar] [CrossRef]
- Mohamed Hussein, A.A.; Saad, M.; Zayan, H.E.; Abdelsayed, M.; Moustafa, M.; Ezzat, A.R.; Helmy, R.; Abd-Elaal, H.; Aly, K.; Abdelrheem, S.; et al. Post-COVID-19 functional status: Relation to age, smoking, hospitalization, and previous comorbidities. Ann. Thorac. Med. 2021, 16, 260–265. [Google Scholar] [CrossRef]
- Vonbank, K.; Lehmann, A.; Bernitzky, D.; Gysan, M.R.; Simon, S.; Schrott, A.; Burtscher, M.; Idzko, M.; Gompelmann, D. Predictors of Prolonged Cardiopulmonary Exercise Impairment After COVID-19 Infection: A Prospective Observational Study. Front. Med. 2021, 8, 773788. [Google Scholar] [CrossRef]
- Barbagelata, L.; Masson, W.; Iglesias, D.; Lillo, E.; Migone, J.F.; Orazi, M.L.; Maritano Furcada, J. Cardiopulmonary Exercise Testing in Patients with Post-COVID-19 Syndrome. Med. Clin. 2021. [Google Scholar] [CrossRef]
- Aparisi, A.; Ybarra-Falcon, C.; Garcia-Gomez, M.; Tobar, J.; Iglesias-Echeverria, C.; Jaurrieta-Largo, S.; Ladron, R.; Uribarri, A.; Catala, P.; Hinojosa, W.; et al. Exercise Ventilatory Inefficiency in Post-COVID-19 Syndrome: Insights from a Prospective Evaluation. J. Clin. Med. 2021, 10, 2591. [Google Scholar] [CrossRef]
- Mohr, A.; Dannerbeck, L.; Lange, T.J.; Pfeifer, M.; Blaas, S.; Salzberger, B.; Hitzenbichler, F.; Koch, M. Cardiopulmonary exercise pattern in patients with persistent dyspnoea after recovery from COVID-19. Multidiscip. Respir. Med. 2021, 16, 732. [Google Scholar] [CrossRef]
- Ladlow, P.; O’Sullivan, O.; Houston, A.; Barker-Davies, R.; May, S.; Mills, D.; Dewson, D.; Chamley, R.; Naylor, J.; Mulae, J.; et al. Dysautonomia following COVID-19 is not associated with subjective limitations or symptoms but is associated with objective functional limitations. Heart Rhythm 2021, 19, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Maiese, A.; Passaro, G.; Matteis, A.; Fazio, V.; Raffaele, R.; Paolo, M.D. Thromboinflammatory response in SARS-CoV-2 sepsis. Med. Leg. J. 2020, 88, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Zanza, C.; Romenskaya, T.; Manetti, A.C.; Franceschi, F.; La Russa, R.; Bertozzi, G.; Maiese, A.; Savioli, G.; Volonnino, G.; Longhitano, Y. Cytokine Storm in COVID-19: Immunopathogenesis and Therapy. Medicina 2022, 58, 144. [Google Scholar] [CrossRef] [PubMed]
- Raman, B.; Cassar, M.P.; Tunnicliffe, E.M.; Filippini, N.; Griffanti, L.; Alfaro-Almagro, F.; Okell, T.; Sheerin, F.; Xie, C.; Mahmod, M.; et al. Medium-term effects of SARS-CoV-2 infection on multiple vital organs, exercise capacity, cognition, quality of life and mental health, post-hospital discharge. EClinicalMedicine 2021, 31, 100683. [Google Scholar] [CrossRef]
- Taboada, M.; Moreno, E.; Carinena, A.; Rey, T.; Pita-Romero, R.; Leal, S.; Sanduende, Y.; Rodriguez, A.; Nieto, C.; Vilas, E.; et al. Quality of life, functional status, and persistent symptoms after intensive care of COVID-19 patients. Br. J. Anaesth. 2021, 126, e110–e113. [Google Scholar] [CrossRef]
- Maglietta, G.; Diodati, F.; Puntoni, M.; Lazzarelli, S.; Marcomini, B.; Patrizi, L.; Caminiti, C. Prognostic Factors for Post-COVID-19 Syndrome: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 1541. [Google Scholar] [CrossRef]
- Johnsen, S.; Sattler, S.M.; Miskowiak, K.W.; Kunalan, K.; Victor, A.; Pedersen, L.; Andreassen, H.F.; Jorgensen, B.J.; Heeboll, H.; Andersen, M.B.; et al. Descriptive analysis of long COVID sequelae identified in a multidisciplinary clinic serving hospitalised and non-hospitalised patients. ERJ Open Res. 2021, 7, 00205-2021. [Google Scholar] [CrossRef]
- Debeaumont, D.; Boujibar, F.; Ferrand-Devouge, E.; Artaud-Macari, E.; Tamion, F.; Gravier, F.E.; Smondack, P.; Cuvelier, A.; Muir, J.F.; Alexandre, K.; et al. Cardiopulmonary Exercise Testing to Assess Persistent Symptoms at 6 Months in People With COVID-19 Who Survived Hospitalization: A Pilot Study. Phys. Ther 2021, 101, pzab099. [Google Scholar] [CrossRef]
- Blokland, I.J.; Ilbrink, S.; Houdijk, H.; Dijkstra, J.W.; van Bennekom, C.A.M.; Fickert, R.; de Lijster, R.; Groot, F.P. Exercise capacity after mechanical ventilation because of COVID-19: Cardiopulmonary exercise tests in clinical rehabilitation. Ned. Tijdschr. Geneeskd. 2020, 164, D5253. [Google Scholar]
- Cassar, M.P.; Tunnicliffe, E.M.; Petousi, N.; Lewandowski, A.J.; Xie, C.; Mahmod, M.; Samat, A.H.A.; Evans, R.A.; Brightling, C.E.; Ho, L.P.; et al. Symptom Persistence Despite Improvement in Cardiopulmonary Health—Insights from longitudinal CMR, CPET and lung function testing post-COVID-19. EClinicalMedicine 2021, 41, 101159. [Google Scholar] [CrossRef]
- Alba, G.A.; Ziehr, D.R.; Rouvina, J.N.; Hariri, L.P.; Knipe, R.S.; Medoff, B.D.; Hibbert, K.A.; Kowal, A.; Hoenstine, C.; Ginns, L.C.; et al. Exercise performance in patients with post-acute sequelae of SARS-CoV-2 infection compared to patients with unexplained dyspnea. EClinicalMedicine 2021, 39, 101066. [Google Scholar] [CrossRef] [PubMed]
- Rinaldo, R.F.; Mondoni, M.; Parazzini, E.M.; Baccelli, A.; Pitari, F.; Brambilla, E.; Luraschi, S.; Balbi, M.; Guazzi, M.; Di Marco, F.; et al. Severity does not impact on exercise capacity in COVID-19 survivors. Respir. Med. 2021, 187, 106577. [Google Scholar] [CrossRef] [PubMed]
- Csulak, E.; Petrov, A.; Kovats, T.; Tokodi, M.; Lakatos, B.; Kovacs, A.; Staub, L.; Suhai, F.I.; Szabo, E.L.; Dohy, Z.; et al. The Impact of COVID-19 on the Preparation for the Tokyo Olympics: A Comprehensive Performance Assessment of Top Swimmers. Int. J. Environ. Res. Public Health 2021, 18, 9770. [Google Scholar] [CrossRef] [PubMed]
- Cavigli, L.; Frascaro, F.; Turchini, F.; Mochi, N.; Sarto, P.; Bianchi, S.; Parri, A.; Carraro, N.; Valente, S.; Focardi, M.; et al. A prospective study on the consequences of SARS-CoV-2 infection on the heart of young adult competitive athletes: Implications for a safe return-to-play. Int. J. Cardiol. 2021, 336, 130–136. [Google Scholar] [CrossRef]
- Komici, K.; Bianco, A.; Perrotta, F.; Dello Iacono, A.; Bencivenga, L.; D’Agnano, V.; Rocca, A.; Bianco, A.; Rengo, G.; Guerra, G. Clinical Characteristics, Exercise Capacity and Pulmonary Function in Post-COVID-19 Competitive Athletes. J. Clin. Med. 2021, 10, 3053. [Google Scholar] [CrossRef]
- Anastasio, F.; La Macchia, T.; Rossi, G.; D’Abbondanza, M.; Curcio, R.; Vaudo, G.; Pucci, G. Mid-term impact of mild-moderate COVID-19 on cardiorespiratory fitness in elite athletes. J. Sports Med. Phys. Fitness 2021. [Google Scholar] [CrossRef]
- Clavario, P.; De Marzo, V.; Lotti, R.; Barbara, C.; Porcile, A.; Russo, C.; Beccaria, F.; Bonavia, M.; Bottaro, L.C.; Caltabellotta, M.; et al. Cardiopulmonary exercise testing in COVID-19 patients at 3 months follow-up. Int. J. Cardiol. 2021, 340, 113–118. [Google Scholar] [CrossRef]
- Mancini, D.M.; Brunjes, D.L.; Lala, A.; Trivieri, M.G.; Contreras, J.P.; Natelson, B.H. Use of Cardiopulmonary Stress Testing for Patients With Unexplained Dyspnea Post-Coronavirus Disease. JACC Heart Fail. 2021, 9, 927–937. [Google Scholar] [CrossRef]
- Singh, I.; Joseph, P.; Heerdt, P.M.; Cullinan, M.; Lutchmansingh, D.D.; Gulati, M.; Possick, J.D.; Systrom, D.M.; Waxman, A.B. Persistent Exertional Intolerance After COVID-19: Insights From Invasive Cardiopulmonary Exercise Testing. Chest 2022, 161, 54–63. [Google Scholar] [CrossRef]
- Motiejunaite, J.; Balagny, P.; Arnoult, F.; Mangin, L.; Bancal, C.; d’Ortho, M.P.; Frija-Masson, J. Hyperventilation: A Possible Explanation for Long-Lasting Exercise Intolerance in Mild COVID-19 Survivors? Front. Physiol. 2020, 11, 614590. [Google Scholar] [CrossRef]
- Driver, S.; Reynolds, M.; Brown, K.; Vingren, J.L.; Hill, D.W.; Bennett, M.; Gilliland, T.; McShan, E.; Callender, L.; Reynolds, E.; et al. Effects of wearing a cloth face mask on performance, physiological and perceptual responses during a graded treadmill running exercise test. Br. J. Sports Med. 2022, 56, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Kersten, J.; Baumhardt, M.; Hartveg, P.; Hoyo, L.; Hull, E.; Imhof, A.; Kropf-Sanchen, C.; Nita, N.; Morike, J.; Rattka, M.; et al. Long COVID: Distinction between Organ Damage and Deconditioning. J. Clin. Med. 2021, 10, 3782. [Google Scholar] [CrossRef] [PubMed]
| Characteristic | Did Not Reach 85% Maximum HR (n = 40) | Reached 85% Maximum HR (n = 40) | p for Difference |
|---|---|---|---|
| Baseline characteristics | |||
| Mean age, years (SD) | 50.0 (9.7) | 42.0 (7.6) | <0.001 ^ |
| Female sex (%) | 72.5 | 70.0 | 0.805 + |
| Mean BMI, Kg/m2 (SD) | 29.0 (5.4) | 26.3 (4.2) | 0.050 ^ |
| Median days post-COVID-19 (IQR) | 256.5 (294.5) | 464.0 (288.0) | 0.012 ^ |
| Hospitalized during COVID-19 illness (%) | 27.8 | 7.9 | 0.025 + |
| Admitted to ICU (%) | 2.5 | 0.0 | 1.000 ++ |
| Previous respiratory disease (%) | 17.5 | 10.0 | 0.330 + |
| Previous heart disease (%) | 5.0 | 0.0 | 0.247 ++ |
| Treated hypertension (%) | 22.5 | 12.5 | 0.239 + |
| Cardiopulmonary disease (%) | 40.0 | 20.0 | 0.051 + |
| On beta blockers (%) | 15.0 | 7.5 | 0.481 ++ |
| Never smoked (%) | 47.2 | 62.2 | 0.200 + |
| Mean seated SBP, mmHg (SD) | 132.3 (18.2) | 128.0 (13.5) | 0.503 ^ |
| Mean seated DBP, mmHg (SD) | 80.3 (13.5) | 81.1 (7.9) | 0.972 ^ |
| Mean resting HR, bpm (SD) | 69.6 (10.3) | 72.8 (11.1) | 0.320 ^ |
| Long COVID symptomatology | |||
| Shortness of breath (%) | 75.7 | 71.1 | 0.651 + |
| Cough (%) | 21.6 | 26.3 | 0.634 + |
| Throat pain (%) | 37.8 | 28.9 | 0.414 + |
| Chest tightness (%) | 56.8 | 55.3 | 0.896 + |
| Chest pain (%) | 32.4 | 36.8 | 0.688 + |
| Heart palpitations (%) | 59.5 | 55.3 | 0.713 + |
| Headache (%) | 62.2 | 73.7 | 0.285 + |
| Loss of smell (%) | 21.6 | 13.2 | 0.333 + |
| Loss of taste (%) | 18.9 | 13.2 | 0.496 + |
| Brain fog (%) | 56.8 | 71.1 | 0.197 + |
| Sleeping problems (%) | 73.0 | 55.3 | 0.110 + |
| Dizziness (%) | 73.0 | 50.0 | 0.041 + |
| Muscular weakness (%) | 10.8 | 7.9 | 0.711 ++ |
| Muscular pain (%) | 59.5 | 47.4 | 0.294 + |
| Joint pain (%) | 59.5 | 34.2 | 0.028 + |
| Median CFQ score (IQR) | 25.5 (9.3) | 24.5 (8.0) | 0.711 ^ |
| CPET characteristics | |||
| Mean predicted 85%HRmax, bpm (SD) | 147.1 (5.8) | 151.8 (4.5) | <0.001 ^ |
| Mean predicted VO2 max, mL/Kg/min (SD) | 29.4 (7.1) | 29.8 (8.4) | 0.761 ^ |
| Mean CPET duration, seconds (SD) | 402.1 (136.4) | 469.2 (96.2) | 0.008 ^ |
| Mean peak HR achieved during CPET, bpm (SD) | 123.5 (16.7) | 153.7 (5.4) | <0.001 ^ |
| Mean peak work rate achieved during CPET, W (SD) | 96.0 (40.1) | 133.5 (57.6) | 0.002 ^ |
| Mean peak VO2 achieved during last 30 s of exercise per Kg, mL/Kg/min (SD) | 16.1 (5.5) | 21.8 (7.2) | <0.001 ^ |
| Mean VE/VCO2 during last 30 s of exercise (SD) | 33.2 (5.5) | 29.8 (4.6) | 0.007 ^ |
| Mean lowest SpO2% during CPET (SD) | 96.0 (1.9) | 96.7 (1.8) | 0.128 ^ |
| Mean maximum Borg score during CPET (SD) | 6.7 (1.6) | 5.9 (1.4) | 0.026 ^ |
| Odds Ratio | 95% Confidence Interval for Odds Ratio | p | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Age | 0.879 | 0.815 | 0.949 | 0.001 |
| Days post-COVID-19 | 1.006 | 1.001 | 1.010 | 0.008 |
| Hospitalized | 0.227 | 0.040 | 1.297 | 0.095 |
| Joint pain | 0.372 | 0.118 | 1.177 | 0.093 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-Ortuno, R.; Jennings, G.; Xue, F.; Duggan, E.; Gormley, J.; Monaghan, A. Predictors of Submaximal Exercise Test Attainment in Adults Reporting Long COVID Symptoms. J. Clin. Med. 2022, 11, 2376. https://doi.org/10.3390/jcm11092376
Romero-Ortuno R, Jennings G, Xue F, Duggan E, Gormley J, Monaghan A. Predictors of Submaximal Exercise Test Attainment in Adults Reporting Long COVID Symptoms. Journal of Clinical Medicine. 2022; 11(9):2376. https://doi.org/10.3390/jcm11092376
Chicago/Turabian StyleRomero-Ortuno, Roman, Glenn Jennings, Feng Xue, Eoin Duggan, John Gormley, and Ann Monaghan. 2022. "Predictors of Submaximal Exercise Test Attainment in Adults Reporting Long COVID Symptoms" Journal of Clinical Medicine 11, no. 9: 2376. https://doi.org/10.3390/jcm11092376
APA StyleRomero-Ortuno, R., Jennings, G., Xue, F., Duggan, E., Gormley, J., & Monaghan, A. (2022). Predictors of Submaximal Exercise Test Attainment in Adults Reporting Long COVID Symptoms. Journal of Clinical Medicine, 11(9), 2376. https://doi.org/10.3390/jcm11092376