
Incidence and Outcome of Patients with Cardiogenic Shock and Detection of Herpes Simplex Virus in the Lower Respiratory Tract

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sedation, Ventilation, Mechanical Support Devices and Bronchial Lavage
2.3. Statistical Analysis
3. Results
3.1. Study Population and Baseline Characteristics
3.2. Comparison between Patients with HSV vs. without HSV Detection
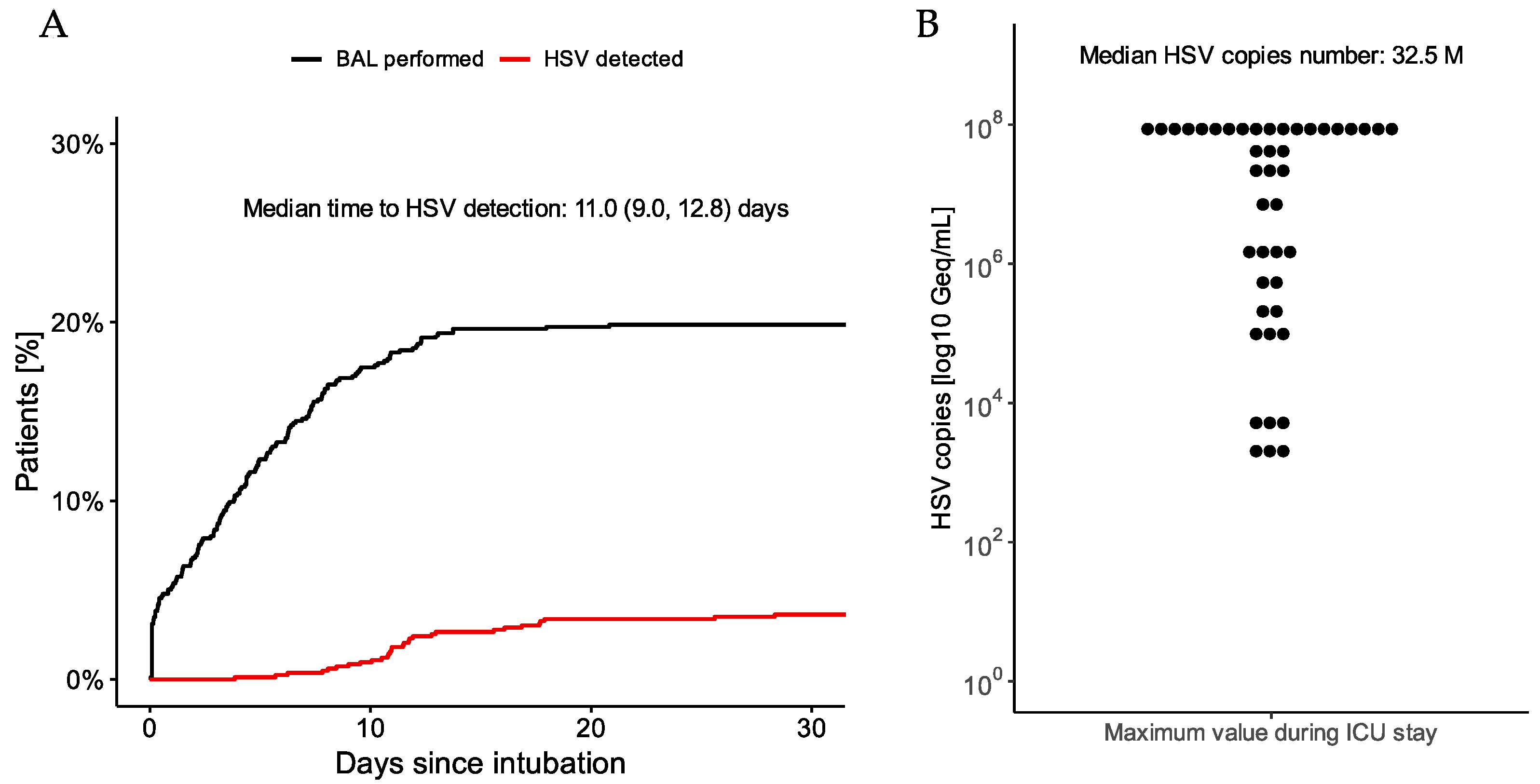
3.3. Characteristics of HSV Reactivation and Antiviral Therapy
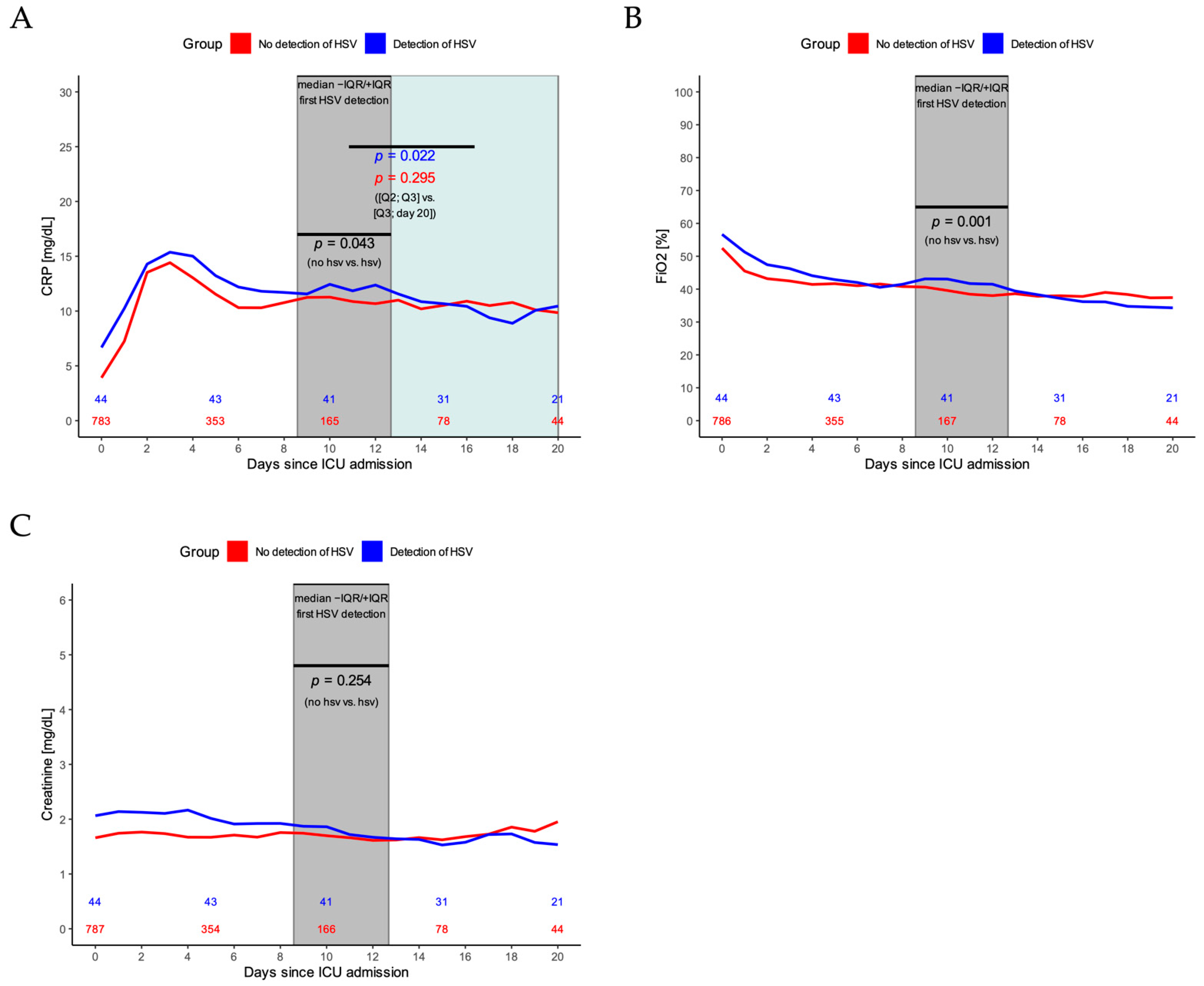
3.4. Impact of HSV Reactivation on Inflammation and Ventilation
3.5. Risk Factors for HSV Occurrence
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC)Developed with the Special Contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [PubMed]
- Samsky, M.D.; Morrow, D.A.; Proudfoot, A.G.; Hochman, J.S.; Thiele, H.; Rao, S.V. Cardiogenic Shock after Acute Myocardial Infarction: A Review. JAMA 2021, 326, 1840–1850. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Ohman, E.M.; De Waha-Thiele, S.; Zeymer, U.; Desch, S. Management of cardiogenic shock complicating myocardial infarction: An update 2019. Eur. Heart J. 2019, 40, 2671–2683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunner, S.; Guenther, S.P.; Lackermair, K.; Peterss, S.; Orban, M.; Boulesteix, A.-L.; Michel, S.; Hausleiter, J.; Massberg, S.; Hagl, C. Extracorporeal Life Support in Cardiogenic Shock Complicating Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2019, 73, 2355–2357. [Google Scholar] [CrossRef] [PubMed]
- Lüsebrink, E.; Orban, M.; Kupka, D.; Scherer, C.; Hagl, C.; Zimmer, S.; Luedike, P.; Thiele, H.; Westermann, D.; Massberg, S.; et al. Prevention and treatment of pulmonary congestion in patients undergoing venoarterial extracorporeal membrane oxygenation for cardiogenic shock. Eur. Heart J. 2020, 41, 3753–3761. [Google Scholar] [CrossRef] [PubMed]
- Cheng, R.; Hachamovitch, R.; Kittleson, M.; Patel, J.; Arabia, F.; Moriguchi, J.; Esmailian, F.; Azarbal, B. Complications of Extracorporeal Membrane Oxygenation for Treatment of Cardiogenic Shock and Cardiac Arrest: A Meta-Analysis of 1,866 Adult Patients. Ann. Thorac. Surg. 2014, 97, 610–616. [Google Scholar] [CrossRef]
- Schmidt, M.; Bréchot, N.; Hariri, S.; Guiguet, M.; Luyt, C.E.; Makri, R.; Leprince, P.; Trouillet, J.-L.; Pavie, A.; Chastre, J.; et al. Nosocomial Infections in Adult Cardiogenic Shock Patients Supported by Venoarterial Extracorporeal Membrane Oxygenation. Clin. Infect. Dis. 2012, 55, 1633–1641. [Google Scholar] [CrossRef] [Green Version]
- Simoons-Smit, A.M.; Kraan, E.M.; Beishuizen, A.; van Schijndel, R.J.S.; Vandenbroucke-Grauls, C.M. Herpes simplex virus type 1 and respiratory disease in critically-ill patients: Real pathogen or innocent bystander? Clin. Microbiol. Infect. 2006, 12, 1050–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagel, S.; Scherag, A.; Schuierer, L.; Hoffmann, R.; Luyt, C.-E.; Pletz, M.W.; Kesselmeier, M.; Weis, S. Effect of antiviral therapy on the outcomes of mechanically ventilated patients with herpes simplex virus detected in the respiratory tract: A systematic review and meta-analysis. Crit. Care 2020, 24, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Luyt, C.-E.; Combes, A.; Deback, C.; Aubriot-Lorton, M.-H.; Nieszkowska, A.; Trouillet, J.-L.; Capron, F.; Agut, H.; Gibert, C.; Chastre, J. Herpes Simplex Virus Lung Infection in Patients Undergoing Prolonged Mechanical Ventilation. Am. J. Respir. Crit. Care Med. 2007, 175, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Zeymer, U.; Neumann, F.-J.; Ferenc, M.; Olbrich, H.-G.; Hausleiter, J.; Richardt, G.; Hennersdorf, M.; Empen, K.; Fuernau, G.; et al. Intraaortic Balloon Support for Myocardial Infarction with Cardiogenic Shock. N. Engl. J. Med. 2012, 367, 1287–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiele, H.; Akin, I.; Sandri, M.; De Waha-Thiele, S.; Meyer-Saraei, R.; Fuernau, G.; Eitel, I.; Nordbeck, P.; Geisler, T.; Landmesser, U.; et al. One-Year Outcomes after PCI Strategies in Cardiogenic Shock. N. Engl. J. Med. 2018, 379, 1699–1710. [Google Scholar] [CrossRef] [PubMed]
- Scherer, C.; Lüsebrink, E.; Kupka, D.; Stocker, T.J.; Stark, K.; Stremmel, C.; Orban, M.; Petzold, T.; Germayer, A.; Mauthe, K.; et al. Long-Term Clinical Outcome of Cardiogenic Shock Patients Undergoing Impella CP Treatment vs. Standard of Care. J. Clin. Med. 2020, 9, 3803. [Google Scholar] [CrossRef] [PubMed]
- Lüsebrink, E.; Stremmel, C.; Stark, K.; Petzold, T.; Hein-Rothweiler, R.; Scherer, C.; Schüttler, D.; Massberg, S.; Orban, M. Percutaneous Decannulation Instead of Surgical Removal for Weaning after Venoarterial Extracorporeal Membrane Oxygenation—A Crossed Perclose ProGlide Closure Device Technique Using a Hemostasis Valve Y Connector. Crit. Care Explor. 2019, 1, e0018. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (Strobe) Statement: Guidelines for Reporting Observational Studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuinet, J.; Garbagnati, A.; Rusca, M.; Yerly, P.; Schneider, A.G.; Kirsch, M.; Liaudet, L. Cardiogenic shock elicits acute inflammation, delayed eosinophilia, and depletion of immune cells in most severe cases. Sci. Rep. 2020, 10, 7639. [Google Scholar] [CrossRef] [PubMed]
- Zhai, R.; Sheu, C.-C.; Su, L.; Gong, M.N.; Tejera, P.; Chen, F.; Wang, Z.; Convery, M.P.; Thompson, B.T.; Christiani, D.C. Serum bilirubin levels on ICU admission are associated with ARDS development and mortality in sepsis. Thorax 2009, 64, 784–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Variables | All Patients n = 837 | No BL n = 656 | No HSV in BL n = 137 | BL with HSV n = 44 | p-Value (No HSV vs. HSV in BL) |
|---|---|---|---|---|---|
| Age, years (SD) | 64.8 (14.9) | 66.1 (14.9) | 59.8 (14.3) | 61.1 (11.5) | 0.58 |
| Male gender, n (%) | 617 (73.7) | 475 (72.4) | 112 (81.8) | 30 (68.2) | 0.09 |
| Body mass index, kg/m2 (IQR) | 26.5 (24.2, 29.7) | 26.3 (24.2, 29.4) | 27.5 (24.8, 30.4) | 25.4 (23.4, 29.7) | 0.11 |
| Previous PCI, n (%) | 252 (30.1) | 191 (29.1) | 41 (29.9) | 20 (45.5) | 0.09 |
| Previous CABG, n (%) | 90 (10.8) | 73 (11.1) | 14 (10.2) | 3 (6.8) | 0.71 |
| Previous stroke, n (%) | 86 (10.3) | 68 (10.4) | 13 (9.5) | 5 (11.4) | 0.94 |
| Known peripheral artery disease, n (%) | 98 (11.7) | 85 (13.0) | 9 (6.6) | 4 (9.1) | 0.82 |
| Smoker, n (%) | 0.69 | ||||
| Active smoker | 203 (24.3) | 146 (22.3) | 45 (32.8) | 12 (27.3) | |
| Former smoker | 152 (18.2) | 125 (19.1) | 19 (13.9) | 8 (18.2) | |
| Never smoked | 482 (57.6) | 482 (57.6) | 73 (53.3) | 24 (54.5) | |
| Hypertension, n (%) | 621 (74.2) | 496 (75.6) | 94 (68.6) | 31 (70.5) | 0.97 |
| Dyslipidemia, n (%) | 369 (44.1) | 287 (43.8) | 62 (45.3) | 20 (45.5) | 1.00 |
| Diabetes mellitus, n (%) | 277 (33.1) | 217 (33.1) | 45 (32.8) | 15 (34.1) | 1.00 |
| Positive cardiovascular family history, n (%) | 508 (60.7) | 396 (60.4) | 81 (59.1) | 31 (70.5) | 0.24 |
| Cardiac arrest, n (%) | 600 (71.7) | 466 (71.0) | 105 (76.6) | 29 (65.9) | 0.22 |
| Out-of-hospital cardiac arrest, n (%) | 302 (36.1) | 249 (38.0) | 40 (29.2) | 13 (29.5) | 1.00 |
| Duration of cardio-pulmonary resuscitation if applicable, minutes (IQR) | 20.0 (12.0, 33.0) | 20.0 (12.0, 35.0) | 20.0 (14.0, 30.0) | 15.0 (10.0, 25.5) | 0.38 |
| Cause of cardiogenic shock, n (%) | 0.66 | ||||
| Primary arrhythmia | 83 (9.9) | 73 (11.1) | 7 (5.1) | 3 (6.8) | |
| Decompensated CMP | 95 (11.4) | 75 (11.4) | 13 (9.5) | 7 (15.9) | |
| Myocarditis | 23 (2.7) | 15 (2.3) | 5 (3.6) | 3 (6.8) | |
| NSTEMI | 205 (24.5) | 163 (24.8) | 35 (25.5) | 7 (15.9) | |
| Other | 83 (9.9) | 64 (9.8) | 14 (10.2) | 5 (11.4) | |
| STEMI | 280 (33.5) | 211 (32.2) | 54 (39.4) | 15 (34.1) | |
| Valvular | 68 (8.1) | 55 (8.4) | 9 (6.6) | 4 (9.1) | |
| Percutaneous coronary intervention, n (%) | 495 (59.1) | 384 (58.5) | 89 (65.0) | 22 (50.0) | 0.17 |
| Variables | All Patients n = 837 | No BL n = 656 | No HSV in BL n = 137 | BL with HSV n = 44 | p-Value (no HSV vs. HSV in BL) |
|---|---|---|---|---|---|
| Duration of ICU stay, days (IQR) | 7.6 (2.2, 13.7) | 5.4 (1.6, 10.3) | 13.3 (8.4, 20.8) | 22.8 (19.0, 28.9) | <0.01 |
| SAPS II score (IQR) | 76.0 (68.0, 84.0) | 76.0 (68.0, 85.0) | 74.0 (66.0, 82.0) | 75.5 (70.0, 83.0) | 0.35 |
| SOFA score on ICU admission (IQR) | 12.0 (10.0, 14.0) | 12.0 (10.0, 14.0) | 13.0 (11.0, 15.0) | 13.0 (11.0, 15.0) | 0.72 |
| Lactate on ICU admission, mmol/L (IQR) | 6.1 (2.6, 9.5) | 5.9 (2.5, 9.5) | 7.1 (2.9, 9.6) | 6.3 (2.6, 9.4) | 0.37 |
| pH on ICU admission (IQR) | 7.3 (7.2, 7.3) | 7.3 (7.2, 7.3) | 7.3 (7.2, 7.3) | 7.3 (7.2, 7.3) | 0.70 |
| Creatinine on ICU admission, mg/dL (IQR) | 1.4 (1.1, 2.0) | 1.4 (1.1, 1.9) | 1.6 (1.3, 1.9) | 1.7 (1.3, 2.4) | 0.22 |
| GFR on ICU admission, mL/min (IQR) | 46.0 (32.5, 60.6) | 47.5 (32.1, 61.8) | 44.9 (34.8, 56.1) | 37.8 (23.8, 55.0) | 0.10 |
| Platelet count on ICU admission, G/L (IQR) | 206.0 (148.0, 259.0) | 206.0 (148.0, 257.0) | 204.0 (145.0, 268.0) | 209.0 (155.5, 268.2) | 0.70 |
| Hemoglobin on ICU admission, g/dL (IQR) | 11.6 (9.7, 13.7) | 11.7 (9.8, 13.7) | 11.8 (9.7, 13.9) | 11.2 (9.3, 12.9) | 0.60 |
| Albumin on ICU admission, g/dL (IQR) | 2.9 (2.5, 3.3) | 3.0 (2.5, 3.4) | 2.8 (2.4, 3.1) | 2.8 (2.5, 3.2) | 0.77 |
| Bilirubin on ICU admission, mg/dL (IQR) | 0.9 (0.5, 1.5) | 0.9 (0.6, 1.4) | 0.8 (0.5, 1.4) | 1.3 (0.9, 2.5) | <0.01 |
| Horowitz index (paO2/FiO2) on admission (IQR) | 157.6 (107.0, 238.8) | 170.7 (114.3, 245.8) | 131.2 (86.8, 197.0) | 129.2 (89.6, 202.8) | 0.93 |
| Average systolic blood pressure, mmHg (IQR) | 108.6 (98.0, 119.9) | 108.7 (96.5, 120.5) | 106.7 (99.6, 114.8) | 109.8 (102.2, 118.0) | 0.09 |
| Average diastolic blood pressure, mmHg (IQR) | 57.8 (52.3, 62.5) | 57.7 (51.6, 62.5) | 58.4 (54.2, 63.1) | 57.2 (54.4, 61.0) | 0.51 |
| Average heart rate, bpm (IQR) | 84.4 (76.1, 92.9) | 84.0 (75.4, 92.7) | 86.7 (78.4, 93.8) | 84.8 (79.0, 95.1) | 0.93 |
| Renal replacement therapy, n (%) | 269 (32.1) | 169 (25.8) | 70 (51.1) | 30 (68.2) | 0.07 |
| Duration of mechanical ventilation in hours, n (%) | 90.0 (19.2, 223.5) | 57.1 (12.0, 159.1) | 255.3 (161.0, 457.5) | 453.8 (326.4, 604.1) | <0.01 |
| Tracheotomy, n (%) | 129 (15.4) | 56 (8.5) | 48 (35.0) | 25 (56.8) | 0.02 |
| Therapeutic hypothermia, n (%) | 270 (32.3) | 201 (30.6) | 55 (40.1) | 14 (31.8) | 0.42 |
| VA-ECMO treatment, n (%) | 312 (37.3) | 207 (31.6) | 80 (58.4) | 25 (56.8) | 0.99 |
| Duration VA-ECMO treatment in days, n (%) | 4.1 (3.0) | 3.3 (2.7) | 5.3 (2.9) | 6.1 (3.5) | 0.23 |
| SAVE score (SD) | −9.0 (5.1) | −9.0 (5.1) | −8.5 (5.1) | −10.6 (4.2) | 0.13 |
| Coaxial left ventricular assist device (Impella) treatment, n (%) | 111 (13.3) | 79 (12.0) | 23 (16.8) | 9 (20.5) | 0.74 |
| IABP treatment, n (%) | 43 (5.1) | 39 (5.9) | 4 (2.9) | 0 (0.0) | 0.58 |
| CPC score on ICU discharge, n (%) | 0.04 | ||||
| CPC 1 | 50 (6.0) | 42 (6.4) | 4 (2.9) | 4 (9.1) | |
| CPC 2 | 121 (14.5) | 109 (16.6) | 9 (6.6) | 3 (6.8) | |
| CPC 3 | 210 (25.1) | 143 (21.8) | 45 (32.8) | 22 (50.0) | |
| CPC 4 | 85 (10.2) | 60 (9.1) | 23 (16.8) | 2 (4.5) | |
| CPC 5 | 371 (44.3) | 302 (46.0) | 56 (40.9) | 13 (29.5) |
| Pathogen Name | Number of Patients (%) |
|---|---|
| Candida albicans | 30 (68.2%) |
| Coagulase-negative staphylococci | 5 (11.4%) |
| Enterococcus faecium | 4 (9.1%) |
| Candida glabrata | 3 (6.8%) |
| Klebsiella pneumoniae | 2 (4.5%) |
| Cytomegalovirus | 1 (2.3%) |
| Staphylococcus hominis | 1 (2.3%) |
| Enterobacter cloacae | 1 (2.3%) |
| Klebsiella oxytoca | 1 (2.3%) |
| Candida tropicalis | 1 (2.3%) |
| Hafnia alvei | 1 (2.3%) |
| Risk Factor | Univariate Analysis | Multivariate Analysis after Feature Selection | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p Value | Hazard Ratio | 95% CI | p Value | |
| Age (years) | 0.998 | 0.969–1.027 | 0.868 | |||
| Male gender | 0.337 | 0.142–0.796 | 0.013 | 0.377 | 0.129–1.086 | 0.070 |
| Hypertension | 1.289 | 0.594–2.916 | 0.529 | 3.240 | 1.146–10.305 | 0.034 |
| Diabetes mellitus | 1.232 | 0.557–2.662 | 0.599 | |||
| Body mass index (per kg/m2) | 0.936 | 0.865–1.002 | 0.080 | 0.934 | 0.852–1.006 | 0.105 |
| First lactate on ICU (per mmol/L) | 0.958 | 0.884–1.028 | 0.260 | |||
| Creatinine on admission (per mL/min) | 1.248 | 0.904–1.734 | 0.173 | |||
| Renal replacement therapy | 1.830 | 0.853–4.111 | 0.129 | |||
| Bilirubin on admission (per mg/dL) | 1.558 | 1.178–2.192 | 0.005 | 2.125 | 1.495–3.216 | <0.001 |
| Duration of mechanical ventilation (per day) | 1.063 | 1.015–1.116 | 0.011 | 1.106 | 1.047–1.176 | 0.001 |
| Horowitz (paO2/FiO2) index on admission (per mmHg/%) | 1.001 | 0.997–1.006 | 0.590 | |||
| Average systolic blood pressure (per mmHg) | 1.026 | 0.996–1.058 | 0.094 | 1.034 | 0.994–1.079 | 0.104 |
| Cardiac arrest | 0.654 | 0.293–1.493 | 0.304 | 0.336 | 0.105–1.031 | 0.059 |
| Out-of-hospital cardiac arrest | 1.442 | 0.634–3.202 | 0.372 | 3.429 | 1.152–10.859 | 0.030 |
| Myocardial infarction | 0.347 | 0.161–0.738 | 0.006 | |||
| VA-ECMO treatment | 0.656 | 0.312–1.389 | 0.267 | |||
| Coaxial left ventricular assist device (Impella) treatment | 1.197 | 0.471–2.884 | 0.695 | 2.596 | 0.789–8.624 | 0.113 |
| Tracheotomy | 1.630 | 0.787–3.438 | 0.192 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scherer, C.; Lüsebrink, E.; Binzenhöfer, L.; Stocker, T.J.; Kupka, D.; Chung, H.P.; Stambollxhiu, E.; Alemic, A.; Kellnar, A.; Deseive, S.; et al. Incidence and Outcome of Patients with Cardiogenic Shock and Detection of Herpes Simplex Virus in the Lower Respiratory Tract. J. Clin. Med. 2022, 11, 2351. https://doi.org/10.3390/jcm11092351
Scherer C, Lüsebrink E, Binzenhöfer L, Stocker TJ, Kupka D, Chung HP, Stambollxhiu E, Alemic A, Kellnar A, Deseive S, et al. Incidence and Outcome of Patients with Cardiogenic Shock and Detection of Herpes Simplex Virus in the Lower Respiratory Tract. Journal of Clinical Medicine. 2022; 11(9):2351. https://doi.org/10.3390/jcm11092351
Chicago/Turabian StyleScherer, Clemens, Enzo Lüsebrink, Leonhard Binzenhöfer, Thomas J. Stocker, Danny Kupka, Hieu Phan Chung, Era Stambollxhiu, Ahmed Alemic, Antonia Kellnar, Simon Deseive, and et al. 2022. "Incidence and Outcome of Patients with Cardiogenic Shock and Detection of Herpes Simplex Virus in the Lower Respiratory Tract" Journal of Clinical Medicine 11, no. 9: 2351. https://doi.org/10.3390/jcm11092351
APA StyleScherer, C., Lüsebrink, E., Binzenhöfer, L., Stocker, T. J., Kupka, D., Chung, H. P., Stambollxhiu, E., Alemic, A., Kellnar, A., Deseive, S., Stark, K., Petzold, T., Hagl, C., Hausleiter, J., Massberg, S., & Orban, M. (2022). Incidence and Outcome of Patients with Cardiogenic Shock and Detection of Herpes Simplex Virus in the Lower Respiratory Tract. Journal of Clinical Medicine, 11(9), 2351. https://doi.org/10.3390/jcm11092351