
Survival in Korean Patients with Frontotemporal Dementia Syndrome: Association with Behavioral Features and Parkinsonism

 , , , , , , ,
, , , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Behavioral Assessment
2.3. Assessment of Parkinsonism and Neurological Examinations
2.4. Statistics
3. Results
3.1. Demographic, Neurological, Behavioral, and Parkinsonian Features
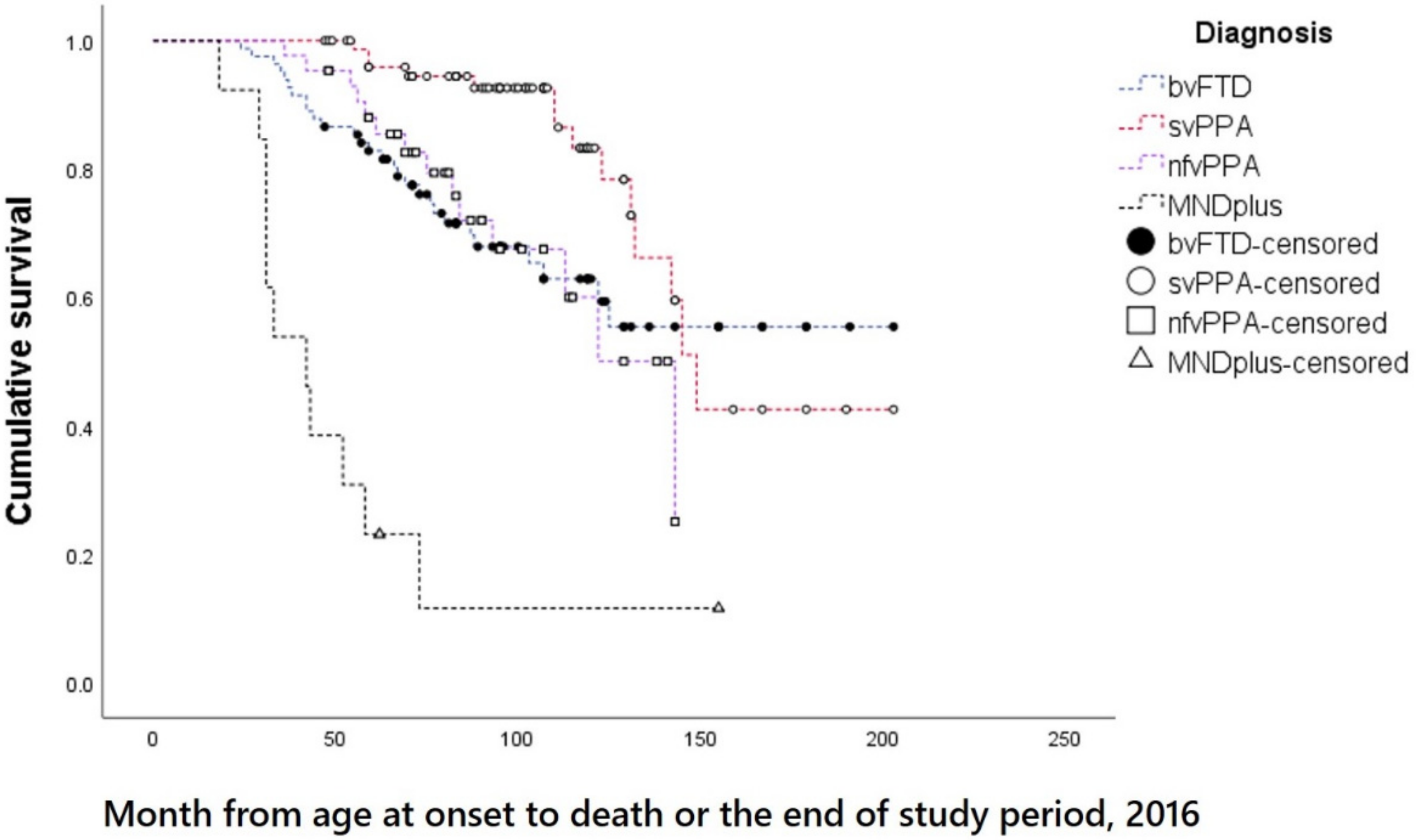
3.2. Survival Times and Its Associated Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kansal, K.; Mareddy, M.; Sloane, K.L.; Minc, A.A.; Rabins, P.V.; McGready, J.B.; Onyike, C.U. Survival in Frontotemporal Dementia Phenotypes: A Meta-Analysis. Dement. Geriatr. Cogn. Disord. 2016, 41, 109–122. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, G.; Sancarlo, D.; Panza, F.; Copetti, M.; Cascavilla, L.; Paris, F.; Seripa, D.; Matera, M.G.; Solfrizzi, V.; Pellegrini, F.; et al. Neuropsychiatric symptoms and functional status in Alzheimer’s disease and vascular dementia patients. Curr. Alzheimer Res. 2012, 9, 759–771. [Google Scholar] [CrossRef] [PubMed]
- Krell-Roesch, J.; Cerhan, L.P.; Machulda, M.M.; Roberts, R.O.; Mielke, M.M.; Knopman, D.S.; Syrjanen, J.A.; Christianson, T.J.; Petersen, R.C.; Geda, Y.E. Functional Activity and Neuropsychiatric Symptoms in Normal Aging and Mild Cognitive Impairment: The Mayo Clinic Study of Aging. Alzheimer Dis. Assoc. Disord. 2019, 33, 68–71. [Google Scholar] [CrossRef] [PubMed]
- van der Linde, R.M.; Matthews, F.E.; Dening, T.; Brayne, C. Patterns and persistence of behavioural and psychological symptoms in those with cognitive impairment: The importance of apathy. Int. J. Geriatr. Psychiatry 2017, 32, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Ahmed, R.M.; D’Mello, M.; Foxe, D.; Kaizik, C.; Kiernan, M.C.; Halliday, G.M.; Piguet, O.; Hodges, J.R. Predictors of survival and progression in behavioural variant frontotemporal dementia. Eur. J. Neurol. 2019, 26, 774–779. [Google Scholar] [CrossRef]
- Park, H.K.; Park, K.H.; Yoon, B.; Lee, J.H.; Choi, S.H.; Joung, J.H.; Yoon, S.J.; Kim, B.C.; Kim, S.H.; Kim, E.J.; et al. Clinical characteristics of parkinsonism in frontotemporal dementia according to subtypes. J. Neurol. Sci. 2017, 372, 51–56. [Google Scholar] [CrossRef]
- Le Ber, I.; Guedj, E.; Gabelle, A.; Verpillat, P.; Volteau, M.; Thomas-Anterion, C.; Decousus, M.; Hannequin, D.; Vera, P.; Lacomblez, L.; et al. Demographic, neurological and behavioural characteristics and brain perfusion SPECT in frontal variant of frontotemporal dementia. Brain 2006, 129, 3051–3065. [Google Scholar] [CrossRef]
- Roberson, E.D.; Hesse, J.H.; Rose, K.D.; Slama, H.; Johnson, J.K.; Yaffe, K.; Forman, M.S.; Miller, C.A.; Trojanowski, J.Q.; Kramer, J.H.; et al. Frontotemporal dementia progresses to death faster than Alzheimer disease. Neurology 2005, 65, 719–725. [Google Scholar] [CrossRef]
- Baizabal-Carvallo, J.F.; Jankovic, J. Parkinsonism, movement disorders and genetics in frontotemporal dementia. Nat. Rev. Neurol. 2016, 12, 175–185. [Google Scholar] [CrossRef]
- Kang, S.J.; Cha, K.R.; Seo, S.W.; Kim, E.A.; Cheong, H.K.; Kim, E.J.; Na, D.L.; Jeong, J.H. Survival in frontotemporal lobar degeneration in a Korean population. Alzheimer Dis. Assoc. Disord. 2010, 24, 339–342. [Google Scholar] [CrossRef]
- Rascovsky, K.; Hodges, J.R.; Knopman, D.; Mendez, M.F.; Kramer, J.H.; Neuhaus, J.; van Swieten, J.C.; Seelaar, H.; Dopper, E.G.; Onyike, C.U.; et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain 2011, 134, 2456–2477. [Google Scholar] [CrossRef] [PubMed]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Yoon, Y.-J.; Oh, J.-H.; Ahn, B.-Y.; Jo, M.-K.; Kim, G.W.; Bak, S.-H.; Park, K.-H.; Chin, J.H.; Na, D.L.; Kim, E.J. Reliability and validity of the Korean version of the Frontal Behavioral Inventory in patients with dementia. J. Korean Neurol. Assoc. 2011. [Google Scholar]
- Kertesz, A.; Davidson, W.; Fox, H. Frontal behavioral inventory: Diagnostic criteria for frontal lobe dementia. Can. J. Neurol. Sci. J. Can. Sci. Neurol. 1997, 24, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Louis, E.D.; Schupf, N.; Manly, J.; Marder, K.; Tang, M.X.; Mayeux, R. Association between mild parkinsonian signs and mild cognitive impairment in a community. Neurology 2005, 64, 1157–1161. [Google Scholar] [CrossRef]
- Graff-Radford, J.; Duffy, J.R.; Strand, E.A.; Josephs, K.A. Parkinsonian motor features distinguish the agrammatic from logopenic variant of primary progressive aphasia. Parkinsonism Relat. Disord. 2012, 18, 890–892. [Google Scholar] [CrossRef]
- Finger, E.C. Frontotemporal Dementias. Contin. Lifelong Learn. Neurol. 2016, 22, 464–489. [Google Scholar] [CrossRef]
- van Smeden, M.; Moons, K.G.; de Groot, J.A.; Collins, G.S.; Altman, D.G.; Eijkemans, M.J.; Reitsma, J.B. Sample size for binary logistic prediction models: Beyond events per variable criteria. Stat. Methods Med. Res. 2019, 28, 2455–2474. [Google Scholar] [CrossRef]
- Bang, J.; Spina, S.; Miller, B.L. Frontotemporal dementia. Lancet 2015, 386, 1672–1682. [Google Scholar] [CrossRef]
- Coyle-Gilchrist, I.T.; Dick, K.M.; Patterson, K.; Rodriquez, P.V.; Wehmann, E.; Wilcox, A.; Lansdall, C.J.; Dawson, K.E.; Wiggins, J.; Mead, S.; et al. Prevalence, characteristics, and survival of frontotemporal lobar degeneration syndromes. Neurology 2016, 86, 1736–1743. [Google Scholar] [CrossRef]
- El-Wahsh, S.; Finger, E.C.; Piguet, O.; Mok, V.; Rohrer, J.D.; Kiernan, M.C.; Ahmed, R.M. Predictors of survival in frontotemporal lobar degeneration syndromes. J. Neurol. Neurosurg. Psychiatry 2021, 92, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Hongisto, K.; Hallikainen, I.; Selander, T.; Tormalehto, S.; Vaatainen, S.; Martikainen, J.; Valimaki, T.; Hartikainen, S.; Suhonen, J.; Koivisto, A.M. Quality of Life in relation to neuropsychiatric symptoms in Alzheimer’s disease: 5-year prospective ALSOVA cohort study. Int. J. Geriatr. Psychiatry 2018, 33, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Benito-Leon, J.; Cubo, E.; Coronell, C.; Group, A.S. Impact of apathy on health-related quality of life in recently diagnosed Parkinson’s disease: The ANIMO study. Mov. Disord. Off. J. Mov. Disord. Soc. 2012, 27, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Ayers, E.; Shapiro, M.; Holtzer, R.; Barzilai, N.; Milman, S.; Verghese, J. Symptoms of Apathy Independently Predict Incident Frailty and Disability in Community-Dwelling Older Adults. J. Clin. Psychiatry 2017, 78, e529–e536. [Google Scholar] [CrossRef]
- Benoit, M.; Andrieu, S.; Lechowski, L.; Gillette-Guyonnet, S.; Robert, P.H.; Vellas, B. Apathy and depression in Alzheimer’s disease are associated with functional deficit and psychotropic prescription. Int. J. Geriatr. Psychiatry 2008, 23, 409–414. [Google Scholar] [CrossRef]
- Eurelings, L.S.; van Dalen, J.W.; Ter Riet, G.; van Charante, E.P.M.; Richard, E.; van Gool, W.A.; Almeida, O.P.; Alexandre, T.S.; Baune, B.T.; Bickel, H.; et al. Apathy and depressive symptoms in older people and incident myocardial infarction, stroke, and mortality: A systematic review and meta-analysis of individual participant data. Clin. Epidemiol. 2018, 10, 363–379. [Google Scholar] [CrossRef]
- Lee, M.; Chodosh, J. Dementia and life expectancy: What do we know? J. Am. Med. Dir. Assoc. 2009, 10, 466–471. [Google Scholar] [CrossRef]
- Sanders, C.L.; Wengreen, H.J.; Schwartz, S.; Behrens, S.J.; Corcoran, C.; Lyketsos, C.G.; Tschanz, J.T.; County, I.C. Nutritional Status is Associated With Severe Dementia and Mortality: The Cache County Dementia Progression Study. Alzheimer Dis. Assoc. Disord. 2018, 32, 298–304. [Google Scholar] [CrossRef]
- Chowdhury, R.; Khan, H.; Heydon, E.; Shroufi, A.; Fahimi, S.; Moore, C.; Stricker, B.; Mendis, S.; Hofman, A.; Mant, J.; et al. Adherence to cardiovascular therapy: A meta-analysis of prevalence and clinical consequences. Eur. Heart J. 2013, 34, 2940–2948. [Google Scholar] [CrossRef]
- Veronese, N.; Stubbs, B.; Volpato, S.; Zuliani, G.; Maggi, S.; Cesari, M.; Lipnicki, D.M.; Smith, L.; Schofield, P.; Firth, J.; et al. Association Between Gait Speed With Mortality, Cardiovascular Disease and Cancer: A Systematic Review and Meta-analysis of Prospective Cohort Studies. J. Am. Med. Dir. Assoc. 2018, 19, 981–988.e7. [Google Scholar] [CrossRef]
- Jakobsen, A.S.; Speyer, H.; Norgaard, H.C.B.; Hjorthoj, C.; Krogh, J.; Mors, O.; Nordentoft, M. Associations between clinical and psychosocial factors and metabolic and cardiovascular risk factors in overweight patients with schizophrenia spectrum disorders—Baseline and two-years findings from the CHANGE trial. Schizophr. Res. 2018, 199, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Hjorthoj, C.; Sturup, A.E.; McGrath, J.J.; Nordentoft, M. Years of potential life lost and life expectancy in schizophrenia: A systematic review and meta-analysis. Lancet Psychiatry 2017, 4, 295–301. [Google Scholar] [CrossRef]
- Correll, C.U.; Solmi, M.; Veronese, N.; Bortolato, B.; Rosson, S.; Santonastaso, P.; Thapa-Chhetri, N.; Fornaro, M.; Gallicchio, D.; Collantoni, E.; et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: A large-scale meta-analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry 2017, 16, 163–180. [Google Scholar] [CrossRef] [PubMed]
- Marin, O. Interneuron dysfunction in psychiatric disorders. Nat. Rev. Neurosci. 2012, 13, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Ferrer, I. Neurons and their dendrites in frontotemporal dementia. Dement. Geriatr. Cogn. Disord. 1999, 10, 55–60. [Google Scholar] [CrossRef]
- Benussi, A.; Alberici, A.; Buratti, E.; Ghidoni, R.; Gardoni, F.; Di Luca, M.; Padovani, A.; Borroni, B. Toward a Glutamate Hypothesis of Frontotemporal Dementia. Front. Neurosci. 2019, 13, 304. [Google Scholar] [CrossRef]
- Glasmacher, S.A.; Leigh, P.N.; Saha, R.A. Predictors of survival in progressive supranuclear palsy and multiple system atrophy: A systematic review and meta-analysis. J. Neurol. Neurosurg. Psychiatry 2017, 88, 402–411. [Google Scholar] [CrossRef]
- Wenning, G.K.; Litvan, I.; Jankovic, J.; Granata, R.; Mangone, C.A.; McKee, A.; Poewe, W.; Jellinger, K.; Chaudhuri, K.R.; D’Olhaberriague, L.; et al. Natural history and survival of 14 patients with corticobasal degeneration confirmed at postmortem examination. J. Neurol. Neurosurg. Psychiatry 1998, 64, 184–189. [Google Scholar] [CrossRef]
- Macleod, A.D.; Taylor, K.S.; Counsell, C.E. Mortality in Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. Off. J. Mov. Disord. Soc. 2014, 29, 1615–1622. [Google Scholar] [CrossRef]
- Oosterveld, L.P.; Allen, J.C., Jr.; Reinoso, G.; Seah, S.H.; Tay, K.Y.; Au, W.L.; Tan, L.C. Prognostic factors for early mortality in Parkinson’s disease. Parkinsonism Relat. Disord. 2015, 21, 226–230. [Google Scholar] [CrossRef]
- Lo, R.Y.; Tanner, C.M.; Albers, K.B.; Leimpeter, A.D.; Fross, R.D.; Bernstein, A.L.; McGuire, V.; Quesenberry, C.P.; Nelson, L.M.; Eeden, S.K.V.D. Clinical features in early Parkinson disease and survival. Arch. Neurol. 2009, 66, 1353–1358. [Google Scholar] [CrossRef] [PubMed]
- Selikhova, M.; Williams, D.R.; Kempster, P.A.; Holton, J.L.; Revesz, T.; Lees, A.J. A clinico-pathological study of subtypes in Parkinson’s disease. Brain 2009, 132, 2947–2957. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Gong, D.D.; Man, C.F.; Fan, Y. Parkinson’s disease and risk of mortality: Meta-analysis and systematic review. Acta Neurol. Scand. 2014, 129, 71–79. [Google Scholar] [CrossRef]
- Williams, D.R.; Litvan, I. Parkinsonian syndromes. Continuum 2013, 19, 1189–1212. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.E.; Rabinovici, G.D.; Mayo, M.C.; Wilson, S.M.; Seeley, W.W.; DeArmond, S.J.; Huang, E.J.; Trojanowski, J.Q.; Growdon, M.E.; Jang, J.Y.; et al. Clinicopathological correlations in corticobasal degeneration. Ann. Neurol. 2011, 70, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.J.; Carter, F.L.; Altman, K.W. Relationship between Dysarthria and Oral-Oropharyngeal Dysphagia: The present evidence. Ear Nose Throat J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Duffy, J.R.; Strand, E.A.; Josephs, K.A. Motor Speech Disorders Associated with Primary Progressive Aphasia. Aphasiology 2014, 28, 1004–1017. [Google Scholar] [CrossRef]
- Alster, P.; Migda, B.; Madetko, N.; Duszynska-Was, K.; Drzewinska, A.; Charzynska, I.; Starczynski, M.; Szepelska, A.; Krolicki, L.; Friedman, A. The Role of Frontal Assessment Battery and Frontal Lobe Single-Photon Emission Computed Tomography in the Differential Diagnosis of Progressive Supranuclear Palsy Variants and Corticobasal Syndrome-A Pilot Study. Front. Neurol. 2021, 12, 630153. [Google Scholar] [CrossRef]
- Guasp, M.; Molina-Porcel, L.; Painous, C.; Caballol, N.; Camara, A.; Perez-Soriano, A.; Sanchez-Gomez, A.; Garrido, A.; Munoz, E.; Marti, M.J.; et al. Association of PSP phenotypes with survival: A brain-bank study. Parkinsonism Relat. Disord. 2021, 84, 77–81. [Google Scholar] [CrossRef]
- Santos-Santos, M.A.; Mandelli, M.L.; Binney, R.J.; Ogar, J.; Wilson, S.M.; Henry, M.L.; Hubbard, H.I.; Meese, M.; Attygalle, S.; Rosenberg, L.; et al. Features of Patients With Nonfluent/Agrammatic Primary Progressive Aphasia With Underlying Progressive Supranuclear Palsy Pathology or Corticobasal Degeneration. JAMA Neurol. 2016, 73, 733–742. [Google Scholar] [CrossRef]
- Ogar, J.M.; Dronkers, N.F.; Brambati, S.M.; Miller, B.L.; Gorno-Tempini, M.L. Progressive nonfluent aphasia and its characteristic motor speech deficits. Alzheimer Dis. Assoc. Disord. 2007, 21, S23–S30. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | bvFTD | svPPA | nfvPPA | FTD-MND | p | |
|---|---|---|---|---|---|---|
| Subjects/death, n | 216/67 | 82/28 | 78/14 | 43/14 | 13/11 | |
| Male (%) | 109 (50.5) | 44 (53.7) | 33 (42.3) | 25 (58.1) | 7 (53.8) | 0.323 |
| Education (y) | 9.7 ± 5.1 | 9.8 ± 5.1 | 9.6 ± 4.9 | 10.4 ± 5.7 | 7.9 ± 4.3 | 0.487 |
| Age at onset (y) | 62.6 ± 9.3 | 62.1 ± 10.6 | 62.5 ± 7.4 | 64.7 ± 9.2 | 60.5 ± 10.5 | 0.371 |
| Age at diagnosis(y) | 65.6 ± 8.9 | 65.1 ± 10.2 | 65.8 ± 7.4 | 67.1 ± 8.8 | 62.9 ± 10.0 | 0.447 |
| Age at assessment (y) | 65.9 ± 8.9 | 65.3 ± 10.2 | 66.3 ± 7.3 | 67.3 ± 8.8 | 63.1 ± 9.7 | 0.400 |
| Onset-assessment interval (months) | 39.2 ± 26.8 | 39.5 ± 28.6 | 44.9 ± 27.9 | 31.1 ± 20.6 c | 29.2 ± 18.1 | 0.024 |
| MMSE | 19.0 (7.7) | 19.4 (6.8) | 18.3 (8.8) | 20.6 (7.3) | 14.9 (6.7) | 0.109 |
| CDR-SB | 5.7 (4.3) | 6.9 (4.2) | 5.4 (4.4) | 3.5 (3.2) a,b | 7.8 (4.8) | <0.001 |
| FTD CDR-SB | 11.2 (6.4) | 9.5 (5.2) | 8.0 (5.5) | 5.7 (3.9) a,b | 11.2 (6.4) | <0.001 |
| Diabetes, n (%) | 37 (17.4) | 21 (26.6) d,g | 10 (12.8) | 6 (14.0) | 0 (0) | 0.031 |
| Hypertension | 79 (36.9) | 33 (41.3) | 22 (28.2) | 17 (39.5) | 7 (53.8) | 0.178 |
| Hyperlipidemia | 30 (14.0) | 14 (17.5) | 9 (11.5) | 5 (11.6) | 2 (15.4) | 0.699 |
| Heart disease | 20 (9.4) | 11 (13.9) | 7 (9.0) | 2 (4.7) | 0 (0) | 0.221 |
| Stroke | 6 (2.8) | 3 (3.8) | 1 (1.3) | 1 (2.3) | 1 (7.7) | 0.549 |
| Cancer | 14 (6.6) | 4 (5.1) | 3 (3.8) | 6 (14.0) | 1 (7.7) | 0.166 |
| Neurological Examination (n = 145) | ||||||
| Dysarthria | 16 (11) | 3 (5.3) | 0 (0) | 7 (22.6) a,c | 6 (66.7) b,f,g | <0.001 |
| EOM limitation | 3 (2.1) | 2 (3.5) | 0 (0) | 1 (3.2) | 0 (0) | 0.546 |
| Facial palsy | 1 (0.7) | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 1.000 |
| Motor weakness | 8 (5.5) | 2 (3.5) | 1 (2.1) | 0 (0) | 5 (55.6) b,f,g | <0.001 |
| Sensory loss | 1 (0.7) | 1 (1.8) | 0 (0) | 0 (0) | 0 (0) | 1.000 |
| Increased DTR | 9 (6.2) | 5 (8.8) | 1 (2.1) | 1 (3.2) | 2 (22.2) | 0.090 |
| Decreased DTR | 23 (15.9) | 9 (15.8) | 6 (12.5) | 4 (12.9) | 4 (44.4) | 0.148 |
| Babinski/Chaddock | 13 (9.0) | 6 (10.5) | 5 (10.4) | 1 (3.2) | 1 (11.1) | 0.588 |
| Median survival from onset to death (y, 95% CI) | 12.1 | NA | 12.4 ± 0.4 d,e,f (11.6–13.3) | 10.2 ± 0.9 (8.4–11.9) | 3.5 ± 0.6 b,g (2.3–4.7) | <0.001 |
| Median survival from diagnosis to death (y, 95% CI) | 8.8 ± 0.7 (7.3–10.2) | NA | 9.0 ± 0.8 d,e,f (7.4–10.6) | 8.8 ± 0 (NA) | 1.3 ± 0.3 b,g (0.7–1.9) | <0.001 |
| Total (n = 216) | bvFTD (n = 82) | svPPA (n = 78) | nfvPPA (n = 43) | FTD-MND (n = 13) | p | |
|---|---|---|---|---|---|---|
| FBI total † | 26.6 ± 15.2 | 32.5 ± 13.1 a,d | 25.9 ± 16.1 b | 16.6 ± 11.9 | 28.7 ± 14.5 e | <0.001 |
| FBI_negative | 17.8 ± 9.2 | 20.5 ± 8.4 d | 17.5 ± 9.6 b | 12.5 ± 8.0 | 20.1 ±9.4 e | <0.001 |
| FBI_positive | 8.9 ± 7.5 | 12.0 ± 7.3 a,d | 8.4 ± 7.9 b | 4.1 ± 4.7 | 8.6 ± 5.7 | <0.001 |
| Presence of Parkisonism, n (%) * | 104 (51.5) | 41 (53.9) | 28 (38.4) c | 25 (61.0) | 10 (83.3) | 0.009 |
| UPDRS total score | 7.0 (11.6) | 8.4 (12.5) | 4.1 (10.1) | 9.3 (12.8) | 8.2 (6.1) | 0.055 |
| UPDRS Speech/facial | 1.0 ± 1.5 | 1.1 ± 1.5 | 0.4 ± 1.2 a,b,c | 1.5 ± 1.6 | 1.8 ± 1.9 | <0.001 |
| UPDRS UPDRS Tremor | 0.5 ± 1.3 | 0.7 ± 1.8 | 0.2 ± 0.6 | 0.5 ± 0.9 | 0.9 ± 2.1 | 0.102 |
| UPDRS Rigidity | 1.1 ± 2.8 | 1.6 ± 3.3 | 0.7 ± 2.5 | 1.2 ± 2.4 | 0.3 ± 1.2 | 0.221 |
| UPDRS bradykinesia | 3.4 ± 5.6 | 3.7 ± 5.6 | 2.0 ± 4.4 | 5.0 ± 7.1 b | 4.9 ± 4.5 | 0.026 |
| UPDRS Gait/posture | 1.0 ± 2.3 | 1.2 ± 2.4 | 0.7 ± 2.3 | 1.2 ± 2.5 | 0.3 ± 0.6 | 0.386 |
| Total | bvFTD | svPPA | nfvPPA | FTD-MND | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | |
| FBI total | 0.008 | 1.020 (1.005–1.035) | 0.012 | 1.037 (1.008–1.067) | n.s | n.s | n.s | n.s | n.s | n.s |
| FBI_negative | 0.004 | 1.041 (1.013–1.070) | 0.003 | 1.110 (1.037–1.187) | n.s | n.s | n.s | n.s | n.s | n.s |
| FBI_positive | n.s | n.s | n.s | n.s | n.s | n.s | n.s | n.s | n.s | n.s |
| UPDRS speech/facial | 0.024 | 1.161 (1.020–1.322) | 0.032 | 1.324 (1.025–1.711) | n.s | n.s | n.s | n.s | n.s | n.s |
| UPDRS tremor | n.s | n.s | n.s | n.s | n.s | n.s | n.s | n.s | n.s | n.s |
| UPDRS rigidity | n.s | n.s | 0.004 | 1.171 (1.053–1.302) | n.s | n.s | n.s | n.s | n.s | n.s |
| UPDRS bradykinesia | 0.022 | 1.041 (1.006–1.077) | <0.001 | 1.140 (1.064–1.222) | n.s | n.s | n.s | n.s | n.s | n.s |
| UPDRS gait/posture | n.s | n.s | <0.001 | 1.245 (1.102–1.407) | n.s | n.s | n.s | n.s | n.s | n.s |
| Dysarthria | <0.001 | 5.413 (2.788–10.507) | n.s | n.s | NA | NA | 0.030 | 7.593 (1.221–47.226) | NA | NA |
| Decreased DTR | n.s | n.s | n.s | n.s | n.s | n.s | n.s | n.s | n.s | n.s |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, N.-Y.; Park, K.H.; Seo, S.W.; Kim, H.J.; Roh, J.H.; Lee, J.-H.; Park, K.W.; Kwon, J.C.; Jeong, J.H.; Yoon, S.J.; et al. Survival in Korean Patients with Frontotemporal Dementia Syndrome: Association with Behavioral Features and Parkinsonism. J. Clin. Med. 2022, 11, 2260. https://doi.org/10.3390/jcm11082260
Jung N-Y, Park KH, Seo SW, Kim HJ, Roh JH, Lee J-H, Park KW, Kwon JC, Jeong JH, Yoon SJ, et al. Survival in Korean Patients with Frontotemporal Dementia Syndrome: Association with Behavioral Features and Parkinsonism. Journal of Clinical Medicine. 2022; 11(8):2260. https://doi.org/10.3390/jcm11082260
Chicago/Turabian StyleJung, Na-Yeon, Kee Hyung Park, Sang Won Seo, Hee Jin Kim, Jee Hoon Roh, Jae-Hong Lee, Kyung Won Park, Jay C. Kwon, Jee Hyang Jeong, Soo Jin Yoon, and et al. 2022. "Survival in Korean Patients with Frontotemporal Dementia Syndrome: Association with Behavioral Features and Parkinsonism" Journal of Clinical Medicine 11, no. 8: 2260. https://doi.org/10.3390/jcm11082260
APA StyleJung, N.-Y., Park, K. H., Seo, S. W., Kim, H. J., Roh, J. H., Lee, J.-H., Park, K. W., Kwon, J. C., Jeong, J. H., Yoon, S. J., Kim, B. C., Park, Y. H., Kim, S., Jang, J.-W., Youn, Y. C., Yang, D. W., Choi, S. H., Na, D. L., & Kim, E.-J. (2022). Survival in Korean Patients with Frontotemporal Dementia Syndrome: Association with Behavioral Features and Parkinsonism. Journal of Clinical Medicine, 11(8), 2260. https://doi.org/10.3390/jcm11082260