
Alexithymia and Psychopathological Manifestations Centered on the Body: Somatization and Self-Harm


Abstract
1. Introduction
- (a)
- To obtain information on the three groups’ psychopathological correlates in order to investigate their differences and similarities. Based on literature we expect differences between the three groups: in the NSSI + SSD group we expect more severe internalizing and externalizing psychopathology than in the other two groups, furthermore we assume differences between NSSI group and SSD group, in particular that NSSI correlate more with mood disorders [27,30] and SSD correlate more closely than NSSI with anxiety [31];
- (b)
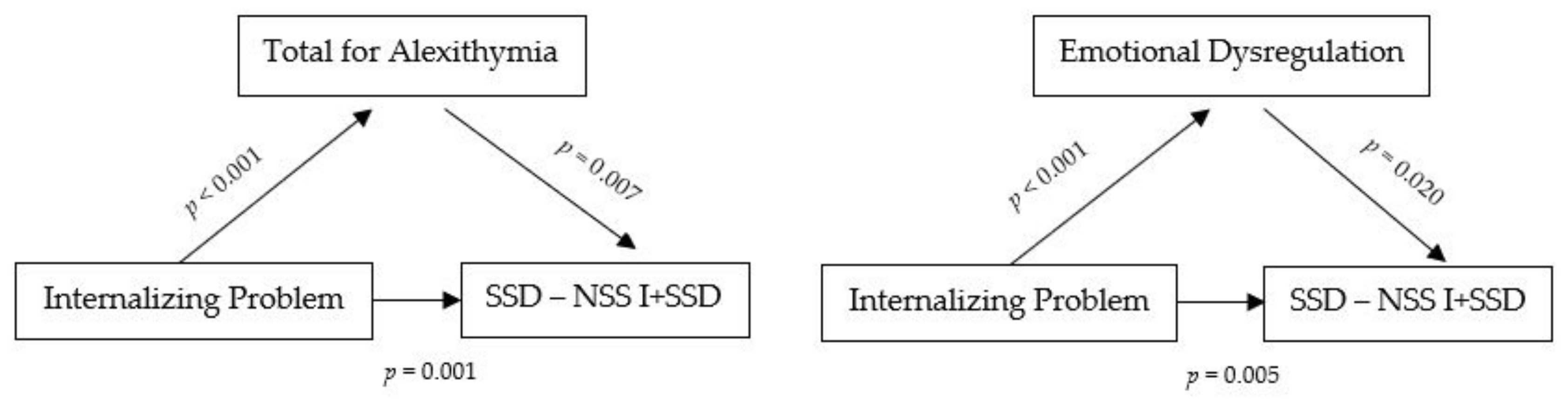
- To further investigate the mediation role of alexithymia and emotional dysregulation in NSSI and SSD related to internalizing problems. Our hypothesis emerging from the literature suggests that emotional dysregulation may play a mediating role in the development of self-harm, particularly in individuals with mood disorders, interpersonal problems, history of trauma, and physical and emotional abuse [14,32,33,34]. Furthermore, we hypothesise that alexithymia represents mediating factor in the development of self-harm in the context of internalizing problems, particularly in situations of exposure to traumatic experiences and bullying, according to Norman and Borrill [11].
2. Materials and Methods
3. Results
3.1. Psychopathological Characteristics
3.2. Impairments in Emotion Regulation
3.3. Alexithymia in the Three Groups
3.4. Mediation Role of Alexithymia and Emotional Dysregulation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brunner, R.; Kaess, M.; Parzer, P.; Fischer, G.; Carli, V.; Hoven, C.; Wasserman, C.; Sarchiapone, M.; Resch, F.; Apter, A.; et al. Life-time prevalence and psychosocial correlates of adolescent direct self-injurious behavior: A comparative study of findings in 11 European countries. J. Child Psychol. Psychiatry 2014, 55, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K. Self-Injury. Annu. Rev. Clin. Psychol. 2010, 6, 339–363. [Google Scholar] [CrossRef] [PubMed]
- BrauschPeter, A.M.; Gutierrez, P. Differences in Non-Suicidal Self-Injury and Suicide Attempts in Adolescents. J. Youth Adolesc. 2010, 39, 233–242. [Google Scholar] [CrossRef]
- Grandclerc, S.; De Labrouhe, D.; Spodenkiewicz, M.; Lachal, J.; Moro, M.-R. Relations between Nonsuicidal Self-Injury and Suicidal Behavior in Adolescence: A Systematic Review. PLoS ONE 2016, 11, e0153760. [Google Scholar] [CrossRef]
- Hamza, C.A.; Stewart, S.L.; Willoughby, T. Examining the link between nonsuicidal self-injury and suicidal behavior: A review of the literature and an integrated model. Clin. Psychol. Rev. 2012, 32, 482–495. [Google Scholar] [CrossRef]
- Hawton, K.; Saunders, K.E.A.; O’Connor, R.C. Self-harm and suicide in adolescents. Lancet 2012, 379, 2373–2382. [Google Scholar] [CrossRef]
- Gyori, D.; Balazs, J. Nonsuicidal Self-Injury and Perfectionism: A Systematic Review. Front. Psychiatry 2021, 12, 1076. [Google Scholar] [CrossRef]
- Iskric, A.; Ceniti, A.K.; Bergmans, Y.; McInerney, S.; Rizvi, S.J. Alexithymia and self-harm: A review of nonsuicidal self-injury, suicidal ideation, and suicide attempts. Psychiatry Res. 2020, 288, 112920. [Google Scholar] [CrossRef]
- Burke, T.A.; Connolly, S.L.; Hamilton, J.L.; Stange, J.P.; Abramson, L.Y.; Alloy, L.B. Cognitive Risk and Protective Factors for Suicidal Ideation: A Two Year Longitudinal Study in Adolescence. J. Abnorm. Child Psychol. 2015, 44, 1145–1160. [Google Scholar] [CrossRef]
- Gatta, M.; Sisti, M.; Sudati, L.; Miscioscia, M.; Simonelli, A. The Lausanne Trilogue Play within the outcome evaluation in infant mental health: A preliminary report. Res. Psychother. Psychopathol. Process Outcome 2016, 19, 1. [Google Scholar] [CrossRef][Green Version]
- Norman, H.; Borrill, J. The relationship between self-harm and alexithymia. Scand. J. Psychol. 2015, 56, 405–419. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Rasmussen, S.; Hawton, K. Predicting depression, anxiety and self-harm in adolescents: The role of perfectionism and acute life stress. Behav. Res. Ther. 2010, 48, 52–59. [Google Scholar] [CrossRef]
- Quiñones, V.; Jurska, J.; Fener, E.; Miranda, R. Active and Passive Problem Solving: Moderating Role in the Relation between Depressive Symptoms and Future Suicidal Ideation Varies by Suicide Attempt History. J. Clin. Psychol. 2015, 71, 402–412. [Google Scholar] [CrossRef]
- Paulus, F.W.; Ohmann, S.; Möhler, E.; Plener, P.; Popow, C. Emotional Dysregulation in Children and Adolescents with Psychiatric Disorders. A Narrative Review. Front. Psychiatry 2021, 12, 628252. [Google Scholar] [CrossRef]
- De Klerk, S.; van Noorden, M.S.; van Giezen, A.E.; Spinhoven, P.; Hollander-Gijsman, M.D.; Giltay, E.; Speckens, A.; Zitman, F.G. Prevalence and correlates of lifetime deliberate self-harm and suicidal ideation in naturalistic outpatients: The Leiden Routine Outcome Monitoring study. J. Affect. Disord. 2011, 133, 257–264. [Google Scholar] [CrossRef]
- Gratz, K.L.; Roemer, L. Multidimensional Assessment of Emotion Regulation and Dysregulation: Development, Factor Structure, and Initial Validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Nock, M.K.; Prinstein, M.J. A Functional Approach to the Assessment of Self-Mutilative Behavior. J. Consult. Clin. Psychol. 2004, 72, 885–890. [Google Scholar] [CrossRef]
- Cipriano, A.; Cella, S.; Cotrufo, P. Nonsuicidal Self-injury: A Systematic Review. Front. Psychol. 2017, 8, 1946. [Google Scholar] [CrossRef]
- Nock, M.K.; Joiner, T.E., Jr.; Gordon, K.H.; Lloyd-Richardson, E.; Prinstein, M.J. Non-suicidal self-injury among adolescents: Diagnostic correlates and relation to suicide attempts. Psychiatry Res. 2006, 144, 65–72. [Google Scholar] [CrossRef]
- Glenn, C.R.; Klonsky, E.D. Nonsuicidal Self-Injury Disorder: An Empirical Investigation in Adolescent Psychiatric Patients. J. Clin. Child Adolesc. Psychol. 2013, 42, 496–507. [Google Scholar] [CrossRef]
- Muehlenkamp, J.J.; Claes, L.; Smits, D.; Peat, C.M.; Vandereycken, W. Non-suicidal self-injury in eating disordered patients: A test of a conceptual model. Psychiatry Res. 2011, 188, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Turner, B.J.; Yiu, A.; Layden, B.K.; Claes, L.; Zaitsoff, S.; Chapman, A.L. Temporal Associations between Disordered Eating and Nonsuicidal Self-Injury: Examining Symptom Overlap Over 1 Year. Behav. Ther. 2015, 46, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Houston, K.; Haw, C.; Townsend, E.; Hawton, K. General practitioner contacts with patients before and after de-liberate self harm. Br. J. Gen. Pract. 2003, 53, 365–370. [Google Scholar] [PubMed]
- Idenfors, H.; Strömsten, L.M.; Renberg, E.S. Are non-psychiatric hospitalisations before self-harm associated with an increased risk for suicide among young people? J. Psychosom. Res. 2019, 120, 96–101. [Google Scholar] [CrossRef]
- Joiner, T.E.; Pfaff, J.J.; Acres, J.G. Characteristics of suicidal adolescents and young adults presenting to primary care with non-suicidal (indeed non-psychological) complaints. Eur. J. Public Health 2002, 12, 177–179. [Google Scholar] [CrossRef]
- Güleç, M.Y.; Ýnanç, L.; Yanartaþ, Ö.; Üzer, A.; Gulec, H. Predictors of suicide in patients with conversion disorder. Compr. Psychiatry 2014, 55, 457–462. [Google Scholar] [CrossRef]
- Raffagnato, A.; Angelico, C.; Valentini, P.; Miscioscia, M.; Gatta, M. Using the Body When There Are No Words for Feelings: Alexithymia and Somatization in Self-Harming Adolescents. Front. Psychiatry 2020, 11, 262. [Google Scholar] [CrossRef]
- Gatta, M.; Spitaleri, C.; Balottin, L.; Spoto, A.; Mangano, S.; Battistella, P. Alexithymic characteristics in pediatric patients with primary headache: A comparison between migraine and tension-type headache. J. Headache Pain 2015, 16, 98. [Google Scholar] [CrossRef][Green Version]
- Lanzara, R.; Conti, C.; Camelio, M.; Cannizzaro, P.; Lalli, V.; Bellomo, R.G.; Saggini, R.; Porcelli, P. Alexithymia and Somatization in Chronic Pain Patients: A Sequential Mediation Model. Front. Psychol. 2020, 11, 545881. [Google Scholar] [CrossRef]
- Rodav, O.; Levy, S.; Hamdan, S. Clinical characteristics and functions of non-suicide self-injury in youth. Eur. Psychiatry 2014, 29, 503–508. [Google Scholar] [CrossRef]
- Ginsburg, G.S.; Riddle, M.A.; Davies, M. Somatic Symptoms in Children and Adolescents with Anxiety Disorders. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 1179–1187. [Google Scholar] [CrossRef]
- Kranzler, A.; Fehling, K.B.; Anestis, M.D.; Selby, E.A. Emotional Dysregulation, Internalizing Symptoms, and Self-Injurious and Suicidal Behavior: Structural Equation Modeling Analysis. Death Stud. 2016, 40, 358–366. [Google Scholar] [CrossRef]
- Titelius, E.N.; Cook, E.; Spas, J.; Orchowski, L.; Kivisto, K.; McManama O’Brien, K.H.; Frazier, E.; Wolff, J.C.; Dickstein, D.P.; Kim, K.L.; et al. Emotion dysregulation mediates the relationship between child maltreatment and non-suicidal self-injury. J. Aggress. Maltreat. Trauma 2018, 27, 323–331. [Google Scholar] [CrossRef]
- Tamas, Z.; Kovacs, M.; Gentzler, A.L.; Tepper, P.; Gádoros, J.; Kiss, E.; Kapornai, K.; Vetró, A. The relations of tem-perament and emotion self- regulation with suicidal behaviors in a clinical sample of depressed children in Hungary. J. Abnorm. Child Psychol. 2007, 35, 640–652. [Google Scholar] [CrossRef]
- Parker, J.D.A.; Bagby, R.M.; Taylor, G.J.; Endler, N.S.; Schmitz, P. Factorial validity of the 20-item Toronto Alexithymia Scale. Eur. J. Pers. 1993, 7, 221–232. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Rescorla, L.A. Manual for ASEBA School-Age Forms and Profiles; University of Vermont, Research Center for Children, Youth and Families: Burlington, VT, USA, 2001. [Google Scholar]
- Althoff, R.R.; Rettew, D.C.; Ayer, L.A.; Hudziak, J.J. Cross-informant agreement of the Dysregulation Profile of the Child Behavior Checklist. Psychiatry Res. 2010, 178, 550–555. [Google Scholar] [CrossRef]
- Bellina, M.; Bianchi, V.; Bonivento, C.; Brambilla, P.; Busti, C.S.; Colombo, P.; Fornasari, L.; Garzitto, M.; Molteni, M.; Nobile, M. Deficit di regolazione emotiva in età evolutiva: Analisi dei profili di funzionamento in un campione clinico italiano. Quad. DI Psicoter. Cogn. 2015, 1, 103–115. [Google Scholar] [CrossRef]
- Biederman, J.; Petty, C.R.; Monuteaux, M.C.; Evans, M.; Parcell, T.; Faraone, S. The Child Behavior Checklist-Pediatric Bipolar Disorder Profile Predicts a Subsequent Diagnosis of Bipolar Disorder and Associated Impairments in ADHD Youth Growing Up. J. Clin. Psychiatry 2009, 70, 732–740. [Google Scholar] [CrossRef]
- Spencer, T.J.; Faraone, S.V.; Surman, C.B.H.; Petty, C.; Clarke, A.; Batchelder, H.; Wozniak, J.; Biederman, J. To-ward defining deficient emotional self regulation in children with attention-deficit/hyperactivity disorder using the Child Behavior Checklist: A controlled study. Postgrad. Med. 2011, 123, 50–59. [Google Scholar] [CrossRef]
- Zanus, C.; Battistutta, S.; Aliverti, R.; Monasta, L.; Montico, M.; Ronfani, L.; Carrozzi, M. High-school students and self-injurious thoughts and behaviours: Clues of emotion dysregulation. Ital. J. Pediatr. 2021, 47, 1–14. [Google Scholar] [CrossRef]
- Baetens, I.; Claes, L.; Muehlenkamp, J.; Grietens, H.; Onghena, P. Non-Suicidal and Suicidal Self-Injurious Behavior among Flemish Adolescents: A Web-Survey. Arch. Suicide Res. 2011, 15, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Parolin, M.; Miscioscia, M.; De Carli, P.; Cristofalo, P.; Gatta, M.; Simonelli, A. Alexithymia in Young Adults with Substance Use Disorders: Critical Issues About Specificity and Treatment Predictivity. Front. Psychol. 2018, 9, 645. [Google Scholar] [CrossRef] [PubMed]
- Muehlenkamp, J.J.; Gutierrez, P. Risk for Suicide Attempts Among Adolescents Who Engage in Non-Suicidal Self-Injury. Arch. Suicide Res. 2007, 11, 69–82. [Google Scholar] [CrossRef] [PubMed]
- Gatta, M.; Dal Santo, F.; Rago, A.; Spoto, A.; Battistella, P.A. Alexithymia, impulsiveness, and psychopathology in nonsuicidal self-injured adolescents. Neuropsychiatr. Dis. Treat. 2016, 12, 2307–2317. [Google Scholar] [CrossRef]
- Andover, M.S.; Morris, B.W. Expanding and Clarifying the Role of Emotion Regulation in Nonsuicidal Self-Injury. Can. J. Psychiatry 2014, 59, 569–575. [Google Scholar] [CrossRef]
- Taylor, G.J.; Bagby, R.M.; Parker, J.D.A. Disorders of affect regulation: Alexithymia in medical and psychiatric illness. Clin. Psychol. Psychother. 1997, 7, 240. [Google Scholar] [CrossRef]
- Martin, J.B.; Pihl, R. The Stress-Alexithymia Hypothesis: Theoretical and Empirical Considerations. Psychother. Psychosom. 1985, 43, 169–176. [Google Scholar] [CrossRef]
- Davoodi, E.; Wen, A.; Dobson, K.; Noorbala, A.A.; Mohammadi, A.; Farahmand, Z. Emotion Regulation Strategies in Depression and Somatization Disorder. Psychol. Rep. 2018, 122, 2119–2136. [Google Scholar] [CrossRef]
- Cerutti, R.; Zuffiano, A.; Spensieri, V. The Role of Difficulty in Identifying and Describing Feelings in Non-Suicidal Self-Injury Behavior (NSSI): Associations with Perceived Attachment Quality, Stressful Life Events, and Suicidal Ideation. Front. Psychol. 2018, 9, 318. [Google Scholar] [CrossRef]
- Greene, D.; Boyes, M.; Hasking, P. The associations between alexithymia and both non-suicidal self-injury and risky drinking: A systematic review and meta-analysis. J. Affect. Disord. 2020, 260, 140–166. [Google Scholar] [CrossRef]
- Kämpfer, N.; Staufenbiel, S.; Wegener, I.; Rambau, S.; Urbach, A.S.; Mücke, M.; Geiser, F.; Conrad, R. Suicidality in patients with somatoform disorder—The speechless expression of anger? Psychiatry Res. 2016, 246, 485–491. [Google Scholar] [CrossRef]
- Gatta, M.; Miscioscia, M.; Sisti, M.; Comis, I.; Battistella, P.A. Interactive Family Dynamics and Non-suicidal Self-Injury in Psychiatric Adolescent Patients: A Single Case Study. Front. Psychol. 2017, 8, 46. [Google Scholar] [CrossRef]
- Miscioscia, M.; Angelico, C.; Raffagnato, A.; Gatta, M. Psychopathological and Interactive-Relational Characteristics in Non-Suicidal Self-Injury Adolescent Outpatients. J. Clin. Med. 2022, 11, 1218. [Google Scholar] [CrossRef]


{kind=link}
| YSR | |||||
|---|---|---|---|---|---|
| SSD | NSSI | NSSI + SSD | ANOVA | ||
| Activities | M(SD) | 40.6 (10.28) | 36.3 (9.12) | 38.1 (9.55) | F = 2.51; p = 0.086 |
| Social | M(SD) | 44.2 (9.87) | 39.5 (11.20) | 39.0 (8.77) | F = 5.22; p = 0.007 |
| Total competences | M(SD) | 39.6 (9.42) | 34.7 (11.01) | 35.3 (8.88) | F = 4.11; p = 0.019 |
| Internalizing Problems | M(SD) | 64.2 (8.61) | 63.3 (8.97) | 73.8 (9.78) | F = 25.26; p < 0.001 |
| Externalizing Problems | M(SD) | 55.2 (8.48) | 55.1 (8.63) | 60.9 (9.66) | F = 8.53; p < 0.001 |
| Total Problems | M(SD) | 60.5 (7.69) | 60.7 (8.21) | 69.7 (8.26) | F = 28.34; p < 0.001 |
| Anxious/Depressed | M(SD) | 63.4 (9.44) | 64.9 (8.79) | 73.8 (12.98) | F = 16.11; p < 0.001 |
| Withdrawn/Depressed | M(SD) | 61.1 (10.60) | 65.5 (10.36) | 72.0 (12.65) | F = 14.63; p < 0.001 |
| Somatic Complaints | M(SD) | 64.2 (6.49) | 55.5 (4.19) | 69.2 (7.46) | F = 96.00; p < 0.001 |
| Social Problems | M(SD) | 59.1 (10.38) | 62.9 (9.08) | 67.9 (9.60) | F = 12.97; p < 0.001 |
| Thought Problems | M(SD) | 57.2 (6.13) | 60.2 (7.94) | 67.4 (10.56) | F = 25.09; p < 0.001 |
| Attention Problems | M(SD) | 57.6 (9.24) | 61.4 (9.09) | 64.7 (9.83) | F = 9.20; p < 0.001 |
| Rule-Breaking Behavior | M(SD) | 56.5 (6.57) | 56.8 (7.46) | 60.8 (8.66) | F = 6.04; p = 0.003 |
| Aggressive Behavior | M(SD) | 56.6 (6.87) | 56.2 (6.42) | 61.2 (9.14) | F = 7.71; p < 0.001 |
| Affective Problems | M(SD) | 60.3 (7.90) | 66.2 (10.53) | 75.8 (11.37) | F = 43.31; p < 0.001 |
| Anxiety Problems | M(SD) | 61.1 (7.39) | 61.3 (7.94) | 66.3 (8.44) | F = 9.01; p < 0.001 |
| Somatic Problems | M(SD) | 65.0 (6.18) | 52.9 (2.62) | 68.4 (7.48) | F = 196.95; p < 0.001 |
| Attention/Deficit | M(SD) | 54.8 (5.41) | 56.7 (5.88) | 58.9 (7.10) | F =7.55; p < 0.001 |
| Oppositional Defiant Problems | M(SD) | 55.7 (6.59) | 56.4 (6.14) | 60.0 (8.18) | F = 6.39; p = 0.002 |
| Conduct Problems | M(SD) | 53.3 (7.13) | 54.9 (6.84) | 60.0 (9.20) | F = 12.03; p < 0.001 |
| NSSI + SSD | NSSI | SSD | |
|---|---|---|---|
| Internalizing problems | p-value | <0.001 | <0.001 |
| Externalizing problems | p-value | 0.002 | 0.001 |
| Total problems | p-value | <0.001 | <0.001 |
| Anxiety/depression | p-value | <0.001 | <0.001 |
| Withdrawal/depression | p-value | 0.007 | <0.001 |
| Social problems | p-value | 0.011 | <0.001 |
| Thought problems | p-value | <0.001 | <0.001 |
| Rule-breaking behavior | p-value | 0.018 | 0.004 |
| Aggressive behavior | p-value | 0.001 | 0.003 |
| Anxiety problems | p-value | 0.003 | <0.001 |
| Oppositional defiant problems | p-value | 0.017 | 0.003 |
| Conduct problems | p-value | 0.002 | <0.001 |
| TAS-20 | SSD | NSSI | NSSI + SSD | |
|---|---|---|---|---|
| Difficulty identifying feelings | M(SD) | 20.2 (5.91) | 21.0 (6.26) | 24.6 (6.45) |
| Difficulty describing feelings | M(SD) | 15.9 (4.73) | 15.4 (4.90) | 18.7 (4.03) |
| Externally-oriented thinking | M(SD) | 20.3 (3.49) | 21.9 (4.35) | 23.6 (4.59) |
| Total for alexithymia | M(SD) | 56.5 (10.74) | 58.3 (11.84) | 66.9 (11.06) |
| Type | Effect | Estimate | SE | 95% C.I. | β | z | p | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Indirect | Internalizing Problems ⟹ Total for Alexithymia ⟹ SSD-NSSI + SSD | 0.007 | 0.003 | 0.002 | 0.012 | 0.146 | 2.56 | 0.010 |
| Component | Internalizing Problems ⟹ Total for Alexithymia | 0.677 | 0.083 | 0.515 | 0.840 | 0.581 | 8.16 | <0.001 |
| Total for Alexithymia ⟹ SSD-NSSI + SSD | 0.010 | 0.004 | 0.003 | 0.018 | 0.251 | 2.70 | 0.007 | |
| Direct | Internalizing Problems ⟹ SSD-NSSI + SSD | 0.015 | 0.004 | 0.006 | 0.024 | 0.306 | 3.28 | 0.001 |
| Total | Internalizing Problems ⟹ SSD-NSSI + SSD | 0.022 | 0.004 | 0.014 | 0.029 | 0.452 | 5.77 | <0.001 |
| Indirect | Internalizing Problems ⟹ Emotional Dysregulation ⟹ SSD-NSSI + SSD | 0.008 | 0.003 | 0.001 | 0.015 | 0.166 | 2.28 | 0.023 |
| Component | Internalizing Problems ⟹ Emotional Dysregulation | 1.647 | 0.150 | 1.353 | 1.940 | 0.687 | 10.99 | <0.001 |
| Emotional Dysregulation ⟹ SSD-NSSI + SSD | 0.005 | 0.002 | 7.61 × 10−4 | 0.009 | 0.241 | 2.33 | 0.020 | |
| Direct | Internalizing Problems ⟹ SSD-NSSI + SSD | 0.014 | 0.005 | 0.004 | 0.023 | 0.290 | 2.80 | 0.005 |
| Total | Internalizing Problems ⟹ SSD-NSSI + SSD | 0.022 | 0.004 | 0.015 | 0.029 | 0.455 | 5.92 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gatta, M.; Angelico, C.; Rigoni, F.; Raffagnato, A.; Miscioscia, M. Alexithymia and Psychopathological Manifestations Centered on the Body: Somatization and Self-Harm. J. Clin. Med. 2022, 11, 2220. https://doi.org/10.3390/jcm11082220
Gatta M, Angelico C, Rigoni F, Raffagnato A, Miscioscia M. Alexithymia and Psychopathological Manifestations Centered on the Body: Somatization and Self-Harm. Journal of Clinical Medicine. 2022; 11(8):2220. https://doi.org/10.3390/jcm11082220
Chicago/Turabian StyleGatta, Michela, Caterina Angelico, Francesca Rigoni, Alessia Raffagnato, and Marina Miscioscia. 2022. "Alexithymia and Psychopathological Manifestations Centered on the Body: Somatization and Self-Harm" Journal of Clinical Medicine 11, no. 8: 2220. https://doi.org/10.3390/jcm11082220
APA StyleGatta, M., Angelico, C., Rigoni, F., Raffagnato, A., & Miscioscia, M. (2022). Alexithymia and Psychopathological Manifestations Centered on the Body: Somatization and Self-Harm. Journal of Clinical Medicine, 11(8), 2220. https://doi.org/10.3390/jcm11082220