
The Incidence of Myocarditis and Pericarditis in Post COVID-19 Unvaccinated Patients—A Large Population-Based Study

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Setting
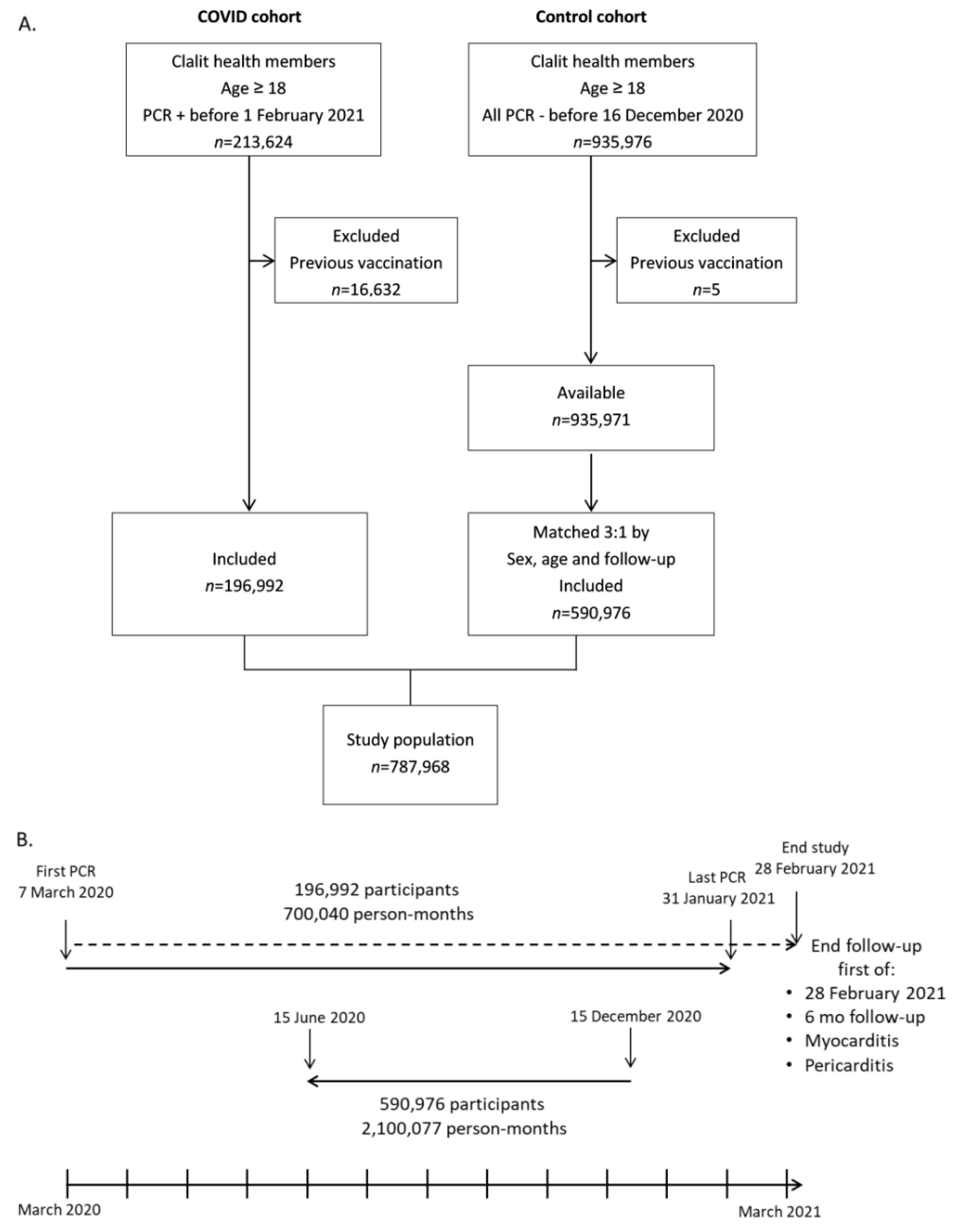
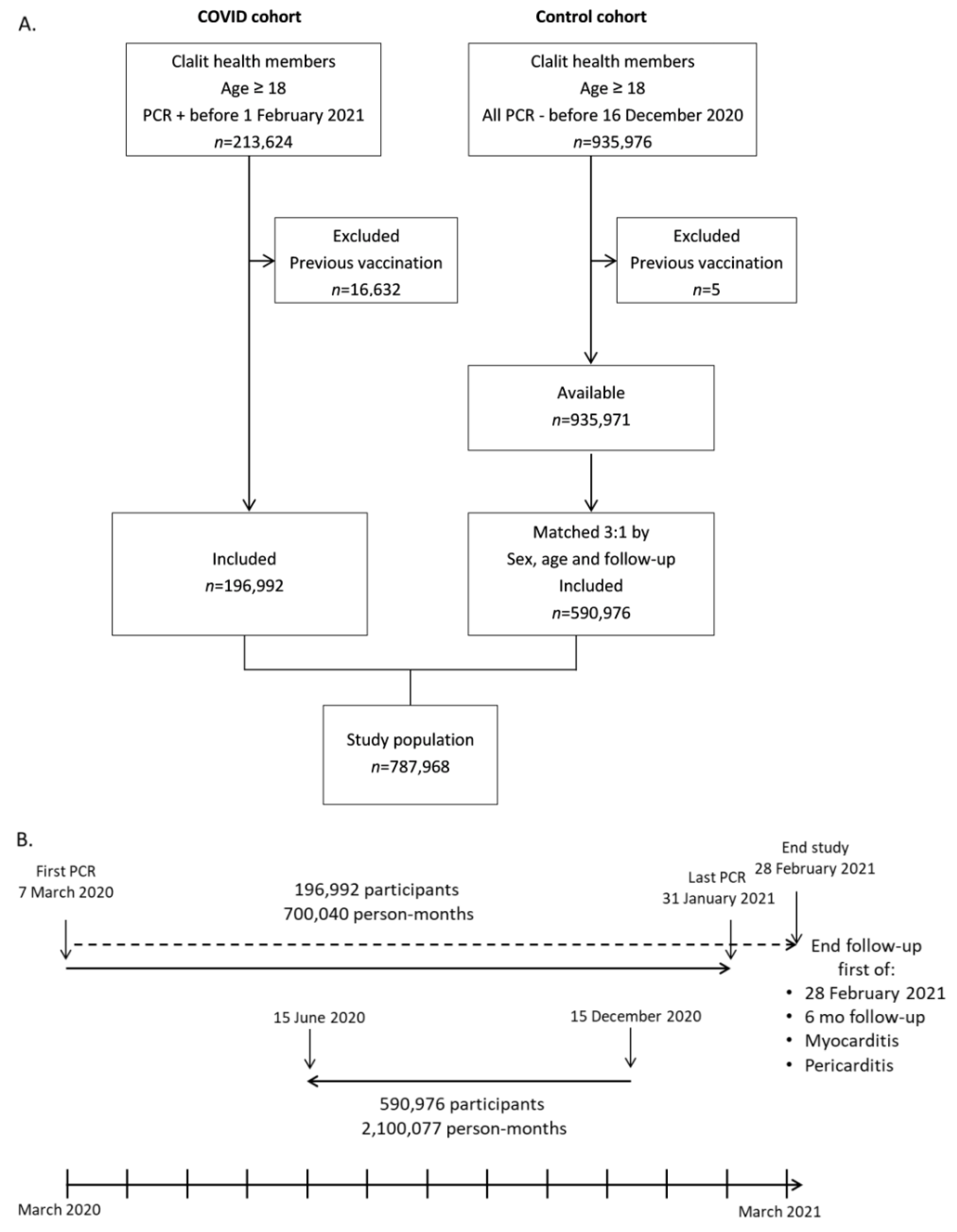
2.2. Study Design and Patient Population
2.3. Statistical Analysis
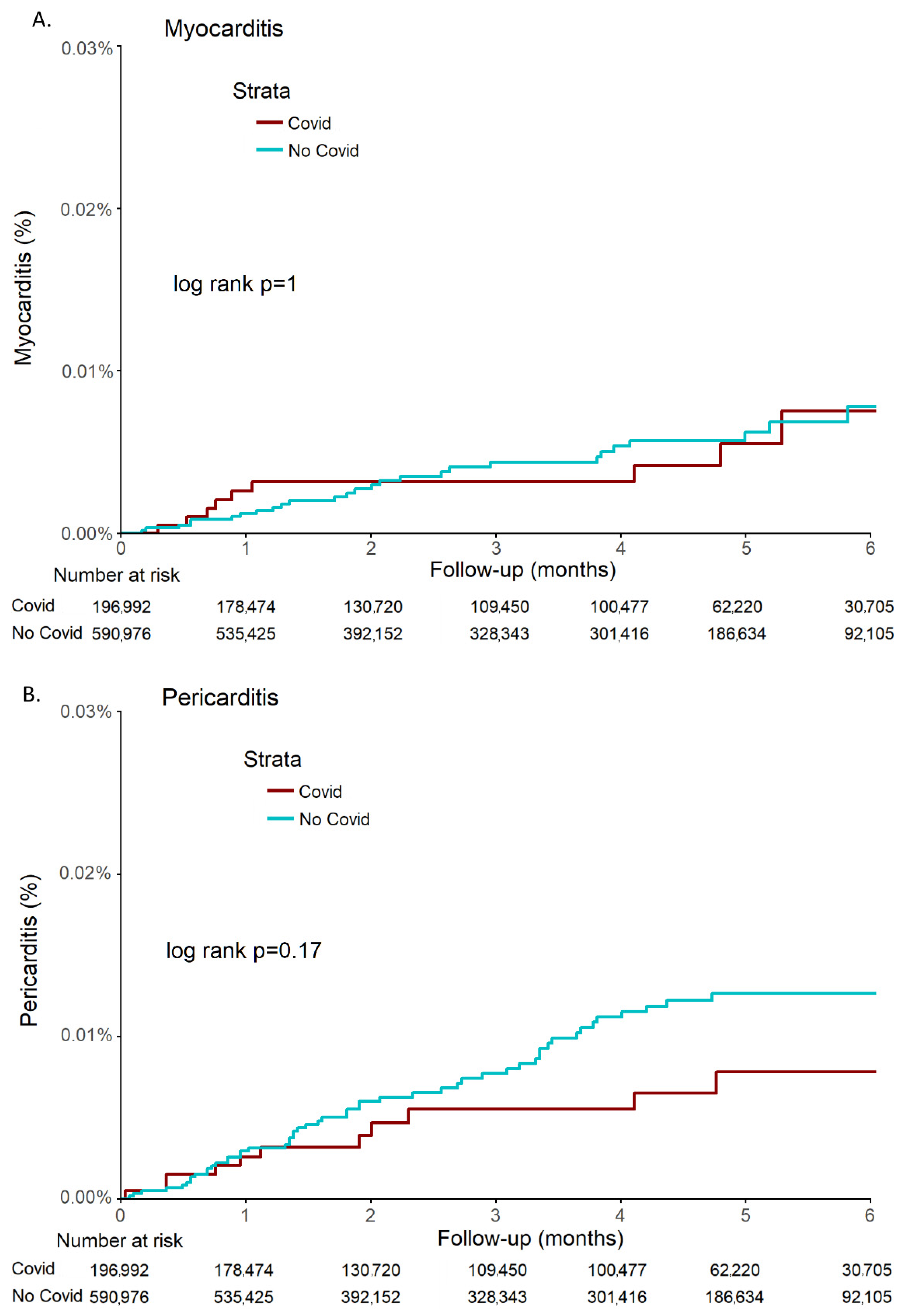
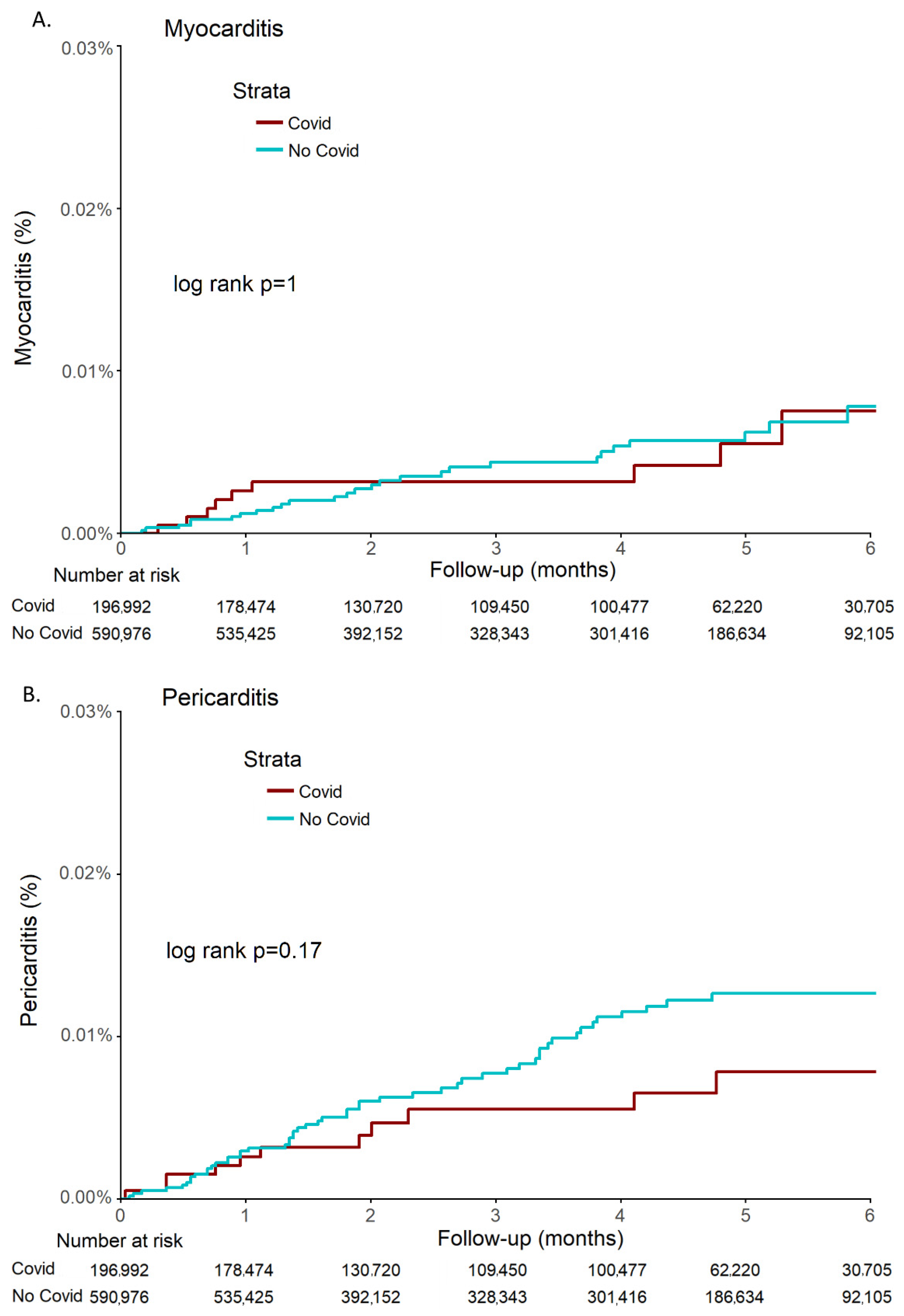
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Paules, C.I.; Marston, H.D.; Fauci, A.S. Coronavirus Infections—More Than Just the Common Cold. JAMA 2020, 323, 707–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Shuwa, H.A.; Shaw, T.N.; Knight, S.B.; Wemyss, K.; McClure, F.A.; Pearmain, L.; Prise, I.; Jagger, C.; Morgan, D.J.; Khan, S.; et al. Alterations in T and B cell function persist in convalescent COVID-19 patients. Med 2021, 2, 720–735.e4. [Google Scholar] [CrossRef] [PubMed]
- McElvaney, O.J.; McEvoy, N.L.; McElvaney, O.F.; Carroll, T.P.; Murphy, M.P.; Dunlea, D.M.; Ni Choileain, O.; Clarke, J.; O’Connor, E.; Hogan, G.; et al. Characterization of the Inflammatory Response to Severe COVID-19 Illness. Am. J. Respir. Crit. Care Med. 2020, 202, 812–821. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal Coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Ercolini, A.M.; Miller, S.D. The role of infections in autoimmune disease. Clin. Exp. Immunol. 2009, 155, 1–15. [Google Scholar] [CrossRef]
- Yazdanpanah, N.; Rezaei, N. Autoimmune complications of COVID-19. J. Med. Virol. 2021, 94, 54–62. [Google Scholar] [CrossRef]
- Fujinami, R.S.; von Herrath, M.G.; Christen, U.; Whitton, J.L. Molecular Mimicry, Bystander Activation, or Viral Persistence: Infections and Autoimmune Disease. Clin. Microbiol. Rev. 2006, 19, 80–94. [Google Scholar] [CrossRef] [Green Version]
- Caforio, A.L.P.; Mahon, N.; Baig, M.K.; Tona, F.; Murphy, R.T.; Elliott, P.M.; McKenna, W.J. Prospective Familial Assessment in Dilated Cardiomyopathy: Cardiac autoantibodies predict disease development in asymptomatic relatives. Circulation 2007, 115, 76–83. [Google Scholar] [CrossRef] [Green Version]
- Matsui, S.; Fu, M.L.; Katsuda, S.; Hayase, M.; Yamaguchi, N.; Teraoka, K.; Kurihara, T.; Takekoshi, N.; Murakami, E.; Hoebeke, J.; et al. Peptides Derived from Cardiovascular G-protein-coupled Receptors Induce Morphological Cardiomyopathic Changes in Immunized Rabbits. J. Mol. Cell. Cardiol. 1997, 29, 641–655. [Google Scholar] [CrossRef] [PubMed]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef] [PubMed]
- Marom, T.; Tshori, S.; Shefer, G.; Pitaro, J. Pneumococcal Conjugated Vaccines Decreased Acute Otitis Media Burden: A Population-Based Study in Israel. J. Pediatr. 2021, 235, 233–238.e3. [Google Scholar] [CrossRef] [PubMed]
- Lo, A.W.; Tang, N.L.; To, K.-F. How the SARS coronavirus causes disease: Host or organism? J. Pathol. 2006, 208, 142–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyuwa, S.; Yamaguchi, K.; Toyoda, Y.; Fujiwara, K. Induction of self-reactive T cells after murine coronavirus infection. J. Virol. 1991, 65, 1789–1795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmi, A.; Ziola, B.; Hovi, T.; Reunanen, M. Antibodies to coronaviruses OC43 and 229E in multiple sclerosis patients. Neurology 1982, 32, 292–295. [Google Scholar] [CrossRef]
- Lardans, V.; Godfraind, C.; Van Der Logt, J.T.M.; Heessen, F.W.A.; Gonzalez, M.-D.; Coutelier, J.-P. Polyclonal B lymphocyte activation induced by mouse hepatitis virus A59 infection. J. Gen. Virol. 1996, 77, 1005–1009. [Google Scholar] [CrossRef]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Le Bert, N.; Tan, A.T.; Kunasegaran, K.; Tham, C.Y.L.; Hafezi, M.; Chia, A.; Chng, M.H.Y.; Lin, M.; Tan, N.; Linster, M.; et al. SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature 2020, 584, 457–462. [Google Scholar] [CrossRef]
- Su, Y.; Yuan, D.; Chen, D.G.; Ng, R.H.; Wang, K.; Choi, J.; Li, S.; Hong, S.; Zhang, R.; Xie, J.; et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell 2022, 185, 881–895.e20. [Google Scholar] [CrossRef]
- Late-Breaking Science Abstracts and Featured Science Abstracts From the American Heart Association’s Scientific Sessions 2020 and Late-Breaking Abstracts in Resuscitation Science From the Resuscitation Science Symposium 2020. Circulation 2020, 142, e470–e500. [CrossRef]
- Montero, F.; Martínez-Barrio, J.; Serrano-Benavente, B.; González, T.; Rivera, J.; Collada, J.M.; Castrejón, I.; Álvaro-Gracia, J. Coronavirus disease 2019 (COVID-19) in autoimmune and inflammatory conditions: Clinical characteristics of poor outcomes. Rheumatol. Int. 2020, 40, 1593–1598. [Google Scholar] [CrossRef]
- Tan, C.; Zheng, X.; Sun, F.; He, J.; Shi, H.; Chen, M.; Tu, C.; Huang, Y.; Wang, Z.; Liang, Y.; et al. Hypersensitivity may be involved in severe COVID-19. Clin. Exp. Allergy 2021, 52, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Feng, Z. The Role of Toll-Like Receptor Signaling in the Progression of Heart Failure. Mediat. Inflamm. 2018, 2018, 9874109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saad, M.A.; Alfishawy, M.; Nassar, M.; Mohamed, M.; Esene, I.N.; Elbendary, A. COVID-19 and Autoimmune Diseases: A Systematic Review of Reported Cases. Curr. Rheumatol. Rev. 2021, 17, 193–204. [Google Scholar] [CrossRef]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265–1273. [Google Scholar] [CrossRef]
- Tereshchenko, L.G.; Bishop, A.; Fisher-Campbell, N.; Levene, J.; Morris, C.; Patel, H.; Khan, A. Risk of Cardiovascular Events after COVID-19: A double-cohort study. medRxiv 2021. [Google Scholar] [CrossRef]
- Huang, L.; Zhao, P.; Tang, D.; Zhu, T.; Han, R.; Zhan, C.; Liu, W.; Zeng, H.; Tao, Q.; Xia, L. Cardiac Involvement in Patients Recovered From COVID-2019 Identified Using Magnetic Resonance Imaging. JACC Cardiovasc. Imaging 2020, 13, 2330–2339. [Google Scholar] [CrossRef]
- Rali, A.S.; Ranka, S.; Shah, Z.; Sauer, A.J. Mechanisms of Myocardial Injury in Coronavirus Disease 2019. Card. Fail. Rev. 2020, 6, e15. [Google Scholar] [CrossRef]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Control | COVID-19 | |
|---|---|---|
| (n = 590,976) | (n = 196,992) | |
| Age (year) | 42.4 (17.7) | 42.4 (17.7) |
| Sex | ||
| Male | 270,210 (45.7) | 90,070 (45.7) |
| Female | 320,766 (54.3) | 106,922 (54.3) |
| BMI (kg/m2) | 26.1 (7.1) | 27.1 (6.7) |
| Sector | ||
| Arab | 109,759 (18.6) | 58,841 (29.9) |
| Bedouin | 19,956 (3.4) | 5306 (2.7) |
| Jewish | 436,986 (74.1) | 108,360 (55.0) |
| Other | 23,285 (3.9) | 24,475 (12.4) |
| Smoking | ||
| Never | 383,002 (69.3) | 137,079 (78.0) |
| Current | 101,475 (18.4) | 19,824 (11.3) |
| Past | 67,992 (12.3) | 18,917 (10.8) |
| Obesity | 145,537 (24.6) | 58,807 (29.9) |
| Diabetes | 61,978 (10.5) | 25,583 (13.0) |
| Hyperlipidemia | 183,704 (31.1) | 60,629 (30.8) |
| CKD | 18,593 (3.1) | 6725 (3.4) |
| PVD | 8016 (1.4) | 2448 (1.2) |
| Hypertension | 100,736 (17.0) | 36,502 (18.5) |
| ACS | 32,987 (5.6) | 11,027 (5.6) |
| CVA | 22,032 (3.7) | 7833 (4.0) |
| Heart failure | 13,228 (2.2) | 5132 (2.6) |
| Myocarditis | Pericarditis | ||||||
|---|---|---|---|---|---|---|---|
| No COVID (n = 27) | COVID (n = 9) | p-Value | No COVID (n = 52) | COVID (n = 11) | p-Value | ||
| Days in hospital | 3 [3–5] | 5 [2–25] | 0.291 | 3 [1.8–5.3] | 2 [2–3.5] | 0.272 | |
| Age (year) | 39.1 (16.8) | 36.4 (19.7) | 0.695 | 49.1 (20.3) | 45.6 (19.3) | 0.609 | |
| Sex (male) | 20 (74.1) | 8 (88.9) | 0.643 | 31 (59.6) | 8 (72.7) | 0.637 | |
| BMI (kg/m2) | 27.3 (6.1) | 26.3 (6.9) | 0.713 | 26.5 (5.8) | 28.6 (3.8) | 0.319 | |
| Diabetes | 4 (14.8) | 1 (11.1) | 1.000 | 12 (23.1) | 1 (9.1) | 0.528 | |
| Hyperlipidemia | 6 (22.2) | 2 (22.2) | 1.000 | 25 (48.1) | 4 (36.4) | 0.708 | |
| Obesity | 14 (51.9) | 1 (11.1) | 0.079 | 15 (28.8) | 6 (54.5) | 0.197 | |
| CKD | 3 (11.1) | 1 (11.1) | 1.000 | 7 (13.5) | 1 (9.1) | 1.000 | |
| Smoking | Now | 6 (26.1) | 1 (12.5) | 0.602 | 9 (19.1) | 1 (9.1) | 0.777 |
| Past | 3 (13.0) | 2 (25.0) | 7 (14.9) | 1 (9.1) | |||
| PVD | 2 (7.4) | 0 (0.0) | 1.000 | 4 (7.7) | 2 (18.2) | 0.609 | |
| ACS | 3 (11.1) | 2 (22.2) | 0.781 | 9 (17.3) | 2 (18.2) | 1.000 | |
| Hypertension | 5 (18.5) | 2 (22.2) | 1.000 | 15 (28.8) | 3 (27.3) | 1.000 | |
| CVA | 3 (11.1) | 2 (22.2) | 0.781 | 5 (9.6) | 2 (18.2) | 0.769 | |
| HF | 5 (18.5) | 2 (22.2) | 1.000 | 6 (11.5) | 1 (9.1) | 1.000 | |
| Severe COVID | - | 2 (22.2) | NA | - | 0 (0.0) | NA | |
| Myocarditis | Pericarditis | |||
|---|---|---|---|---|
| aHR (95% CI) | p-Value | aHR (95% CI) | p-Value | |
| COVID-19 | 1.08 (0.45–2.56) | 0.869 | 0.53 (0.25–1.13) | 0.100 |
| Age | 0.96 (0.93–1.00) | 0.045 * | 1.01 (0.99–1.03) | 0.537 |
| Sex (male) | 4.42 (1.64–11.96) | 0.003 * | 1.93 (1.09–3.41) | 0.025 * |
| BMI | 1.00 (0.97–1.04) | 0.935 | 1.00 (0.94–1.06) | 0.897 |
| Diabetes | 1.15 (0.26–5.00) | 0.856 | 0.97 (0.43–2.21) | 0.950 |
| Hyperlipidemia | 0.33 (0.08–1.43) | 0.139 | 1.13 (0.54–2.38) | 0.749 |
| Obesity | 2.31 (0.99–5.41) | 0.053 | 1.32 (0.64–2.71) | 0.448 |
| CKD | 3.80 (0.82–17.66) | 0.088 | 1.91 (0.72–5.05) | 0.191 |
| Smoking (Now) | 1.62 (0.65–4.06) | 0.304 | 0.85 (0.42–1.74) | 0.661 |
| Smoking (Past) | 1.85 (0.61–5.64) | 0.277 | 0.73 (0.33–1.63) | 0.439 |
| PVD | 1.35 (0.14–12.84) | 0.793 | 4.20 (1.50–11.72) | 0.006 * |
| ACS | 3.93 (0.76–20.40) | 0.104 | 1.52 (0.61–3.80) | 0.366 |
| Hypertension | 1.46 (0.36–5.87) | 0.592 | 0.88 (0.38–2.06) | 0.770 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuvali, O.; Tshori, S.; Derazne, E.; Hannuna, R.R.; Afek, A.; Haberman, D.; Sella, G.; George, J. The Incidence of Myocarditis and Pericarditis in Post COVID-19 Unvaccinated Patients—A Large Population-Based Study. J. Clin. Med. 2022, 11, 2219. https://doi.org/10.3390/jcm11082219
Tuvali O, Tshori S, Derazne E, Hannuna RR, Afek A, Haberman D, Sella G, George J. The Incidence of Myocarditis and Pericarditis in Post COVID-19 Unvaccinated Patients—A Large Population-Based Study. Journal of Clinical Medicine. 2022; 11(8):2219. https://doi.org/10.3390/jcm11082219
Chicago/Turabian StyleTuvali, Ortal, Sagi Tshori, Estela Derazne, Rebecca Regina Hannuna, Arnon Afek, Dan Haberman, Gal Sella, and Jacob George. 2022. "The Incidence of Myocarditis and Pericarditis in Post COVID-19 Unvaccinated Patients—A Large Population-Based Study" Journal of Clinical Medicine 11, no. 8: 2219. https://doi.org/10.3390/jcm11082219
APA StyleTuvali, O., Tshori, S., Derazne, E., Hannuna, R. R., Afek, A., Haberman, D., Sella, G., & George, J. (2022). The Incidence of Myocarditis and Pericarditis in Post COVID-19 Unvaccinated Patients—A Large Population-Based Study. Journal of Clinical Medicine, 11(8), 2219. https://doi.org/10.3390/jcm11082219