
Use of Vaginal Dinoprostone (PGE2) in Patients with Premature Rupture of Membranes (PROM) Undergoing Induction of Labor: A Comparative Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Methods
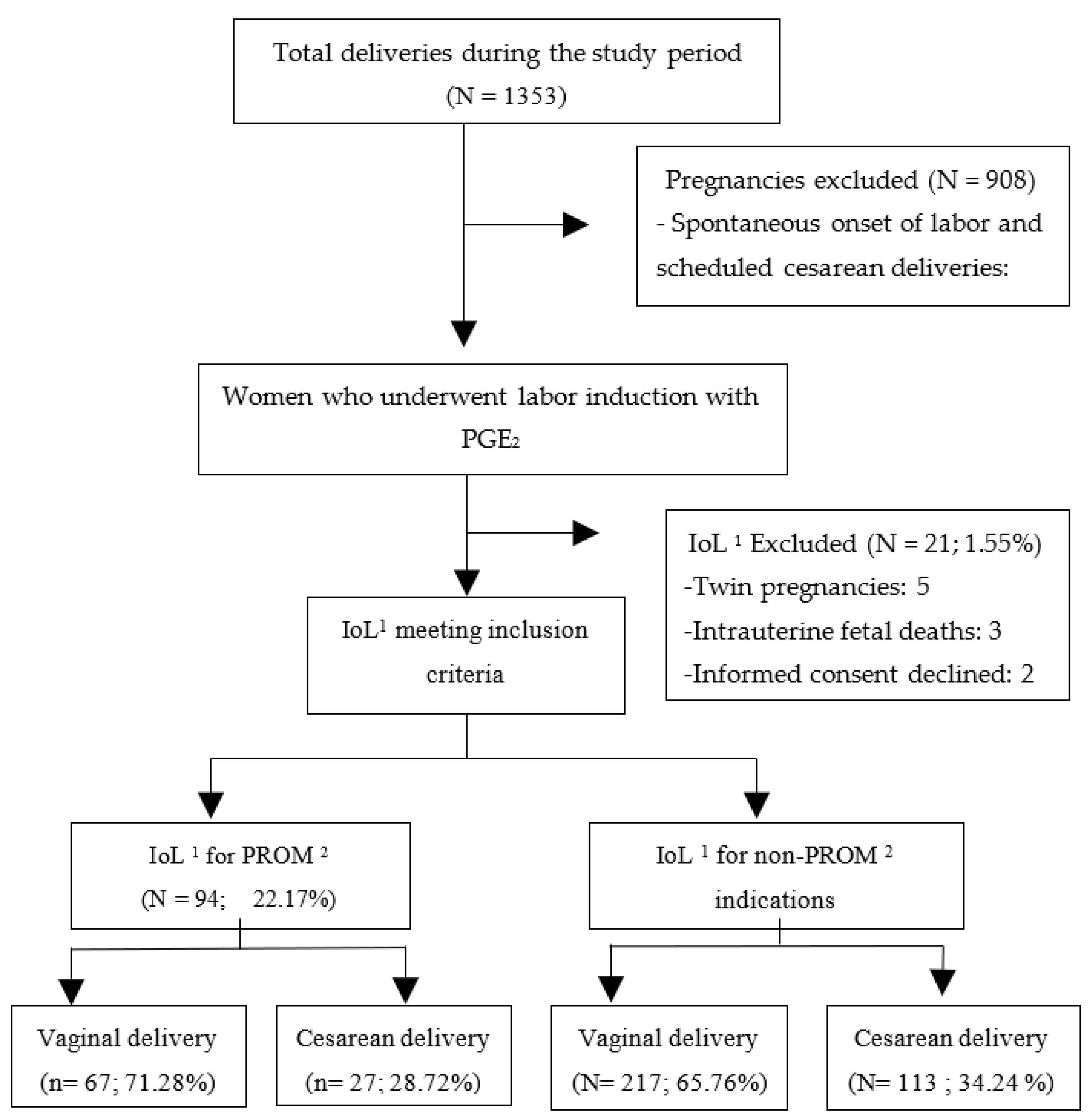
2.2. Inclusion and Exclusion Criteria
2.3. Information Sources
2.4. Induction of Labour Protocol at the Study Center
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Women Undergoing IoL with PROM and without PROM
3.2. Obstetric Outcomes According to PROM Status
3.3. Neonatal Morbidity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ACOG Practice Bulletins. Clinical Management Guidelines for Obstetrician—Gynecologists. Obs. Gynecol. 2020, 133, 168–186. [Google Scholar]
- Middleton, P.; Shepherd, E.; Flenady, V.; McBain, R.D.; A Crowther, C. Planned early birth versus expectant management (waiting) for prelabour rupture of membranes at term (37 weeks or more). Cochrane Database Syst. Rev. 2017, 2017, CD005302. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Yoon, B.H.; Mazor, M.; Gomez, R.; Gonzalez, R.; Diamond, M.P.; Baumann, P.; Araneda, H.; Kenney, J.S.; Cotton, D.B.; et al. A comparative study of the diagnostic performance of amniotic fluid glucose, white blood cell count, interleukin-6, and Gram stain in the detection of microbial invasion in patients with preterm premature rupture of membranes. Am. J. Obstet. Gynecol. 1993, 169, 839–851. [Google Scholar] [CrossRef]
- Asrat, T. Intra-amniotic infection in patients with preterm prelabor rupture of membranes: Pathophysiology, detection, and management. Clin. Perinatol. 2001, 28, 735–751. [Google Scholar] [CrossRef]
- Kacerovsky, M.; Musilová, I.K.; Khatibi, A.; Skogstrand, K.; Hougaard, D.M.; Tambor, V.; Tosner, J.; Jacobsson, B. Intraamniotic inflammatory response to bacteria: Analysis of multiple amniotic fluid proteins in women with preterm prelabor rupture of membranes. J. Matern. Neonatal Med. 2012, 25, 2014–2019. [Google Scholar] [CrossRef]
- Zeitlin, J.; Mohangoo, A.; Delnord, M. European Perinatal Health Report: The Health and Care of Pregnant Women and Babies in Europe in 2010.; Euro-Peristat: Paris, France, 2013. [Google Scholar]
- Lin, M.G.; Nuthalapaty, F.S.; Carver, A.R.; Case, A.S.; Ramsey, P.S. Misoprostol for Labor Induction in Women with Term Premature Rupture of Membranes. Obstet. Gynecol. 2005, 106, 593–601. [Google Scholar] [CrossRef]
- McQueen, D.; Neilson, J.P.; Whittle, M.J. Pre-labour rupture of membranes with an unripe cervix: A random trial of management. J. Obstet. Gynaecol. 1990, 10, 495–498. [Google Scholar] [CrossRef]
- Kulhan, N.G.; Kulhan, M. Labor induction in term nulliparous women with premature rupture of membranes: Oxytocin versus dinoprostone. Arch. Med. Sci. 2019, 15, 896–901. [Google Scholar] [CrossRef]
- Hannah, M.E.; Ohlsson, A.; Farine, D.; Hewson, S.A.; Hodnett, E.D.; Myhr, T.L.; Wang, E.E.; Weston, J.A.; Willan, A.R. Induction of Labor Compared with Expectant Management for Prelabor Rupture of the Membranes at Term. N. Engl. J. Med. 1996, 334, 1005–1010. [Google Scholar] [CrossRef]
- Güngördük, K.; Asicioglu, O.; Besimoglu, B.; Güngördük, O.C.; Yildirm, G.; Ark, C.; Şahbaz, A. Labor induction in term premature rupture of membranes: Comparison between oxytocin and dinoprostone followed 6 hours later by oxytocin. Am. J. Obstet. Gynecol. 2012, 206, 60.e1–60.e8. [Google Scholar] [CrossRef]
- Agencia Española de Medicamentos y Productos Sanitarios (AEMPS). Ficha Técnica Propess. Available online: https://cima.aemps.es/cima/dochtml/ft/62088/FT_62088.html (accessed on 13 December 2021).
- Sociedad Española de Ginecología y Obstetricia. Rotura Prematura de Membranas. Protocolos ProSEGO 2012. Available online: https://sego.es (accessed on 13 December 2021).
- Lyrenas, S.; Clason, I.; Ulmsten, U. In vivo controlled release of PGE2 from a vaginal insert (0.8 mm, 10 mg) during induction of labour. BJOG Int. J. Obstet. Gynaecol. 2001, 108, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Kagan, K.O.; Sonek, J. How to measure cervical length. Ultrasound Obstet. Gynecol. 2015, 45, 358–362. [Google Scholar] [CrossRef] [PubMed]
- The Fetal Medicine Foundation. Cervical Assessment. Available online: https://fetalmedicine.org/education/cervical-assessment (accessed on 13 December 2021).
- Parer, J.T.; Ikeda, T.; King, T.L. The 2008 National Institute of Child Health and Human Development Report on Fetal Heart Rate Monitoring. Obstet. Gynecol. 2009, 114, 136–138. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, X.; Liu, Y.; Jiang, T.; Dai, Y.; Gong, Y.; Li, Q.; Wang, X. Effect of premature rupture of membranes on time to delivery and outcomes in full-term pregnancies with vaginal dinoprostone-induced labour. Arch. Gynecol. Obstet. 2019, 301, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Kehl, S.; Weiss, C.; Dammer, U.; Baier, F.; Faschingbauer, F.; Beckmann, M.W.; Sütterlin, M.; Pretscher, J. Effect of Premature Rupture of Membranes on Induction of Labor: A Historical Cohort Study. Geburtshilfe und Frauenheilkd. 2017, 77, 1174–1181. [Google Scholar] [CrossRef][Green Version]
- Shirley, M. Dinoprostone Vaginal Insert: A Review in Cervical Ripening. Drugs 2018, 78, 1615–1624. [Google Scholar] [CrossRef] [PubMed]
- Alfirevic, Z.; Keeney, E.; Dowswell, T.; Welton, N.; Dias, S.; Jones, L.V.; Navaratnam, K.; Caldwell, D.M. Labour induction with prostaglandins: A systematic review and network meta-analysis. BMJ 2015, 350, h217. [Google Scholar] [CrossRef]
- Tran, S.H.; Cheng, Y.W.; Kaimal, A.J.; Caughey, A.B. Length of rupture of membranes in the setting of premature rupture of membranes at term and infectious maternal morbidity. Am. J. Obstet. Gynecol. 2008, 198, 700.e1–700.e5. [Google Scholar] [CrossRef]
- Seaward, P.; Hannah, M.E.; Myhr, T.L.; Farine, D.; Ohlsson, A.; Wang, E.E.; Haque, K.; Weston, J.A.; Hewson, S.A.; Ohel, G.; et al. International Multicentre Term Prelabor Rupture of Membranes Study: Evaluation of predictors of clinical chorioamnionitis and postpartum fever in patients with prelabor rupture of membranes at term. Am. J. Obstet. Gynecol. 1997, 177, 1024–1029. [Google Scholar] [CrossRef]
- Higgins, R.D.; Saade, G.; Polin, R.A.; Grobman, W.A.; Buhimschi, I.A.; Watterberg, K.; Silver, R.M.; Raju, T.N.; Chorioamnionitis Workshop Participants. Evaluation and Management of Women and Newborns with a Maternal Diagnosis of Chorioamnionitis. Obstet. Gynecol. 2016, 127, 426–436. [Google Scholar] [CrossRef]
- Chiossi, G.; D’Amico, R.; Tramontano, A.L.; Sampogna, V.; Laghi, V.; Facchinetti, F. Prevalence of uterine rupture among women with one prior low transverse cesarean and women with unscarred uterus undergoing labor induction with PGE2: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0253957. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | PROM 1 (n= 94) | Non-PROM 1 (n = 330) | p-Value |
|---|---|---|---|
| Maternal characteristics | |||
| Maternal age (years) * | 32.29 (4.83) | 33.10 (5.16) | 0.174 |
| Pregestational weight (kg) * | 66.68 (12.95) | 69.82 (14.84) | 0.062 |
| Antepartum weight (kg) * | 78.47 (14.53) | 80.82 (14.91) | 0.178 |
| Pregestational Body Mass Index (BMI) (kg/m2) * | 29.43 (4.70) | 30.20 (5.31) | 0.203 |
| Obstetrical characteristics | |||
| Previous cesarean delivery | |||
| No | 85 (90.4%) | 292 (88.5%) | 0.597 |
| Yes | 9 (9.6%) | 38 (11.5%) | |
| Parity | |||
| Primiparity | 21 (22.3%) | 123 (37.3%) | 0.007 |
| Multiparity | 73 (77.7%) | 207 (62.7%) | |
| Preexisting or gestational diabetes | |||
| No | 91 (96.8%) | 294 (89.1%) | 0.154 |
| Preexisting diabetes | 0 (0%) | 4 (1.2%) | |
| Gestational diabetes | 3 (3.2%) | 32 (9.7%) | |
| Hypertensive state in pregnancy | |||
| No | 92 (97.9%) | 292 (88.5%) | 0.043 |
| Chronic hypertension | 2 (2.1%) | 6 (1.8%) | |
| Gestational hypertension | 0 (0%) | 18 (5.5%) | |
| Preeclampsia | 0 (0%) | 13 (3.9%) | |
| Preeclampsia with severe features | 0 (0%) | 1 (0.3%) | |
| Fetal Growth Restriction (FGR) | |||
| No | 94 (100%) | 310 (93.9%) | 0.014 |
| Yes | 0 (0%) | 20 (6.1%) | |
| Gestational age at birth (weeks) | |||
| <37 + 0 days | 12 (12.8%) | 3 (0.09%) | <0.001 |
| ≥37 + 0 days | 82 (87.2%) | 327 (99.1%) | |
| Cervical length prior to IoL 2 (CL) *, millimeters (mm) | 21.27 (8.10) | 28.04 (9.11) | <0.001 |
| Bishop score on admission | 2.13 (1.53) | 2.81 (1.45) | <0.001 |
| Prepartum Amniotic Fluid Index (AFI) | |||
| Normal | 78 (83%) | 270 (81.8%) | 0.025 |
| Oligoamnios | 15 (16%) | 34 (10.3%) | |
| Hydramnios | 1 (1.1%) | 26 (7.9%) | |
| Variable | PROM 1 (n = 94) | Non-PROM 1 (n = 330) | Univariate Analysis | Multivariate Analysis ** | ||
|---|---|---|---|---|---|---|
| OR/MD 95% CI | p-Value | OR/MD 95% CI | p-Value | |||
| Bishop score >6 after PGE2 | ||||||
| No | 26 (27.7) | 161 (48.8) | 2.49 (1.51–4.11) | <0.001 | 2.73 (1.50–4.99) | 0.001 |
| Yes | 68 (72.3) | 169 (51.2) | ||||
| Nulliparous Bishop score >6 after PGE2 | ||||||
| No | 19 (20.2) | 116 (35,2) | 3.62 (2.01–6.54) | <0.001 | ||
| Yes | 54 (57.45) | 91 (27.6) | ||||
| Multiparous Bishop score >6 after PGE2 | ||||||
| No | 7 (7.45) | 45 (13.6) | 1.15 (0.43–3.07) | 0.774 | ||
| Yes | 14 (14.9) | 78 (23.6) | ||||
| Time with PGE2 (min) * | 418.51 (310.22) | 792.42 (420.50) | 373.92 (281.40–466.43) | <0.001 | 1884.52 (752.09–3016.96) | 0.001 |
| Total duration of IoL (min) * | 903.03 (525.73) | 1345.38(653.9) | 442.35 (297.29–597.41) | <0.001 | 2823.37 (1257.30–4389.43) | <0.001 |
| Duration of 2nd stage (min) * | 104.50 (82.61) | 90.56 (78.35) | −13.94 (−35.79–7.83) | 0.209 | −274.51 (−542.58–6.43) | 0.45 |
| Type of delivery | ||||||
| Vaginal delivery | 67 (71.3) | 217 (65.8) | 0.77 (0.47–1.28) | 0.316 | 0.87 (0.47–1.60) | 0.652 |
| Cesarean delivery | 27 (28.7) | 113 (34.2) | ||||
| Meconium | ||||||
| No | 86 (91.5) | 278 (84.2) | 0.50 (0.23–1.09) | 0.080 | 0.64 (0.26–1.57) | 0.327 |
| Yes | 8 (8.5) | 52 (15.8) | ||||
| Reason for cesarean delivery | ||||||
| Arrest of labor | 12 (12.8) | 27 (8.2) | 1.64 (0.80–3.38) | 0.178 | 2.32 (0.95–5.69) | 0.066 |
| Failed induction | 4 (4.3) | 32 (9.7) | 0.41 (0.14–1.20) | 0.105 | 0.51 (0.15–1.74) | 0.282 |
| Cephalopelvic disproportion | 5 (5.3) | 11 (3.3) | 1.63 (0.55–4.81) | 0.377 | 1.42 (0.40–5.12) | 0.588 |
| Emergent | 6 (6.4) | 43 (13) | 0.45 (0.19–1.10) | 0.082 | 0533 (0.20–1.41) | 0.206 |
| Intrapartum fever | ||||||
| No | 88 (93.6) | 313 (94.8) | 0.75 (0.28–1.97) | 0.560 | 0.60 (0.20–1.80) | 0.362 |
| Yes | 6 (6.4) | 16 (4.8) | ||||
| Missing data | 1 (0.3) | |||||
| Intrapartum chorioamnionitis | ||||||
| No | 89 (94.7) | 323 (97.9) | 3.03 (0.91–10.17) | 0.072 | 5.36 (1.18–24.42) | 0.030 |
| Yes | 5 (5.3) | 6 (1.8) | ||||
| Missing data | 1 (0.3) | |||||
| CTG 2: NICHD 3 2 | ||||||
| No | 68 (72.3) | 234 (70.9) | 0.93 (0.55–1.55) | 0.787 | 0.90 (0.51–1.57) | 0.702 |
| Yes | 26 (27.7) | 96 (29.1) | ||||
| CTG 2: NICHD 3 3 | ||||||
| No | 91 (96.8) | 312 (94.5) | 0.57 (0.17–1.98) | 0.378 | 0.55 (0.15–2.06) | 0.372 |
| Yes | 3 (3.2) | 18 (5.5) | ||||
| Postpartum hemorrhage 4 | ||||||
| No | 87 (92.6) | 304 (92.1) | 1.06 (0.44–2.56) | 0.891 | 0.91 (0.33–2.51) | 0.852 |
| Yes | 7 (7.4) | 23 (7.0) | ||||
| Missing data | 3 (0.9) | |||||
| Uterine rupture 5 | ||||||
| No | 93 (98.9) | 327 (99.1) | 3.52 (0.29–56.75) | 0.376 | NC | 0.994 |
| Yes | 1 (0.3) | 1 (0.3) | ||||
| Missing data | 2 (0.6) | |||||
| Blood loss >3.5 (l) | ||||||
| No | 90 (95.7) | 308 (93.3) | 0.57 (0.16–1.98) | 0.377 | 0.84 (0.21–3.45) | 0.814 |
| Yes | 3 (3.2) | 18 (5.5) | ||||
| Missing data | 1 (1.1) | 4 (1.2) | ||||
| ICU 6 admission | ||||||
| No | 93 (98.9) | 326 (98.8) | 3.50 (0.22–56.58) | 0.377 | 0.67 (0–54.31) | 0.858 |
| Yes | 1 (1.1) | 1 (0.3) | ||||
| Missing data | 3 (0.9) | |||||
| Need for transfusion | ||||||
| No | 90 (95.7) | 318 (96.4) | 1.32 (0.34–5.10) | 0.682 | 1.57 (0.30–8.13) | 0.592 |
| Yes | 3 (3.2) | 8 (2.4) | ||||
| Missing data | 1 (1.1) | 4 (1.2) | ||||
| Variable | PROM 5 (n = 94) | Non-PROM 5 (n = 330) | Univariate Analysis | Multivariate Analysis ** | ||
|---|---|---|---|---|---|---|
| OR 95% CI | p-Value | OR 95% CI | p-Value | |||
| APGAR 1 score <7 at 1 min | ||||||
| No | 91 (96.8%) | 321 (97.3%) | 1.18 (0.31–4.43) | 0.811 | 1.70 (0.37–7.83) | 0.494 |
| Yes | 3 (3.2%) | 9 (2.7%) | ||||
| APGAR score <7 at 5 min | ||||||
| No | 94 (100%) | 328 (99.4%) | NC | 0.997 | 2.54 (NC) | 1 |
| Yes | 0 (0%) | 2 (0.6%) | ||||
| NICU 2 admission | ||||||
| No | 82 (87.2%) | 296 (89.7%) | 0.78 (0.39–1.58) | 0.499 | 1.24 (0.47–3.28) | 0.661 |
| Yes | 12 (12.8%) | 34 (10.3%) | ||||
| REA 3 III–IV | ||||||
| No | 91 (96.8%) | 322 (97.6%) | 1.33 (0.34–5.10) | 0.681 | 3.77 (0.68–21.33) | 0.133 |
| Yes | 3 (3.2%) | 8 (2.4%) | ||||
| U. artery 4 pH <7.20 at birth | ||||||
| No | 86 (91.5) | 282 (85.5) | 0.50 (1.19–1.31) | 0.158 | 0.87 (0.30–2.54) | 0.795 |
| Yes | 5 (5.3) | 33 (10.0) | ||||
| Missing data | 3 (1.2) | 15 (4.5) | ||||
| U. artery 4 pH < 7.10 at birth | ||||||
| No | 90 (95.8) | 313 (94.85) | 1.74 (0.16–19.40) | 0.653 | NC | 0.957 |
| Yes | 1 (0.3) | 2 (0.6) | ||||
| Missing data | 3 (1.2) | 15 (4.55) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Jiménez, N.; García-Sánchez, F.; Pailos, R.H.; Rodrigo-Álvaro, V.; Pascual-Pedreño, A.; Moreno-Cid, M.; Hernández-Martínez, A.; Molina-Alarcón, M. Use of Vaginal Dinoprostone (PGE2) in Patients with Premature Rupture of Membranes (PROM) Undergoing Induction of Labor: A Comparative Study. J. Clin. Med. 2022, 11, 2217. https://doi.org/10.3390/jcm11082217
López-Jiménez N, García-Sánchez F, Pailos RH, Rodrigo-Álvaro V, Pascual-Pedreño A, Moreno-Cid M, Hernández-Martínez A, Molina-Alarcón M. Use of Vaginal Dinoprostone (PGE2) in Patients with Premature Rupture of Membranes (PROM) Undergoing Induction of Labor: A Comparative Study. Journal of Clinical Medicine. 2022; 11(8):2217. https://doi.org/10.3390/jcm11082217
Chicago/Turabian StyleLópez-Jiménez, Nuria, Fiamma García-Sánchez, Rafael Hernández Pailos, Valentin Rodrigo-Álvaro, Ana Pascual-Pedreño, María Moreno-Cid, Antonio Hernández-Martínez, and Milagros Molina-Alarcón. 2022. "Use of Vaginal Dinoprostone (PGE2) in Patients with Premature Rupture of Membranes (PROM) Undergoing Induction of Labor: A Comparative Study" Journal of Clinical Medicine 11, no. 8: 2217. https://doi.org/10.3390/jcm11082217
APA StyleLópez-Jiménez, N., García-Sánchez, F., Pailos, R. H., Rodrigo-Álvaro, V., Pascual-Pedreño, A., Moreno-Cid, M., Hernández-Martínez, A., & Molina-Alarcón, M. (2022). Use of Vaginal Dinoprostone (PGE2) in Patients with Premature Rupture of Membranes (PROM) Undergoing Induction of Labor: A Comparative Study. Journal of Clinical Medicine, 11(8), 2217. https://doi.org/10.3390/jcm11082217