
Association between Childhood Maltreatment and Suicidal Ideation: A Path Analysis Study

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Descriptive Analysis
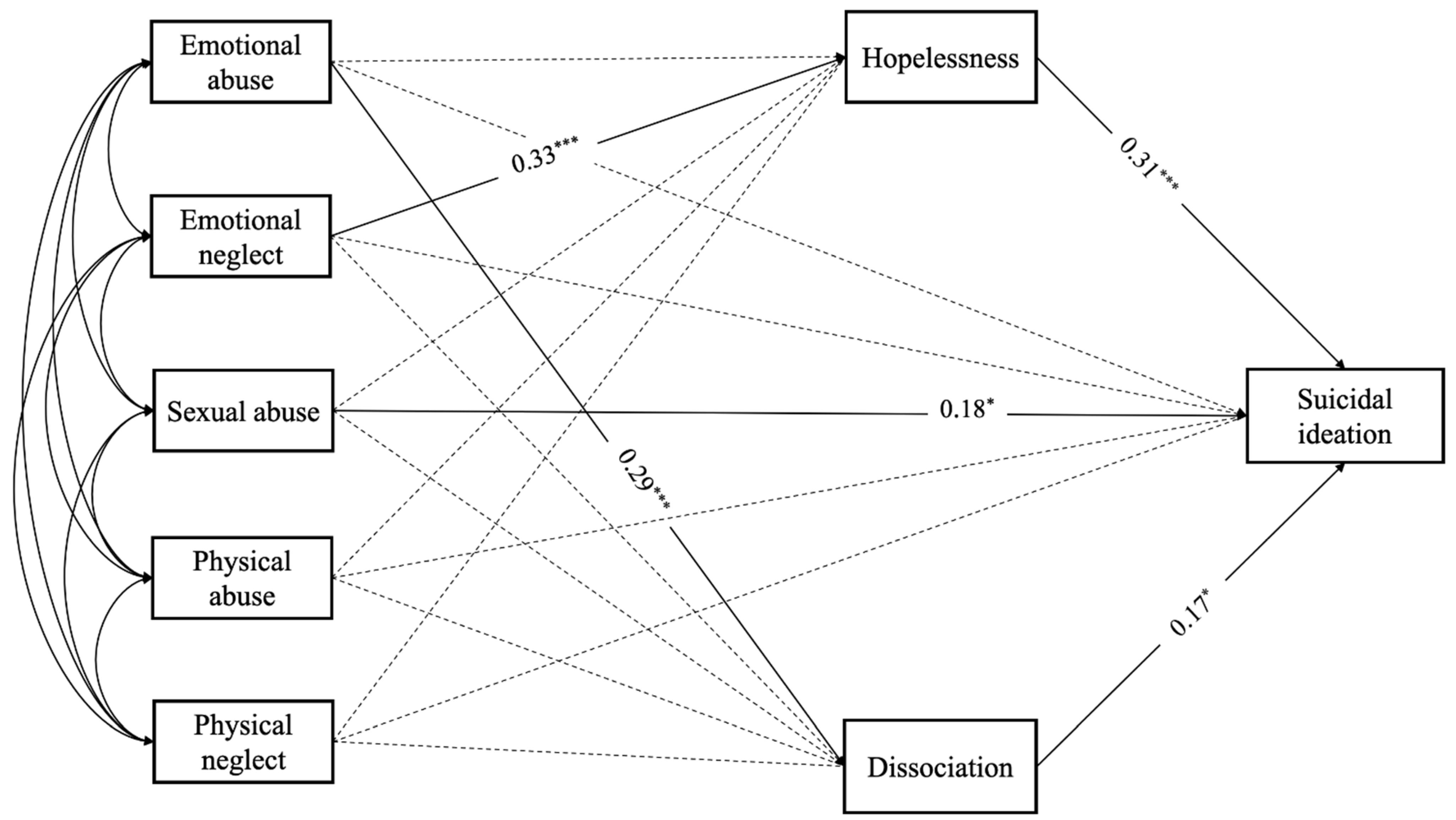
3.2. Path Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hussey, J.M.; Chang, J.J.; Kotch, J.B. Child Maltreatment in the United States: Prevalence, Risk Factors, and Adolescent Health Consequences. Pediatrics 2006, 118, 933–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finkelhor, D.; Turner, H.A.; Shattuck, A.; Hamby, S.L. Violence, Crime, and Abuse Exposure in a National Sample of Children and Youth: An Update. JAMA Pediatr. 2013, 167, 614–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merrick, M.T.; Ford, D.C.; Ports, K.A.; Guinn, A.S. Prevalence of Adverse Childhood Experiences from the 2011–2014 Behavioral Risk Factor Surveillance System in 23 States. JAMA Pediatr. 2018, 172, 1038–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giano, Z.; Wheeler, D.L.; Hubach, R.D. The Frequencies and Disparities of Adverse Childhood Experiences in the US. BMC Public Health 2020, 20, 1327. [Google Scholar] [CrossRef]
- Walsh, K.; McLaughlin, K.A.; Hamilton, A.; Keyes, K.M. Trauma Exposure, Incident Psychiatric Disorders, and Disorder Transitions in a Longitudinal Population Representative Sample. J. Psychiatr. Res. 2017, 92, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Keyes, K.M.; Eaton, N.R.; Krueger, R.F.; McLaughlin, K.A.; Wall, M.M.; Grant, B.F.; Hasin, D.S. Childhood Maltreatment and the Structure of Common Psychiatric Disorders. Br. J. Psychiatry 2012, 200, 107–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varese, F.; Smeets, F.; Drukker, M.; Lieverse, R.; Lataster, T.; Viechtbauer, W.; Read, J.; van Os, J.; Bentall, R.P. Childhood Adversities Increase the Risk of Psychosis: A Meta-Analysis of Patient-Control, Prospective-and Cross-Sectional Cohort Studies. Schizophr. Bull. 2012, 38, 661–671. [Google Scholar] [CrossRef]
- Pompili, M.; Innamorati, M.; Lamis, D.A.; Erbuto, D.; Venturini, P.; Ricci, F.; Serafini, G.; Amore, M.; Girardi, P. The Associations among Childhood Maltreatment, “Male Depression” and Suicide Risk in Psychiatric Patients. Psychiatry Res. 2014, 220, 571–578. [Google Scholar] [CrossRef]
- Zatti, C.; Rosa, V.; Barros, A.; Valdivia, L.; Calegaro, V.C.; Freitas, L.H.; Ceresér, K.M.M.; Rocha, N.S.D.; Bastos, A.G.; Schuch, F.B. Childhood Trauma and Suicide Attempt: A Meta-Analysis of Longitudinal Studies from the Last Decade. Psychiatry Res. 2017, 256, 353–358. [Google Scholar] [CrossRef]
- Thompson, M.P.; Kingree, J.B.; Lamis, D. Associations of Adverse Childhood Experiences and Suicidal Behaviors in Adulthood in a US Nationally Representative Sample. Child Care Health Dev. 2019, 45, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Posner, K.; Oquendo, M.A.; Gould, M.; Stanley, B.; Davies, M. Columbia Classification Algorithm of Suicide Assessment (C-CASA): Classification of Suicidal Events in the FDA’s Pediatric Suicidal Risk Analysis of Antidepressants. Am. J. Psychiatry 2007, 164, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Angelakis, I.; Gillespie, E.L.; Panagioti, M. Childhood Maltreatment and Adult Suicidality: A Comprehensive Systematic Review with Meta-Analysis. Psychol. Med. 2019, 49, 1057–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angelakis, I.; Austin, J.L.; Gooding, P. Association of Childhood Maltreatment with Suicide Behaviors among Young People: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2020, 3, e2012563. [Google Scholar] [CrossRef] [PubMed]
- Dervic, K.; Grunebaum, M.F.; Burke, A.K.; Mann, J.J.; Oquendo, M.A. Protective Factors against Suicidal Behavior in Depressed Adults Reporting Childhood Abuse. J. Nerv. Ment. Dis. 2006, 194, 971–974. [Google Scholar] [CrossRef]
- Beristianos, M.H.; Maguen, S.; Neylan, T.C.; Byers, A.L. Trauma Exposure and Risk of Suicidal Ideation among Ethnically Diverse Adults. Depress. Anxiety 2016, 33, 495–501. [Google Scholar] [CrossRef] [Green Version]
- De Mattos Souza, L.D.; Molina, M.L.; da Silva, R.A.; Jansen, K. History of Childhood Trauma as Risk Factors to Suicide Risk in Major Depression. Psychiatry Res. 2016, 246, 612–616. [Google Scholar] [CrossRef]
- Barbosa, L.P.; Quevedo, L.; da Silva, G.D.G.; Jansen, K.; Pinheiro, R.T.; Branco, J.; Lara, D.; Oses, J.; da Silva, R.A. Childhood Trauma and Suicide Risk in a Sample of Young Individuals Aged 14–35 Years in Southern Brazil. Child Abus. Negl. 2014, 38, 1191–1196. [Google Scholar] [CrossRef]
- Prokopez, C.R.; Vallejos, M.; Farinola, R.; Alberio, G.; Caporusso, G.B.; Cozzarin, L.G.; Chiapella, L.C.; Fuentes, P.; Daray, F.M. The History of Multiple Adverse Childhood Experiences in Patients with Schizophrenia Is As-Sociated with More Severe Symptomatology and Suicidal Behavior with Gender-Specific Characteristics. Psychiatry Res. 2020, 293, 113411. [Google Scholar] [CrossRef]
- Agnew-Blais, J.; Danese, A. Childhood Maltreatment and Unfavourable Clinical Outcomes in Bipolar Disorder: A Systematic Review and Meta-Analysis. Lancet Psychiatry 2016, 3, 342–349. [Google Scholar] [CrossRef]
- Thomas, S.; Höfler, M.; Schäfer, I.; Trautmann, S. Childhood Maltreatment and Treatment Outcome in Psychotic Disorders: A Systematic Review and Meta-Analysis. Acta Psychiatr. Scand. 2019, 140, 295–312. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Ford, J.D.; Gómez, J.M. Self-Injury and Suicidality: The Impact of Trauma and Dissociation. J. Trauma Dissociation 2015, 16, 225–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connors, R. Self-Injury in Trauma Survivors: 1. Functions and Meanings. Am. J. Orthopsychiatry 1996, 66, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Serafini, G.; Lamis, D.A.; Aguglia, A.; Amerio, A.; Nebbia, J.; Geoffroy, P.A.; Pompili, M.; Amore, M. Hopelessness and Its Correlates with Clinical Outcomes in an Outpatient Setting. J. Affect. Disord. 2020, 263, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Mueller-Pfeiffer, C.; Moergeli, H.; Schumacher, S.; Martin-Soelch, C.; Wirtz, G.; Fuhrhans, C.; Hindermann, E.; Rufer, M. Characteristics of Child Maltreatment and Their Relation to Dissociation, Posttraumatic Stress Symptoms, and Depression in Adult Psychiatric Patients. J. Nerv. Ment. Dis. 2013, 201, 471–477. [Google Scholar] [CrossRef] [Green Version]
- Courtney, E.A.; Johnson, J.G.; Alloy, L.B. Associations of Childhood Maltreatment with Hopelessness and Depression among Adolescent Primary Care Patients. Int. J. Cogn. Ther. 2008, 1, 4–17. [Google Scholar] [CrossRef]
- Kuo, W.H.; Gallo, J.J.; Eaton, W.W. Hopelessness, Depression, Substance Disorder, and Suicidality—A 13-Year Community-Based Study. Soc. Psychiatry Psychiatr. Epidemiol. 2004, 39, 497–501. [Google Scholar] [CrossRef]
- David Klonsky, E.; Kotov, R.; Bakst, S.; Rabinowitz, J.; Bromet, E.J. Hopelessness as a Predictor of Attempted Suicide among First Admission Patients with Psychosis: A 10-Year Cohort Study. Suicide Life-Threat. Behav. 2012, 42, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Franklin, J.C.; Ribeiro, J.D.; Fox, K.R.; Bentley, K.H.; Kleiman, E.M.; Huang, X.; Musacchio, K.M.; Jaroszewski, A.C.; Chang, B.P.; Nock, M.K. Risk Factors for Suicidal Thoughts and Behaviors: A Meta-Analysis of 50 Years of Research. Psychol. Bull. 2017, 143, 187–232. [Google Scholar] [CrossRef]
- Berardelli, I.; Belvisi, D.; Corigliano, V.; Costanzo, M.; Innamorati, M.; Fabbrini, G.; Berardelli, A.; Pompili, M. Suicidal Ideation, Perceived Disability, Hopelessness and Affective Temperaments in Patients Affected by Parkinson’s Disease. Int. J. Clin. Pract. 2018, 19, e13287. [Google Scholar] [CrossRef]
- Calati, R.; Bensassi, I.; Courtet, P. The Link between Dissociation and Both Suicide Attempts and Non-suicidal Self-Injury: Meta-Analyses. Psychiatry Res. 2017, 251, 103–114. [Google Scholar] [CrossRef]
- Brokke, S.S.; Bertelsen, T.B.; Landrø, N.I.; Haaland, V.Ø. The Effect of Sexual Abuse and Dissociation on Suicide Attempt. BMC Psychiatry 2022, 22, 29. [Google Scholar] [CrossRef] [PubMed]
- Freeman, T.W.; Keesee, N.; Thornton, C.; Gillette, G.; Young, K. Dissociative Symptoms in Posttraumatic Stress Disorder Subjects with a History of Suicide Attempts. J. Nerv. Ment. Dis. 1995, 183, 664–666. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Srednicki, O. Childhood Sexual Abuse, Dissociation, and Adult Self-Destructive Behavior. J. Child Sex. Abus. 2002, 10, 75–89. [Google Scholar] [CrossRef] [PubMed]
- Zoroglu, S.S.; Tuzun, U.; Sar, V.; Tutkun, H.; Savaçs, H.A.; Ozturk, M.; Alyanak, B.; Kora, M.E. Suicide Attempt and Self-Mutilation among Turkish High School Students in Relation with Abuse, Neglect and Dissociation. Psychiatry Clin. Neurosci. 2003, 57, 119–126. [Google Scholar] [CrossRef]
- Tamar-Gurol, D.; Sar, V.; Karadag, F.; Evren, C.; Karagoz, M. Childhood Emotional Abuse, Dissociation, and Suicidality among Patients with Drug Dependency in Turkey. Psychiatry Clin. Neurosci. 2008, 62, 540–547. [Google Scholar] [CrossRef]
- Swannell, S.; Martin, G.; Page, A.; Hasking, P.; Hazell, P.; Taylor, A.; Protani, M. Child Maltreatment, Subsequent Non-suicidal Self-Injury and the Mediating Roles of Dissociation, Alexithymia and Self-Blame. Child Abus. Negl. 2012, 36, 572–584. [Google Scholar] [CrossRef]
- Bertule, M.; Sebre, S.B.; Kolesovs, A. Childhood Abuse Experiences, Depression and Dissociation Symptoms in Relation to Suicide Attempts and Suicidal Ideation. J. Trauma Dissociation 2021, 22, 598–614. [Google Scholar] [CrossRef]
- Haatainen, K.M.; Tanskanen, A.; Kylmä, J.; Honkalampi, K.; Koivumaa-Honkanen, H.; Hintikka, J.; Antikainen, R.; Viinamäki, H. Gender Differences in the Association of Adult Hopelessness with Adverse Childhood Experiences. Soc. Psychiatry Psychiatr. Epidemiol. 2003, 38, 12–17. [Google Scholar] [CrossRef]
- Brenner, L.A.; Forster, J.E.; Hoffberg, A.S.; Matarazzo, B.B.; Hostetter, T.A.; Signoracci, G.; Simpson, G.K. Window to Hope: A Randomized Controlled Trial of a Psychological Intervention for the Treatment of Hopelessness among Veterans with Moderate to Severe Traumatic Brain Injury. J. Head Trauma Rehabil. 2018, 33, E64–E73. [Google Scholar] [CrossRef]
- Erbuto, D.; Innamorati, M.; Lamis, D.A.; Berardelli, I.; Forte, A.; De Pisa, E.; Migliorati, M.; Serafini, G.; Gonda, X.; Rihmer, Z.; et al. Mediators in the Association Between Affective Temperaments and Suicide Risk among Psychiatric Inpatients. Psychiatry 2018, 81, 240–257. [Google Scholar] [CrossRef]
- Janiri, D.; De Rossi, P.; Kotzalidis, G.D.; Girardi, P.; Koukopoulos, A.E.; Reginaldi, D.; Dotto, F.; Manfredi, G.; Jollant, F.; Gorwood, P.; et al. Psychopathological Characteristics and Adverse Childhood Events Are Differentially Associated with Suicidal Ideation and Suicidal Acts in Mood Disorders. Eur. Psychiatry 2018, 53, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Gibb, B.E.; Alloy, L.B.; Abramson, L.Y.; Rose, D.T.; Whitehouse, W.G.; Hogan, M.E. Childhood Maltreatment and College Students’ Current Suicidal Ideation: A Test of the Hopelessness Theory. Suicide Life-Threat. Behav. 2001, 31, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Abramson, L.Y.; Alloy, L.B.; Hogan, M.E.; Whitehouse, W.G.; Gibb, B.E.; Hankin, B.L.; Cornette, M.M. The Hopelessness Theory of Suicidality. In Suicide Science: Expanding Boundaries; Joiner, T.E., Rudd, M.D., Eds.; Kluwer Academic/Plenum Publishers: New York, NY, USA, 2000; pp. 17–32. [Google Scholar]
- Meadows, L.A.; Kaslow, N.J. Hopelessness as Mediator of the Link between Reports of a History of Child Maltreatment and Suicidality in African American Women. Cognit. Ther. Res. 2008, 26, 657–674. [Google Scholar] [CrossRef]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5 Disorders, Clinician Version (SCID-5-CV); American Psychiatric Association: Arlington, VA, USA, 2016. [Google Scholar]
- Silverman, M.M.; Berman, A.L.; Sanddal, N.D.; O’carroll, P.W.; Joiner, T.E. Rebuilding the tower of Babel: A revised nomenclature for the study of suicide and suicidal behaviors. Part 1: Background, rationale, and methodology. Suicide Life-Threat Behav. 2007, 37, 248–263. [Google Scholar] [PubMed]
- Silverman, M.M.; Berman, A.L.; Sanddal, N.D.; O’carroll, P.W.; Joiner, T.E. Rebuilding the tower of Babel: A revised nomenclature for the study of suicide and suicidal behaviors. Part 2: Suicide-related ideations, communications, and behaviors. Suicide Life-Threat Behav. 2007, 37, 264–277. [Google Scholar] [CrossRef]
- Posner, K.; Brent, D.; Lucas, C.; Gould, M.; Stanley, B.; Brown, G.; Fisher, P.; Zelazny, J.; Burke, A.; Oquendo, M.; et al. Columbia-Suicide Severity Rating Scale (C-SSRS); Columbia University Medical Center: New York, NY, USA, 2008; p. 10. [Google Scholar]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, G.A.; Greenhill, L.; Shen, S.; et al. The Columbia-Suicide Severity Rating Scale: Initial Validity and Internal Consistency Findings from Three Multisite Studies with Adolescents and Adults. Am. J. Psychiatry 2011, 168, 1266–1277. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, D.P.; Fink, L.; Handelsman, L.; Foote, J.; Lovejoy, M.; Wenzel, K.; Sapareto, E.; Ruggiero, J. Initial Reliability and Validity of a New Retrospective Measure of Child Abuse and Neglect. Am. J. Psychiatry 1994, 151, 1132–1136. [Google Scholar]
- Bernstein, D.P.; Fink, L.A. CTQ: Childhood Trauma Questionnaire: A retrospective Self-Report; Psychological Corp.: San Antonio, TX, USA, 1998. [Google Scholar]
- Beck, A.T.; Steer, R.A. Manual for the Beck Hopelessness Scale, 2nd ed.; Psychological Corp: San Antonio, TX, USA, 1993. [Google Scholar]
- Pompili, M.; Iliceto, P.; Lester, D.; Innamorati, M.; Girardi, P.; Tatarelli, R. BHS Beck Hopelessness Scale: Manuale; Giunti O.S. Organizzazioni Speciali: Firenze, Italy, 2008. [Google Scholar]
- Innamorati, M.; Lester, D.; Balsamo, M.; Erbuto, D.; Ricci, F.; Amore, M.; Girardi, P.; Pompili, M. Factor validity of the Beck Hopelessness Scale in Italian medical patients. J. Psychopathol. Behav. Assess. 2014, 36, 300–307. [Google Scholar] [CrossRef]
- Beck, A.T.; Brown, G.; Berchick, R.J.; Stewart, B.L.; Steer, R.A. Relationship between Hopelessness and Ultimate Suicide: A Replication with Psychiatric Outpatients. Am. J. Psychiatry 1990, 147, 190–195. [Google Scholar] [CrossRef] [Green Version]
- Granö, N.; Oksanen, J.; Kallionpää, S.; Roine, M. Specificity and Sensitivity of the Beck Hopelessness Scale for Suicidal Ideation among Adolescents Entering Early Intervention Service. Nord. J. Psychiatry 2017, 71, 72–76. [Google Scholar] [CrossRef]
- McMillan, D.; Gilbody, S.; Beresford, E.; Neilly, L. Can we predict suicide and non-fatal self- harm with the Beck Hopelessness Scale? A meta-analysis. Psychol. Med. 2007, 37, 769–778. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, E.M.; Putnam, F.W. Development, Reliability, and Validity of a Dissociation Scale. J. Nerv. Ment. Dis. 1986, 174, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Carlson, E.B.; Putnam, F.W. An Update on the Dissociative Experiences Scale. Dissociation 1993, 6, 16–27. [Google Scholar]
- Mazzotti, E.; Farina, B.; Imperatori, C.; Mansutti, F.; Prunetti, E.; Speranza, A.M.; Barbaranelli, C. Is the Dissociative Experiences Scale able to identify detachment and compartmentalization symptoms? Factor structure of the Dissociative Experiences Scale in a large sample of psychiatric and nonpsychiatric subjects. Neuropsychiatr. Dis. Treat. 2016, 12, 1295–1302. [Google Scholar]
- Muthén, L.K.; Muthén, B. Mplus. The Comprehensive Modelling Program for Applied Researchers: User’s Guide, 5th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2018. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 2nd ed.; Guilford: New York, NY, USA, 2005. [Google Scholar]
- Hart, S.N.; Brassard, M.R.; Karlson, H.C. Psychological Maltreatment. In The APSAC Handbook on Child Maltreatment; Brier, J., Berliner, L., Bulkley, J.A., Jenny, C., Raid, T., Eds.; Sage Publications: Thousand Oaks, CA, USA, 1996; pp. 72–89. [Google Scholar]
- Lin, L.; Du, Q.Q.; Hu, N.B.; Jia, G.Z.; Wang, P.Y. Study on the Correlation between Childhood Neglect and Coping Styles of Middle School Students. Chin. J. Child Health Care 2012, 20, 890–892. [Google Scholar]
- Liu, J.; Fang, Y.; Gong, J.; Cui, X.; Meng, T.; Xiao, B.; He, Y.; Shen, Y.; Luo, X. Associations between Suicidal Behavior and Childhood Abuse and Neglect: A Meta-Analysis. J. Affect. Disord. 2017, 220, 147–155. [Google Scholar] [CrossRef] [PubMed]
- McGee, R.A.; Wolfe, D.A.; Wilson, S.K. Multiple Maltreatment Experiences and Adolescent Behavior Problems: Adolescents’ Perspectives. Dev. Psychopathol. 1997, 9, 131–149. [Google Scholar] [CrossRef]
- Martins-Monteverde, C.M.S.; Baes, C.V.W.; Reisdorfer, E.; Padovan, T.; Tofoli, S.M.D.C.; Juruena, M.F. Relationship between Depression and Subtypes of Early Life Stress in Adult Psychiatric Patients. Front. Psychiatry 2019, 10, 19. [Google Scholar] [CrossRef]
- Abramson, L.Y.; Metalsky, G.I.; Alloy, L.B. Hopelessness Depression: A Theory-Based Subtype of Depression. Psychol. Rev. 1989, 96, 358. [Google Scholar] [CrossRef]
- Freyd, J.J. Betrayal Trauma: Traumatic Amnesia as an Adaptive Response to Childhood Abuse. Ethics Behav. 1994, 4, 307–329. [Google Scholar] [CrossRef]
- Brown, J.; Cohen, P.; Johnson, J.G.; Smailes, E.M. Childhood Abuse and Neglect: Specificity of Effects on Adolescent and Young Adult Depression and Suicidality. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 1490–1496. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, M.E.; Ackard, D.M.; Resnick, M.D. Protective Factors and Suicide Risk in Adolescents with a History of Sexual Abuse. J. Pediatr. 2007, 151, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Bahk, Y.C.; Jang, S.K.; Choi, K.H.; Lee, S.H. The Relationship between Childhood Trauma and Suicidal Ideation: Role of Maltreatment and Potential Mediators. Psychiatry Investig. 2017, 14, 37–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hailes, H.P.; Yu, R.; Danese, A.; Fazel, S. Long-Term Outcomes of Childhood Sexual Abuse: An Umbrella Review. Lancet Psychiatry 2019, 6, 830–839. [Google Scholar] [CrossRef] [Green Version]
- Alloy, L.B.; Abramson, L.Y.; Smith, J.M.; Gibb, B.E.; Neeren, A.M. Role of Parenting and Maltreatment Histories in Unipolar and Bipolar Mood Disorders: Mediation by Cognitive Vulnerability to Depression. Clin. Child Fam. Psychol. Rev. 2006, 9, 23–64. [Google Scholar] [CrossRef]
- Teicher, M.H.; Andersen, S.L.; Polcari, A.; Anderson, C.M.; Navalta, C.P.; Kim, D.M. The Neurobiological Consequences of Early Stress and Childhood Maltreatment. Neurosci. Biobehav. Rev. 2003, 27, 33–44. [Google Scholar] [CrossRef]
- Demirkol, M.E.; Uğur, K.; Tamam, L. The Mediating Effects of Psychache and Dissociation in the Relationship between Childhood Trauma and Suicide Attempts. Anadolu. Psikiyatri. Derg. 2020, 21, 453–460. [Google Scholar] [CrossRef]
- Savitz, J.B.; van der Merwe, L.; Stein, D.J.; Solms, M.; Ramesar, R.S. Neuropsychological Task Performance in Bipolar Spectrum Illness: Genetics, Alcohol Abuse, Medication and Childhood Trauma. Bipolar Disord. 2008, 10, 79–94. [Google Scholar] [CrossRef]
- McLaughlin, K.A.; Colich, N.L.; Rodman, A.M.; Weissman, D.G. Mechanisms Linking Childhood Trauma Exposure and Psychopathology: A Transdiagnostic Model of Risk and Resilience. BMC Med. 2020, 18, 96. [Google Scholar] [CrossRef] [Green Version]
- Jaworska-Andryszewska, P.; Rybakowski, J.K. Childhood Trauma in Mood Disorders: Neurobiological Mechanisms and Implications for Treatment. Pharmacol. Rep. 2019, 71, 112–120. [Google Scholar] [CrossRef]

{kind=link}
| Variables | N | % |
|---|---|---|
| Sex | ||
| Male | 115 | 53.5 |
| Female | 100 | 46.5 |
| Age—M ± SD | 39.72 ± 14.1 | |
| Marital status | ||
| Married | 65 | 30.2 |
| Divorced or widowed | 27 | 12.6 |
| Single | 123 | 57.2 |
| Job | ||
| Employed | 108 | 50.2 |
| Unemployed | 93 | 43.3 |
| Other | 14 | 6.5 |
| Years of education | ||
| <8 years | 62 | 28.8 |
| 9–15 years | 116 | 54.0 |
| >16 years | 37 | 17.2 |
| Diagnosis | ||
| Schizophrenia and other psychoses | 78 | 36.2 |
| Bipolar disorders | 54 | 25.1 |
| Major depression | 28 | 13.0 |
| Other | 23 | 10.7 |
| Comorbidity | ||
| Personality disorder | 27 | 12.6 |
| Addiction | 5 | 2.3 |
| Severity of suicidal ideation M ± SD | 3.08 ± 2.1 | |
| Lifetime suicide attempt | 118 | 54.9 |
| Emotional abuse M ± SD | 9.69 ± 4.6 | |
| Emotional neglect M ± SD | 12.29 ± 5.1 | |
| Sexual abuse M ± SD | 7.24 ± 4.3 | |
| Physical abuse M ± SD | 7.19 ± 3.5 | |
| Physical neglect M ± SD | 7.80 ± 3.0 | |
| BHS M ± SD | 8.55 ± 5.4 | |
| DES-II M ± SD | 24.4 ± 17.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berardelli, I.; Sarubbi, S.; Rogante, E.; Erbuto, D.; Giuliani, C.; Lamis, D.A.; Innamorati, M.; Pompili, M. Association between Childhood Maltreatment and Suicidal Ideation: A Path Analysis Study. J. Clin. Med. 2022, 11, 2179. https://doi.org/10.3390/jcm11082179
Berardelli I, Sarubbi S, Rogante E, Erbuto D, Giuliani C, Lamis DA, Innamorati M, Pompili M. Association between Childhood Maltreatment and Suicidal Ideation: A Path Analysis Study. Journal of Clinical Medicine. 2022; 11(8):2179. https://doi.org/10.3390/jcm11082179
Chicago/Turabian StyleBerardelli, Isabella, Salvatore Sarubbi, Elena Rogante, Denise Erbuto, Carlotta Giuliani, Dorian A. Lamis, Marco Innamorati, and Maurizio Pompili. 2022. "Association between Childhood Maltreatment and Suicidal Ideation: A Path Analysis Study" Journal of Clinical Medicine 11, no. 8: 2179. https://doi.org/10.3390/jcm11082179
APA StyleBerardelli, I., Sarubbi, S., Rogante, E., Erbuto, D., Giuliani, C., Lamis, D. A., Innamorati, M., & Pompili, M. (2022). Association between Childhood Maltreatment and Suicidal Ideation: A Path Analysis Study. Journal of Clinical Medicine, 11(8), 2179. https://doi.org/10.3390/jcm11082179