
Degenerative and Inflammatory Osteoproliferations in Lumbar Radiographs in Psoriatic Arthritis Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Data Collection
2.3. Ethical Approval
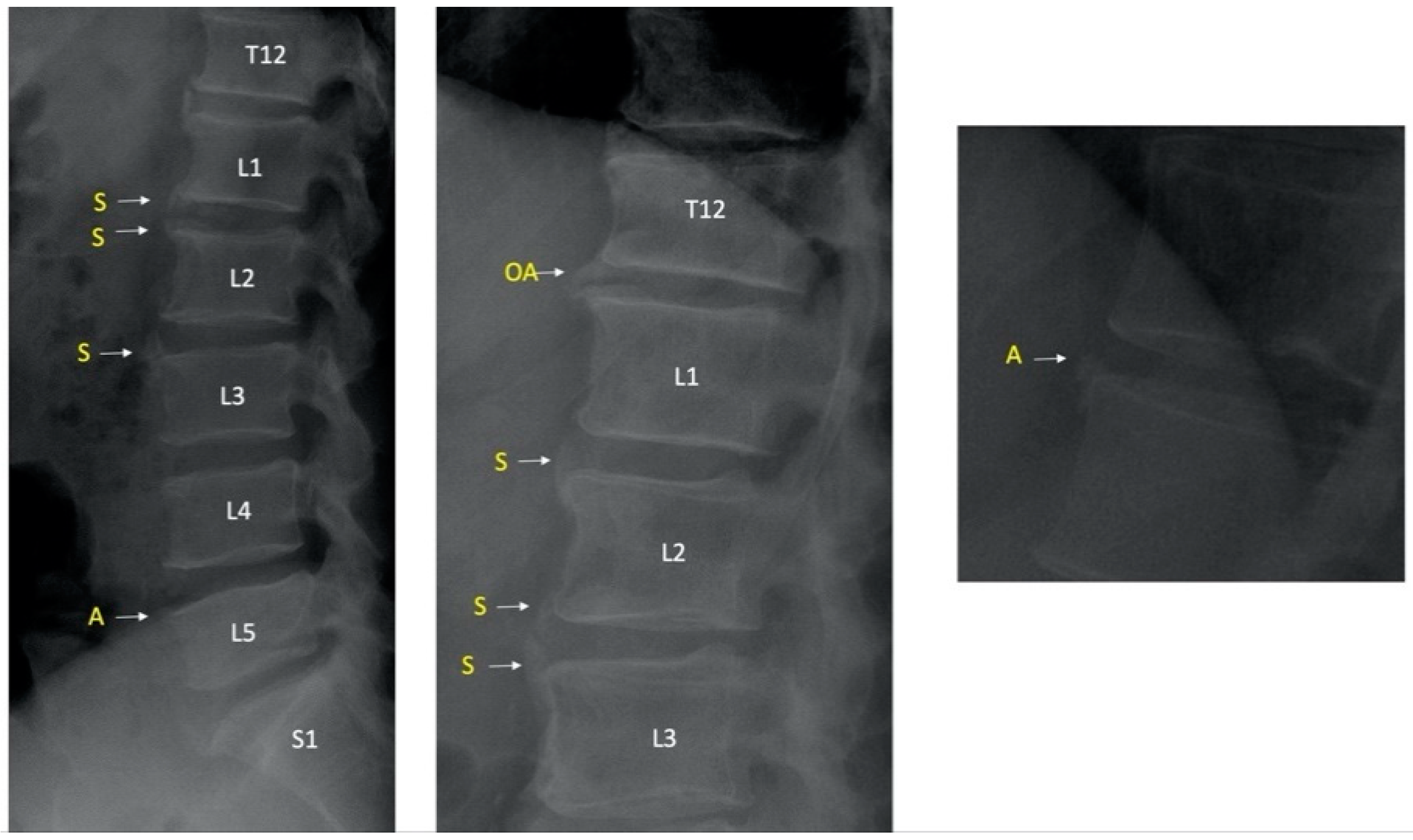
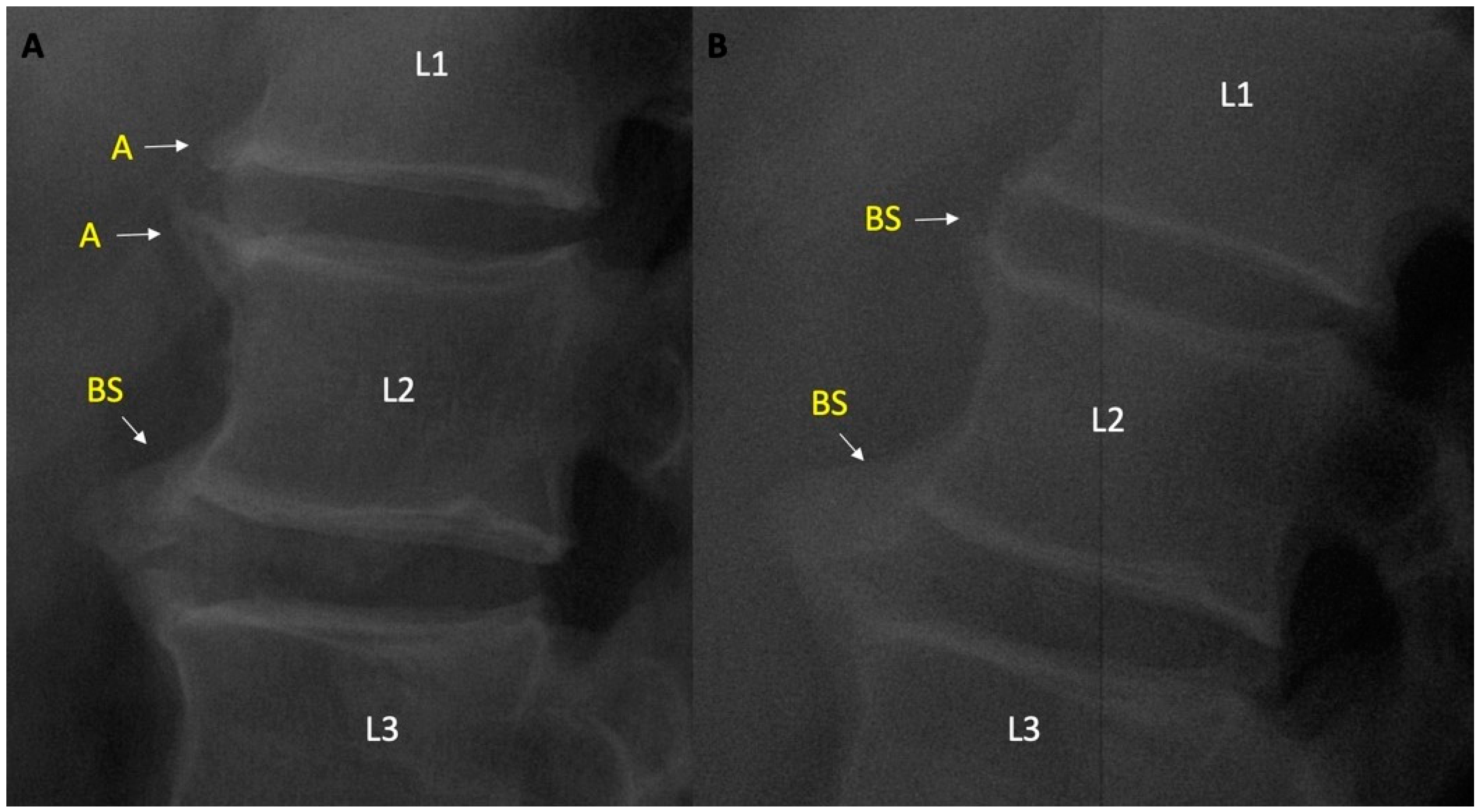
2.4. Pelvic and Lumbar X-ray Readings and Definitions
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Intra- and Interrater Agreement
3.3. Osteophytes on Lateral Lumbar Radiograph in PsA Patients
3.4. Syndesmophytes on Lateral Lumbar Radiograph in PsA Patients
3.5. Ambiguous Lesions on Lateral Lumbar Radiograph in PsA Patients
3.6. AP Lumbar Radiographs in PsA Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Veale, D.J.; Fearon, U. The pathogenesis of psoriatic arthritis. Lancet 2018, 391, 2273–2284. [Google Scholar] [CrossRef]
- Gladman, D.D.; Abufayyah, M.; Salonen, D.; Thavaneswaran, A.; Chandran, V. Radiological characteristics of the calcaneal spurs in psoriatic arthritis. Clin. Exp. Rheumatol. 2014, 32, 401–403. [Google Scholar] [PubMed]
- Finzel, S.; Sahinbegovic, E.; Kocijan, R.; Engelke, K.; Englbrecht, M.; Schett, G. Inflammatory bone spur formation in psoriatic arthritis is different from bone spur formation in hand osteoarthritis. Arthritis Rheumatol. 2014, 66, 2968–2975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathew, A.J.; Østergaard, M. Magnetic Resonance Imaging of Enthesitis in Spondyloarthritis, Including Psoriatic Arthritis-Status and Recent Advances. Front. Med. 2020, 7, 296. [Google Scholar] [CrossRef]
- Taylor, W.J.; Porter, G.G.; Helliwell, P.S. Operational definitions and observer reliability of the plain radiographic features of psoriatic arthritis. J. Rheumatol. 2003, 30, 2645–2658. [Google Scholar]
- Helliwell, P.S.; Hickling, P.; Wright, V. Do the radiological changes of classic ankylosing spondylitis differ from the changes found in the spondylitis associated with inflammatory bowel disease, psoriasis, and reactive arthritis? Ann. Rheum. Dis. 1998, 57, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Biagioni, B.J.; Gladman, D.D.; Cook, R.J.; Eder, L.; Wakhlu, A.; Shen, H.; Chandran, V. Reliability of radiographic scoring methods in axial psoriatic arthritis. Arthritis Care Res. 2014, 66, 1417–1422. [Google Scholar] [CrossRef] [Green Version]
- Baraliakos, X.; Listing, J.; Rudwaleit, M.; Haibel, H.; Brandt, J.; Sieper, J.; Braun, J. Progression of radiographic damage in patients with ankylosing spondylitis: Defining the central role of syndesmophytes. Ann. Rheum. Dis. 2007, 66, 910–915. [Google Scholar] [CrossRef] [PubMed]
- Lane, N.E.; Nevitt, M.C.; Genant, H.K.; Hochberg, M.C. Reliability of new indices of radiographic osteoarthritis of the hand and hip and lumbar disc degeneration. J. Rheumatol. 1993, 20, 1911–1918. [Google Scholar] [PubMed]
- Creemers, M.C.; Franssen, M.J.; van’t Hof, M.A.; Gribnau, F.W.; van de Putte, L.B.; van Riel, P.L. Assessment of outcome in ankylosing spondylitis: An extended radiographic scoring system. Ann. Rheum. Dis. 2005, 64, 127–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Heijde, D.; Braun, J.; Deodhar, A.; Baraliakos, X.; Landewé, R.; Richards, H.B.; Porter, B.; Readie, A. Modified stoke ankylosing spondylitis spinal score as an outcome measure to assess the impact of treatment on structural progression in ankylosing spondylitis. Rheumatology 2019, 58, 388–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lubrano, E.; Marchesoni, A.; Olivieri, I.; D’Angelo, S.; Spadaro, A.; Parsons, W.J.; Cauli, A.; Salvarani, C.; Mathieu, A.; Porter, G.; et al. Psoriatic arthritis spondylitis radiology index: A modified index for radiologic assessment of axial involvement in psoriatic arthritis. J. Rheumatol. 2009, 36, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.; Gladman, D.D.; Thavaneswaran, A.; Eder, L.; Helliwell, P.; Cook, R.J.; Chandran, V. Sensitivity and Specificity of Radiographic Scoring Instruments for Detecting Change in Axial Psoriatic Arthritis. Arthritis Care Res. 2017, 69, 1700–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, S.; Wang, R.; Ward, M.M. Syndesmophyte growth in ankylosing spondylitis. Curr. Opin. Rheumatol. 2015, 27, 326–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, W.; Gladman, D.; Helliwell, P.; Marchesoni, A.; Mease, P.; Mielants, H. Classification criteria for psoriatic arthritis: Development of new criteria from a large international study. Arthritis Rheum 2006, 54, 2665–2673. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Schepper, E.I.; Damen, J.; van Meurs, J.B.; Ginai, A.Z.; Popham, M.; Hofman, A.; Koes, B.; Bierma-Zeinstra, S. The association between lumbar disc degeneration and low back pain: The influence of age, gender, and individual radiographic features. Spine 2010, 35, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.M. An Ongoing Assessment of Osteoarthritis in African Americans and Caucasians in North Carolina: The Johnston County Osteoarthritis Project. Trans. Am. Clin. Climatol. Assoc. 2015, 126, 77–86. [Google Scholar] [PubMed]
- Amoruso, G.F.; Nisticò, S.P.; Iannone, L.; Russo, E.; Rago, G.; Patruno, C.; Bennardo, L. Ixekizumab May Improve Renal Function in Psoriasis. Healthcare 2021, 9, 543. [Google Scholar] [CrossRef] [PubMed]
- Dastoli, S.; Nisticò, S.P.; Morrone, P.; Patruno, C.; Leo, A.; Citraro, R.; Gallelli, L.; Russo, E.; De Sarro, G.; Bennardo, L. Colchicine in Managing Skin Conditions: A Systematic Review. Pharmaceutics 2022, 14, 294. [Google Scholar] [CrossRef]
- Gossec, L.; Baraliakos, X.; Kerschbaumer, A.; de Wit, M.; McInnes, I.; Dougados, M.; Primdahl, J.; McGonagle, D.G.; Aletaha, D.; Balanescu, A.; et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann. Rheum. Dis. 2020, 79, 700–712. [Google Scholar] [CrossRef] [PubMed]
- Jadon, D.R.; Sengupta, R.; Nightingale, A.; Lindsay, M.; Korendowych, E.; Robinson, G.; Jobling, A.; Shaddick, G.; Bi, J.; Winchester, R.; et al. Axial Disease in Psoriatic Arthritis study: Defining the clinical and radiographic phenotype of psoriatic spondyloarthritis. Ann. Rheum. Dis. 2017, 76, 701–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Tubergen, A.; Ramiro, S.; van der Heijde, D.; Dougados, M.; Mielants, H.; Landewé, R. Development of new syndesmophytes and bridges in ankylosing spondylitis and their predictors: A longitudinal study. Ann. Rheum. Dis. 2012, 71, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Feld, J.; Ye, J.Y.; Chandran, V.; Inman, R.D.; Haroon, N.; Cook, R.; Gladman, D.D. Axial Disease in Psoriatic arthritis: The presence and progression of unilateral grade 2 sacroiliitis in a psoriatic arthritis cohort. Semin. Arthritis Rheum. 2021, 51, 464–468. [Google Scholar] [CrossRef] [PubMed]
- Coates, L.C.; Baraliakos, X.; Blanco, F.J.; Blanco-Morales, E.A.; Braun, J.; Chandran, V.; Fernandez-Sueiro, J.L.; FitzGerald, O.; Gallagher, P.; Gladman, D.D. The Phenotype of Axial Spondyloarthritis: Is It Dependent on HLA-B27 Status? Arthritis Care Res. 2021, 73, 856–860. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.H.; Raj, S.; Chen, C.H.; Hung, K.H.; Chou, C.T.; Chen, I.H.; Chien, J.T.; Lin, I.Y.; Yang, S.Y.; Angata, T.; et al. HLA-B27-mediated activation of TNAP phosphatase promotes pathogenic syndesmophyte formation in ankylosing spondylitis. J. Clin. Invest. 2019, 129, 5357–5373. [Google Scholar] [CrossRef] [PubMed]
- Queiro, R.; Sarasqueta, C.; Belzunegui, J.; Gonzalez, C.; Figueroa, M.; Torre-Alonso, J.C. Psoriatic spondyloarthropathy: A comparative study between HLA-B27 positive and HLA-B27 negative disease. Semin. Arthritis Rheum. 2002, 31, 413–418. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| All Patients n = 182 | Patients with Normal Lumbar Radiograph n = 71 | Patients with Any Syndesmophyte n = 44 | Patients with ≥Grade 2 Osteophyte n = 33 | Patients with Ambiguous Lesions n = 13 | |
|---|---|---|---|---|---|
| Female gender, n (%) | 126 (69.2) | 44 (62.0) | 28 (63.6) | 25 (75.8) | 8 (61.5) |
| Age at the time of lumbar radiograph, mean (SD), years | 44.8 (12.8) | 39.6 (12.8) | 46.7 (9.9) | 52.4 (11.7) | 50.9 (8) |
| PsA diagnosis age, mean (SD), years | 39.7 (12.7) | 34.8 (12.3) | 41.8 (10.7) | 48.0 (11.2) | 45.5 (9.7) |
| PsA disease duration until first lumbar radiograph, mean (SD), years | 4.8 (6.2) | 4.9 (5.4) | 4.8 (7.2) | 3.2 (7.8) | 5 (7.9) |
| PsO disease duration until first lumbar radiograph, mean (SD), years | 13. 7 (11.4) | 14.8 (11.5) | 13.4 (11.2) | 12.4 (13.1) | 14.2 (9.6) |
| PsO/PsA family history, n (%) | 45 (40.5) | 15 (34.9) | 14 (50.0) | 9 (47.4) | 3 (33.3) |
| PsO start > 40 age, n (%) | 41 (28.9) | 6 (11.1) | 9 (25.7) | 16 (59.3) | 5 (55.6) |
| BMI, mean (SD) BMI > 30, n (%) | 29.1 (5.6) 76 (42.2) | 27.7 (5.3) 23 (32.2) | 29.7 (5.8) 21 (47.7) | 30.8 (5.5) 21 (63.6) | 32 (4.1) 8 (61.5) |
| Smoking (ever), n (%) | 105 (58.3) | 46 (65.7) | 27 (61.4) | 19 (57.6) | 8 (61.5) |
| CCI = 0, n (%) CCI = 1, n (%) CCI > 1, n (%) | 90 (51.1) 41 (23.3) 45 (25.5) | 45 (64.3) 13 (18.6) 12 (17.0) | 19 (46.3) 12 (29.3) 10 (24.3) | 8 (25.0) 11 (34.4) 13 (40.0) | 3 (23.1) 5 (38.5) 5 (38.5) |
| RF positivity, n (%) | 19 (15.0) | 7 (14.3) | 6 (20.0) | 3 (13.0) | 2 (18.2) |
| Anti-CCP positivity, n (%) | 8 (10.7) | 2 (9.5) | 4 (20.0) | 2 (11.8) | 1 (14.3) |
| HLA-B27 positivity, n (%) | 13 (20.6) | 7 (21.9) | 4 (25.0) | 1 (12.5) | 0 (0) |
| Dactylitis (ever), n (%) | 37 (30.6) | 16 (34.0) | 8 (25.8) | 8 (32.0) | 5 (50.0) |
| Enthesitis (ever), n (%) | 34 (37.0) | 14 (36.8) | 7 (30.4) | 10 (50.0) | 2 (28.6) |
| Nail involvement, n (%) | 46 (41.4) | 22 (48.9) | 9 (32.1) | 6 (28.6) | 1 (11.1) |
| Sacroiliitis according to mNY criteria, n (%) | 112 (61.5) | 44 (62.0) | 35 (79.5) | 19 (57.6) | 8 (61.5) |
| Ischium ≥ grade 2, n (%) | 45 (34.1) | 16 (31.4) | 14 (31.8) | 10 (38.5) | 2 (25) |
| Iliac wing ≥ grade 2, n (%) | 18 (13.1) | 2 (3.6) | 8 (18.2) | 8 (29.6) | 3 (37.5) |
| All Patients n = 182 | Patients with Normal Lumbar Radiograph n = 71 | Patients with Any Syndesmophyte n = 44 | Patients with ≥Grade 2 Osteophyte n = 33 | Patients with Ambiguous Lesions n = 13 | ||
|---|---|---|---|---|---|---|
| BASDAI, mean (SD) | Baseline | 6.1 (2.1) | 6.3 (2.1) | 5.8 (1.9) | 6.6 (2.1) | 7.2 (1.7) |
| Last visit | 4.4 (2.5) | 4.2 (2.7) | 4.6 (2.5) | 4.9 (2.6) | 4.9 (1.8) | |
| BASDAI > 4, n (%) | Baseline | 92 (83.6) | 36 (83.7) | 12 (27.2) | 20 (95.2) | 6 (100) |
| Last visit | 80 (53) | 28 (46.7) | 19 (51.4) | 16 (61.5) | 8 (72.7) | |
| BASFI, mean (SD) | Baseline | 4.4 (2.5) | 4.3 (2.6) | 4.3 (2.8) | 5.1 (3.2) | 5.9 (2.7) |
| Last visit | 3.6 (2.5) | 3.2 (2.6) | 3.6 (2.6) | 4.3 (2.6) | 3.9 (2.8) | |
| BASFI > 4, n (%) | Baseline | 56 (53.8) | 19 (46.3) | 12 (48) | 13 (65) | 4 (66.7) |
| Last visit | 59 (42.8) | 18 (35.3) | 14 (37.8) | 15 (55.6) | 6 (46.2) | |
| DAS-28, mean (SD) | Baseline | 3.7 (1.3) | 3.5 (1.3) | 3.7 (1.3) | 4.4 (1.3) | 4.5 (1.3) |
| Last visit | 2.7 (1.3) | 2.5 (1.2) | 2.9 (1.5) | 3.1 (1.4) | 2.9 (1.4) | |
| DAPSA-28, mean (SD) | Baseline | 19.2 (9.7) | 18.8 (8.6) | 17.1 (10.9) | 21.2 (13.6) | 24.3 (13.9) |
| Last visit | 11.5 (9.4) | 11.5 (8.7) | 11.2 (11.9) | 13.1 (10.3) | 11.8 (9.1) | |
| CRP, mean (SD) | Baseline | 1.9 (2.6) | 1.5 (1.9) | 2.2 (2.8) | 1.9 (3.1) | 2.9 (3.8) |
| Last visit | 0.8 (1.4) | 1.0 (1.7) | 0.7 (1.0) | 1.1 (1.9) | 0.9 (0.7) | |
| CRP, >0.8, n (%) | Baseline | 84 (57.1) | 30 (51.7) | 21 (58.3) | 20 (71.4) | 9 (81.8) |
| Last visit | 48 (27.9) | 22 (32.4) | 9 (22.0) | 13 (41.9) | 6 (46.2) | |
| HAQ-DI, mean (SD) | Baseline | 0.75 (0.58) | 0.68 (0.58) | 0.73 (0.52) | 0.89 (0.67) | 1.1 (0.6) |
| Last visit | 0.53 (0.54) | 0.43 (0.45) | 0.61 (0.60) | 0.73 (0.69) | 0.83 (0.51) | |
| HAQ-DI < 0.5, n (%) | Baseline | 43 (46.7) | 21 (51.2) | 10 (52.6) | 8 (42.1) | 2 (40.0) |
| Last visit | 97 (56.4) | 41 (61.2) | 23 (53.5) | 15 (46.9) | 4 (30.8) | |
| HAQ > 1.0, n (%) | Baseline | 29 (31.5) | 12 (29.3) | 6 (31.6) | 9 (47.4) | 3 (60.0) |
| Last visit | 36 (20.9) | 9 (13.4) | 11 (25.6) | 11 (34.4) | 7 (53.8) | |
| Last visit DAS-28 remission, n (%) | 92 (53.8) | 40 (59.7) | 20 (48.8) | 12 (38.7) | 6 (46.2) | |
| Last visit DAPSA-28 remission, n (%) | 45 (26.3) | 17 (25.4) | 11 (26.8) | 7 (22.6) | 2 (15.4) | |
| Location | Osteophyte | Osteophyte ≥ 2 | Corner SP | Bridging SP | All SP | Erosion, Sclerosis, Squaring | Ambiguous |
|---|---|---|---|---|---|---|---|
| T12, L, n (%) | 7 (3.8) | 1 (0.5) | 9 (4.9) | 5 (2.7) | 14 (7.7) | 3 (1.6) | 2 (1.1) |
| L1, U, n (%) | 6 (3.3) | 0 (0) | 10 (5.5) | 5 (2.7) | 15 (8.2) | 2 (1.1) | 2 (1.1) |
| L1, L, n (%) | 10 (5.5) | 6 (3.3) | 8 (4.4) | 6 (3.3) | 14 (7.7) | 4 (2.2) | 0 (0) |
| L2, U, n (%) | 15 (8.2) | 8 (4.4) | 8 (4.4) | 7 (3.8) | 15 (8.2) | 4 (2.2) | 4 (2.2) |
| L2, L, n (%) | 16 (8.8) | 6 (3.3) | 5 (2.7) | 6 (3.3) | 11 (6.0) | 4 (2.2) | 0 (0) |
| L3, U, n (%) | 31 (17.0) | 13 (7.1) | 4 (2.2) | 6 (3.3) | 10 (5.5) | 10 (5.5) | 2 (1.1) |
| L3, L, n (%) | 17 (9.3) | 8 (4.4) | 3 (1.6) | 5 (2.7) | 8 (4.4) | 5 (2.7) | 2 (1.1) |
| L4, U, n (%) | 37 (20.3) | 14 (7.7) | 8 (4.4) | 5 (2.1) | 13 (7.1) | 11 (6.0) | 4 (2.2) |
| L4, L, n (%) | 10 (5.5) | 1 (0.5) | 3 (1.6) | 1 (0.5) | 4 (2.2) | 6 (3.3) | 4 (2.2) |
| L5, U, n (%) | 24 (13.2) | 8 (4.4) | 1 (0.5) | 1 (0.5) | 2 (1.1) | 1 (0.5) | 1 (0.5) |
| L5, L, n (%) | 8 (4.4) | 3 (1.6) | 1 (0.5) | 1 (0.5) | 2 (1.1) | 0 (0) | 0 (0) |
| S1, U, n (%) | 3 (1.6) | 3 (1.6) | 0 (0) | 1 (0.5) | 1 (0.5) | 0 (0) | 0 (0) |
| All vertebral corners (n = 2184) | 184 (8.4) | 75 (3.4) | 60 (2.7) | 49 (2.2) | 109 (4.9) | 50 (2.2) | 21 (1.0) |
| All patients | 77 (42.3) | 33 (18.1) | 36 (19.8) | 17 (9.3) | 44 (24.2) | 22 (12.1) | 13 (4.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayan, G.; Sadic, A.; Kilic, L.; Kalyoncu, U. Degenerative and Inflammatory Osteoproliferations in Lumbar Radiographs in Psoriatic Arthritis Patients. J. Clin. Med. 2022, 11, 2009. https://doi.org/10.3390/jcm11072009
Ayan G, Sadic A, Kilic L, Kalyoncu U. Degenerative and Inflammatory Osteoproliferations in Lumbar Radiographs in Psoriatic Arthritis Patients. Journal of Clinical Medicine. 2022; 11(7):2009. https://doi.org/10.3390/jcm11072009
Chicago/Turabian StyleAyan, Gizem, Abdurrahman Sadic, Levent Kilic, and Umut Kalyoncu. 2022. "Degenerative and Inflammatory Osteoproliferations in Lumbar Radiographs in Psoriatic Arthritis Patients" Journal of Clinical Medicine 11, no. 7: 2009. https://doi.org/10.3390/jcm11072009
APA StyleAyan, G., Sadic, A., Kilic, L., & Kalyoncu, U. (2022). Degenerative and Inflammatory Osteoproliferations in Lumbar Radiographs in Psoriatic Arthritis Patients. Journal of Clinical Medicine, 11(7), 2009. https://doi.org/10.3390/jcm11072009