Prosthesis–Patient Mismatch in Small Aortic Annuli: Self-Expandable vs. Balloon-Expandable Transcatheter Aortic Valve Replacement

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Procedure
2.3. PPM Definition
2.4. Paravalvular Leak Definition
2.5. Small Aortic Annulus Definition
2.6. Follow Up
2.7. Endpoints
2.8. Statistical Analysis
3. Results
3.1. Occurrence of Moderate or Severe PPM at One Month
3.2. Occurrence of Paravalvular Leak at One Month and Pacemaker Implantation during the Thirty-First Days
4. Discussion
- (1)
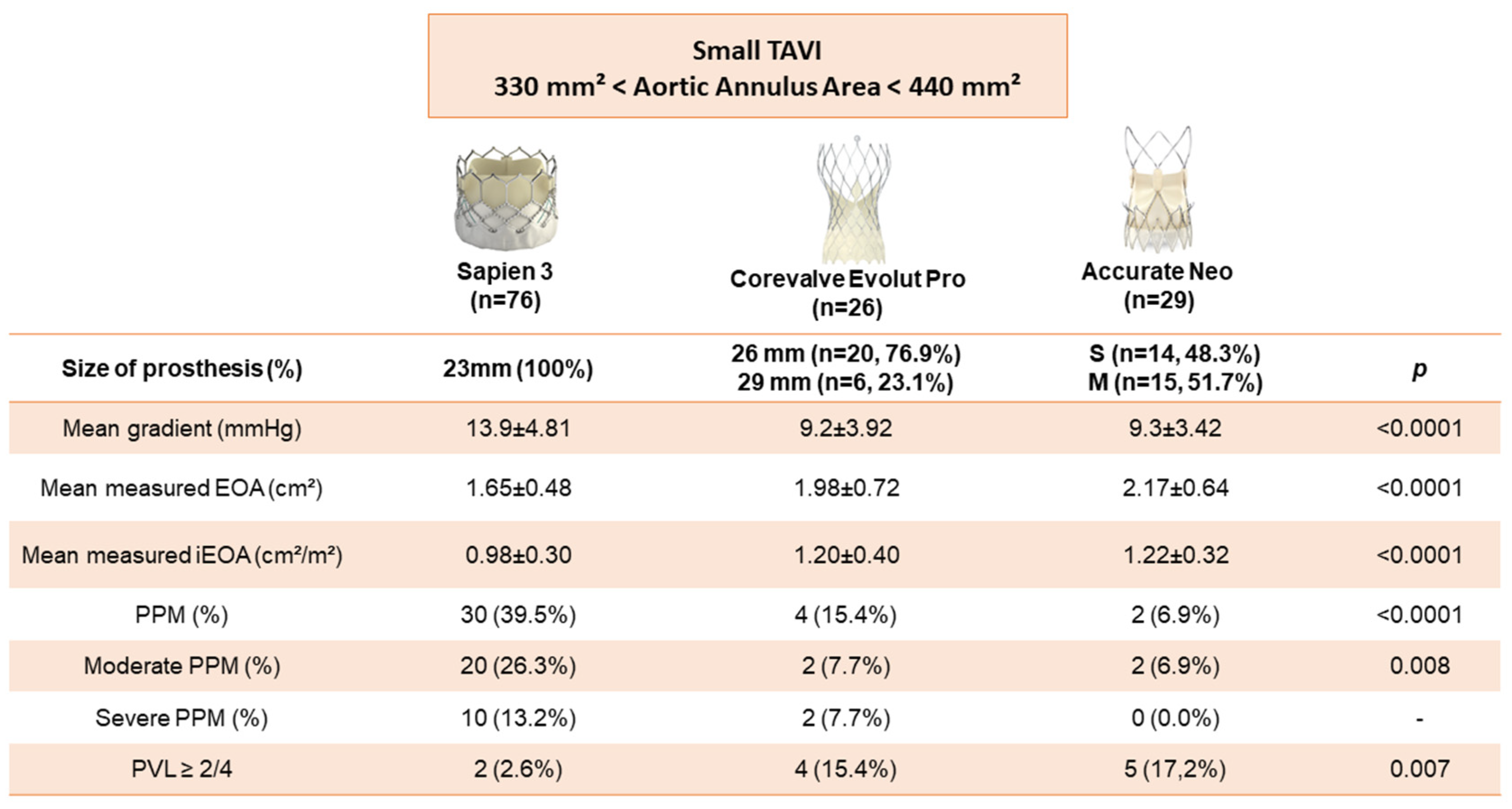
- PPM was more often observed with BE TAVR than with SE TAVR and mean gradients were higher with BE TAVR
- (2)
- The majority of paravalvular leaks ≥ 2/4 occurred with SE TAVR compared to BE TAVR
Strength and Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| TAVR | transcatheter aortic valve replacement |
| SAVR | surgical aortic valve replacement |
| PPM | prosthesis–patient mismatch |
| BE | balloon-expandable |
| SE | self-expandable |
| CT | computed tomography |
| EOA | effective orifice area |
| LVEF | left ventricular ejection fraction |
| VARC | Valve Academic Research Consortium |
| iEOA | indexed EOA |
| LVOT | left ventricular outflow tract obstruction |
| LVOT VTI | left ventricular outflow tract obstruction velocity time integral |
References
- Carroll, J.D.; Mack, M.J.; Vemulapalli, S.; Herrmann, H.C.; Gleason, T.G.; Hanzel, G.; Deeb, G.M.; Thourani, V.H.; Cohen, D.J.; Desai, N.; et al. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2020, 76, 2492–2516. [Google Scholar] [CrossRef] [PubMed]
- Blais, C.; Dumesnil, J.G.; Baillot, R.; Simard, S.; Doyle, D.; Pibarot, P. Impact of valve prosthesis-patient mismatch on short-term mortality after aortic valve replacement. Circulation 2003, 108, 983–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pibarot, P.; Dumesnil, J.G. Prosthesis-patient mismatch: Definition, clinical impact, and prevention. Heart 2006, 92, 1022–1029. [Google Scholar] [CrossRef] [PubMed]
- Tasca, G.; Mhagna, Z.; Perotti, S.; Centurini, P.B.; Sabatini, T.; Amaducci, A.; Brunelli, F.; Cirillo, M.; Tomba, M.D.; Quiani, E.; et al. Impact of prosthesis-patient mismatch on cardiac events and midterm mortality after aortic valve replacement in patients with pure aortic stenosis. Circulation 2006, 113, 570–576. [Google Scholar] [CrossRef] [Green Version]
- Mohty, D.; Dumesnil, J.G.; Echahidi, N.; Mathieu, P.; Dagenais, F.; Voisine, P.; Pibarot, P. Impact of prosthesis-patient mismatch on long-term survival after aortic valve replacement: Influence of age, obesity, and left ventricular dysfunction. J. Am. Coll. Cardiol. 2009, 53, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Head, S.J.; Mokhles, M.M.; Osnabrugge, R.L.; Pibarot, P.; Mack, M.J.; Takkenberg, J.; Bogers, A.J.; Kappetein, A.P. The impact of prosthesis-patient mismatch on long-term survival after aortic valve replacement: A systematic review and meta-analysis of 34 observational studies comprising 27,186 patients with 133,141 patient-years. Eur. Heart J. 2012, 33, 1518–1529. [Google Scholar] [CrossRef] [Green Version]
- Pibarot, P.; Weissman, N.J.; Stewart, W.J.; Hahn, R.; Lindman, B.; McAndrew, T.; Kodali, S.K.; Mack, M.J.; Thourani, V.H.; Miller, D.C.; et al. Incidence and sequelae of prosthesis-patient mismatch in transcatheter versus surgical valve replacement in high-risk patients with severe aortic stenosis: A PARTNER trial cohort—A analysis. J. Am. Coll. Cardiol. 2014, 64, 1323–1334. [Google Scholar] [CrossRef] [Green Version]
- Miyasaka, M.; Tada, N.; Taguri, M.; Kato, S.; Enta, Y.; Otomo, T.; Hata, M.; Watanabe, Y.; Naganuma, T.; Araki, M.; et al. Incidence, Predictors, and Clinical Impact of Prosthesis-Patient Mismatch Following Transcatheter Aortic Valve Replacement in Asian Patients: The OCEAN-TAVI Registry. JACC Cardiovasc. Interv. 2018, 11, 771–780. [Google Scholar] [CrossRef]
- Herrmann, H.C.; Daneshvar, S.A.; Fonarow, G.C.; Stebbins, A.; Vemulapalli, S.; Desai, N.D.; Malenka, D.J.; Thourani, V.H.; Rymer, J.; Kosinski, A.S. Prosthesis-Patient Mismatch in Patients Undergoing Transcatheter Aortic Valve Replacement: From the STS/ACC TVT Registry. J. Am. Coll. Cardiol. 2018, 72, 2701–2711. [Google Scholar] [CrossRef]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Kurz, T.; Feistritzer, H.-J.; Stachel, G.; Hartung, P.; Eitel, I.; Marquetand, C.; Nef, H.; Doerr, O.; Lauten, A.; et al. Comparison of newer generation self-expandable vs. balloon-expandable valves in transcatheter aortic valve implantation: The randomized SOLVE-TAVI trial. Eur. Heart J. 2020, 41, 1890–1899. [Google Scholar] [CrossRef] [PubMed]
- VARC-3 Writing Committee; Généreux, P.; Piazza, N.; Alu, M.C.; Nazif, T.; Hahn, R.T.; Pibarot, P.; Bax, J.J.; Leipsic, J.A.; Blanke, P.; et al. Valve Academic Research Consortium 3, updated endpoint definitions for aortic valve clinical research. Eur. Heart J. 2021, 42, 1825–1857. [Google Scholar] [CrossRef] [PubMed]
- Pibarot, P.; Magne, J.; Leipsic, J.; Côté, N.; Blanke, P.; Thourani, V.H.; Hahn, R. Imaging for Predicting and Assessing Prosthesis-Patient Mismatch After Aortic Valve Replacement. JACC Cardiovasc. Imaging 2019, 12, 149–162. [Google Scholar] [CrossRef]
- Theron, A.; Pinto, J.; Grisoli, D.; Griffiths, K.; Salaun, E.; Jaussaud, N.; Ravis, E.; Lambert, M.; Messous, L.; Amanatiou, C.; et al. Patient-prosthesis mismatch in new generation trans-catheter heart valves: A propensity score analysis. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 225–233. [Google Scholar] [CrossRef] [Green Version]
- Abdelghani, M.; Mankerious, N.; Allali, A.; Landt, M.; Kaur, J.; Sulimov, D.S.; Merten, C.; Sachse, S.; Mehilli, J.; Neumann, F.-J.; et al. Bioprosthetic Valve Performance After Transcatheter Aortic Valve Replacement with Self-Expanding Versus Balloon-Expandable Valves in Large Versus Small Aortic Valve Annuli: Insights from the CHOICE Trial and the CHOICE-Extend Registry. JACC Cardiovasc. Interv. 2018, 11, 2507–2518. [Google Scholar] [CrossRef]
- Hase, H.; Yoshijima, N.; Yanagisawa, R.; Tanaka, M.; Tsuruta, H.; Shimizu, H.; Fukuda, K.; Naganuma, T.; Mizutani, K.; Yamawaki, M.; et al. Transcatheter aortic valve replacement with Evolut R versus Sapien 3 in Japanese patients with a small aortic annulus: The OCEAN-TAVI registry. Catheter. Cardiovasc. Interv. 2021, 97, E875–E886. [Google Scholar] [CrossRef]
- Tang, G.H.; Sengupta, A.; Alexis, S.L.; Bapat, V.N.; Adams, D.H.; Sharma, S.K.; Kini, A.S.; Kodali, S.K.; Ramlawi, B.; Gada, H.; et al. Outcomes of Prosthesis-Patient Mismatch Following Supra-Annular Transcatheter Aortic Valve Replacement: From the STS/ACC TVT Registry. JACC Cardiovasc. Interv. 2021, 14, 964–976. [Google Scholar] [CrossRef]
- Leone, P.P.; Regazzoli, D.; Pagnesi, M.; Sanz-Sanchez, J.; Chiarito, M.; Cannata, F.; Van Mieghem, N.M.; Barbanti, M.; Tamburino, C.; Teles, R.; et al. Predictors and Clinical Impact of Prosthesis-Patient Mismatch After Self-Exapndable TAVR in Small Annuli. JACC Cardiovasc. Interv. 2021, 14, 1218–1228. [Google Scholar] [CrossRef]
- Clavel, M.A.; Rodés-Cabau, J.; Dumont, É.; Bagur, R.; Bergeron, S.; De Larochellière, R.; Doyle, D.; Larose, É.; Dumesnil, J.G.; Pibarot, P. Validation and characterization of transcatheter aortic valve effective orifice area measured by Doppler echocardiography. JACC Cardiovasc. Imaging 2011, 4, 1053–1062. [Google Scholar] [CrossRef] [Green Version]
- Ternacle, J.; Guimaraes, L.; Vincent, F.; Côté, N.; Côté, M.; Lachance, D.; Clavel, M.-A.; Abbas, A.E.; Pibarot, P.; Rodés-Cabau, J. Reclassification of prosthesis-patient mismatch after transcatheter aortic valve replacement using predicted vs. measured indexed effective orifice area. Eur. Heart J. Cardiovasc. Imaging 2020, 22, 11–20. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics at the Baseline | General Population n = 131 | Sapiens 3TM n = 76 | Evolut ProTM n = 26 | Accurate NeoTM n = 29 | p Value |
|---|---|---|---|---|---|
| Age-yr | 82.5 ± 7.06 | 82.45 ± 7.28 | 80.35 ± 6.96 | 84.59 ± 6.10 | 0.52 |
| Male sex–no (%) | 30/131 (22.90%) | 16/76 (21.05%) | 6/26 (23.08%) | 8/29 (27.59%) | 0.78 |
| Body surface–m2 | 1.74 ± 0.25 | 1.76 ± 0.31 | 1.68 ± 0.17 | 1.77 ± 0.20 | 0.63 |
| BMI-kg/m2 | 25.73 ± 4.76 | 25.24 ± 4.33 | 25.83 ± 4.07 | 26.93 ± 6.15 | 0.26 |
| EuroSCORE II | 3.92 ± 2.99 | 4.17 ± 3.05 | 3.52 ± 3.87 | 3.59 ± 1.73 | 0.51 |
| Diabetes mellitus-no./total no. (%) | 28/131 (21.37%) | 17/76 (22.37%) | 5/26 (19.23%) | 6/29 (20.69%) | 0.94 |
| Hypertension-no./total no. (%) | 91/131 (69.47%) | 55/76 (72.37%) | 17/26 (65.38%) | 19/29 (65.52%) | 0.70 |
| Dyslipidemia-no./total no. (%) | 68/131 (51.91%) | 42/76 (55.26%) | 12/26 (46.15%) | 14/29 (48.28%) | 0.79 |
| Dialysis-no./total no. (%) | 4/131 (3.05%) | 2/76 (2.63%) | 1/26 (3.85%) | 1/29 (3.45%) | 0.94 |
| COPD-no./total no. (%) | 17/131 (12.98%) | 10/76 (13.16%) | 2/26 (7.69%) | 5/29 (17.24%) | 0.57 |
| Smoke-no./total no. (%) | 42/131 (32.06%) | 25/76 (32.89%) | 7/26 (26.92%) | 10/29 (34.48%) | 0.81 |
| CAD-no./total no. (%) | 51/131 (38.93%) | 34/76 (44.74%) | 7/26 (26.92%) | 10/29 (34.48%) | 0.27 |
| Atrial fibrillation-no./total no. (%) | 46/131 (35.11%) | 28/76 (36.84%) | 8/26 (30.77%) | 10/29 (34.48%) | 0.85 |
| Cancer-no./total no. (%) | 23/131 (17.56%) | 13/76 (17.11%) | 4/26 (15.38%) | 6/29 (20.69%) | 0.86 |
| NYHA: | 0.31 | ||||
| 54/131 (41.22%) 63/131 (48.09%) 14/131 (10.69%) | 34/76 (44.74%) 32/76 (42.10%) 10/76 (13.16%) | 7/26 (26.92%) 17/26 (65.38%) 2/26 (7.69%) | 13/29 (44.83%) 14/29 (48.28%) 2/29 (6.90%) |
| Echocardiography Data at the Baseline and Access Data | General Population n = 131 | Sapiens 3TM n = 76 | Evolut ProTM n = 26 | Accurate NeoTM n = 29 | p Value |
|---|---|---|---|---|---|
| LVEF-no./total no. (%) | 60.11 ± 11.82 | 60.83 ± 10.03 | 60.15 ± 10.74 | 63.28 ± 9.35 | 0.45 |
| Mean trans-aortic gradient-mmHg | 54.27 ± 15.37 | 55.18 ± 17.58 | 52.62 ± 11.75 | 53.38 ± 11.83 | 0.72 |
| EOA-cm2 | 0.68 ± 0.17 | 0.68 ± 0.17 | 0.68 ± 0.19 | 0.71 ± 0.17 | 0.66 |
| iEAO–cm2/m2 | 0.40 ± 0.11 | 0.40 ± 0.11 | 0.41 ± 0.10 | 0.40 ± 0.09 | 0.82 |
| Aortic annulus area-no./total no. (%) | 378.69 ± 27.45 | 373.76 ± 27.30 | 383.14 ± 29.00 | 383.76 ± 25.52 | 0.06 |
| Transfemoral access-no./total no. (%) | 128/131 (99.2%) | 75/76 (98.68%) | 26/26 (100%) | 29/29 (100%) | 0.70 |
| Echocardiography Data at One Month | General Population n = 131 | Sapiens 3TM n = 76 | Evolut ProTM n = 26 | Accurate NeoTM n = 29 | p Value |
|---|---|---|---|---|---|
| LVEF-% | 63.30 ± 8.06 | 62.78 ± 7.90 | 63.77 ± 10.16 | 64.24 ± 6.33 | 0.67 |
| Mean trans-aortic gradient-mmHg | 11.98 ± 4.92 | 13.92 ± 4.81 | 9.20 ± 3.92 | 9.31 ± 3.42 | <0.001 |
| EOA-cm2 | 1.83 ± 0.60 | 1.65 ± 0.48 | 1.98 ± 0.72 | 2.17 ± 0.64 | <0.001 |
| iEAO–cm2/m2 | 1.08 ± 0.35 | 0.98 ± 0.30 | 1.20 ± 0.40 | 1.22 ± 0.32 | <0.001 |
| PPM-no./total no. (%) | 36/131 (27.48%) | 30/76 (39.5%) | 4/26 (15.4%) | 2/29 (6.9%) | <0.001 |
| Moderate PPM-no./total no. (%) | 24/131 (18.32%) | 20/76 (26.3%) | 2/26 (7.7%) | 2/29 (6.9%) | 0.008 |
| Severe PPM-no./total no. (%) | 12/131 (9.16%) | 10/76 (13.2%) | 2/26 (7.7%) | 0/29 (0.0%) | 0.06 |
| Paravalvular leak ≥ 2-no./total no. (%) | 11/131 (8.40%) | 2/76 (2.6%) | 4/26 (15.4%) | 5/29 (17.2%) | 0.007 |
| Post Procedural Complication | General Population n = 131 | Sapiens 3TM n = 76 | Evolut ProTM n = 26 | Accurate NeoTM n = 29 | p Value |
|---|---|---|---|---|---|
| Pacemaker-no./total no. (%) | 23/131 (17.56%) | 14/76 (18.42%) | 4/26 (15.38%) | 5/29 (17.2%) | 0.93 |
| Vascular complication-no./total no. (%) | 11/131 (8.40%) | 8/76 (10.5%) | 2/26 (7.69%) | 1/29 (3.4%) | - |
Bleeding complication-no./total no. (%)
| 9/131 (6.87%) 6/131 (4.58%) 2/131 (1.53%) | 6/76 (7.89%) 6/76 (7.89%) 0/76 (0.00%) | 2/26 (7.69%) 0/26 (0.00%) 2/26 (7.69%) | 1/29 (3.4%) 0/29 (0.00%) 1/29 (3.4%) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrara, J.; Theron, A.; Porto, A.; Morera, P.; Luporsi, P.; Jaussaud, N.; Gariboldi, V.; Collart, F.; Cuisset, T.; Deharo, P. Prosthesis–Patient Mismatch in Small Aortic Annuli: Self-Expandable vs. Balloon-Expandable Transcatheter Aortic Valve Replacement. J. Clin. Med. 2022, 11, 1959. https://doi.org/10.3390/jcm11071959
Ferrara J, Theron A, Porto A, Morera P, Luporsi P, Jaussaud N, Gariboldi V, Collart F, Cuisset T, Deharo P. Prosthesis–Patient Mismatch in Small Aortic Annuli: Self-Expandable vs. Balloon-Expandable Transcatheter Aortic Valve Replacement. Journal of Clinical Medicine. 2022; 11(7):1959. https://doi.org/10.3390/jcm11071959
Chicago/Turabian StyleFerrara, Jerome, Alexis Theron, Alizee Porto, Pierre Morera, Paul Luporsi, Nicolas Jaussaud, Vlad Gariboldi, Frederic Collart, Thomas Cuisset, and Pierre Deharo. 2022. "Prosthesis–Patient Mismatch in Small Aortic Annuli: Self-Expandable vs. Balloon-Expandable Transcatheter Aortic Valve Replacement" Journal of Clinical Medicine 11, no. 7: 1959. https://doi.org/10.3390/jcm11071959
APA StyleFerrara, J., Theron, A., Porto, A., Morera, P., Luporsi, P., Jaussaud, N., Gariboldi, V., Collart, F., Cuisset, T., & Deharo, P. (2022). Prosthesis–Patient Mismatch in Small Aortic Annuli: Self-Expandable vs. Balloon-Expandable Transcatheter Aortic Valve Replacement. Journal of Clinical Medicine, 11(7), 1959. https://doi.org/10.3390/jcm11071959