
Seven COVID-19 Patients Treated with C-Reactive Protein (CRP) Apheresis


Abstract
:1. Introduction
2. Materials and Methods
2.1. CACOV Registry
2.2. CRP Apheresis
2.3. Ventilation Scheme
2.4. Contraindications
3. Results
3.1. Patient Characteristics
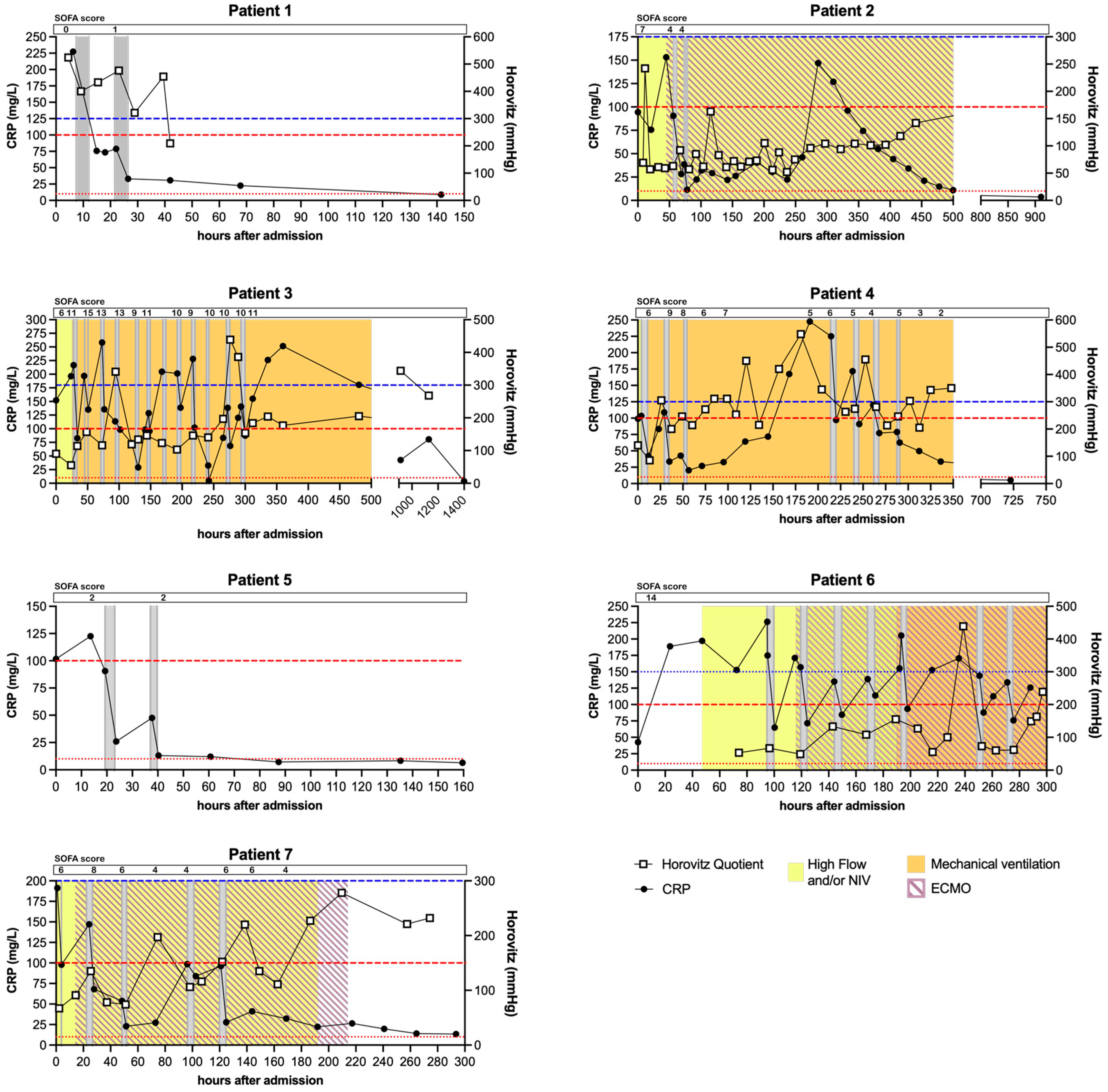
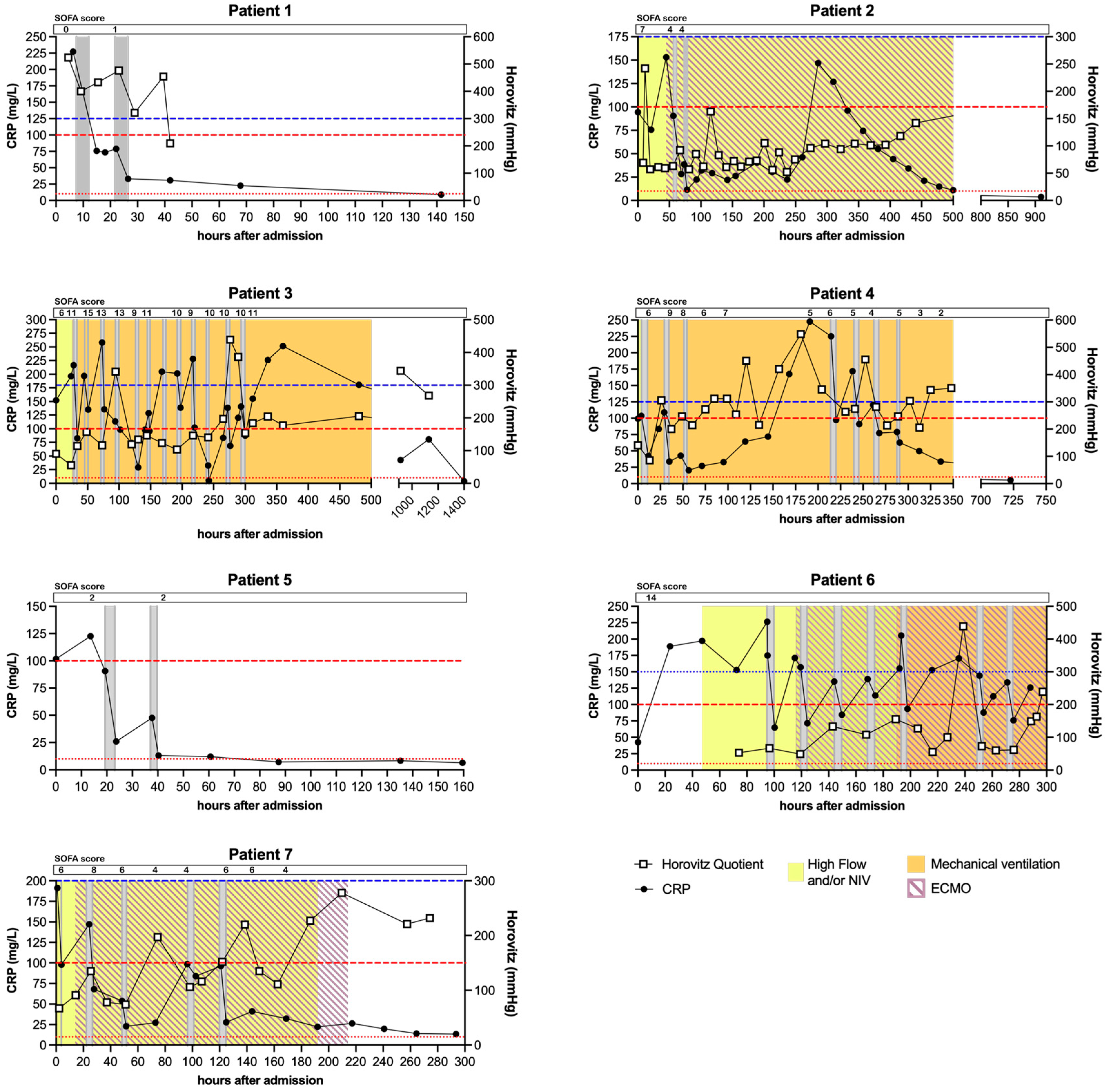
3.2. CRP Kinetics
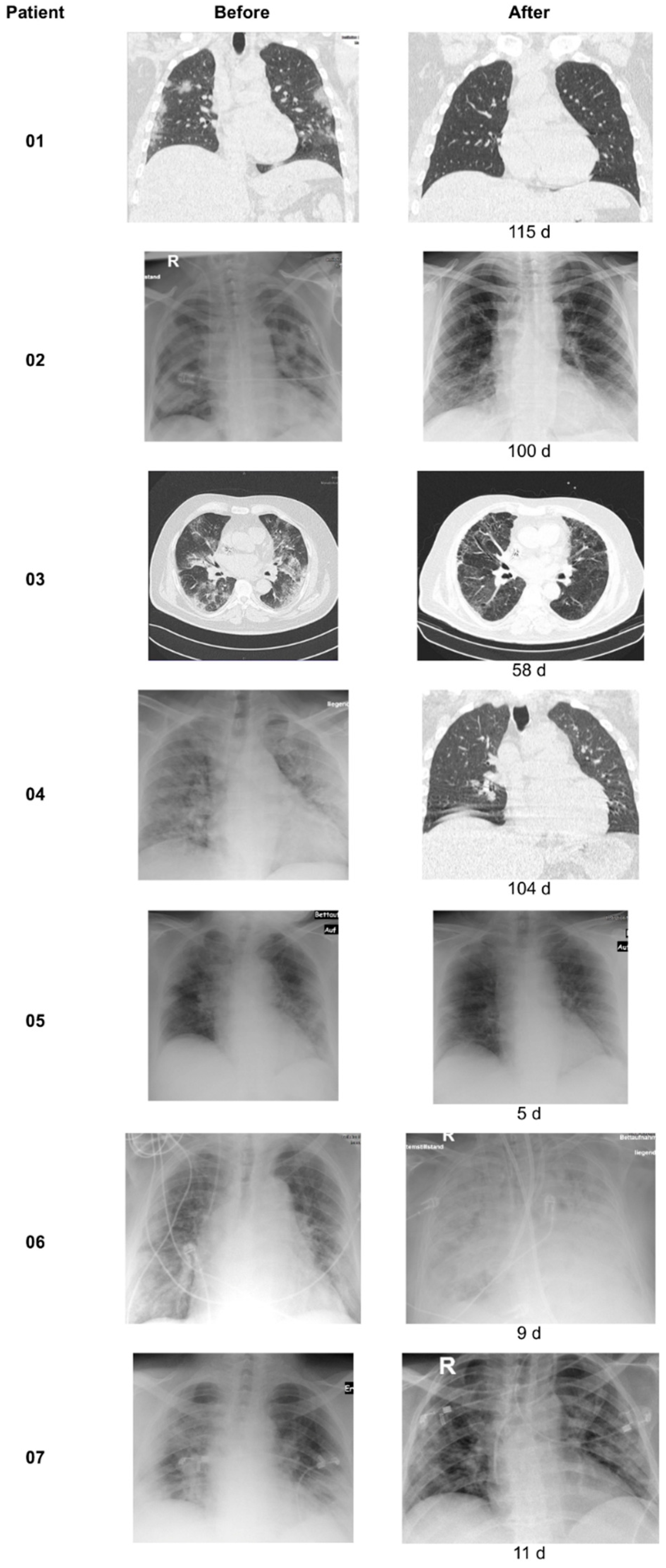
3.3. X-ray/CT Chest Scans
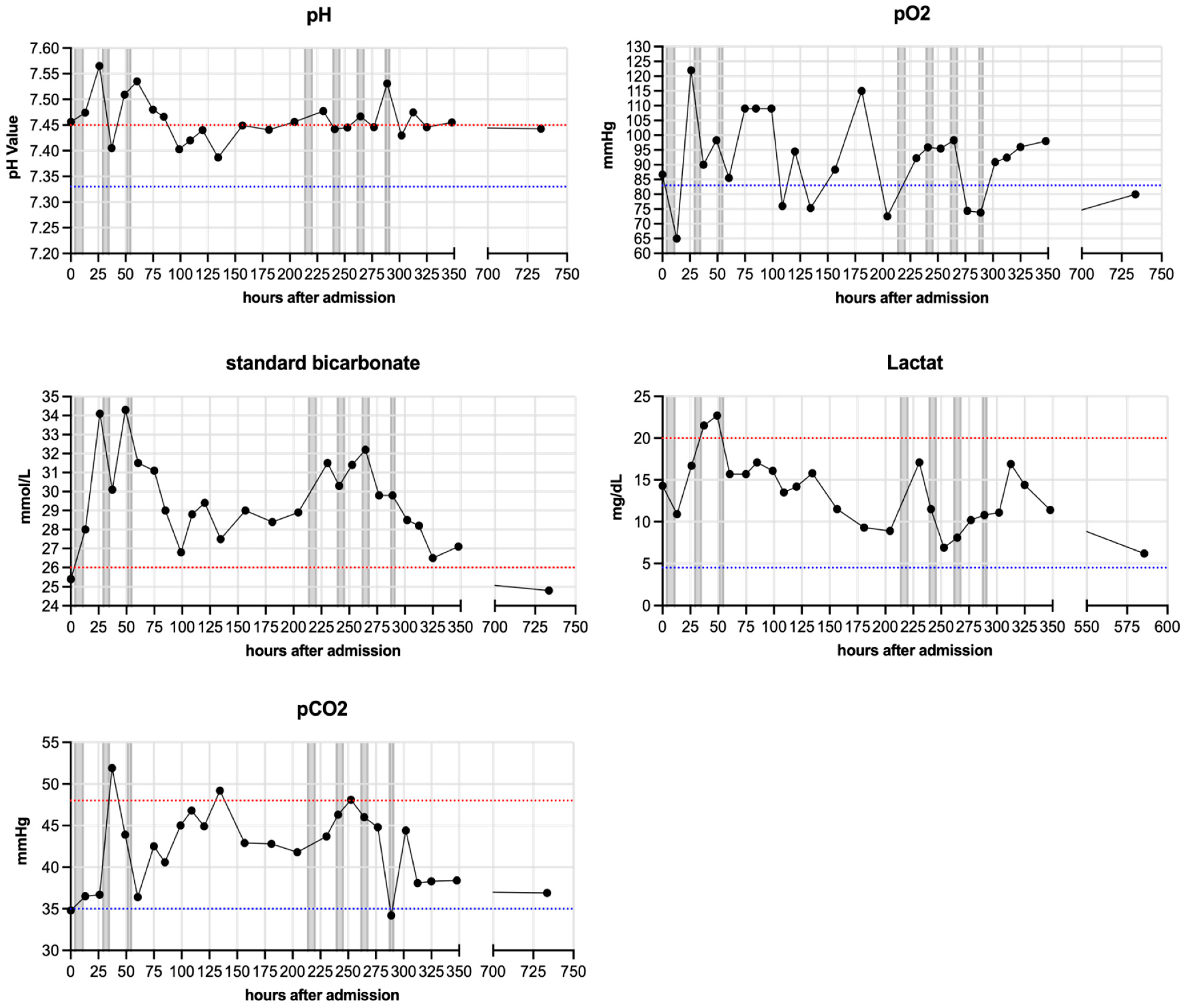
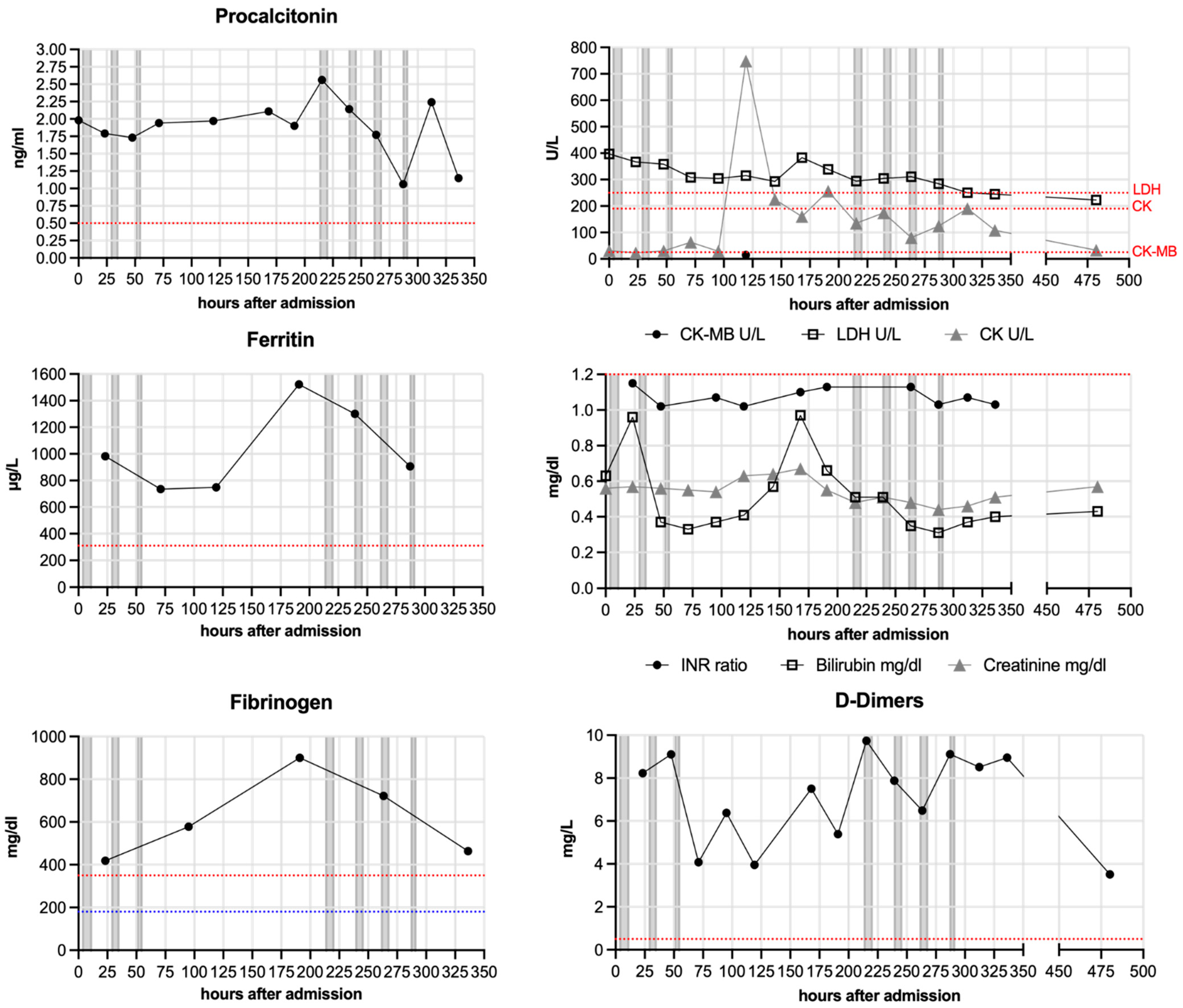
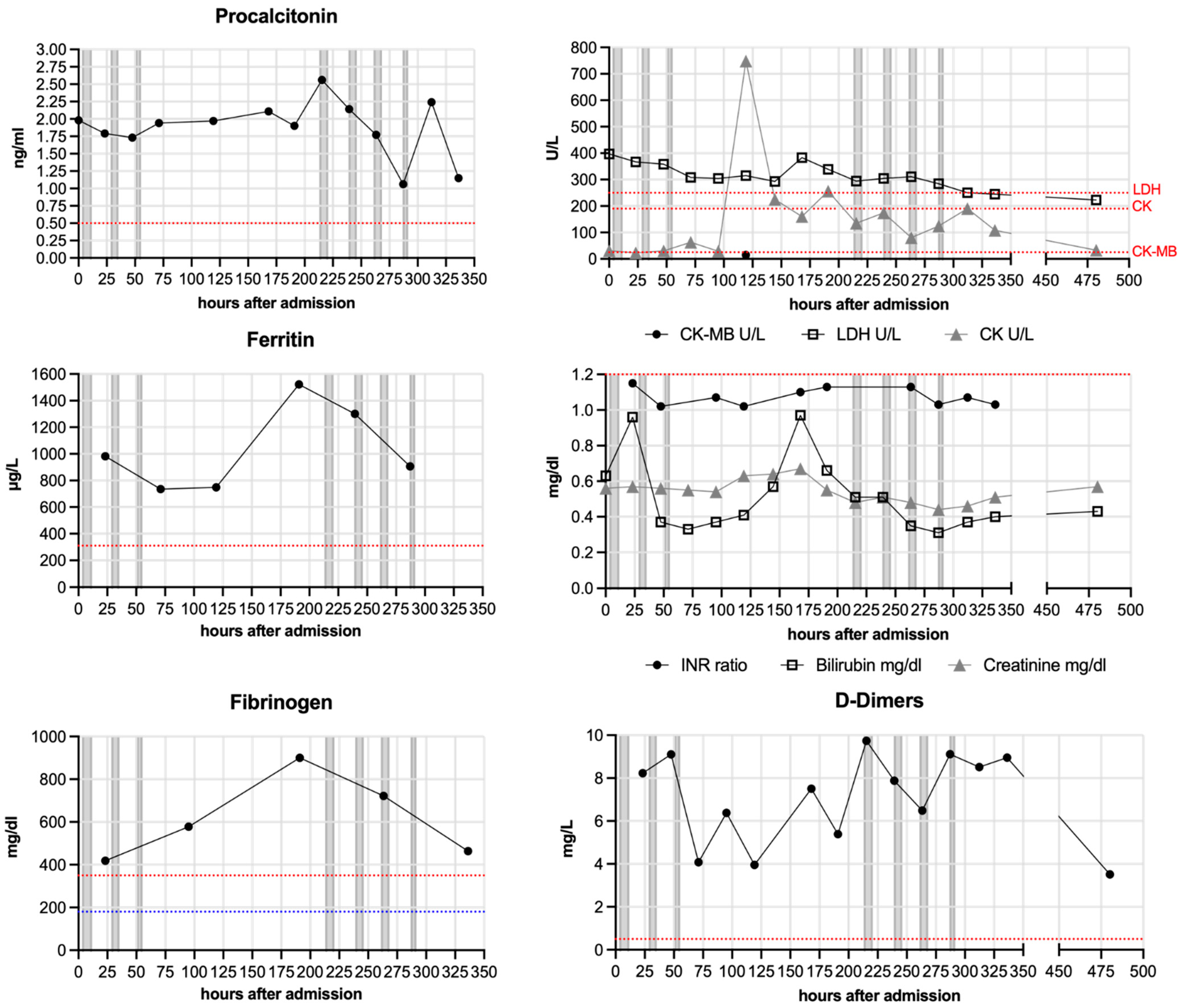
3.4. Respiratory and Laboratory Parameters
3.5. Control Cohort
4. Discussion
4.1. Limitations
4.2. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tillett, W.S.; Francis, T. Serological Reactions in Pneumonia with a Non-Protein Somatic Fraction of Pneumococcus. J. Exp. Med. 1930, 52, 561–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, M.H.; Volanakis, J.E. Interaction of C-reactive protein complexes with the complement system. I. Consumption of human complement associated with the reaction of C-reactive protein with pneumococcal C-polysaccharide and with the choline phosphatides, lecithin and sphingomyelin. J. Immunol. 1974, 112, 2135–2147. [Google Scholar] [PubMed]
- Bharadwaj, D.; Stein, M.P.; Volzer, M.; Mold, C.; Du Clos, T.W. The major receptor for C-reactive protein on leukocytes is fcgamma receptor II. J. Exp. Med. 1999, 190, 585–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manolov, D.E.; Rocker, C.; Hombach, V.; Nienhaus, G.U.; Torzewski, J. Ultrasensitive confocal fluorescence microscopy of C-reactive protein interacting with FcgammaRIIa. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 2372–2377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheriff, A.; Kayser, S.; Brunner, P.; Vogt, B. C-Reactive Protein Triggers Cell Death in Ischemic Cells. Front. Immunol. 2021, 12, 630430. [Google Scholar] [CrossRef]
- Boncler, M.; Wu, Y.; Watala, C. The Multiple Faces of C-Reactive Protein-Physiological and Pathophysiological Implications in Cardiovascular Disease. Molecules 2019, 24, 2062. [Google Scholar] [CrossRef] [Green Version]
- Braig, D.; Nero, T.L.; Koch, H.-G.; Kaiser, B.; Wang, X.; Thiele, J.R.; Morton, C.J.; Zeller, J.; Kiefer, J.; Potempa, L.A.; et al. Transitional changes in the CRP structure lead to the exposure of proinflammatory binding sites. Nat. Commun. 2017, 8, 14188. [Google Scholar] [CrossRef] [Green Version]
- McFadyen, J.D.; Kiefer, J.; Braig, D.; Loseff-Silver, J.; Potempa, L.A.; Eisenhardt, S.U.; Peter, K. Dissociation of C-Reactive Protein Localizes and Amplifies Inflammation: Evidence for a Direct Biological Role of C-Reactive Protein and Its Conformational Changes. Front. Immunol. 2018, 9, 1351. [Google Scholar] [CrossRef] [Green Version]
- Thiele, J.R.; Zeller, J.; Bannasch, H.; Stark, G.B.; Peter, K.; Eisenhardt, S.U. Targeting C-Reactive Protein in Inflammatory Disease by Preventing Conformational Changes. Mediat. Inflamm. 2015, 2015, 372432. [Google Scholar] [CrossRef] [Green Version]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef]
- Mattecka, S.; Brunner, P.; Hähnel, B.; Kunze, R.; Vogt, B.; Sheriff, A. PentraSorb C-Reactive Protein: Characterization of the Selective C-Reactive Protein Adsorber Resin. Ther. Apher. Dial. 2019, 23, 474–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nienhold, R.; Ciani, Y.; Koelzer, V.H.; Tzankov, A.; Haslbauer, J.D.; Menter, T.; Schwab, N.; Henkel, M.; Frank, A.; Zsikla, V.; et al. Two distinct immunopathological profiles in autopsy lungs of COVID-19. Nat. Commun. 2020, 11, 5086. [Google Scholar] [CrossRef] [PubMed]
- Mueller, A.A.; Tamura, T.; Crowley, C.P.; DeGrado, J.R.; Haider, H.; Jezmir, J.L.; Keras, G.; Penn, E.H.; Massaro, A.F.; Kim, E.Y. Inflammatory Biomarker Trends Predict Respiratory Decline in COVID-19 Patients. Cell Rep. Med. 2020, 1, 100144. [Google Scholar] [CrossRef]
- Parimoo, A.; Biswas, A.; Baitha, U.; Gupta, G.; Pandey, S.; Ranjan, P.; Gupta, V.; Barman Roy, D.; Prakash, B.; Wig, N. Dynamics of Inflammatory Markers in Predicting Mortality in COVID-19. Cureus 2021, 13, e19080. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Kunichoff, D.; Garshick, M.; Shah, B.; Pillinger, M.; Hochman, J.S.; Berger, J.S. C-reactive protein and clinical outcomes in patients with COVID-19. Eur. Heart J. 2021, 42, 2270–2279. [Google Scholar] [CrossRef]
- Kayser, S.; Kunze, R.; Sheriff, A. Selective C-reactive protein apheresis for Covid-19 patients suffering from organ damage. Ther. Apher. Dial. 2021, 25, 251–252. [Google Scholar] [CrossRef] [PubMed]
- Pepys, M.B. C-reactive protein predicts outcome in COVID-19: Is it also a therapeutic target? Eur. Heart J. 2021, 42, 2280–2283. [Google Scholar] [CrossRef]
- Sheriff, A.; Schindler, R.; Vogt, B.; Abdel-Aty, H.; Unger, J.K.; Bock, C.; Gebauer, F.; Slagman, A.; Jerichow, T.; Mans, D.; et al. Selective apheresis of C-reactive protein: A new therapeutic option in myocardial infarction? J. Clin. Apher. 2015, 30, 15–21. [Google Scholar] [CrossRef]
- Ries, W.; Sheriff, A.; Heigl, F.; Zimmermann, O.; Garlichs, C.D.; Torzewski, J. “First in Man”: Case Report of Selective C-Reactive Protein Apheresis in a Patient with Acute ST Segment Elevation Myocardial Infarction. Case Rep. Cardiol. 2018, 2018, 4767105. [Google Scholar] [CrossRef]
- Ries, W.; Heigl, F.; Garlichs, C.; Sheriff, A.; Torzewski, J. Selective C-Reactive Protein-Apheresis in Patients. Ther. Apher. Dial. 2019, 23, 570–574. [Google Scholar] [CrossRef]
- Ries, W.; Torzewski, J.; Heigl, F.; Pfluecke, C.; Kelle, S.; Darius, H.; Ince, H.; Mitzner, S.; Nordbeck, P.; Butter, C.; et al. C-Reactive Protein Apheresis as Anti-inflammatory Therapy in Acute Myocardial Infarction: Results of the CAMI-1 Study. Front. Cardiovasc. Med. 2021, 8, 155. [Google Scholar] [CrossRef] [PubMed]
- Torzweski, J.; Heigl, F.; Zimmermann, O.; Wagner, F.; Schumann, C.; Hettich, R.; Bock, C.; Kayser, S.; Sheriff, A. First-in-man: Case report of Selective C-reactive Protein Apheresis in a Patient with SARS-CoV-2 Infection. Am. J. Case Rep. 2020, 21, e925020. [Google Scholar] [CrossRef] [PubMed]
- Ringel, J.; Ramlow, A.; Bock, C.; Sheriff, A. Case Report: C-Reactive Protein Apheresis in a Patient with COVID-19 and Fulminant CRP Increase. Front. Immunol. 2021, 12, 3140. [Google Scholar] [CrossRef] [PubMed]
- Torzewski, J.; Zimmermann, O.; Kayser, S.; Heigl, F.; Wagner, F.; Sheriff, A.; Schumann, C. Successful Treatment of a 39-Year-Old COVID-19 Patient with Respiratory Failure by Selective C-Reactive Protein Apheresis. Am. J. Case Rep. 2021, 22, e932964. [Google Scholar] [CrossRef] [PubMed]
- Schumann, C.; Heigl, F.; Rohrbach, I.J.; Sheriff, A.; Wagner, L.; Wagner, F.; Torzewski, J. A Report on the First 7 Sequential Patients Treated Within the C-Reactive Protein Apheresis in COVID (CACOV) Registry. Am. J. Case Rep. 2022, 23, e935263. [Google Scholar] [CrossRef]
- Herold, T.; Jurinovic, V.; Arnreich, C.; Lipworth, B.J.; Hellmuth, J.C.; von Bergwelt-Baildon, M.; Klein, M.; Weinberger, T. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J. Allergy Clin. Immunol. 2020, 146, 128–136.e124. [Google Scholar] [CrossRef]
- Cappanera, S.; Palumbo, M.; Kwan, S.H.; Priante, G.; Martella, L.A.; Saraca, L.M.; Sicari, F.; Vernelli, C.; Di Giuli, C.; Andreani, P.; et al. When Does the Cytokine Storm Begin in COVID-19 Patients? A Quick Score to Recognize It. J. Clin. Med. 2021, 10, 297. [Google Scholar] [CrossRef]
- Nadeem, R.; Elhoufi, A.M.; Iqbal, N.E.; Obaida, Z.A.; Elgohary, D.M.; Singh, M.K.; Zoraey, S.F.; Abdalla, R.M.; Eltayeb, S.Y.; Danthi, C.S.; et al. Prediction of Cytokine Storm and Mortality in Patients with COVID-19 Admitted to ICU: Do Markers Tell the Story? Dubai Med. J. 2021, 4, 142–150. [Google Scholar] [CrossRef]
- Mosquera-Sulbaran, J.A.; Pedreañez, A.; Carrero, Y.; Callejas, D. C-reactive protein as an effector molecule in Covid-19 pathogenesis. Rev. Med. Virol. 2021, 31, e2221. [Google Scholar] [CrossRef]
- Wu, C.; Wang, G.; Zhang, Q.; Yu, B.; Lv, J.; Zhang, S.; Wu, G.; Wu, S.; Zhong, Y. Association Between Respiratory Alkalosis and the Prognosis of COVID-19 Patients. Front. Med. 2021, 8, 564635. [Google Scholar] [CrossRef]
- Ali, N. Elevated level of C-reactive protein may be an early marker to predict risk for severity of COVID-19. J. Med. Virol. 2020, 92, 2409–2411. [Google Scholar] [CrossRef] [PubMed]
- Sharifpour, M.; Rangaraju, S.; Liu, M.; Alabyad, D.; Nahab, F.B.; Creel-Bulos, C.M.; Jabaley, C.S.; Emory, C.-Q.; Clinical Research, C. C-Reactive protein as a prognostic indicator in hospitalized patients with COVID-19. PLoS ONE 2020, 15, e0242400. [Google Scholar] [CrossRef] [PubMed]
- Villoteau, A.; Asfar, M.; Otekpo, M.; Loison, J.; Gautier, J.; Annweiler, C.; GERIA-COVID Study Group. Elevated C-reactive protein in early COVID-19 predicts worse survival among hospitalized geriatric patients. PLoS ONE 2021, 16, e0256931. [Google Scholar] [CrossRef] [PubMed]
- Günster, C.; Busse, R.; Spoden, M.; Rombey, T.; Schillinger, G.; Hoffmann, W.; Weber-Carstens, S.; Schuppert, A.; Karagiannidis, C. 6-month mortality and readmissions of hospitalized COVID-19 patients: A nationwide cohort study of 8679 patients in Germany. PLoS ONE 2021, 16, e0255427. [Google Scholar] [CrossRef]
- Mainous, A.G., III; Rooks, B.J.; Wu, V.; Orlando, F.A. COVID-19 Post-acute Sequelae Among Adults: 12 Month Mortality Risk. Front. Med. 2021, 8, 778434. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Age | Sex | Hospitalized (Days) | Type of Ventilation (Days) | Treatment | CRP Apheresis (n) | CRP Depletion | Processed Plasma Volume | X-ray Improvement after Apheresis | Survival | Preexisting Diseases | Adipositas | Diabetes (Type) | Cardiovascular | Other | Concurrent Diseases |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 33 | F | 7 | Nasal cannula (3) | Dex, Col, ABs | 2 | 58–67% | 7.5 L | y | y | y | n | y | Factor V Leiden, Factor II Mutation, microcytic anemia | Bacterial s.infection | |
| 2 | 54 | F | 44 | HF and NIV (24) ECMO (19) | ABs | 2 | 69–70% | 7.5–8 L | y (1st) | y | y | Type 2 | y | Bacterial s.infection | ||
| 3 | 69 | M | 75 | HF (3) M ventilation (72) | ABs | 12 | 13–84% | 6.5–10 L | y (6th) | y | y | Type 2 | y | Bacterial s.infection | ||
| 4 | 47 | M | 39 (34 HVL) | HF (1) M ventilation (24) | ABs | 7 | 20–69% | 5–10 L | y (2nd) | y | y | n | y | Bacterial s.infection | ||
| 5 | 72 | F | 9 | Nasal cannula (8) | Dex, Col | 2 | 71–72% | 4–6 L | y (2nd) | y | y | n | n | Alcohol abusement | ||
| 6 | 77 | M | 13 | HF and NIV (7) M Ventilation (5) ECMO (8) | ABs | 7 | 18–71% | 7–9 L | y (5th) Then worse until death | n | n | Type 2 | y | multimorbid | Bacterial s.infection, AKI | |
| 7 | 53 | F | 17 | Nasal cannula (7) HF (10) ECMO (10) | Dex, Col, ABs | 5 | 15–71% | 6–8.5 L | y (5th) | y | n | n | y | Viral hepatitis, Bacterial s.infection | ||
| Mean | 57.9 | 29.1 | 5.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esposito, F.; Matthes, H.; Schad, F. Seven COVID-19 Patients Treated with C-Reactive Protein (CRP) Apheresis. J. Clin. Med. 2022, 11, 1956. https://doi.org/10.3390/jcm11071956
Esposito F, Matthes H, Schad F. Seven COVID-19 Patients Treated with C-Reactive Protein (CRP) Apheresis. Journal of Clinical Medicine. 2022; 11(7):1956. https://doi.org/10.3390/jcm11071956
Chicago/Turabian StyleEsposito, Fabrizio, Harald Matthes, and Friedemann Schad. 2022. "Seven COVID-19 Patients Treated with C-Reactive Protein (CRP) Apheresis" Journal of Clinical Medicine 11, no. 7: 1956. https://doi.org/10.3390/jcm11071956
APA StyleEsposito, F., Matthes, H., & Schad, F. (2022). Seven COVID-19 Patients Treated with C-Reactive Protein (CRP) Apheresis. Journal of Clinical Medicine, 11(7), 1956. https://doi.org/10.3390/jcm11071956