
Delayed Topographical and Refractive Changes Following Corneal Cross-Linking for Keratoconus

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Operative Technique
2.3. Data Collection
2.4. Data Analysis
3. Results
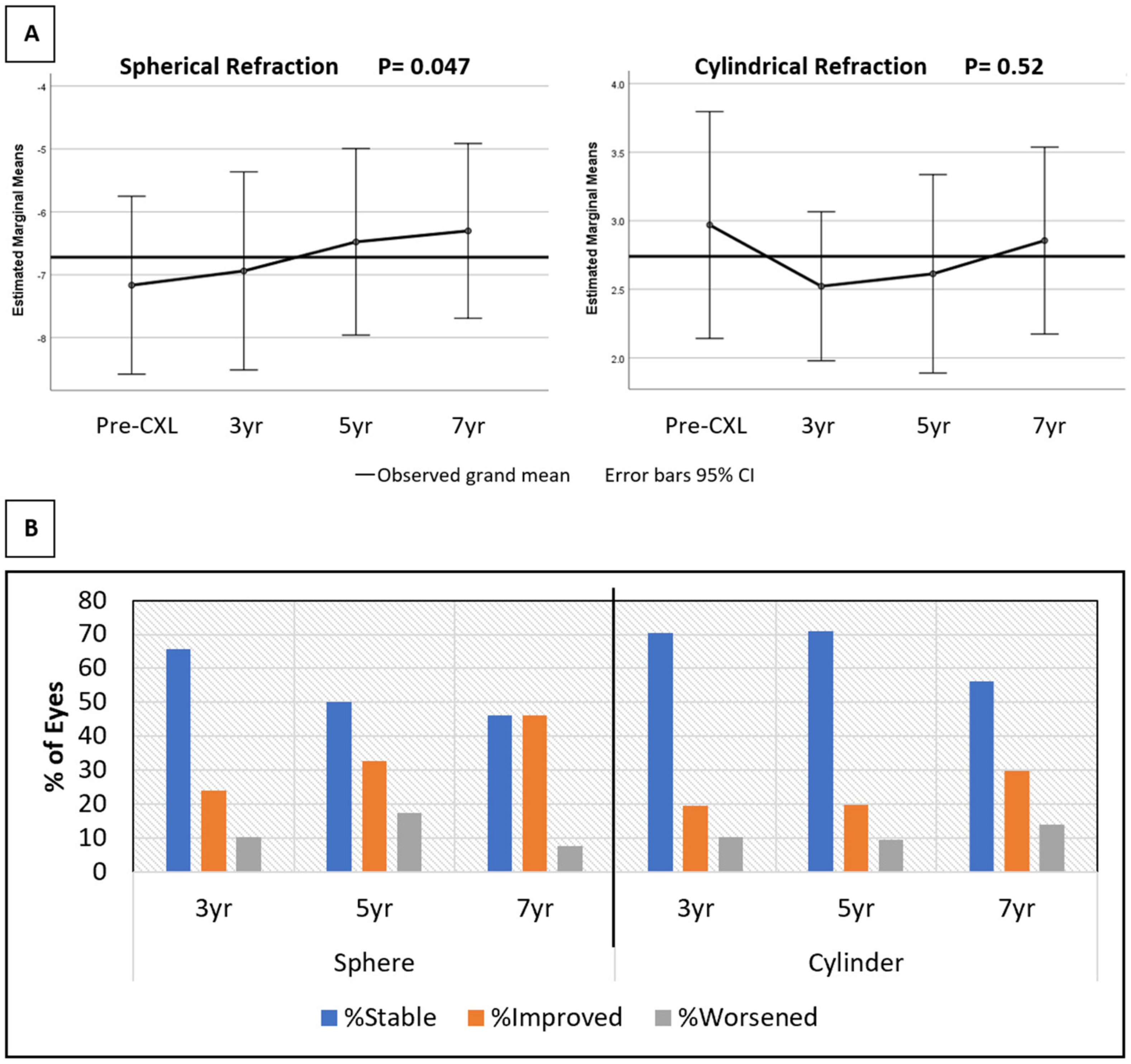
3.1. Refractive Results
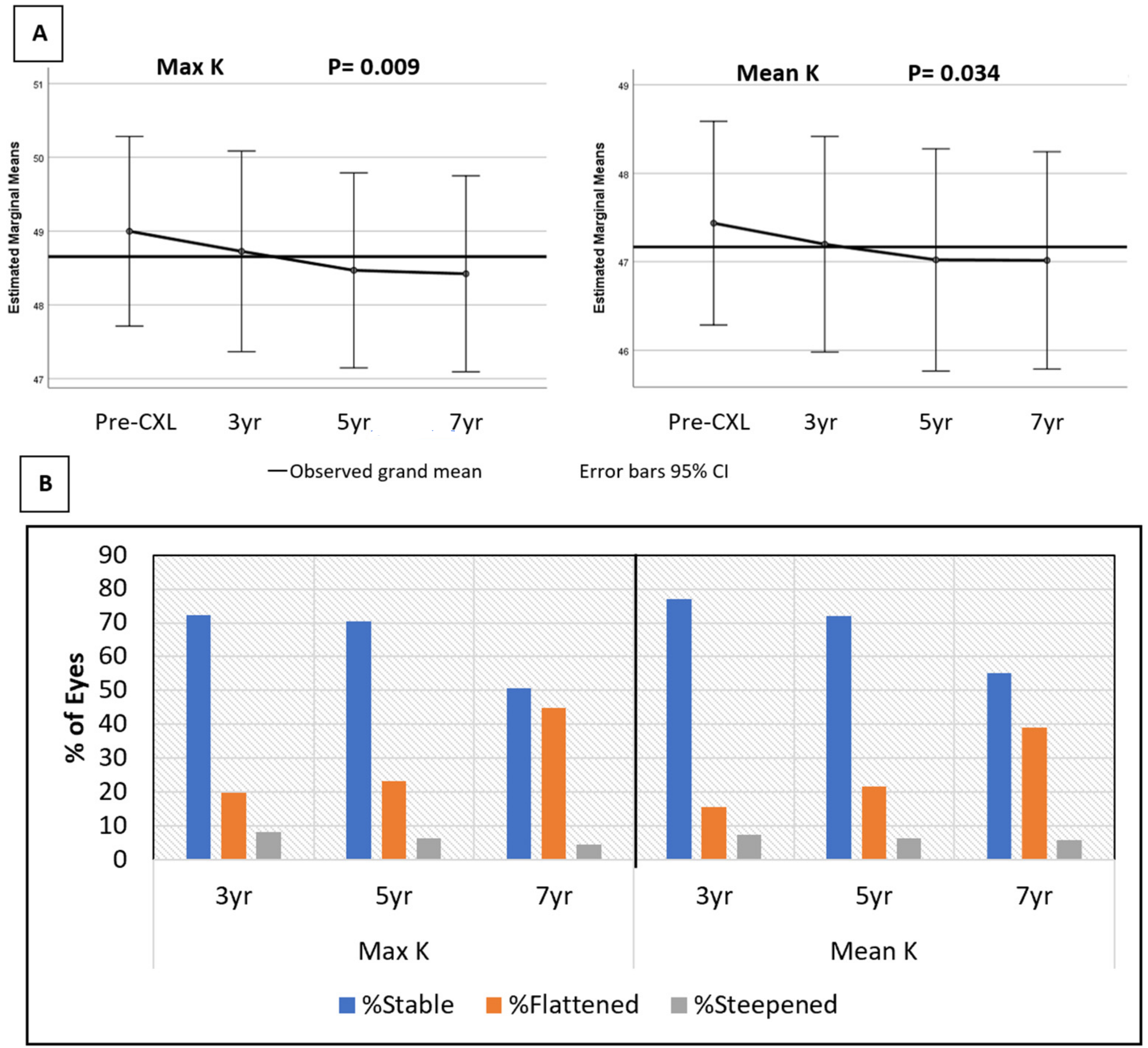
3.2. Topographic Results
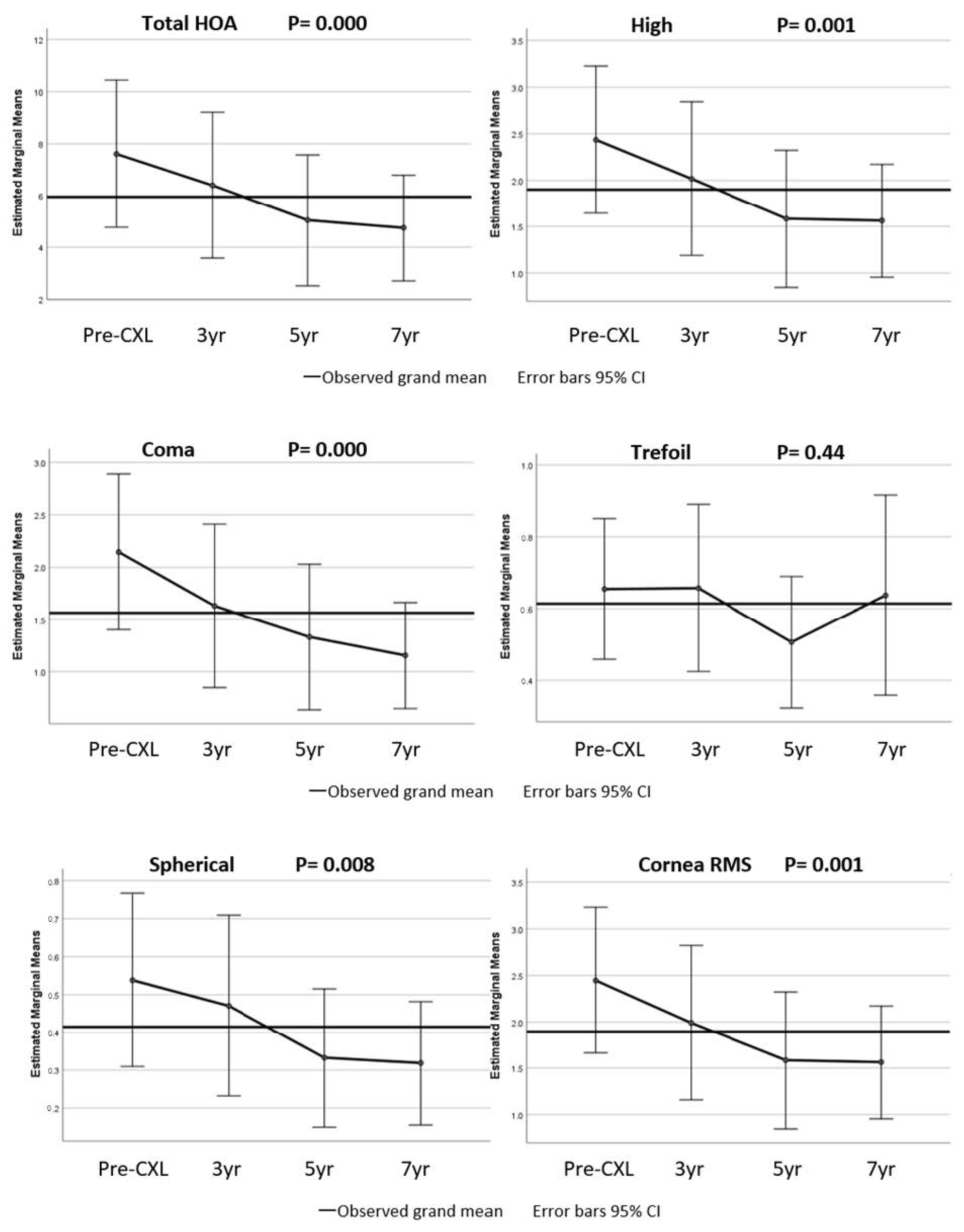
3.3. Corneal Aberrations
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Santodomingo-Rubido, J.; Carracedo, G.; Suzaki, A.; Villa-Collar, C.; Vincent, S.J.; Wolffsohn, J.S. Keratoconus: An updated review. Contact Lens Anterior Eye 2022, 101559. [Google Scholar] [CrossRef] [PubMed]
- Ferdi, A.C.; Nguyen, V.; Gore, D.M.; Allan, B.D.; Rozema, J.; Watson, S.L. Keratoconus Natural Progression. A systematic review of 11,529 eyes. Ophthalmology 2019, 126, 935–945. [Google Scholar] [CrossRef] [PubMed]
- Raiskup-Wolf, F.; Hoyer, A.; Spoerl, E.; Pillunat, L.E. Collagen crosslinking with riboflavin and Ultraviolet-A light in kerato-conus: Long-term results. J. Cataract Refract. Surg. 2008, 34, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Caporossi, A.; Mazzotta, C.; Baiocchi, S.; Caporossi, T. Long-term Results of Riboflavin Ultraviolet A Corneal Collagen Cross-linking for Keratoconus in Italy: The Siena Eye Cross Study. Am. J. Ophthalmol. 2010, 149, 585–593. [Google Scholar] [CrossRef]
- Wollensak, G.; Spoerl, E.; Seiler, T. Riboflavin/ultraviolet-a–induced collagen crosslinking for the treatment of keratoconus. Am. J. Ophthalmol. 2003, 135, 620–627. [Google Scholar] [CrossRef]
- O’Brart, D.P.S.; Kwong, T.Q.; Patel, P.; McDonald, R.J.; O’Brart, N.A. Long-term follow-up of riboflavin/ultraviolet A (370 nm) corneal collagen cross-linking to halt the progression of keratoconus. Br. J. Ophthalmol. 2013, 97, 433–437. [Google Scholar] [CrossRef]
- Kymionis, G.D.; Grentzelos, M.A.; Liakopoulos, D.A.; Paraskevopoulos, T.A.; Klados, N.E.; Tsoulnaras, K.I.; Kankariya, V.P.; Pallikaris, I.G. Long-term Follow-up of Corneal Collagen Cross-linking for Keratoconus—The Cretan Study. Cornea 2014, 33, 1071–1079. [Google Scholar] [CrossRef]
- Hashemi, H.; Seyedian, M.A.; Miraftab, M.; Fotouhi, A.; Asgari, S. Corneal collagen cross-linking with riboflavin and ultraviolet A irradiation for keratoconus: Long-term results. Ophthalmology 2013, 120, 1515. [Google Scholar] [CrossRef]
- Wittig-Silva, C.; Chan, E.; Islam, F.M.A.; Wu, T.; Whiting, M.; Snibson, G.R. A randomized, controlled trial of corneal collagen cross-linking in progressive keratoconus: Three-year results. Ophthalmology 2014, 121, 812. [Google Scholar] [CrossRef]
- Raiskup, F.; Theuring, A.; Pillunat, L.E.; Spoerl, E. Corneal collagen crosslinking with riboflavin and ultraviolet-A light in progressive keratoconus: Ten-year results. J. Cataract. Refract. Surg. 2015, 41, 41–46. [Google Scholar] [CrossRef]
- Mazzotta, C.; Traversi, C.; Baiocchi, S.; Bagaglia, S.; Caporossi, O.; Villano, A.; Caporossi, A. Corneal Collagen Cross-Linking with Riboflavin and Ultraviolet A Light for Pediatric Keratoconus: Ten-Year Results. Cornea 2018, 37, 560–566. [Google Scholar] [CrossRef]
- Raiskup-Wolf, F.; Spoerl, E. Corneal Crosslinking with Riboflavin and Ultraviolet A. Part II. Clinical Indications and Results. Ocul. Surf. 2013, 11, 93–108. [Google Scholar] [CrossRef]
- De Bernardo, M.; Capasso, L.; Lanza, M.; Tortori, A.; Iaccarino, S.; Cennamo, M.; Borrelli, M.; Rosa, N. Long-term results of corneal collagen crosslinking for progressive kerato-conus. J. Optom. 2015, 8, 180–186. [Google Scholar] [CrossRef]
- Koller, T.; Mrochen, M.; Seiler, T. Complication and failure rates after corneal crosslinking. J. Cataract Refract. Surg. 2009, 35, 1358–1362. [Google Scholar] [CrossRef]
- Lim, W.K.; Da Soh, Z.; Choi, H.K.Y.; Theng, J.T.S. Epithelium-on photorefractive intrastromal cross-linking (Pi, XL) for reduction of low myopia. Clin. Ophthalmol. 2017, 11, 1205–1211. [Google Scholar] [CrossRef]
- Fredriksson, A.; Näslund, S.; Behndig, A. A prospective evaluation of photorefractive intrastromal cross-linking for the treatment of low-grade myopia. Acta Ophthalmol. 2020, 98, 201–206. [Google Scholar] [CrossRef]
- Kanellopoulous, A.J. Novel myopic refractive correction with transepithelial very high-fluence collagen cross-linking applied in a customized pattern: Early clinical results of a feasibility study. Clin. Ophthalmol. 2014, 8, 697–702. [Google Scholar] [CrossRef]
- Vinciguerra, P.; Albè, E.; Trazza, S.; Rosetta, P.; Vinciguerra, R.; Seiler, T.; Epstein, D. Refractive, topographic, tomographic, and aberrometric analysis of keratoconic eyes undergoing corneal cross-linking. Ophthalmology 2009, 116, 369–378. [Google Scholar] [CrossRef]
- Elmassry, A.; Dowidar, A.M.; Massoud, T.H.; Tadros, B.G.D. Evaluation of the effect of corneal collagen cross-linking for keratoconus on the ocular higher-order aberrations. Clin. Ophthalmol. 2017, 11, 1461–1469. [Google Scholar] [CrossRef]
- Greenstein, S.A.; Fry, K.L.; Hersh, M.J.; Hersh, P.S. Higher-order aberrations after corneal collagen crosslinking for keratoconus and corneal ectasia. J. Cataract. Refract. Surg. 2012, 38, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Naderan, M.; Jahanrad, A. Higher-order aberration 4 years after corneal collagen cross-linking. Indian J. Ophthalmol. 2017, 65, 808–812. [Google Scholar] [CrossRef]
- Ghanem, R.C.; Santhiago, M.R.; Berti, T.; Netto, M.V.; Ghanem, V.C. Topographic, corneal wavefront, and refractive outcomes 2 years after collagen crosslinking for progressive keratoconus. Cornea 2014, 33, 43–48. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Pre-CXL n: 150 | 3 yrs n: 122 | 5 yrs n: 125 | 7 yrs n: 69 | Last Available n: 150 | p Value * | |
| CDVA (LogMar) | 0.268 ± 0.172 | 0.210 ± 0.139 | 0.215 ± 0.149 | 0.242 ± 0.145 | 0.228 ± 0.160 | 0.020 |
| Sphere Power (D) | −6.72 ± 4.12 | −6.22 ± 4.11 | −6.28 ± 4.07 | −5.80 ± 4.30 | −6.17 ± 4.26 | <0.001 |
| Cylinder Power (D) | 3.42 ± 2.23 | 3.04 ± 2.15 | 3.01 ± 1.95 | 2.99 ± 2.11 | 2.98 ± 1.84 | <0.001 |
| Mean-K (D) | 46.68 ± 2.92 | 46.34 ± 2.93 | 46.36 ± 3.07 | 45.96 ± 3.38 | 46.10 ± 3.04 | <0.001 |
| Max-K (D) | 48.35 ± 3.40 | 47.85 ± 3.43 | 47.89 ± 3.37 | 47.44 ± 3.68 | 47.64 ± 3.41 | <0.001 |
| Pre-CXL n: 82 | 3 yrs n: 108 | 5 yrs n: 112 | 7 yrs n: 69 | Last Available n: 150 | p Value * | |
| Total Corneal Aberrations | 7.85 ± 6.21 | 8.16 ± 7.07 | 7.06 ± 5.52 | 5.29 ± 4.17 | 5.92 ± 4.58 | <0.001 |
| High | 2.38 ± 1.74 | 2.43 ± 1.98 | 2.15 ± 1.54 | 1.71 ± 1.25 | 1.88 ± 1.40 | <0.001 |
| Coma | 2.04 ± 1.65 | 2.09 ± 1.89 | 1.79 ± 1.45 | 1.40 ± 1.16 | 1.52 ± 1.33 | <0.001 |
| Trefoil | 0.81 ± 0.56 | 0.76 ± 0.57 | 0.76 ± 0.52 | 0.61 ± 0.43 | 0.72 ± 0.51 | 0.057 |
| Spherical | 0.45 ± 0.47 | 0.49 ± 0.58 | 0.42 ± 0.51 | 0.35 ± 0.41 | 0.33 ±0.35 | 0.003 |
| Cornea RMS | 2.39 ± 1.74 | 2.43 ± 1.98 | 2.15 ± 1.54 | 1.73 ± 1.24 | 1.88 ± 1.40 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eslami, M.; Ghaseminejad, F.; Dubord, P.J.; Yeung, S.N.; Iovieno, A. Delayed Topographical and Refractive Changes Following Corneal Cross-Linking for Keratoconus. J. Clin. Med. 2022, 11, 1950. https://doi.org/10.3390/jcm11071950
Eslami M, Ghaseminejad F, Dubord PJ, Yeung SN, Iovieno A. Delayed Topographical and Refractive Changes Following Corneal Cross-Linking for Keratoconus. Journal of Clinical Medicine. 2022; 11(7):1950. https://doi.org/10.3390/jcm11071950
Chicago/Turabian StyleEslami, Maryam, Farhad Ghaseminejad, Paul J. Dubord, Sonia N. Yeung, and Alfonso Iovieno. 2022. "Delayed Topographical and Refractive Changes Following Corneal Cross-Linking for Keratoconus" Journal of Clinical Medicine 11, no. 7: 1950. https://doi.org/10.3390/jcm11071950
APA StyleEslami, M., Ghaseminejad, F., Dubord, P. J., Yeung, S. N., & Iovieno, A. (2022). Delayed Topographical and Refractive Changes Following Corneal Cross-Linking for Keratoconus. Journal of Clinical Medicine, 11(7), 1950. https://doi.org/10.3390/jcm11071950