
Efficacy and Safety of Laparoscopy for Mild and Moderate Pediatric Abdominal Trauma: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
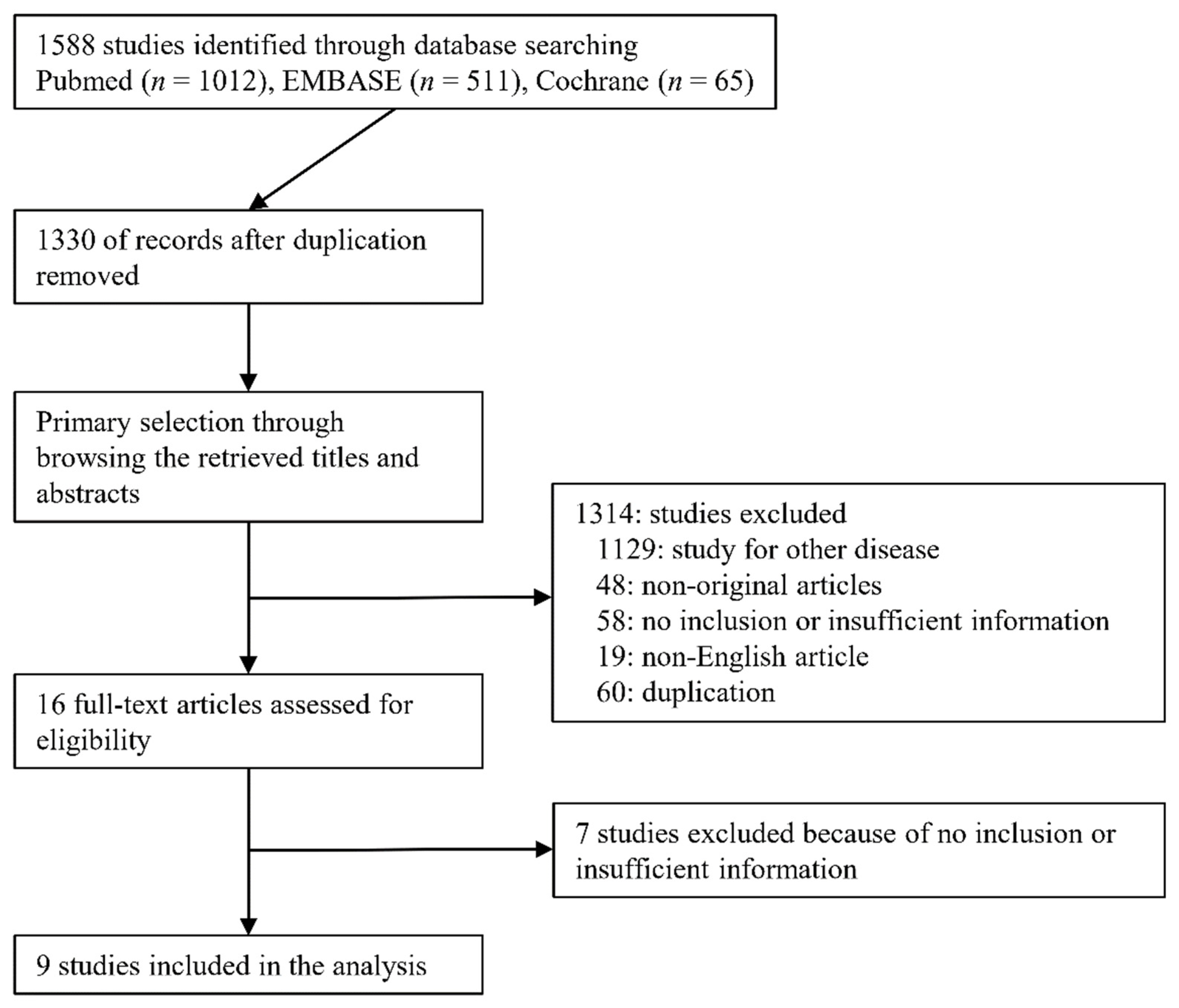
2.1. Published Study Search and Selection Criteria
2.2. Data Extraction
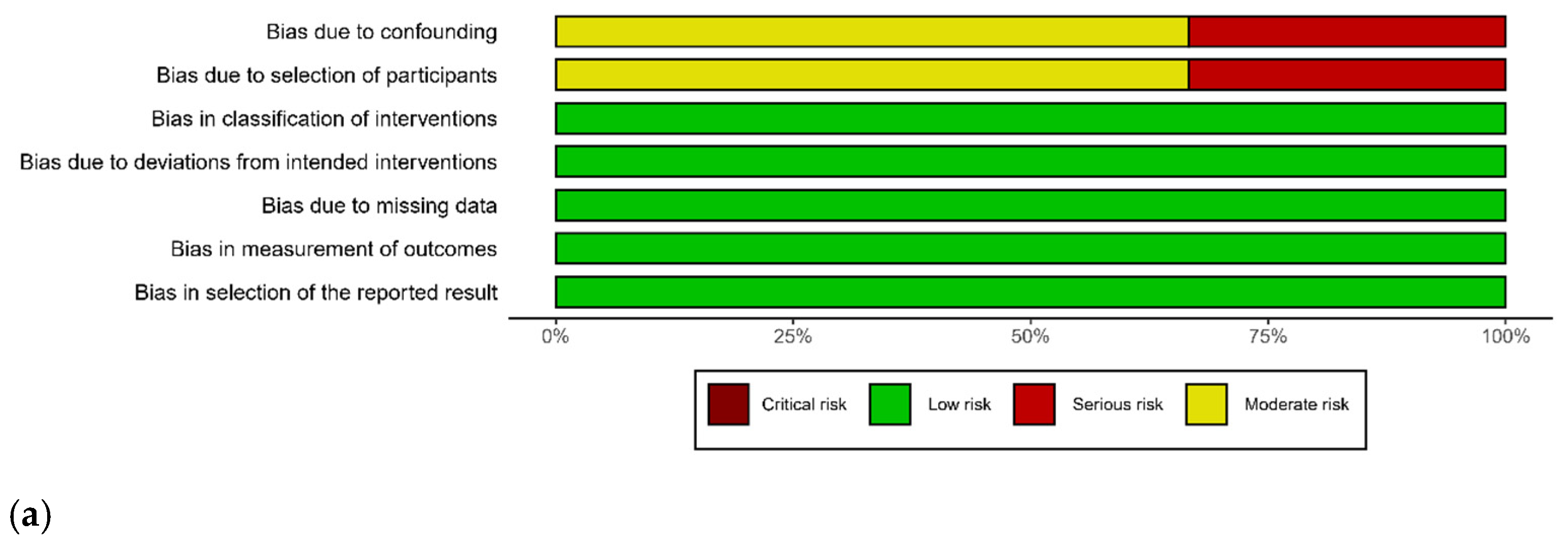
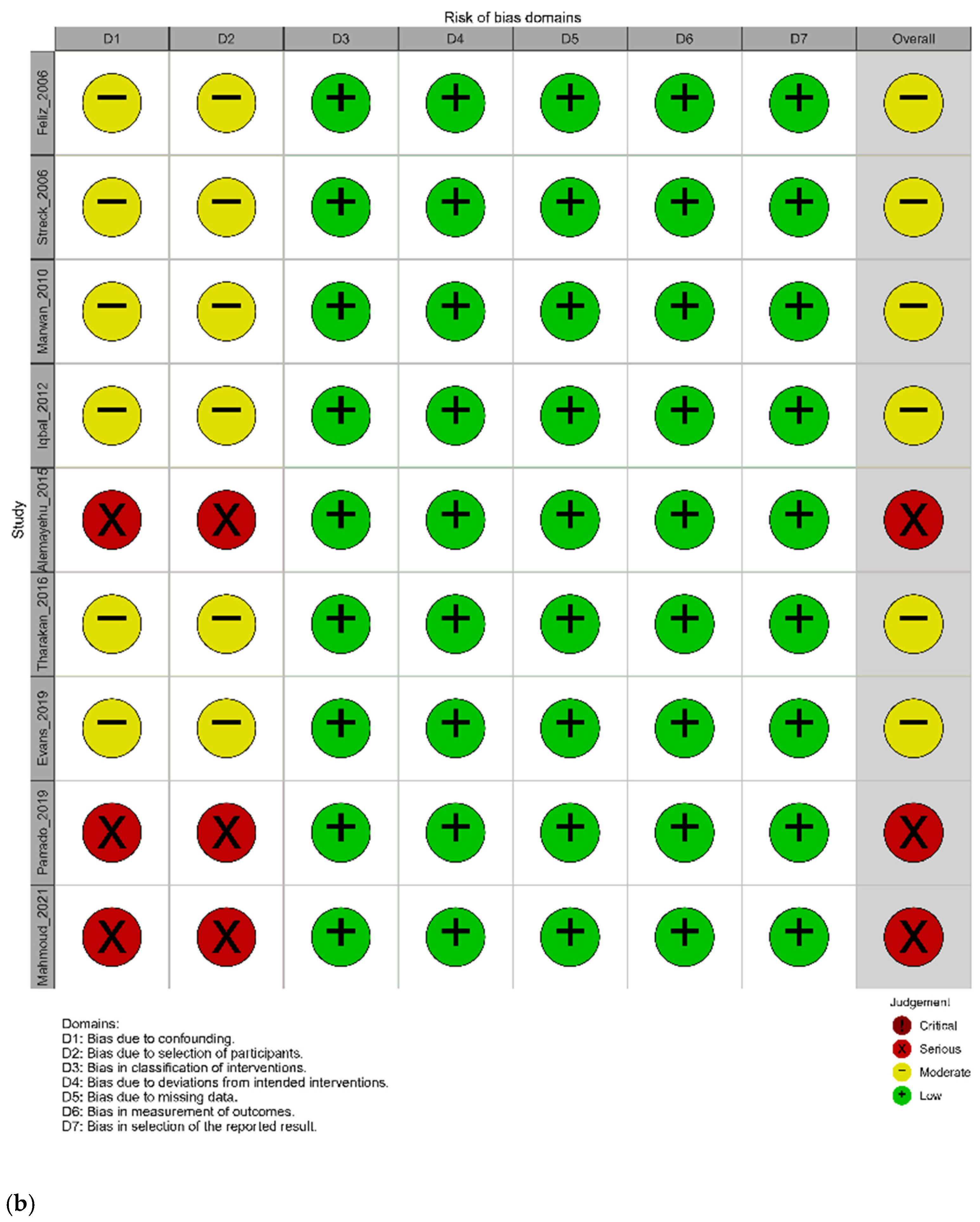
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
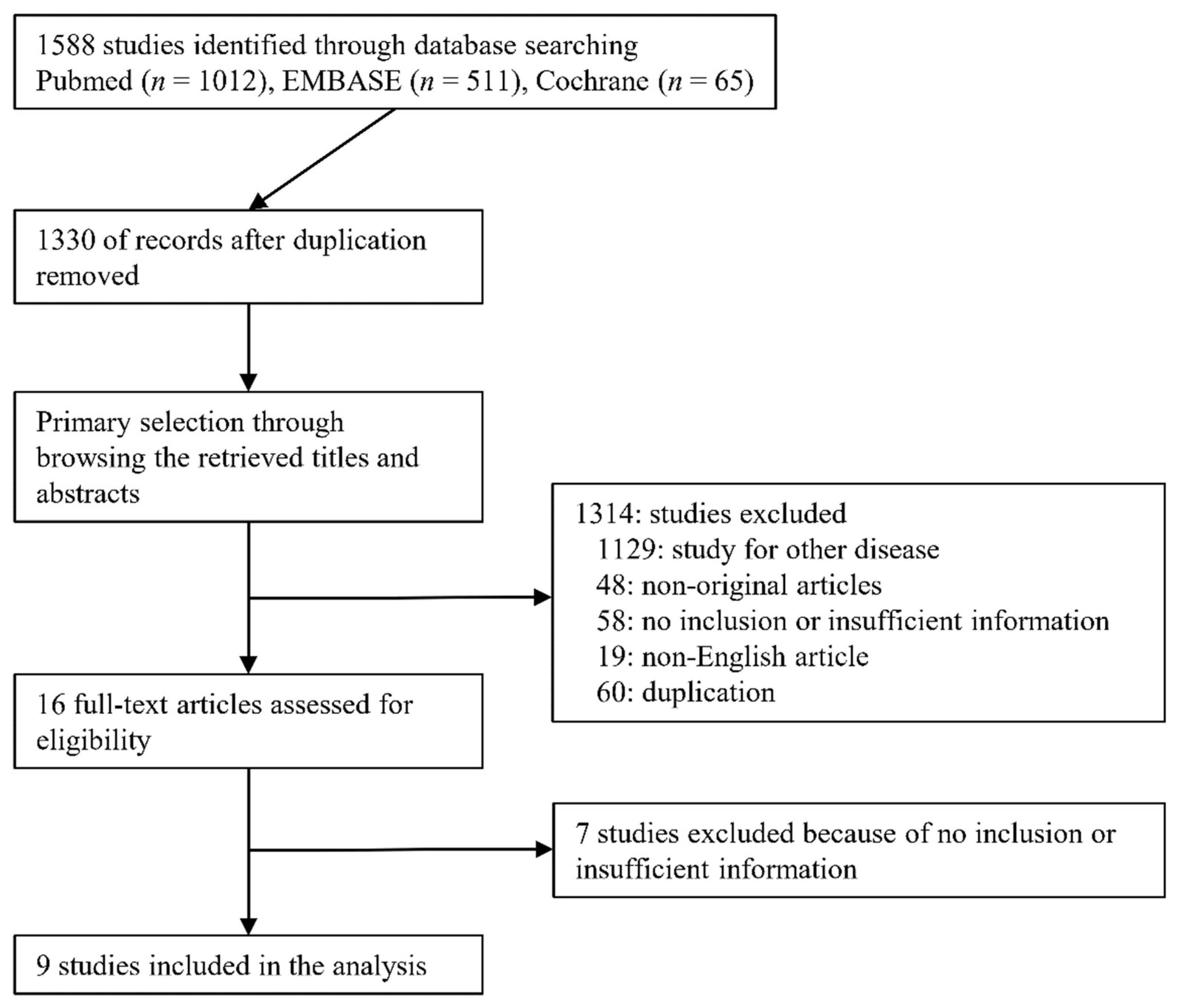
3.1. Selection and Characteristics
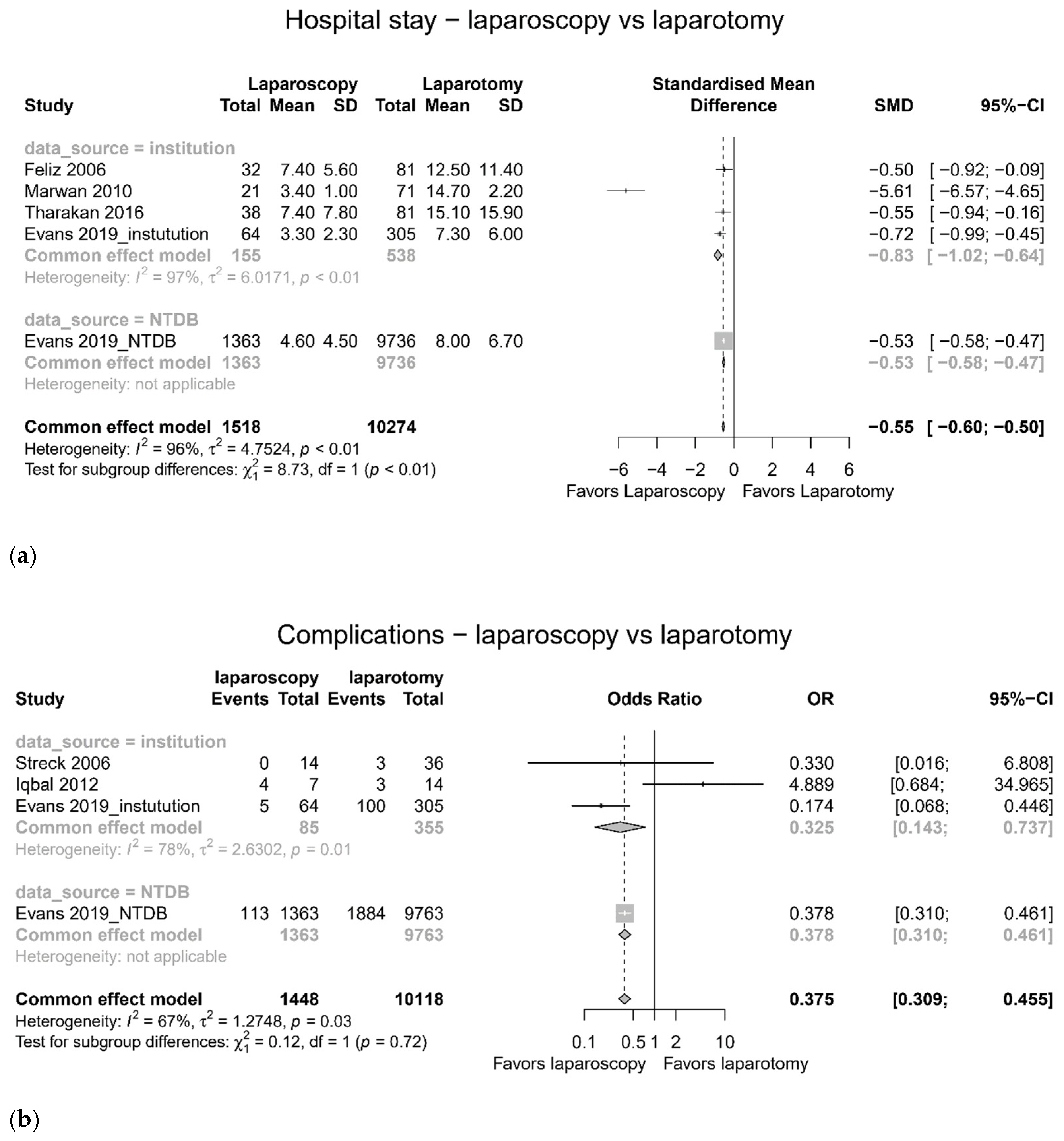
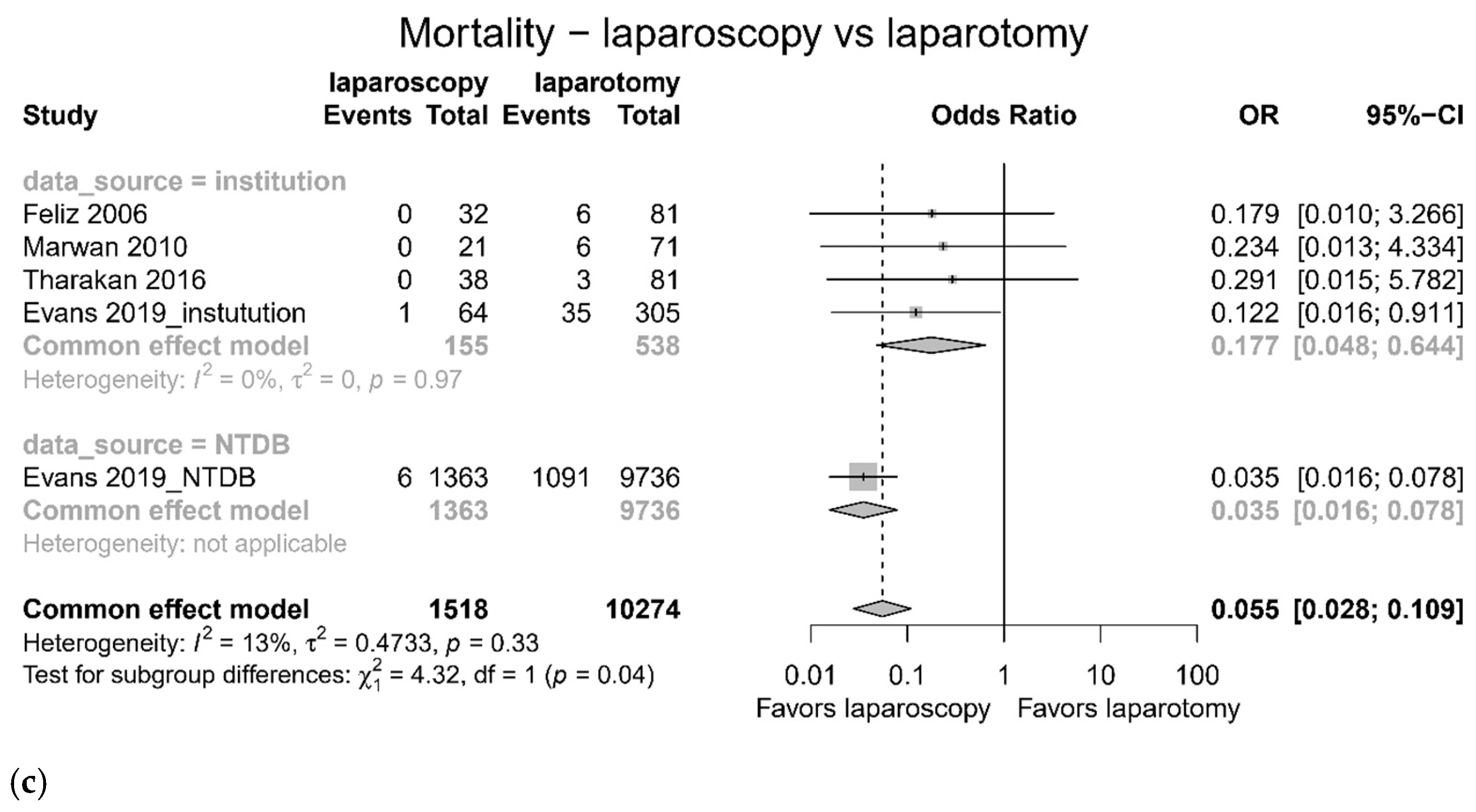
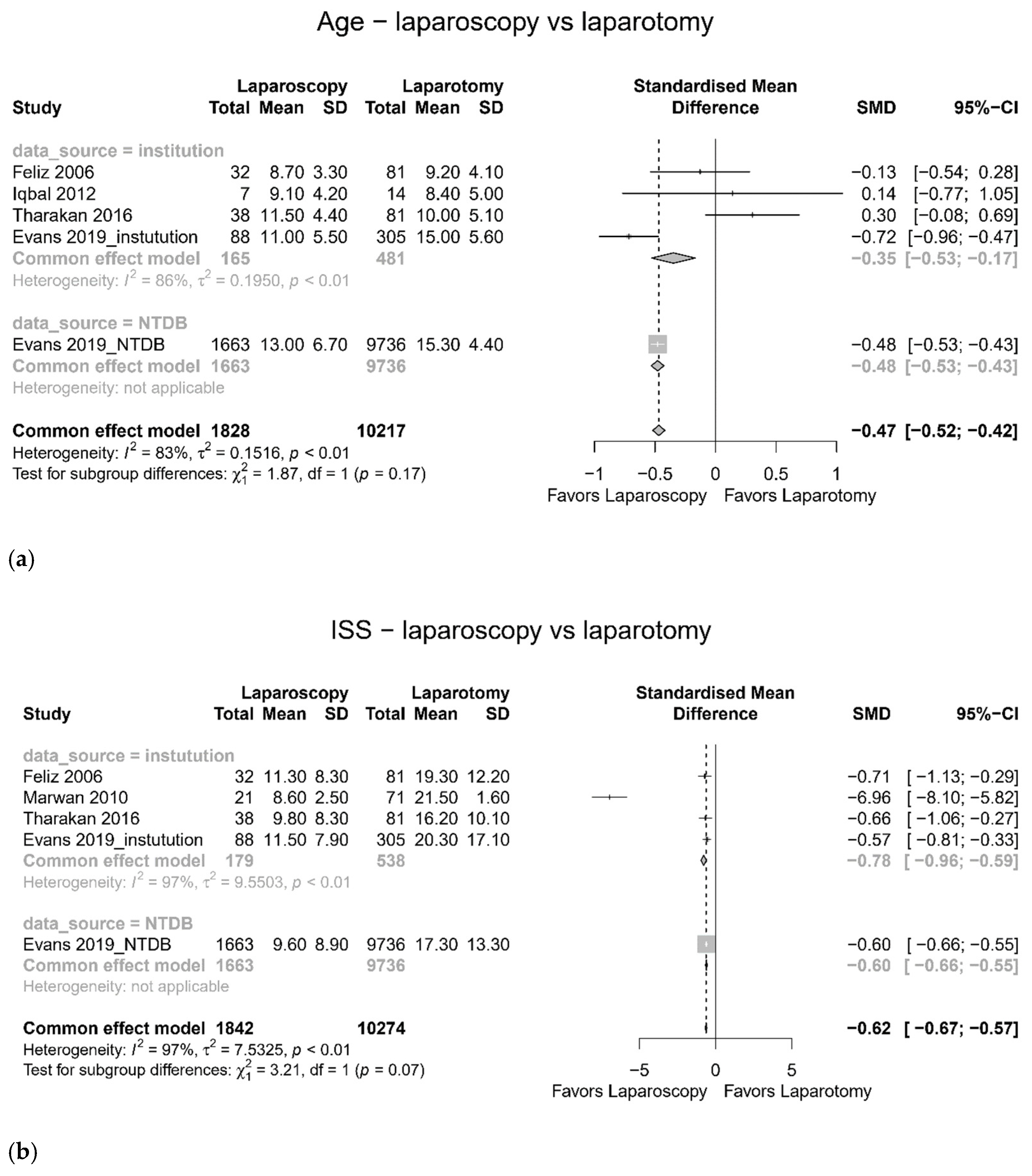
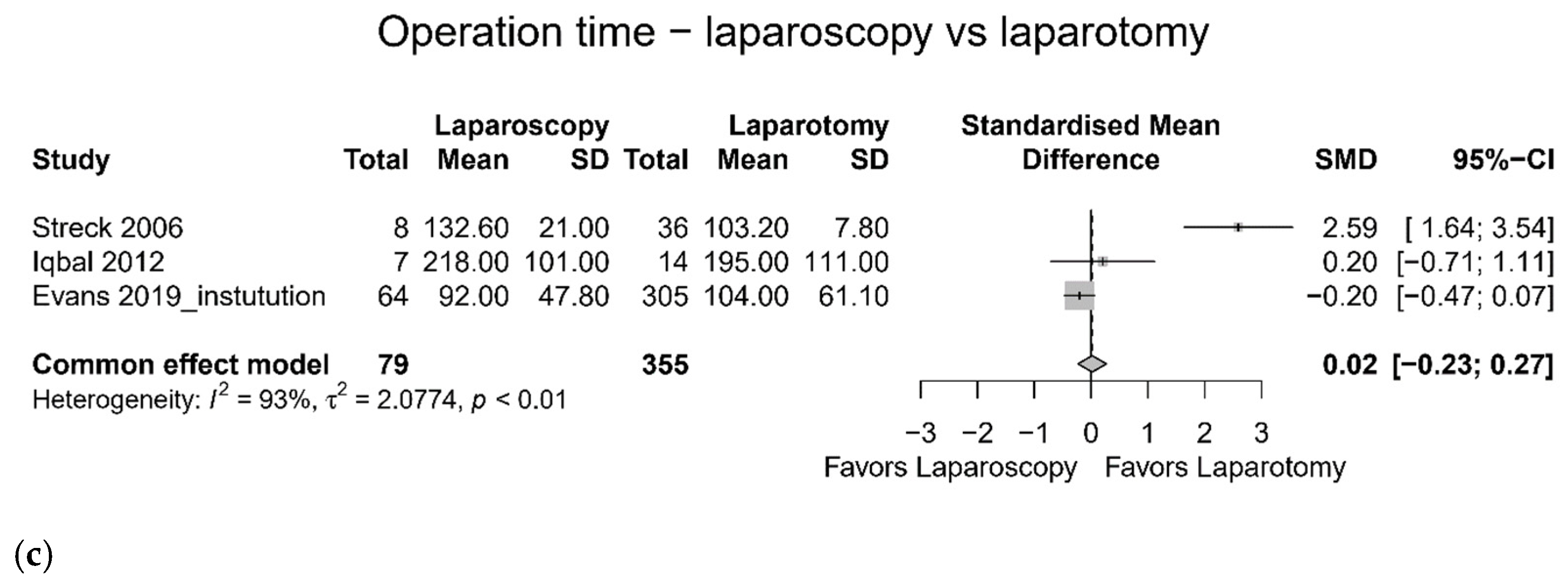
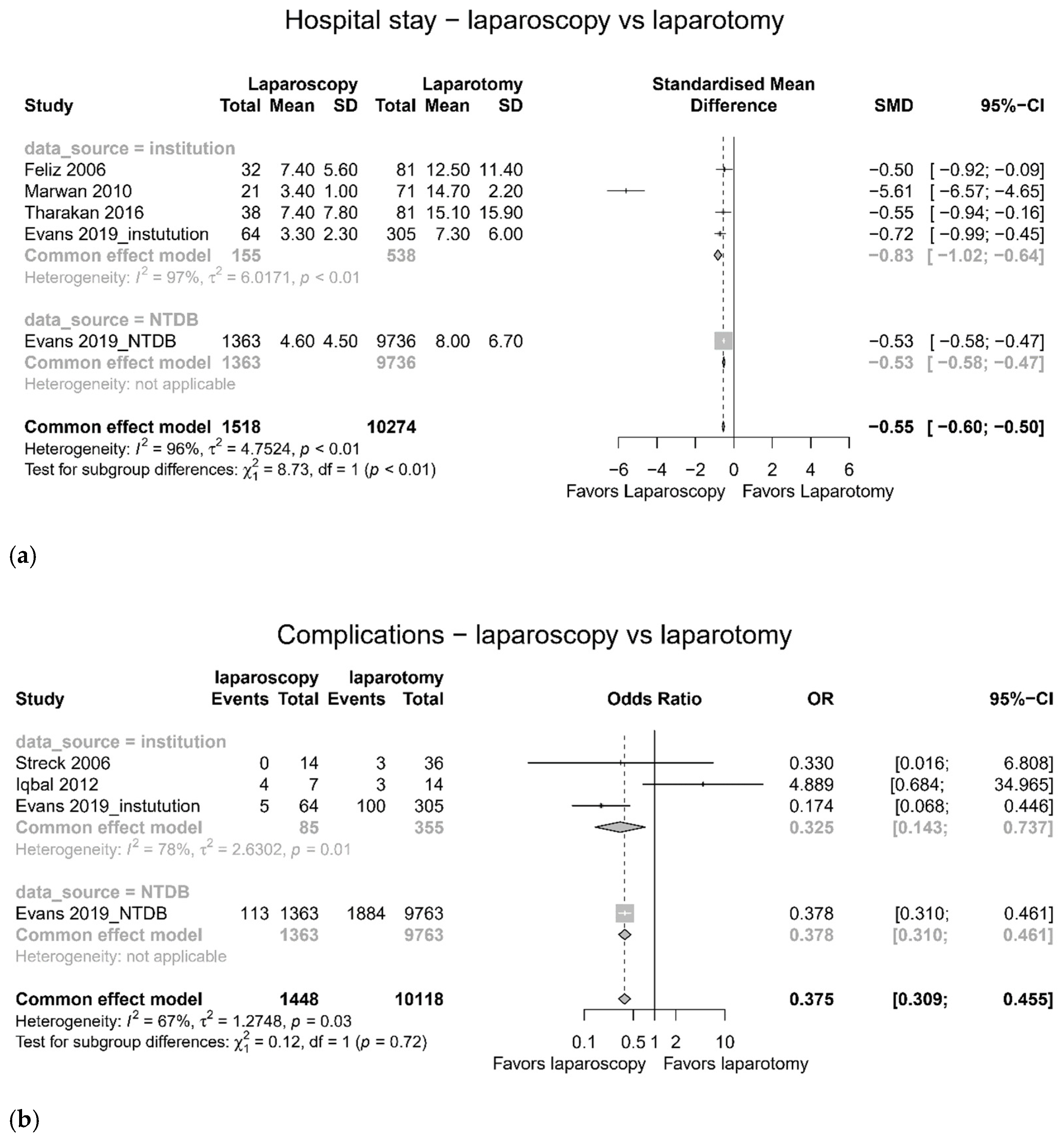
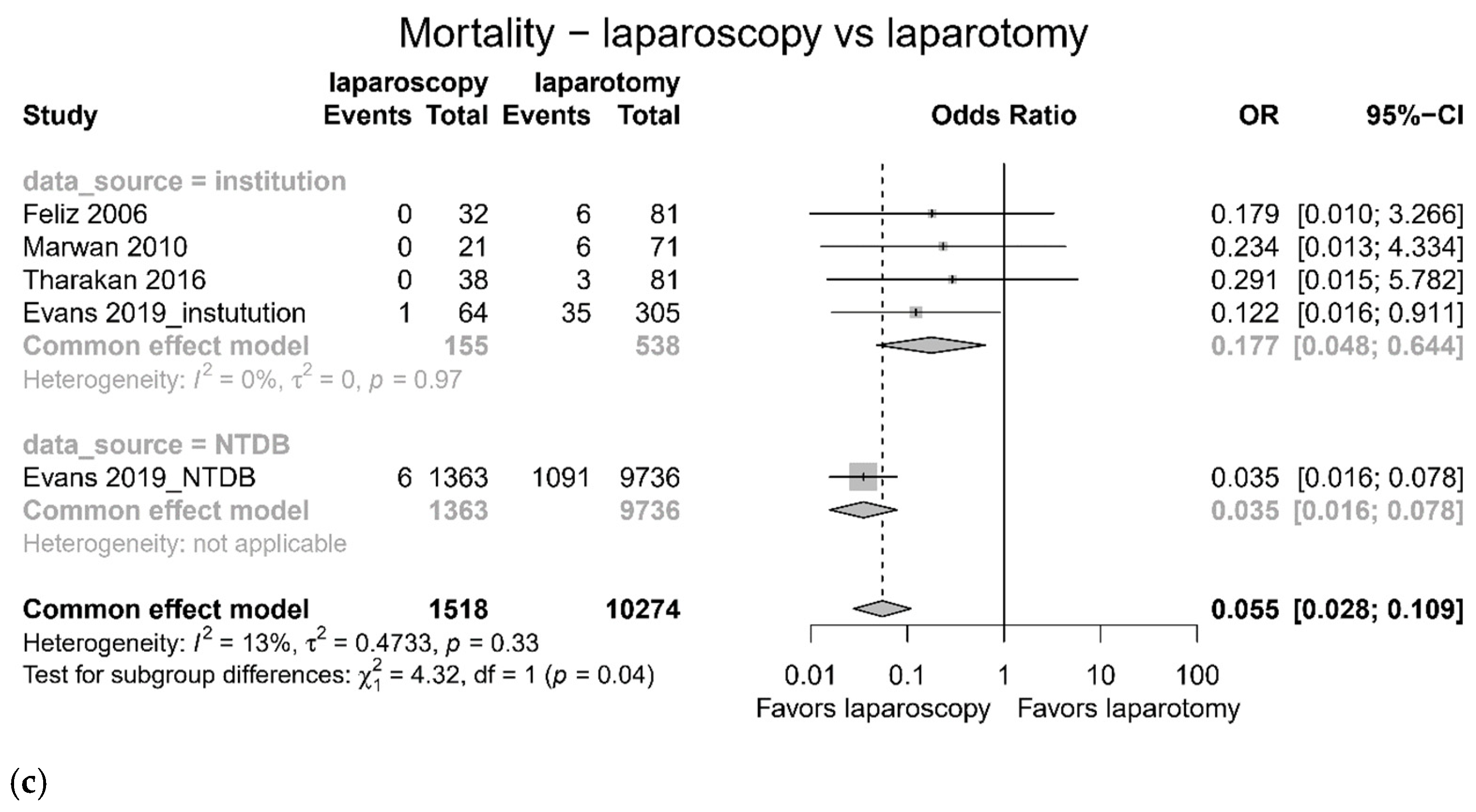
3.2. Comparison between Laparoscopy and Laparotomy
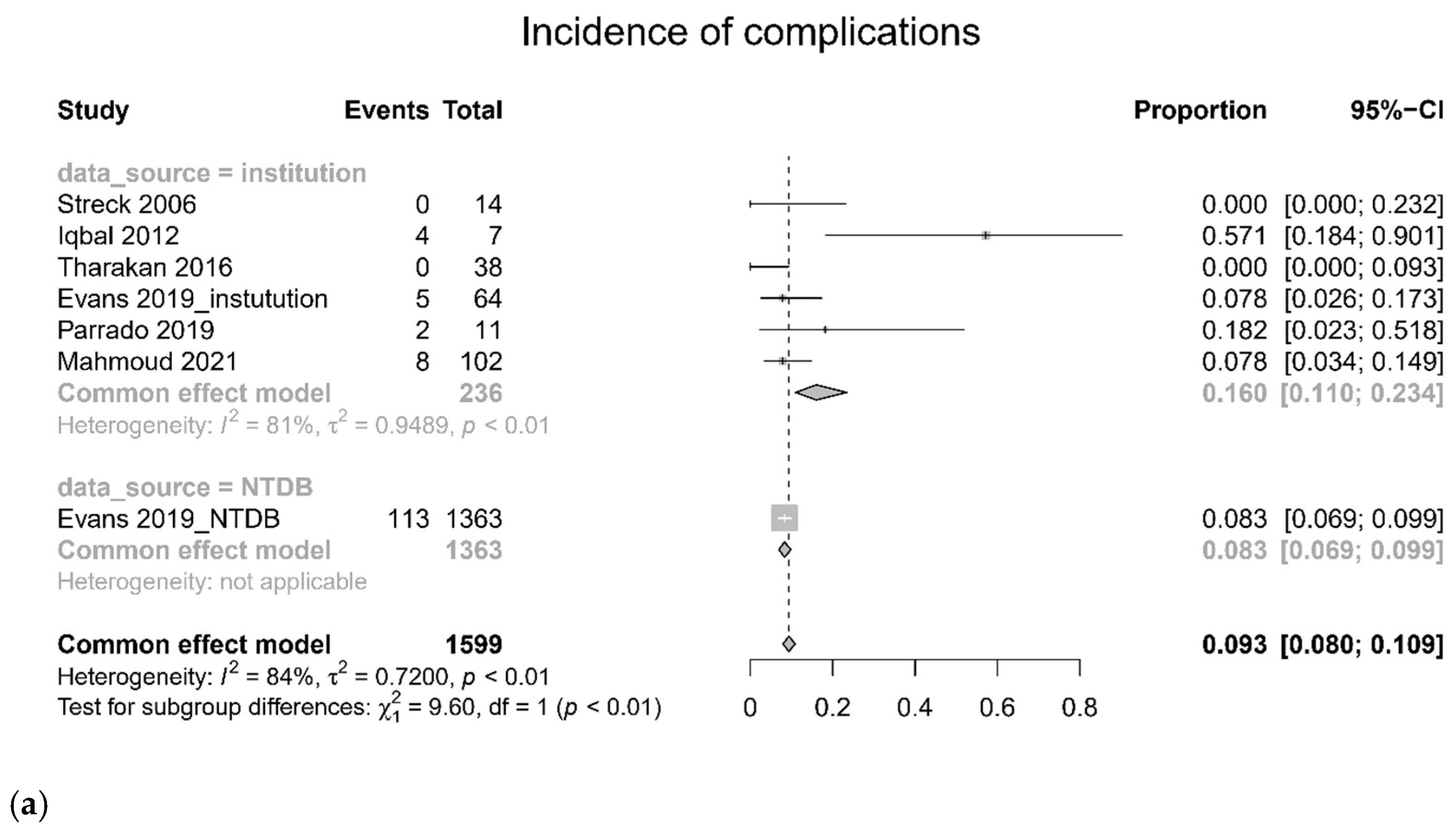
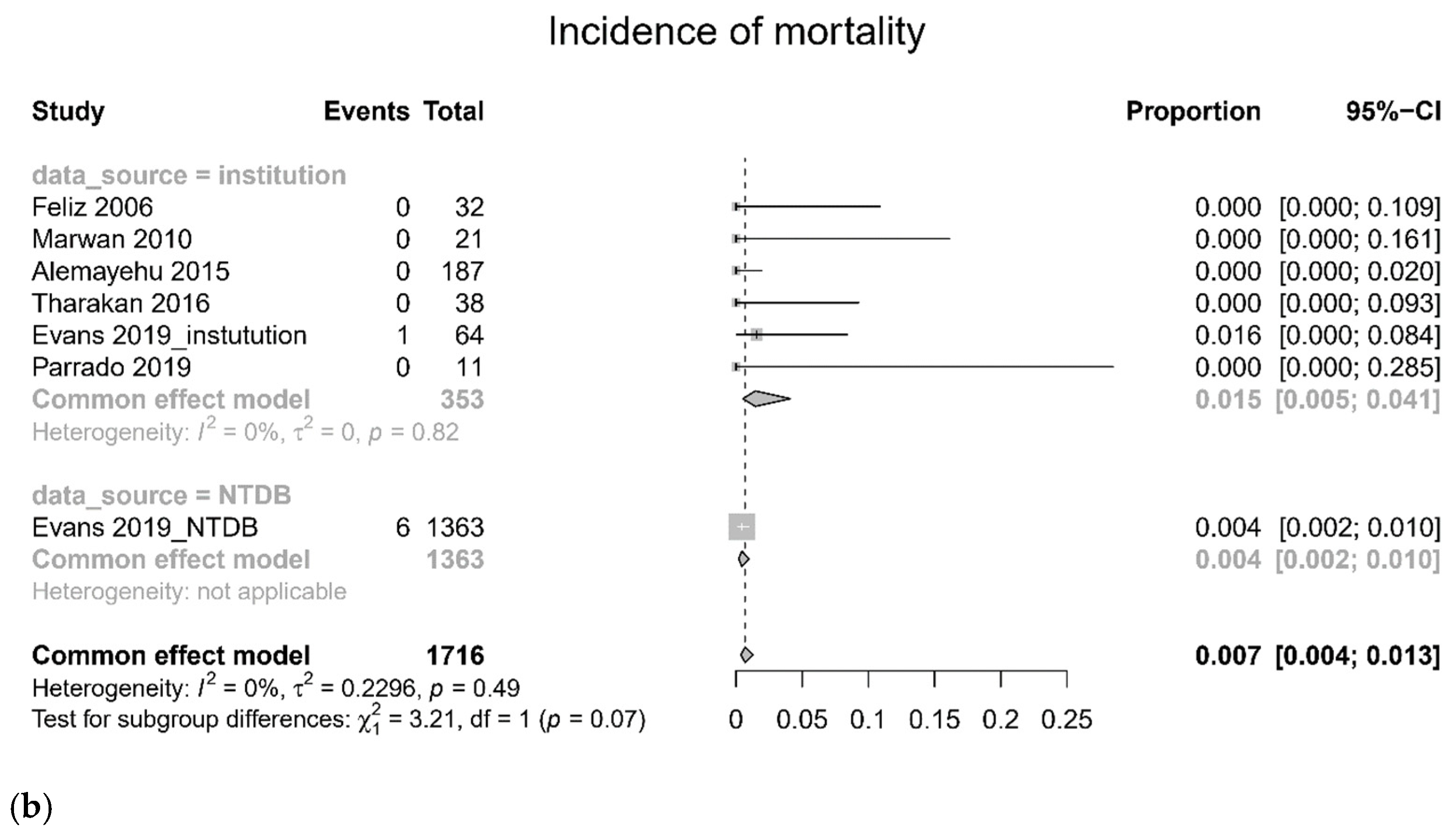
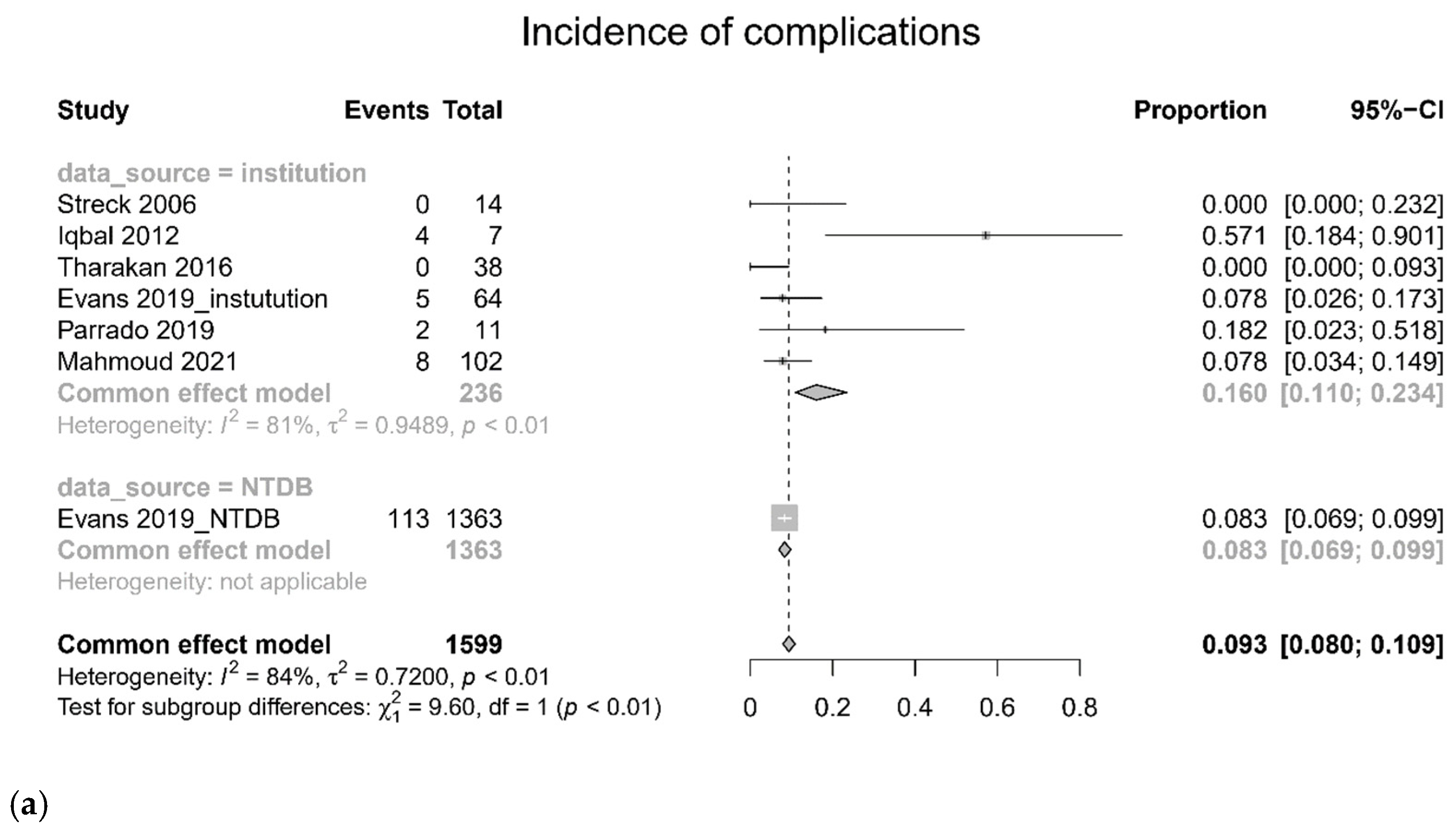
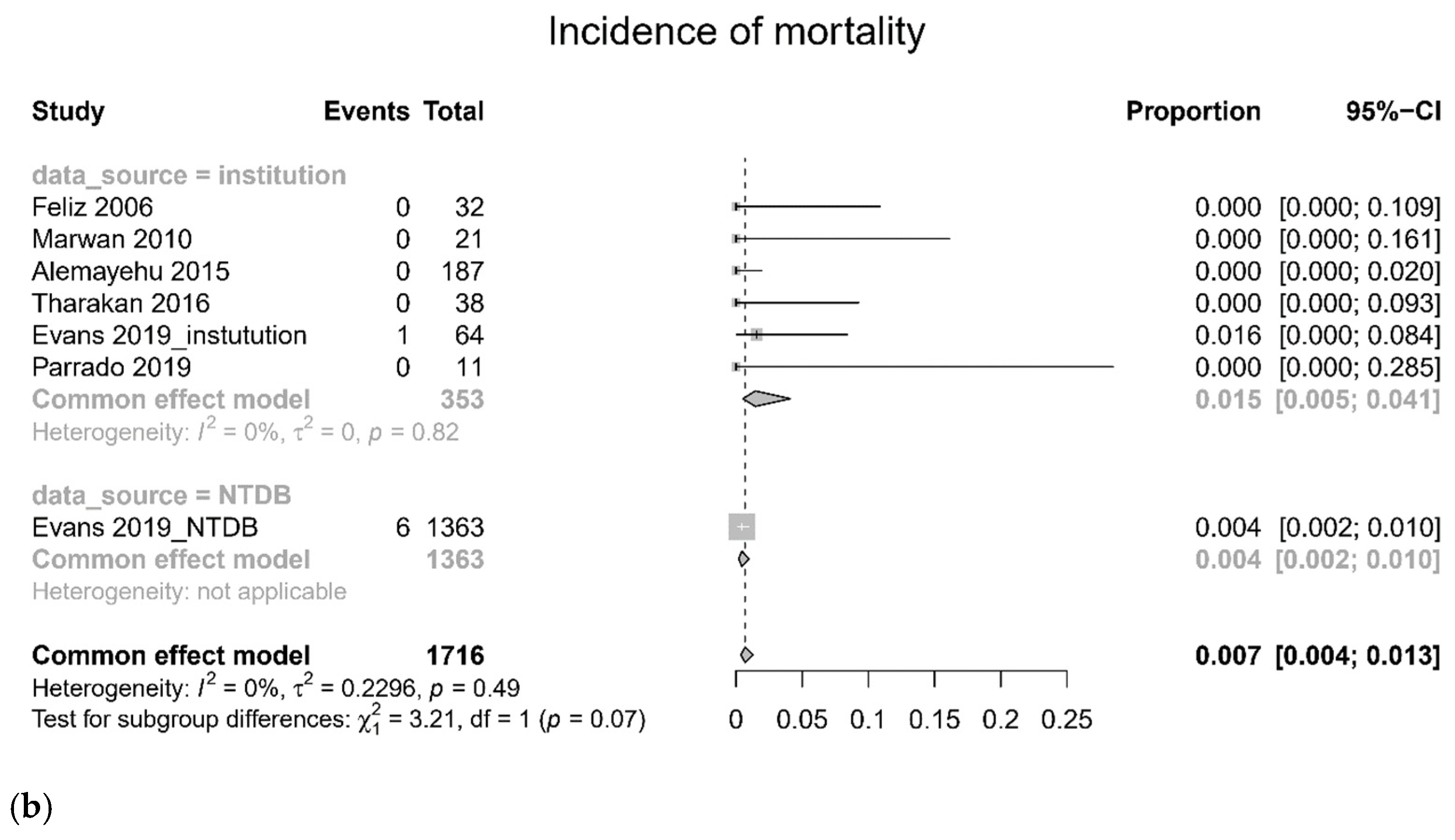
3.3. Pooled Incidence of Morbidity and Mortality in Laparoscopy
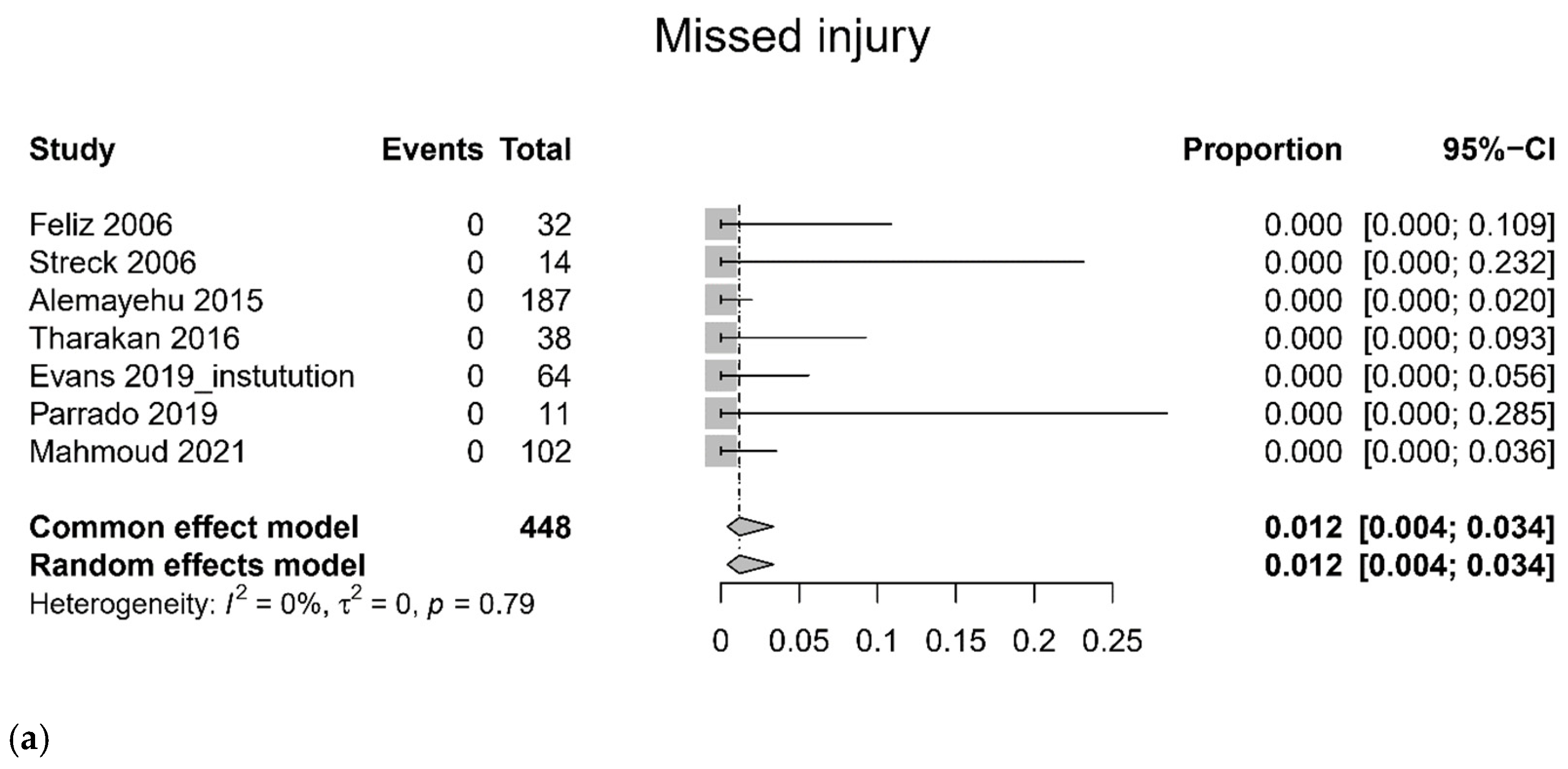
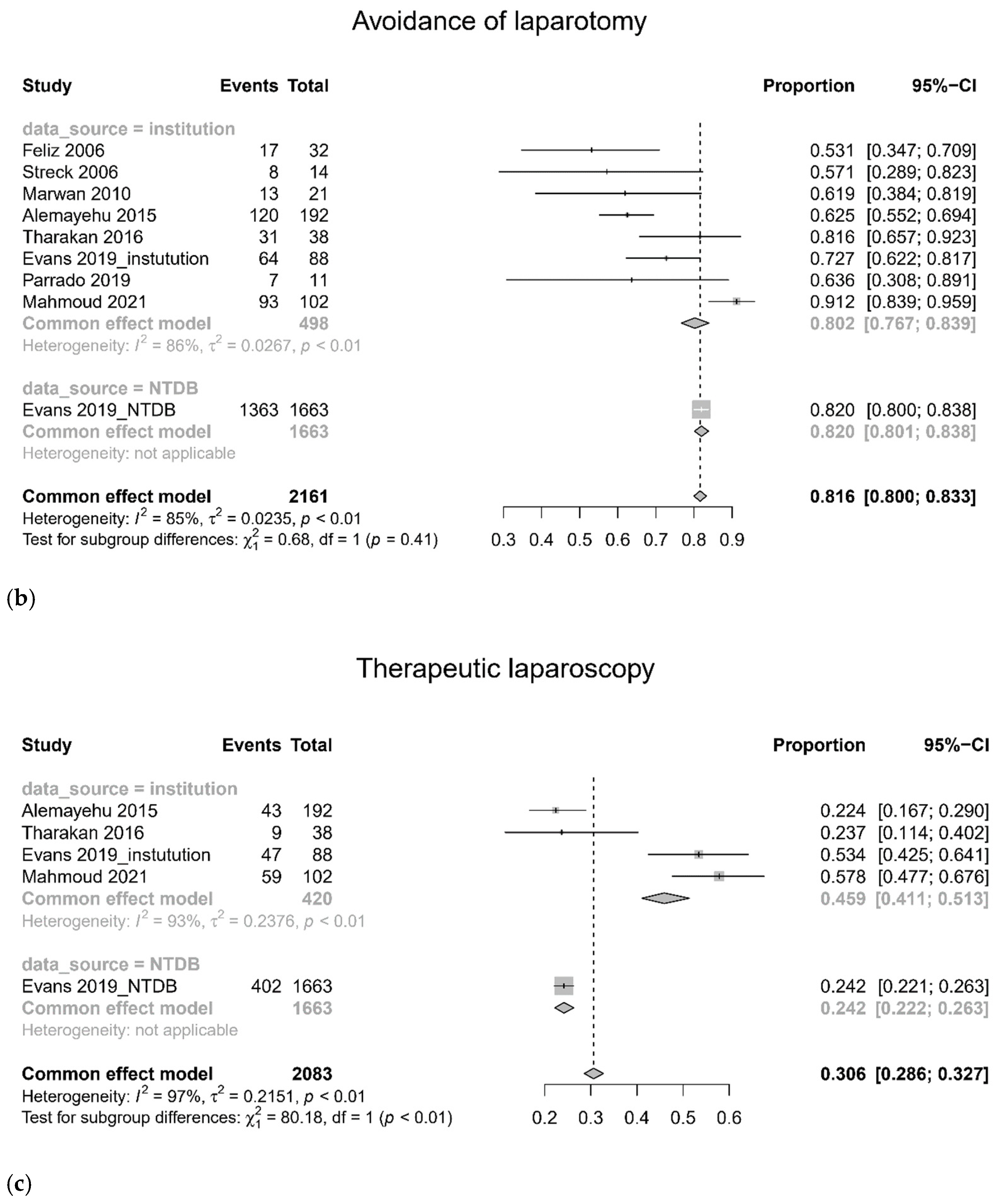
3.4. Quality of Laparoscopic Procedure
3.5. Subgroup Analysis and Sensitivity Analysis
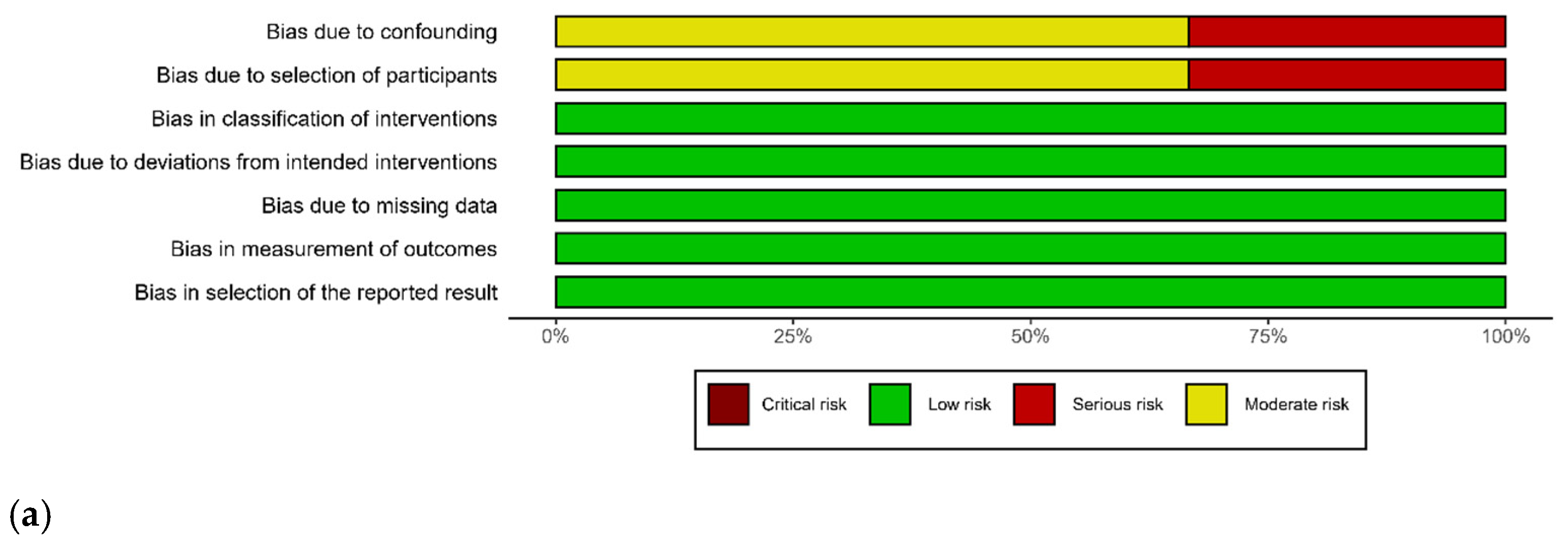
3.6. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ki, Y.-J.; Jo, Y.-G.; Park, Y.-C.; Kang, W.-S. The Efficacy and Safety of Laparoscopy for Blunt Abdominal Trauma: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 1853. [Google Scholar] [CrossRef] [PubMed]
- Shamim, A.A.; Zeineddin, S.; Zeineddin, A.; Olufajo, O.A.; Mathelier, G.O.; Iii, E.E.C.; Fullum, T.; Tran, D. Are we doing too many non-therapeutic laparotomies in trauma? An analysis of the National Trauma Data Bank. Surg. Endosc. 2019, 34, 4072–4078. [Google Scholar] [CrossRef]
- Fredriksson, F.; Christofferson, R.H.; Lilja, H.E. Adhesive small bowel obstruction after laparotomy during infancy. Br. J. Surg. 2016, 103, 284–289. [Google Scholar] [CrossRef]
- Hajibandeh, S.; Hajibandeh, S.; Gumber, A.O.; Wong, C.S. Laparoscopy versus laparotomy for the management of penetrating abdominal trauma: A systematic review and meta-analysis. Int. J. Surg. 2016, 34, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xiang, Y.; Wu, N.; Wu, L.; Yu, Z.; Zhang, M.; Wang, M.; Jiang, J.; Li, Y. A Comparison of Laparoscopy and Laparotomy for the Management of Abdominal Trauma: A Systematic Review and Meta-analysis. World J. Surg. 2015, 39, 2862–2871. [Google Scholar] [CrossRef] [PubMed]
- Cirocchi, R.; Birindelli, A.; Inaba, K.; Mandrioli, M.; Piccinini, A.; Tabola, R.; Carlini, L.; Tugnoli, G.; Di Saverio, S. Laparoscopy for Trauma and the Changes in Its Use from 1990 to 2016: A Current Systematic Review and Meta-Analysis. Surg. Laparosc. Endosc. Percutan. Tech. 2018, 28, 1–12. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, E.; Boyle, E.; O’Callaghan, A.; Coffey, J.C.; Walsh, S.R. Role of Laparoscopy in Penetrating Abdominal Trauma: A Systematic Review. World J. Surg. 2013, 37, 113–122. [Google Scholar] [CrossRef]
- Bonjer, H.J.; Deijen, C.L.; Abis, G.A.; Cuesta, M.A.; Van Der Pas, M.H.G.M.; de Lange-de Klerk, E.S.M.; Lacy, A.M.; Bemelman, W.A.; Andersson, J.; Angenete, E.; et al. A Randomized Trial of Laparoscopic versus Open Surgery for Rectal Cancer. N. Engl. J. Med. 2015, 372, 1324–1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, M.; Nakashima, H. Laparoscopic distal pancreatectomy and pancreatoduodenectomy: Is it worthwhile? A meta-analysis of laparoscopic pancreatectomy. J. Hepato-Biliary-Pancreat. Sci. 2013, 20, 421–428. [Google Scholar] [CrossRef]
- Park, Y.K.; Yoon, H.M.; Kim, Y.-W.; Park, J.Y.; Ryu, K.W.; Lee, Y.-J.; Jeong, O.; Yoon, K.Y.; Lee, J.H.; Lee, S.E.; et al. Laparoscopy-Assisted versus Open D2 Distal Gastrectomy for Advanced Gastric Cancer: Results from a Randomized Phase II Multicenter Clinical Trial (COACT 1001). Ann. Surg. 2018, 267, 638–645. [Google Scholar] [CrossRef]
- Chang, M.C.; Chair TQIP Committee. National Trauma Data Bank Report 2016; American College of Surgeons: Chicago, IL, USA, 2016. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; the PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barendregt, J.J.; Doi, S.A.; Lee, Y.Y.; Norman, R.E.; Vos, T. Meta-analysis of prevalence. J. Epidemiol. Commun. Health 2013, 67, 974–978. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, G.; Chemaitelly, H.; Abu-Raddad, L.J.; Rücker, G. Seriously misleading results using inverse of Freeman-Tukey double arcsine transformation in meta-analysis of single proportions. Res. Synth. Methods 2019, 10, 476–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, J.; Ioannidis, J.P.A.; Terrin, N.; Schmid, C.H.; Olkin, I. The case of the misleading funnel plot. BMJ 2006, 333, 597–600. [Google Scholar] [CrossRef] [Green Version]
- Feliz, A.; Shultz, B.; McKenna, C.; Gaines, B.A. Diagnostic and therapeutic laparoscopy in pediatric abdominal trauma. J. Pediatr. Surg. 2006, 41, 72–77. [Google Scholar] [CrossRef]
- Streck, C.J.; Lobe, T.E.; Pietsch, J.B.; Lovvorn, H.N., 3rd. Laparoscopic repair of traumatic bowel injury in children. J. Pediatr. Surg. 2006, 41, 1864–1869. [Google Scholar] [CrossRef] [PubMed]
- Marwan, A.; Harmon, C.M.; Georgeson, K.E.; Smith, G.F.; Muensterer, O.J. Use of Laparoscopy in the Management of Pediatric Abdominal Trauma. J. Trauma 2010, 69, 761–764. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, C.W.; Levy, S.M.; Tsao, K.; Petrosyan, M.; Kane, T.D.; Pontarelli, E.M.; Upperman, J.S.; Malek, M.; Burns, R.C.; Hill, S.; et al. Laparoscopic Versus Open Distal Pancreatectomy in the Management of Traumatic Pancreatic Disruption. J. Laparoendosc. Adv. Surg. Tech. 2012, 22, 595–598. [Google Scholar] [CrossRef]
- Alemayehu, H.; Clifton, M.; Santore, M.; Diesen, D.; Kane, T.; Petrosyan, M.; Franklin, A.; Lal, D.; Ponsky, T.; Nalugo, M.; et al. Minimally Invasive Surgery for Pediatric Trauma—A Multicenter Review. J. Laparoendosc. Adv. Surg. Tech. 2015, 25, 243–247. [Google Scholar] [CrossRef]
- Kim, A.G.; Collins, J.L.; Nance, M.L.; Blinman, T.A.; Tharakan, S.J. Laparoscopy in Pediatric Abdominal Trauma: A 13-Year Experience. Eur. J. Pediatr. Surg. 2016, 26, 443–448. [Google Scholar] [CrossRef]
- Evans, P.T.; Phelps, H.M.; Zhao, S.; Van Arendonk, K.J.; Greeno, A.L.; Collins, K.F.; Lovvorn, H.N., 3rd. Therapeutic laparoscopy for pediatric abdominal trauma. J. Pediatr. Surg. 2020, 55, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Parrado, R.; Notrica, D.M.; Garcia, N.M.; Alder, A.C.; Eubanks, I.J.; Maxson, R.T.; Letton, R.W.; Ponsky, T.A.; Peter, S.D.S.; Leys, C.; et al. Use of Laparoscopy in Pediatric Blunt and Spleen Injury: An Unexpectedly Common Procedure after Cessation of Bleeding. J. Laparoendosc. Adv. Surg. Tech. 2019, 29, 1281–1284. [Google Scholar] [CrossRef]
- Mahmoud, M.A.; Daboos, M.A.; Bayoumi, A.S.S.; Helal, A.A.; Almaawi, A.; Hassab, M.H.; Aldaraan, K.Z. Role of Minimally Invasive Surgery in Management of Penetrating Abdominal Trauma in Children. Eur. J. Pediatr. Surg. 2021, 31, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Swendiman, R.A.; Goldshore, M.A.; Blinman, T.A.; Nance, M.L. Laparoscopic Management of Pediatric Abdominal Trauma: A National Trauma Data Bank Experience. J. Laparoendosc. Adv. Surg. Tech. 2019, 29, 1052–1059. [Google Scholar] [CrossRef] [PubMed]
- Butler, E.K.; Mills, B.M.; Arbabi, S.; Groner, J.I.; Vavilala, M.S.; Rivara, F.P. Laparoscopy Compared with Laparotomy for the Management of Pediatric Blunt Abdominal Trauma. J. Surg. Res. 2020, 251, 303–310. [Google Scholar] [CrossRef]
- Train, A.T.; Naseem, H.-U.; Chen, Z.; Wilding, G.E.; Bass, K.D.; Noyes, K.; Train, W.W.; Rothstein, D.H. Predictors and Outcomes of Laparoscopy in Pediatric Trauma Patients: A Retrospective Cohort Study. J. Laparoendosc. Adv. Surg. Tech. 2019, 29, 1598–1604. [Google Scholar] [CrossRef]
- Kuebler, J.F.; Dingemann, J.; Ure, B.M.; Schukfeh, N. Thirty Years of Minimally Invasive Surgery in Children: Analysis of Meta-Analyses. Eur. J. Pediatr. Surg. 2020, 30, 420–428. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Data Source | Location | Number of Patients | Study Design | Age (Year) | Hemodynamic Status | Indication | Injury Mechanism in Patients with Laparoscopy |
|---|---|---|---|---|---|---|---|---|---|
| Feliz [19] | 2006 | Single Children’s hospital (2000–2004) | USA | laparoscopy (32), laparotomy (81) | obs, comparative | ≤18 | Stable | pneumoperitoneum, mesenteric infiltration | Blunt (81%), penetrating (19%) |
| Streck [20] | 2006 | Two Children’s hospitals (1998–2003) | USA | laparoscopy (14), laparotomy (36) | obs, comparative | <16 | Stable | isolated bowel injury | Blunt (NR), penetrating (NR) |
| Marwan [21] | 2010 | Single Children’s hospital (1997–2009) | USA | laparoscopy (21), laparotomy (71) | obs, non-comparative | 5 to 15 | Stable | pediatric abdominal trauma | Blunt (28.5%), penetrating (71.5%) |
| Iqbal [22] | 2012 | Six level-1 PTCs (2000–2010) | USA | laparoscopy (14), laparotomy (7) | obs, comparative | <18 | Stable | Grade 3 pancreas injury | NR |
| Alemayehu [23] | 2015 | Six PTCs (2000–2010) | USA | laparoscopy (192) | obs, non-comparative | 9.6 (4.2) | NR | pediatric abdominal trauma | Blunt (60%), penetrating (40%) |
| Tharakan [24] | 2016 | Single level-1 PTC (2000–2012) | USA | laparoscopy (38), laparotomy (81) | obs, comparative | ≤18 | Stable | pediatric abdominal trauma | Blunt (57.9%), penetrating (42.1%) |
| Evans [25] | 2019 | Single level-1 PTC (2005–2017) | USA | laparoscopy (88), laparotomy (305) | obs, comparative | ≤18 | Stable | pediatric abdominal trauma | Blunt (63%), penetrating (31%) |
| NTDB (2010–2015) | USA | laparoscopy (1663), laparotomy (9736) | obs, comparative | ≤18 | Stable | pediatric abdominal trauma | Blunt (50%), penetrating (44%) | ||
| Parrado [26] | 2019 | Ten level-1 PTCs (2013–2016) | USA | laparoscopy (11) | obs, non-comparative | ≤18 | Stable | Blunt liver and spleen injury | Blunt (100%) |
| Mahmoud [27] | 2021 | Three tertiary pediatric surgery center (2015–2020) | Egypt, Saudi Arabia | laparoscopy (102) | obs, non-comparative | 1 to 14 | Stable | penetrating pediatric abdominal trauma | Penetrating (100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, Y.C.; Jo, Y.G.; Ki, Y.-J.; Kang, W.S.; Kim, J. Efficacy and Safety of Laparoscopy for Mild and Moderate Pediatric Abdominal Trauma: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 1942. https://doi.org/10.3390/jcm11071942
Park YC, Jo YG, Ki Y-J, Kang WS, Kim J. Efficacy and Safety of Laparoscopy for Mild and Moderate Pediatric Abdominal Trauma: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(7):1942. https://doi.org/10.3390/jcm11071942
Chicago/Turabian StylePark, Yun Chul, Young Goun Jo, Young-Jun Ki, Wu Seong Kang, and Joongsuck Kim. 2022. "Efficacy and Safety of Laparoscopy for Mild and Moderate Pediatric Abdominal Trauma: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 7: 1942. https://doi.org/10.3390/jcm11071942
APA StylePark, Y. C., Jo, Y. G., Ki, Y.-J., Kang, W. S., & Kim, J. (2022). Efficacy and Safety of Laparoscopy for Mild and Moderate Pediatric Abdominal Trauma: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(7), 1942. https://doi.org/10.3390/jcm11071942