
A Machine-Learning-Based Risk-Prediction Tool for HIV and Sexually Transmitted Infections Acquisition over the Next 12 Months

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Data for 12-Month HIV/STI Risk-Prediction Tool Development
2.2. Predictors for 12-Month HIV/STI Risk Prediction
2.3. Model Development and Training for Building a 12-Month HIV/STI Risk-Prediction Tool
2.4. Twelve-Month HIV/STI Risk Estimate
2.5. Establishment of the 12-Month HIV/STI Risk-Prediction Tool and Implementation of the Tool on a Web Server
3. Results
3.1. Characteristics of the 12-Month HIV/STI Risk-Prediction Tool Development Data
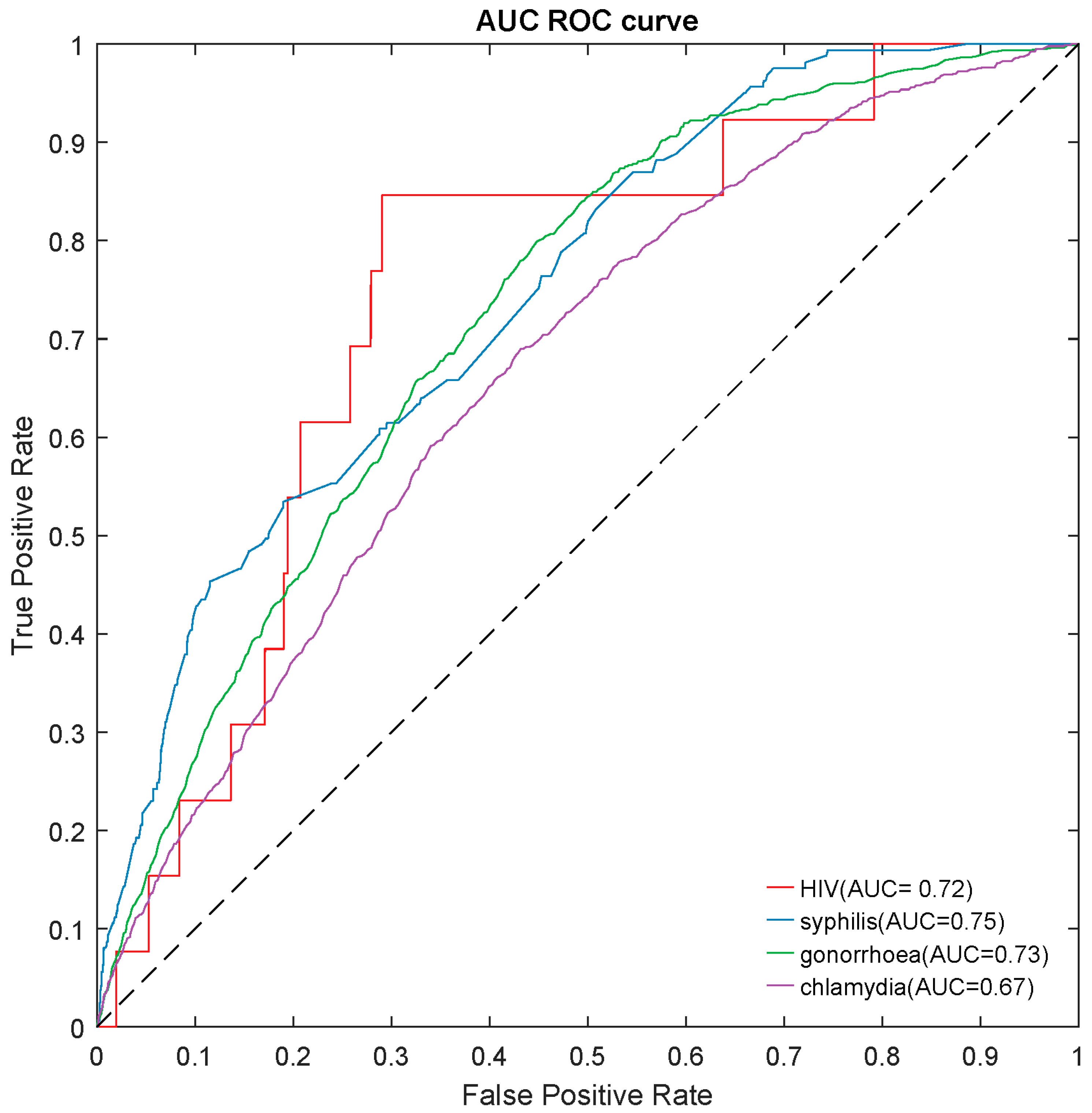
3.2. Selecting the Best Machine Learning Model for 12-Month HIV/STI Risk-Prediction Tool
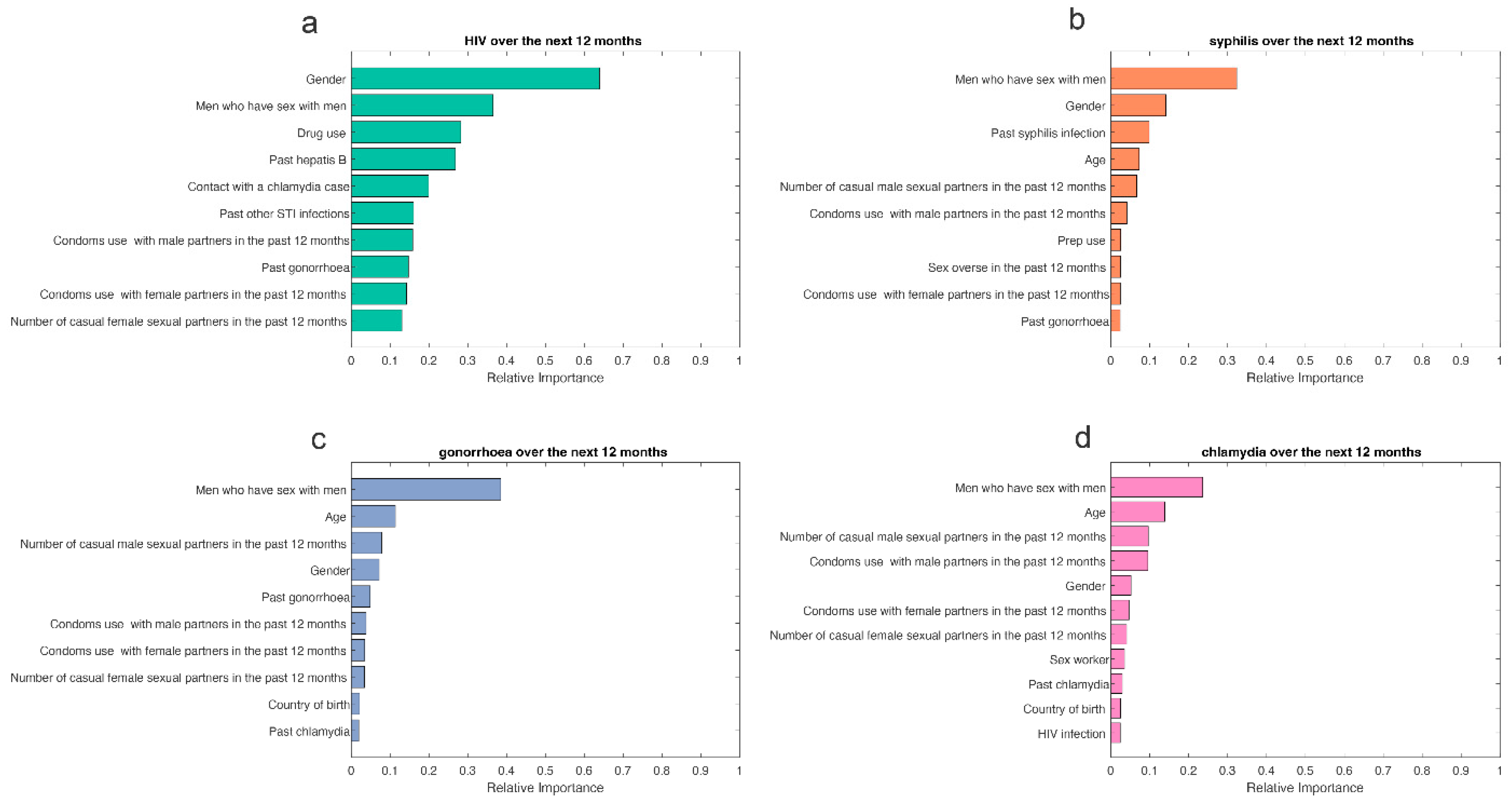
3.3. Selecting the Most Important Predictors for the 12-Month HIV/STI Risk-Prediction Tool
3.4. Establishment of the 12-Month HIV/STI Risk-Prediction Model
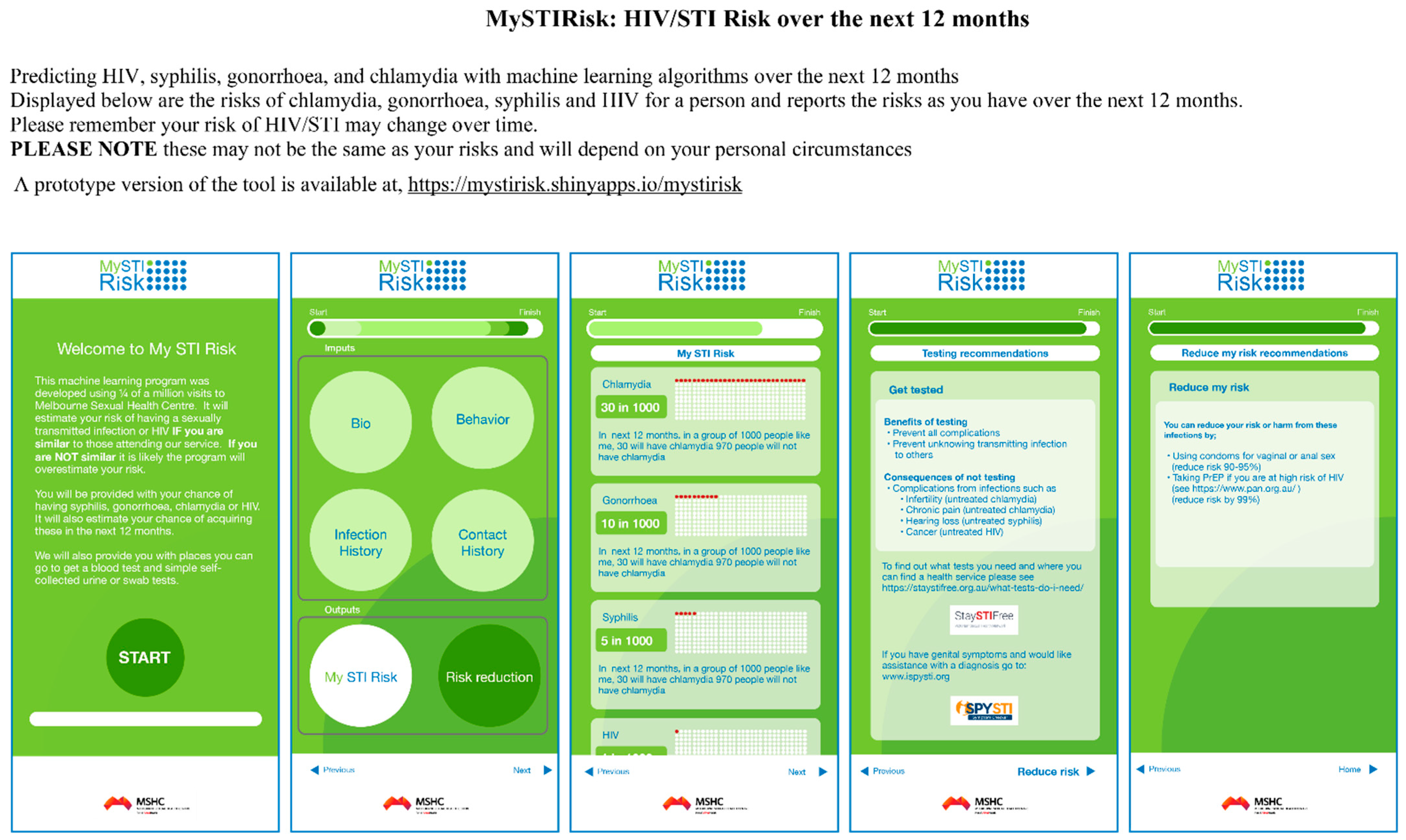
3.5. Twelve-Month HIV/STI Risk Estimates and User Interface
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramchandani, M.S.; Golden, M.R. Confronting Rising STIs in the Era of PrEP and Treatment as Prevention. Curr. HIV/AIDS Rep. 2019, 16, 244–256. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Committee on Prevention and Control of Sexually Transmitted Diseases. The Hidden Epidemic: Confronting Sexually Transmitted Diseases; Eng, T.R., Butler, W.T., Eds.; National Academies Press (US), National Academy of Sciences: Washington, DC, USA, 1997. [Google Scholar]
- World Health Organization. Global health sector strategy on sexually transmitted infections 2016–2021: Toward ending STIs. In Global Health Sector Strategy on Sexually Transmitted Infections 2016–2021: Toward Ending STIs; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- UNAIDS. UNAIDS DATA 2018. Available online: https://www.unaids.org/sites/default/files/media_asset/unaids-data-2018_en.pdf (accessed on 1 March 2022).
- Wei, C.; Herrick, A.; Raymond, H.F.; Anglemyer, A.; Gerbase, A.; Noar, S.M. Social marketing interventions to increase HIV/STI testing uptake among men who have sex with men and male-to-female transgender women. Cochrane Database Syst. Rev. 2011, Cd009337. [Google Scholar] [CrossRef] [PubMed]
- Chow, E.P.F.; Grulich, A.E.; Fairley, C.K. Epidemiology and prevention of sexually transmitted infections in men who have sex with men at risk of HIV. Lancet HIV 2019, 6, e396–e405. [Google Scholar] [CrossRef]
- World Health Organization; Regional Office for South-East Asia. Moving Ahead on Elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region—Progress and Challenges; World Health Organization, Regional Office for South-East Asia: New Delhi, India, 2019. [Google Scholar]
- Vermund, S.H.; Wilson, C.M. Barriers to HIV testing-where next? Lancet 2002, 360, 1186–1187. [Google Scholar] [CrossRef]
- Lemoh, C.; Guy, R.; Yohannes, K.; Lewis, J.; Street, A.; Biggs, B.; Hellard, M. Delayed diagnosis of HIV infection in Victoria 1994 to 2006. Sex. Health 2009, 6, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Sobrino-Vegas, P.; Miguel, L.G.-S.; Caro-Murillo, A.M.; Miró, J.M.; Viciana, P.; Tural, C.; Saumoy, M.; Santos, I.; Sola, J.; Amo, J.d. Delayed diagnosis of HIV infection in a multicenter cohort: Prevalence, risk factors, response to HAART and impact on mortality. Curr. HIV Res. 2009, 7, 224–230. [Google Scholar] [CrossRef]
- Ooi, C.Y.; Ng, C.J.; Sales, A.E.; Lim, H.M. Implementation Strategies for Web-Based Apps for Screening: Scoping Review. J. Med. Internet Res. 2020, 22, e15591. [Google Scholar] [CrossRef]
- Lo, L.L.; Collins, I.M.; Bressel, M.; Butow, P.; Emery, J.; Keogh, L.; Weideman, P.; Steel, E.; Hopper, J.L.; Trainer, A.H.; et al. The iPrevent Online Breast Cancer Risk Assessment and Risk Management Tool: Usability and Acceptability Testing. JMIR Form. Res. 2018, 2, e24. [Google Scholar] [CrossRef]
- Patel, B.; Sengupta, P. Machine learning for predicting cardiac events: What does the future hold? Expert Rev. Cardiovasc. Ther. 2020, 18, 77–84. [Google Scholar] [CrossRef]
- Roy, A.; Nikolitch, K.; McGinn, R.; Jinah, S.; Klement, W.; Kaminsky, Z.A. A machine learning approach predicts future risk to suicidal ideation from social media data. NPJ Digit. Med. 2020, 3, 78. [Google Scholar] [CrossRef]
- Whiting, D.; Fazel, S. How accurate are suicide risk prediction models? Asking the right questions for clinical practice. Evid.-Based Ment. Health 2019, 22, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Farran, B.; AlWotayan, R.; Alkandari, H.; Al-Abdulrazzaq, D.; Channanath, A.; Thanaraj, T.A. Use of Non-invasive Parameters and Machine-Learning Algorithms for Predicting Future Risk of Type 2 Diabetes: A Retrospective Cohort Study of Health Data from Kuwait. Front. Endocrinol. 2019, 10, 624. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Cho, H.E.; Kim, J.H.; Wall, M.M.; Stern, Y.; Lim, H.; Yoo, S.; Kim, H.S.; Cha, J. Machine learning prediction of incidence of Alzheimer’s disease using large-scale administrative health data. NPJ Digit. Med. 2020, 3, 46. [Google Scholar] [CrossRef] [PubMed]
- Kwiecinski, J.; Tzolos, E.; Meah, M.; Cadet, S.; Adamson, P.D.; Grodecki, K.; Joshi, N.V.; Moss, A.J.; Williams, M.C.; van Beek, E.J.; et al. Machine-learning with (18)F-sodium fluoride PET and quantitative plaque analysis on CT angiography for the future risk of myocardial infarction. J. Nucl. Med. 2021, 63, 158–165. [Google Scholar] [CrossRef]
- Gruber, S.; Krakower, D.; Menchaca, J.T.; Hsu, K.; Hawrusik, R.; Maro, J.C.; Cocoros, N.M.; Kruskal, B.A.; Wilson, I.B.; Mayer, K.H.; et al. Using electronic health records to identify candidates for human immunodeficiency virus pre-exposure prophylaxis: An application of super learning to risk prediction when the outcome is rare. Stat. Med. 2020, 39, 3059–3073. [Google Scholar] [CrossRef]
- Marcus, J.L.; Hurley, L.B.; Krakower, D.S.; Alexeeff, S.; Silverberg, M.J.; Volk, J.E. Use of electronic health record data and machine learning to identify candidates for HIV pre-exposure prophylaxis: A modelling study. Lancet HIV 2019, 6, e688–e695. [Google Scholar] [CrossRef]
- Bzdok, D.; Altman, N.; Krzywinski, M. Statistics versus machine learning. Nat. Methods 2018, 15, 233–234. [Google Scholar] [CrossRef]
- Misson, J.; Chow, E.P.F.; Chen, M.Y.; Read, T.R.H.; Bradshaw, C.S.; Fairley, C.K. Trends in gonorrhoea infection and overseas sexual contacts among females attending a sexual health centre in Melbourne, Australia, 2008–2015. Commun. Dis. Intell. 2018, 42, 1–10. [Google Scholar]
- Chow, E.P.F.; Hocking, J.S.; Ong, J.J.; Phillips, T.R.; Fairley, C.K. Sexually Transmitted Infection Diagnoses and Access to a Sexual Health Service Before and After the National Lockdown for COVID-19 in Melbourne, Australia. Open Forum Infect. Dis. 2021, 8, ofaa536. [Google Scholar] [CrossRef]
- Chow, E.P.F.; Ong, J.J.; Donovan, B.; Foster, R.; Phillips, T.R.; McNulty, A.; Fairley, C.K. Comparing HIV Post-Exposure Prophylaxis, Testing, and New Diagnoses in Two Australian Cities with Different Lockdown Measures during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10814. [Google Scholar] [CrossRef]
- Bao, Y.; Medland, N.A.; Fairley, C.K.; Wu, J.; Shang, X.; Chow, E.P.F.; Xu, X.; Ge, Z.; Zhuang, X.; Zhang, L. Predicting the diagnosis of HIV and sexually transmitted infections among men who have sex with men using machine learning approaches. J. Infect. 2021, 82, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Shehzad, A.; Rockwood, K.; Stanley, J.; Dunn, T.; Howlett, S.E. Use of Patient-Reported Symptoms from an Online Symptom Tracking Tool for Dementia Severity Staging: Development and Validation of a Machine Learning Approach. J. Med. Internet Res. 2020, 22, e20840. [Google Scholar] [CrossRef] [PubMed]
- Menardi, G.; Torelli, N. Training and assessing classification rules with imbalanced data. Data Min. Knowl. Discov. 2014, 28, 92–122. [Google Scholar] [CrossRef]
- Liao, X.; Kerr, D.; Morales, J.; Duncan, I. Application of Machine Learning to Identify Clustering of Cardiometabolic Risk Factors in U.S. Adults. Diabetes Technol. Ther. 2019, 21, 245–253. [Google Scholar] [CrossRef]
- Clift, A.K.; Coupland, C.A.C.; Keogh, R.H.; Diaz-Ordaz, K.; Williamson, E.; Harrison, E.M.; Hayward, A.; Hemingway, H.; Horby, P.; Mehta, N.; et al. Living risk prediction algorithm (QCOVID) for risk of hospital admission and mortality from coronavirus 19 in adults: National derivation and validation cohort study. BMJ 2020, 371, m3731. [Google Scholar] [CrossRef]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef]
- Manuel, D.G.; Tuna, M.; Bennett, C.; Hennessy, D.; Rosella, L.; Sanmartin, C.; Tu, J.V.; Perez, R.; Fisher, S.; Taljaard, M. Development and validation of a cardiovascular disease risk-prediction model using population health surveys: The Cardiovascular Disease Population Risk Tool (CVDPoRT). CMAJ 2018, 190, E871–E882. [Google Scholar] [CrossRef]
- Rossello, X.; Dorresteijn, J.A.; Janssen, A.; Lambrinou, E.; Scherrenberg, M.; Bonnefoy-Cudraz, E.; Cobain, M.; Piepoli, M.F.; Visseren, F.L.; Dendale, P. Risk prediction tools in cardiovascular disease prevention: A report from the ESC Prevention of CVD Programme led by the European Association of Preventive Cardiology (EAPC) in collaboration with the Acute Cardiovascular Care Association (ACCA) and the Association of Cardiovascular Nursing and Allied Professions (ACNAP). Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 522–532. [Google Scholar] [CrossRef]
- Fisher, S.; Manuel, D.G.; Hsu, A.T.; Bennett, C.; Tuna, M.; Eddeen, A.B.; Sequeira, Y.; Jessri, M.; Taljaard, M.; Anderson, G.M.; et al. Development and validation of a predictive algorithm for risk of dementia in the community setting. J. Epidemiol. Community Health 2021, 75, 843–853. [Google Scholar] [CrossRef]
- Lai, H.; Huang, H.; Keshavjee, K.; Guergachi, A.; Gao, X. Predictive models for diabetes mellitus using machine learning techniques. BMC Endocr. Disord. 2019, 19, 101. [Google Scholar] [CrossRef]
- Lindström, J.; Tuomilehto, J. The diabetes risk score: A practical tool to predict type 2 diabetes risk. Diabetes Care 2003, 26, 725–731. [Google Scholar] [CrossRef]
- Collins, I.M.; Bickerstaffe, A.; Ranaweera, T.; Maddumarachchi, S.; Keogh, L.; Emery, J.; Mann, G.B.; Butow, P.; Weideman, P.; Steel, E.; et al. iPrevent®: A tailored, web-based, decision support tool for breast cancer risk assessment and management. Breast Cancer Res. Treat. 2016, 156, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Lau, Y.K.; Caverly, T.J.; Cao, P.; Cherng, S.T.; West, M.; Gaber, C.; Arenberg, D.; Meza, R. Evaluation of a personalized, web-based decision aid for lung cancer screening. Am. J. Prev. Med. 2015, 49, e125–e129. [Google Scholar] [CrossRef] [PubMed]
- Brooks, B.A.; Haynes, K.; Smith, J.; McFadden, T.; Robins, D.L. Implementation of web-based autism screening in an urban clinic. Clin. Pediatr. 2016, 55, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Poe, S.S.; Dawson, P.B.; Cvach, M.; Burnett, M.; Kumble, S.; Lewis, M.; Thompson, C.B.; Hill, E.E. The Johns Hopkins Fall Risk Assessment Tool: A Study of Reliability and Validity. J. Nurs. Care Qual. 2018, 33, 10–19. [Google Scholar] [CrossRef]
- Jacobson, N.C.; Yom-Tov, E.; Lekkas, D.; Heinz, M.; Liu, L.; Barr, P.J. Impact of online mental health screening tools on help-seeking, care receipt, and suicidal ideation and suicidal intent: Evidence from internet search behavior in a large U.S. cohort. J. Psychiatr. Res. 2022, 145, 276–283. [Google Scholar] [CrossRef]
- Diez-Canseco, F.; Toyama, M.; Ipince, A.; Perez-Leon, S.; Cavero, V.; Araya, R.; Miranda, J.J. Integration of a Technology-Based Mental Health Screening Program into Routine Practices of Primary Health Care Services in Peru (The Allillanchu Project): Development and Implementation. J. Med. Internet Res. 2018, 20, e100. [Google Scholar] [CrossRef]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Primary prevention of cardiovascular disease through population-wide motivational strategies: Insights from using smartphones in stroke prevention. BMJ Glob. Health 2016, 2, e000306. [Google Scholar] [CrossRef]
- Kay, M.; Santos, J.; Takane, M. mHealth: New horizons for health through mobile technologies. World Health Organ. 2011, 64, 66–71. [Google Scholar]
- Turakhia, M.P.; Desai, S.A.; Harrington, R.A. The outlook of digital health for cardiovascular medicine: Challenges but also extraordinary opportunities. JAMA Cardiol. 2016, 1, 743–744. [Google Scholar] [CrossRef]
- Clifton, S.; Mercer, C.H.; Sonnenberg, P.; Tanton, C.; Field, N.; Gravningen, K.; Hughes, G.; Mapp, F.; Johnson, A.M. STI risk perception in the British population and how it relates to sexual behaviour and STI healthcare use: Findings from a cross-sectional survey (Natsal-3). EClinicalMedicine 2018, 2, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.; Du, J.; Fujimoto, K.; Li, F.; Schneider, J.; Tao, C. Application of artificial intelligence and machine learning for HIV prevention interventions. Lancet HIV 2022, 9, e54–e62. [Google Scholar] [CrossRef]
- Marcus, J.L.; Sewell, W.C.; Balzer, L.B.; Krakower, D.S. Artificial Intelligence and Machine Learning for HIV Prevention: Emerging Approaches to Ending the Epidemic. Curr. HIV/AIDS Rep. 2020, 17, 171–179. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Sexually Transmitted Infections (STIs): The Importance of a Renewed Commitment to STI Prevention and Control in Achieving Global Sexual and Reproductive Health; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Garofalo, R.; Hotton, A.L.; Kuhns, L.M.; Gratzer, B.; Mustanski, B. Incidence of HIV Infection and Sexually Transmitted Infections and Related Risk Factors Among Very Young Men Who Have Sex with Men. J. Acquir. Immune Defic. Syndr. 2016, 72, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Selvey, L.A.; Slimings, C.; Adams, E.; Manuel, J. Incidence and predictors of HIV, chlamydia and gonorrhoea among men who have sex with men attending a peer-based clinic. Sex. Health 2018, 15, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Dukers-Muijrers, N.; van Rooijen, M.S.; Hogewoning, A.; van Liere, G.; Steenbakkers, M.; Hoebe, C. Incidence of repeat testing and diagnoses of Chlamydia trachomatis and Neisseria gonorrhoea in swingers, homosexual and heterosexual men and women at two large Dutch STI clinics, 2006–2013. Sex. Transm. Infect. 2017, 93, 383–389. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cheung, K.T.; Fairley, C.K.; Read, T.R.; Denham, I.; Fehler, G.; Bradshaw, C.S.; Chen, M.Y.; Chow, E.P. HIV Incidence and Predictors of Incident HIV among Men Who Have Sex with Men Attending a Sexual Health Clinic in Melbourne, Australia. PLoS ONE 2016, 11, e0156160. [Google Scholar] [CrossRef]
- Lustria, M.L.A.; Noar, S.M.; Cortese, J.; Van Stee, S.K.; Glueckauf, R.L.; Lee, J. A meta-analysis of web-delivered tailored health behavior change interventions. J. Health Commun. 2013, 18, 1039–1069. [Google Scholar] [CrossRef]
- Wister, A.; Loewen, N.; Kennedy-Symonds, H.; McGowan, B.; McCoy, B.; Singer, J. One-year follow-up of a therapeutic lifestyle intervention targeting cardiovascular disease risk. CMAJ 2007, 177, 859–865. [Google Scholar] [CrossRef]
- Underhill, K.; Operario, D.; Skeer, M.; Mimiaga, M.; Mayer, K. Packaging PrEP to prevent HIV: An integrated framework to plan for pre-exposure prophylaxis implementation in clinical practice. J. Acquir. Immune Defic. Syndr. 2010, 55, 8–13. [Google Scholar] [CrossRef]
- Yuwaki, K.; Kuchiba, A.; Otsuki, A.; Odawara, M.; Okuhara, T.; Ishikawa, H.; Inoue, M.; Tsugane, S.; Shimazu, T. Effectiveness of a Cancer Risk Prediction Tool on Lifestyle Habits: A Randomized Controlled Trial. Cancer Epidemiol. Biomark. Prev. 2021, 30, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Fairley, C.K.; Sze, J.K.; Vodstrcil, L.A.; Chen, M.Y. Computer-assisted self interviewing in sexual health clinics. Sex. Transm. Dis. 2010, 37, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, F.; Qi, Z.; Duan, K.; Xi, D.; Zhu, Y.; Zhu, H.; Xiong, H.; He, Q. A comprehensive survey on transfer learning. Proc. IEEE 2020, 109, 43–76. [Google Scholar] [CrossRef]
- Lee, D.M.; Fairley, C.K.; Sze, J.K.; Kuo, T.; Cummings, R.; Bilardi, J.; Chen, M.Y. Access to sexual health advice using an automated, internet-based risk assessment service. Sex. Health 2009, 6, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Chow, E.P.F.; Ong, J.J.; Hoebe, C.; Williamson, D.; Shen, M.; Kong, F.Y.S.; Hocking, J.S.; Fairley, C.K.; Zhang, L. Modelling the contribution that different sexual practices involving the oropharynx and saliva have on Neisseria gonorrhoeae infections at multiple anatomical sites in men who have sex with men. Sex. Transm. Infect. 2021, 97, 183–189. [Google Scholar] [CrossRef]
- Vandormael, A.; Dobra, A.; Bärnighausen, T.; de Oliveira, T.; Tanser, F. Incidence rate estimation, periodic testing and the limitations of the mid-point imputation approach. Int. J. Epidemiol. 2018, 47, 236–245. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Predictors | HIV | Syphilis | Gonorrhoea | Chlamydia | ||||
|---|---|---|---|---|---|---|---|---|
| No | Yes | No | Yes | No | Yes | No | Yes | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Gender | ||||||||
| Female | 16,478 (25.4%) | 1 (1.5%) | 14,476 (25.8%) | 12 (1.6%) | 18,018 (31.9%) | 298 (7.3%) | 18,652 (31.6%) | 687 (15.0%) |
| Male | 48,499 (74.6%) | 65 (98.5%) | 41,663 (74.2%) | 738 (98.4%) | 38,521 (68.1%) | 3761 (92.7%) | 40,299 (68.4%) | 3891 (85.0%) |
| Men who have sex with men | ||||||||
| No | 5797 (12.0%) | 1 (1.5%) | 3854 (9.3%) | 14 (1.9%) | 5036 (13.1%) | 55 (1.5%) | 6713 (16.7%) | 403 (10.4%) |
| Yes | 42,702 (88.0%) | 64 (98.5%) | 37,809 (90.7%) | 724 (98.1%) | 33,485 (86.9%) | 3706 (98.5%) | 33,586 (83.3%) | 3488 (89.6%) |
| Country of birth | ||||||||
| Australia | 30,473 (46.9%) | 29 (43.9%) | 25,887 (46.1%) | 355 (47.3%) | 25,587 (45.3%) | 2023 (49.8%) | 27,081 (45.9%) | 2112 (46.1%) |
| Overseas | 31,978 (49.2%) | 34 (51.5%) | 28,099 (50.1%) | 367 (48.9%) | 28812 (51.0%) | 1900 (46.8%) | 29,684 (50.4%) | 2310 (50.5%) |
| Missing | 2526 (3.9%) | 3 (4.5%) | 2153 (3.8%) | 28 (3.7%) | 2140 (3.8%) | 136 (3.4%) | 2186 (3.7%) | 156 (3.4%) |
| Age at consultation | ||||||||
| Median [IQR] | 29.0 (25.0, 35.0) | 30.5 (27.0, 43.0) | 29.0 (25.0, 36.0) | 30.0 (26.0, 37.0) | 29.0 (25.0, 35.0) | 29.0 (25.0, 34.0) | 29.0 (25.0, 35.0) | 28.0 (24.0, 34.0) |
| Current PrEP use | ||||||||
| No | 62,195 (95.7%) | 64 (97.0%) | 53,496 (95.3%) | 658 (87.7%) | 53,998 (95.5%) | 3656 (90.1%) | 56,519 (95.9%) | 4167 (91.0%) |
| Yes | 2782 (4.3%) | 2 (3.0%) | 2643 (4.7%) | 92 (12.3%) | 2541 (4.5%) | 403 (9.9%) | 2432 (4.1%) | 411 (9.0%) |
| Current sex worker | ||||||||
| No | 57,383 (88.3%) | 65 (98.5%) | 49,068 (87.4%) | 736 (98.1%) | 49,458 (87.5%) | 3902 (96.1%) | 51,981 (88.2%) | 4418 (96.5%) |
| Yes | 7594 (11.7%) | 1 (1.5%) | 7071 (12.6%) | 14 (1.9%) | 7081 (12.5%) | 157 (3.9%) | 6970 (11.8%) | 160 (3.5%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, X.; Ge, Z.; Chow, E.P.F.; Yu, Z.; Lee, D.; Wu, J.; Ong, J.J.; Fairley, C.K.; Zhang, L. A Machine-Learning-Based Risk-Prediction Tool for HIV and Sexually Transmitted Infections Acquisition over the Next 12 Months. J. Clin. Med. 2022, 11, 1818. https://doi.org/10.3390/jcm11071818
Xu X, Ge Z, Chow EPF, Yu Z, Lee D, Wu J, Ong JJ, Fairley CK, Zhang L. A Machine-Learning-Based Risk-Prediction Tool for HIV and Sexually Transmitted Infections Acquisition over the Next 12 Months. Journal of Clinical Medicine. 2022; 11(7):1818. https://doi.org/10.3390/jcm11071818
Chicago/Turabian StyleXu, Xianglong, Zongyuan Ge, Eric P. F. Chow, Zhen Yu, David Lee, Jinrong Wu, Jason J. Ong, Christopher K. Fairley, and Lei Zhang. 2022. "A Machine-Learning-Based Risk-Prediction Tool for HIV and Sexually Transmitted Infections Acquisition over the Next 12 Months" Journal of Clinical Medicine 11, no. 7: 1818. https://doi.org/10.3390/jcm11071818
APA StyleXu, X., Ge, Z., Chow, E. P. F., Yu, Z., Lee, D., Wu, J., Ong, J. J., Fairley, C. K., & Zhang, L. (2022). A Machine-Learning-Based Risk-Prediction Tool for HIV and Sexually Transmitted Infections Acquisition over the Next 12 Months. Journal of Clinical Medicine, 11(7), 1818. https://doi.org/10.3390/jcm11071818