
Analysis of the Ability to Tolerate Body Balance Disturbance in Relation to Selected Changes in the Sagittal Plane of the Spine in Early School-Age Children

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
- age 7–10 years,
- no health issues that might affect the test result, i.e., diagnosed neurological diseases, posture defects, musculoskeletal injuries (vision defects, disturbances in neuromuscular coordination, excessive body weight, past injuries of the spine and lower limbs),
- written consent of a parent (guardian) to participate in the study,
- consent of school principals to the examination,
- attending primary schools in the Psary commune,
- the ability to communicate with the examined child necessary to conduct the examination (the child’s willingness to undress and prepare for the examination).
- no written consent of the child’s parents or guardians,
- age of the examined child under 7 and over 10 years of age,
- diseases that make it impossible to conduct the test or that may affect its result (injuries, fractures of the lower or upper limbs, or spine),
- inability to communicate with the examined child necessary for the examination (the child’s refusal to undress and prepare for the examination).
- Interview, including information on the date of birth, age in years and months.
- The clinical trial included:
- bodyweight measurement,
- measuring the body height in an upright position,
- assessment of the alignment of the spinous processes of the thoracic and lumbar vertebrae,
- assessment of the location of selected anatomical landmarks of the torso: processes of the scapulae and inferior angles of the scapulae, triangles of the waist, anterior superior and posterior superior iliac spines, and the greater trochanter.
- 3.
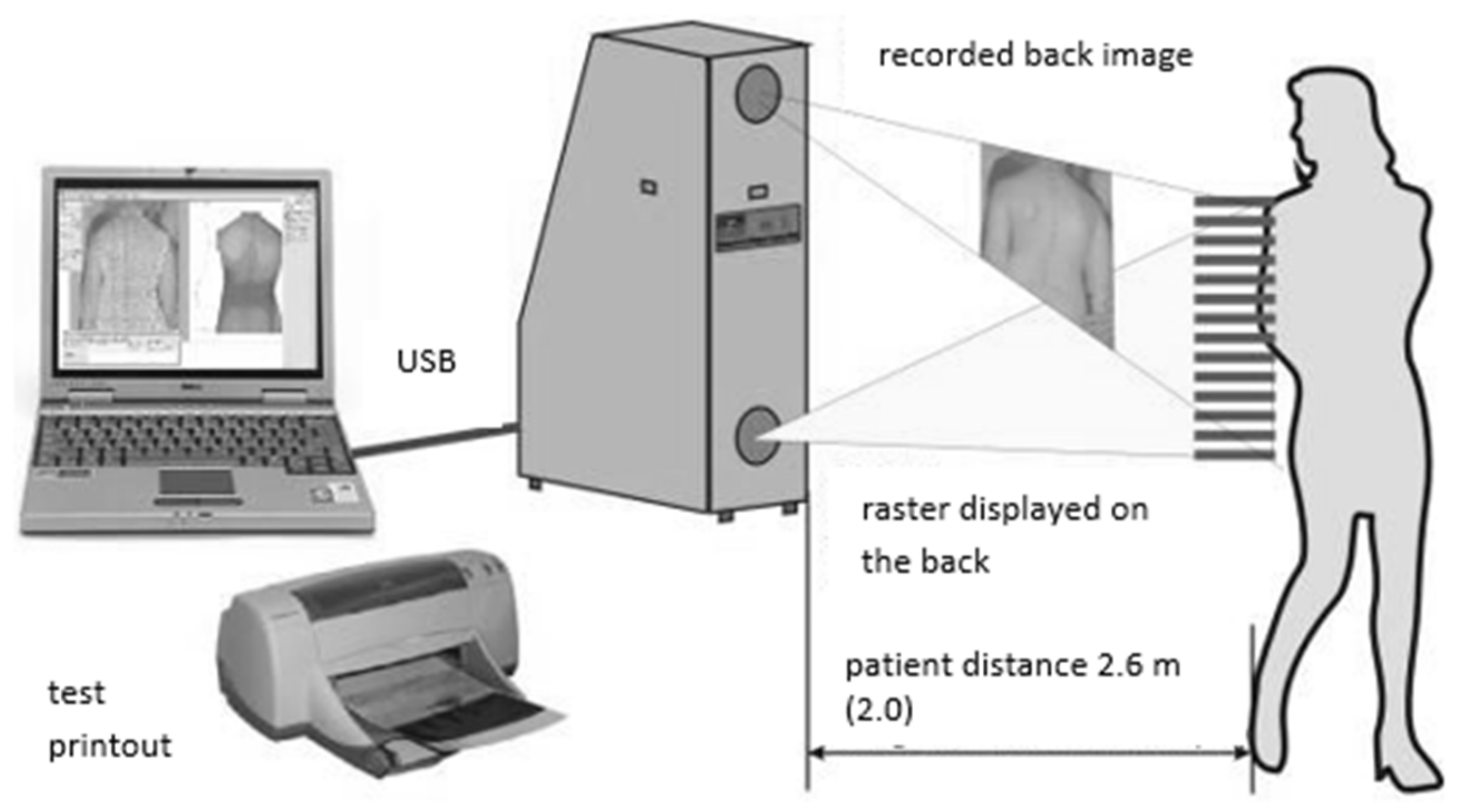
- Physical examination in which the shape of the ridge surface was analysed with the use of the photogrammetric method and the moiré effect projection (Device for Computer Posture Assessment of the Body of the 4th Generation MOIRE system, Wrocław, Poland) (Figure 1).
- 4.
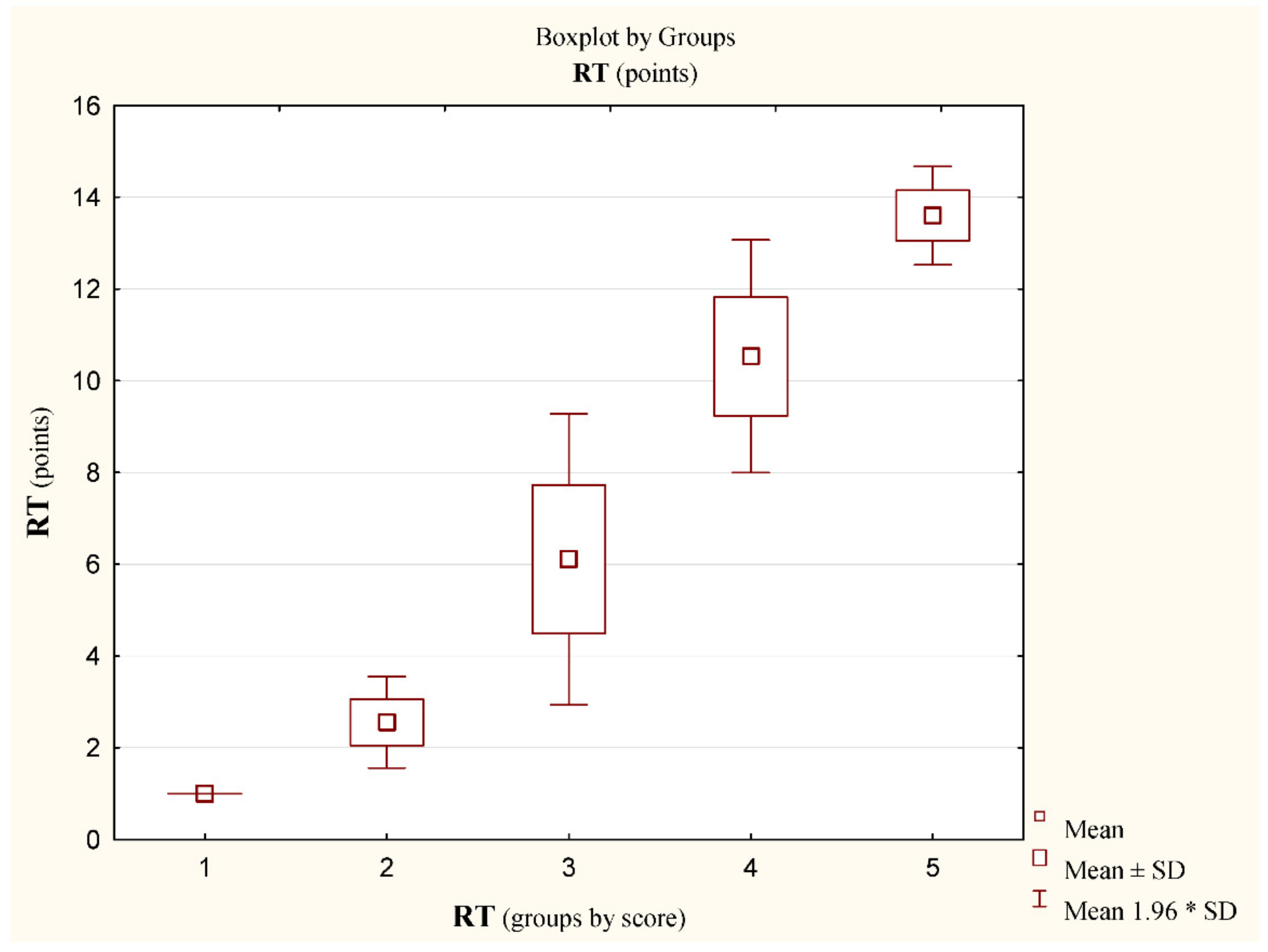
- Assessment of body balance disturbance tolerance skills (BBDTS).
2.1. Outcome Measures
2.2. Intervention
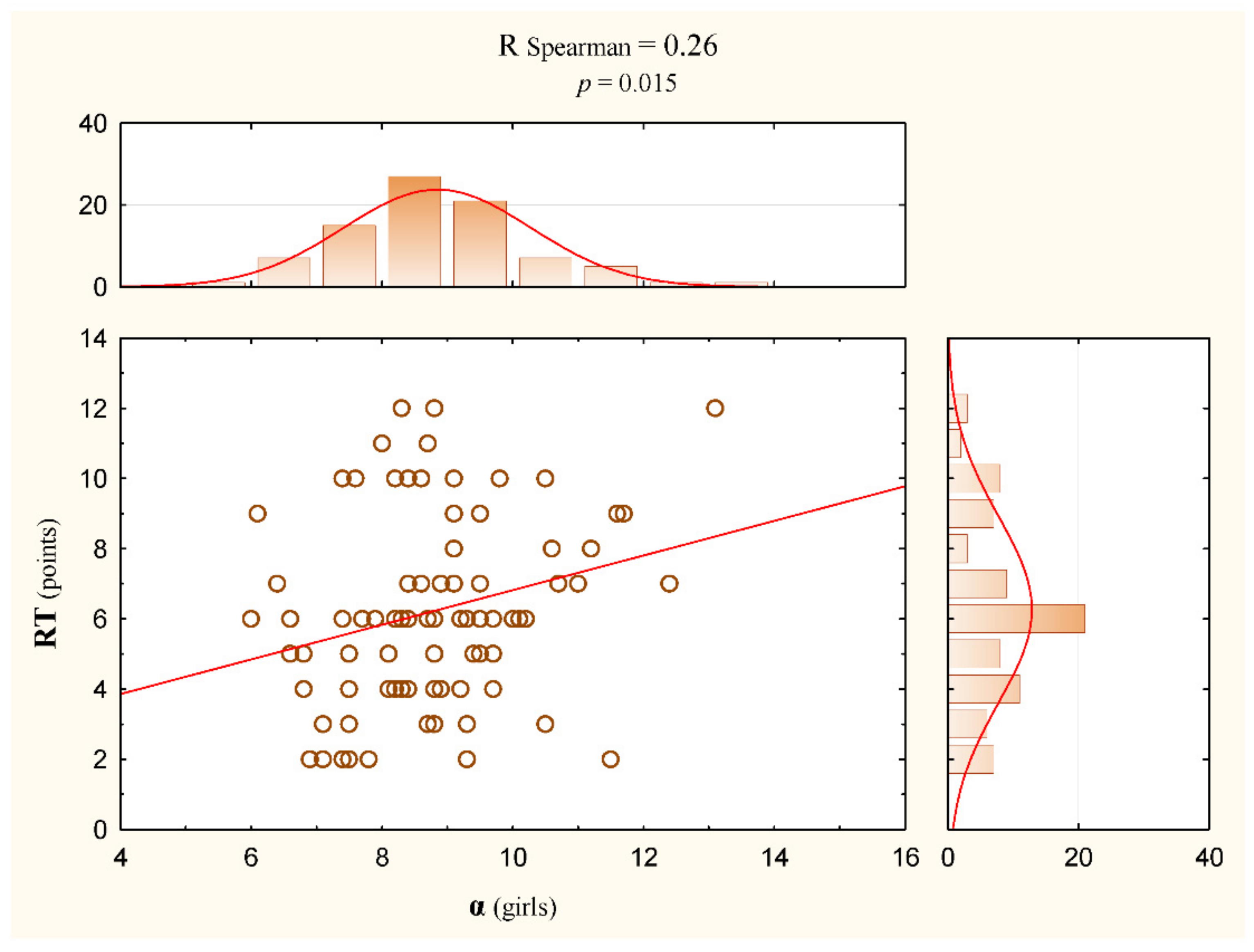
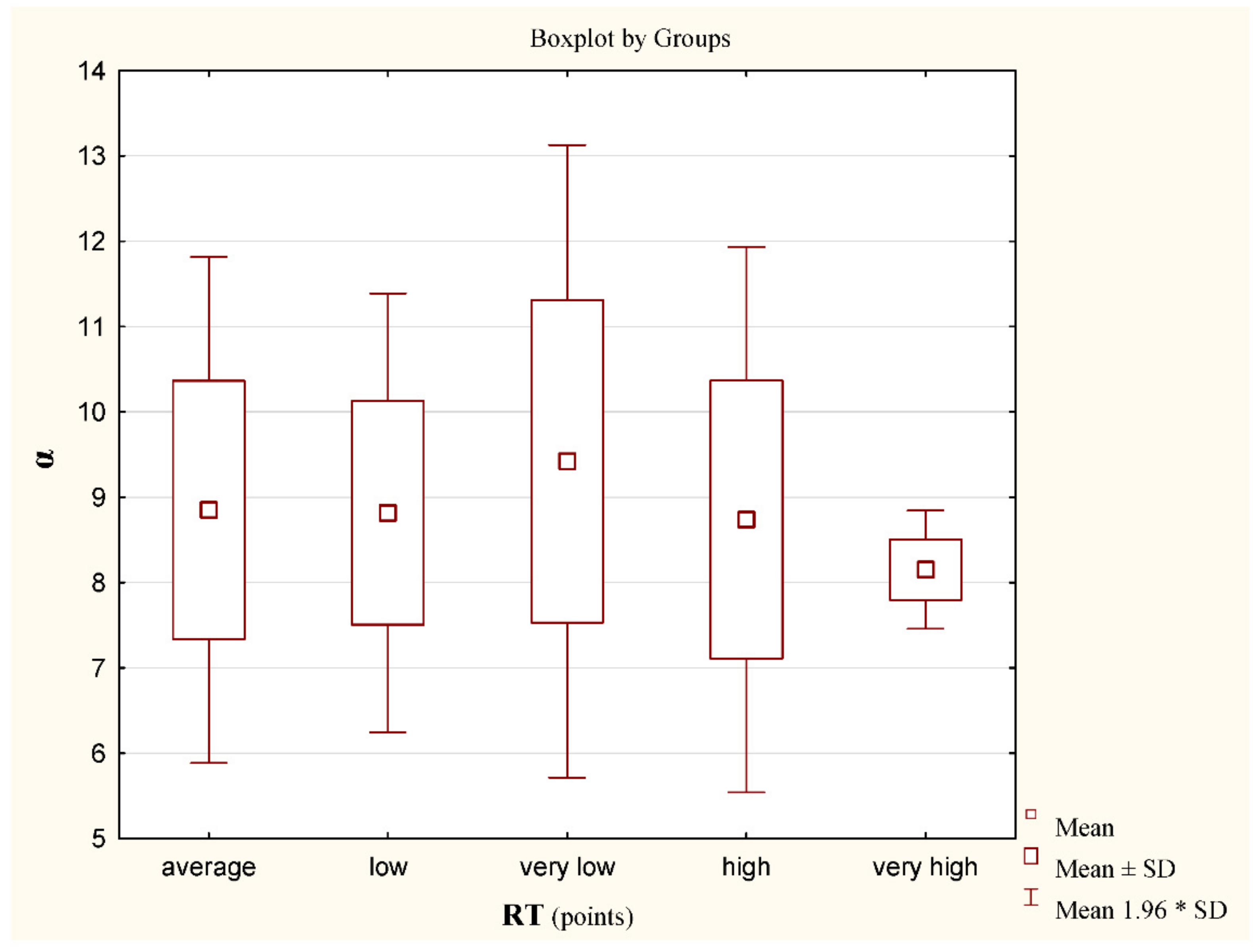
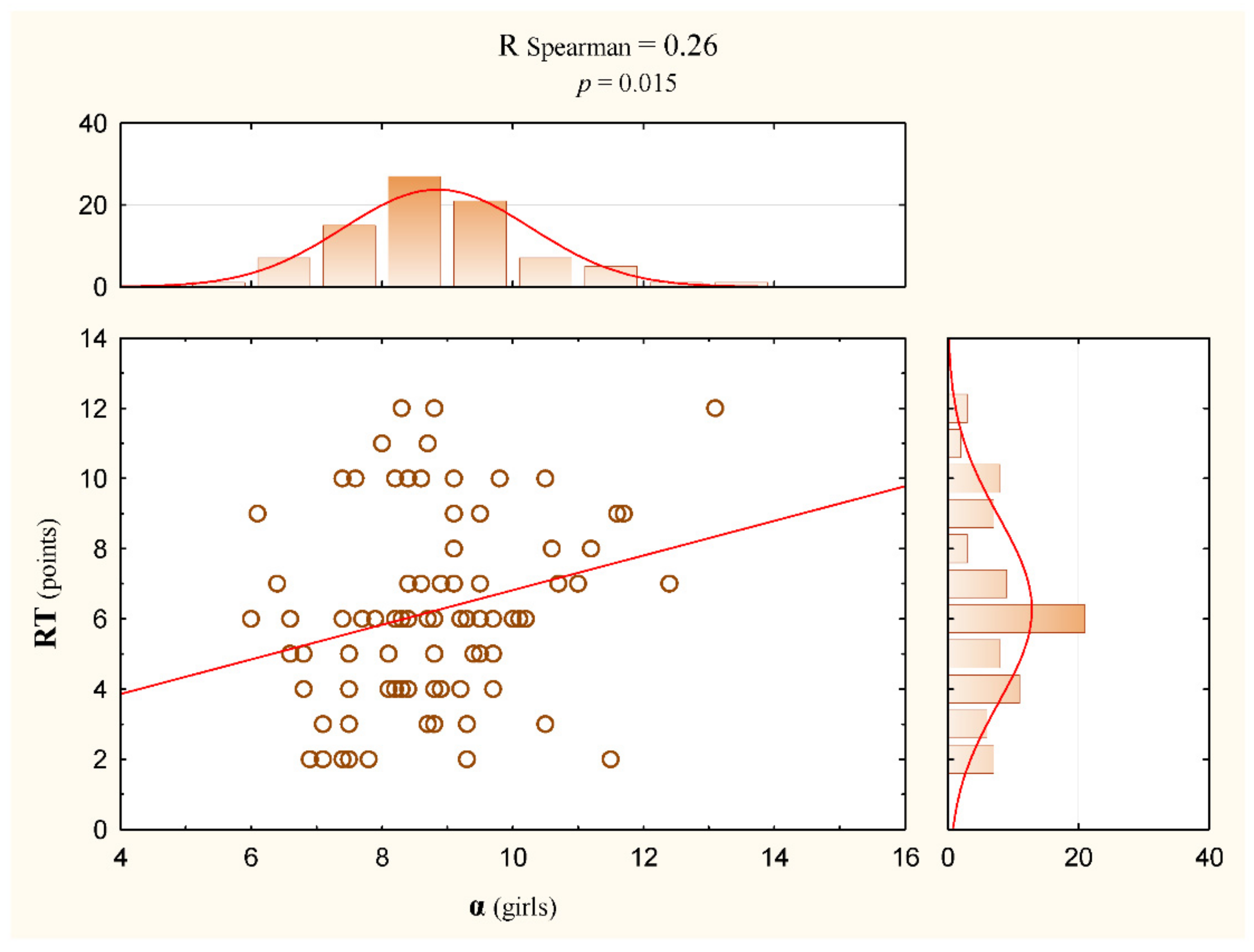
- ALPHA angle [α]—the inclination of the lumbosacral segment. This is the angle between the vertical line and the line between S1 (the spinous process of the first sacral vertebra) and the LL (apex of lumbar lordosis).
- BETA angle [β]—the inclination of the thoracic-lumbar segment. This is the angle between the vertical line and the line between LL (apex of lumbar lordosis) and KP (apex of thoracic kyphosis).
- GAMMA angle [γ]—the slope of the upper thoracic segment. This is the angle between the vertical line and the inclusive line KP (apex of thoracic kyphosis) and C7 (the spinous process of the seventh cervical vertebra).
2.3. Statistical Analysis
3. Results
4. Discussion
Study Limitation
5. Conclusions
- Increasing lumbar lordosis results in the deterioration of body balance disturbance tolerance skills.
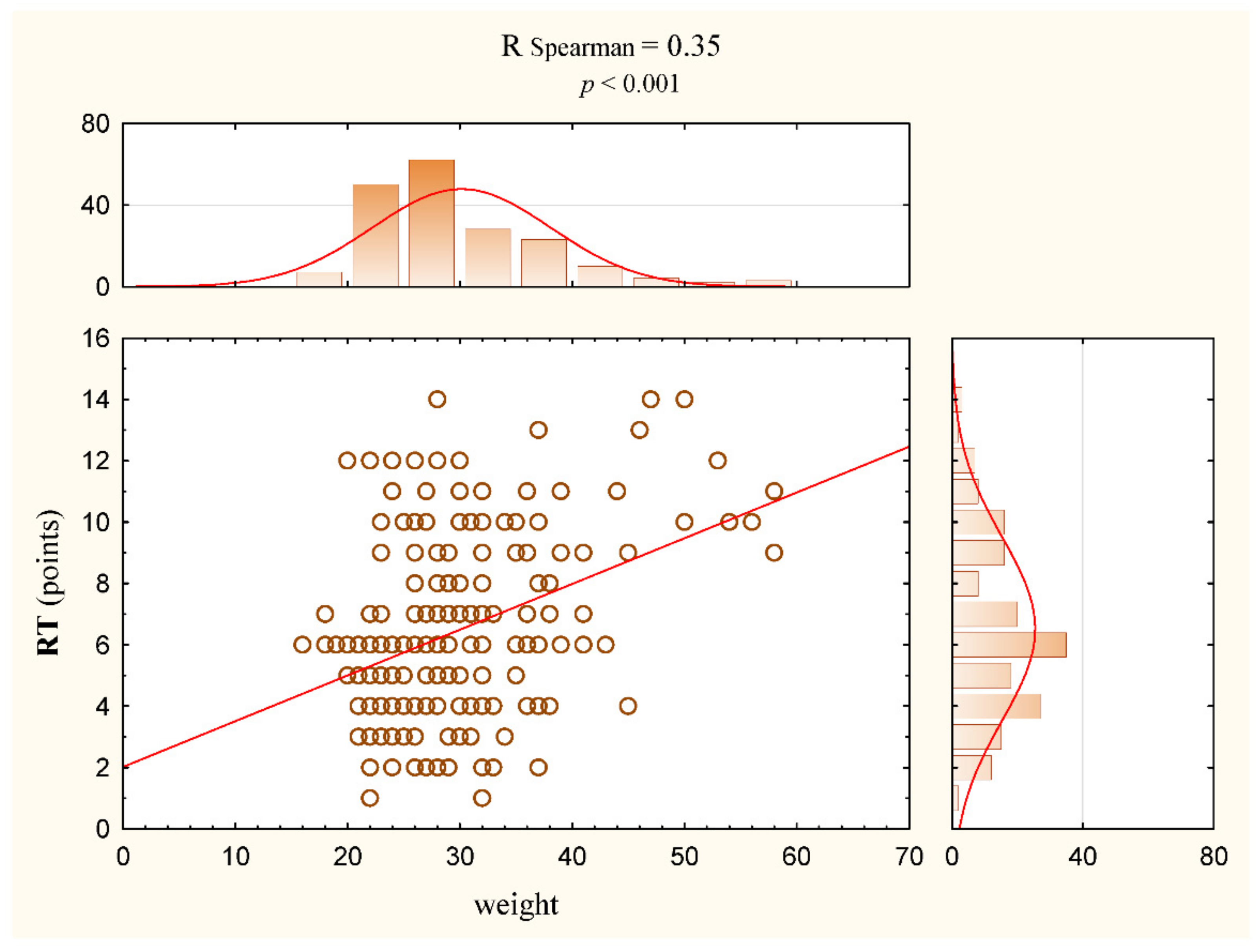
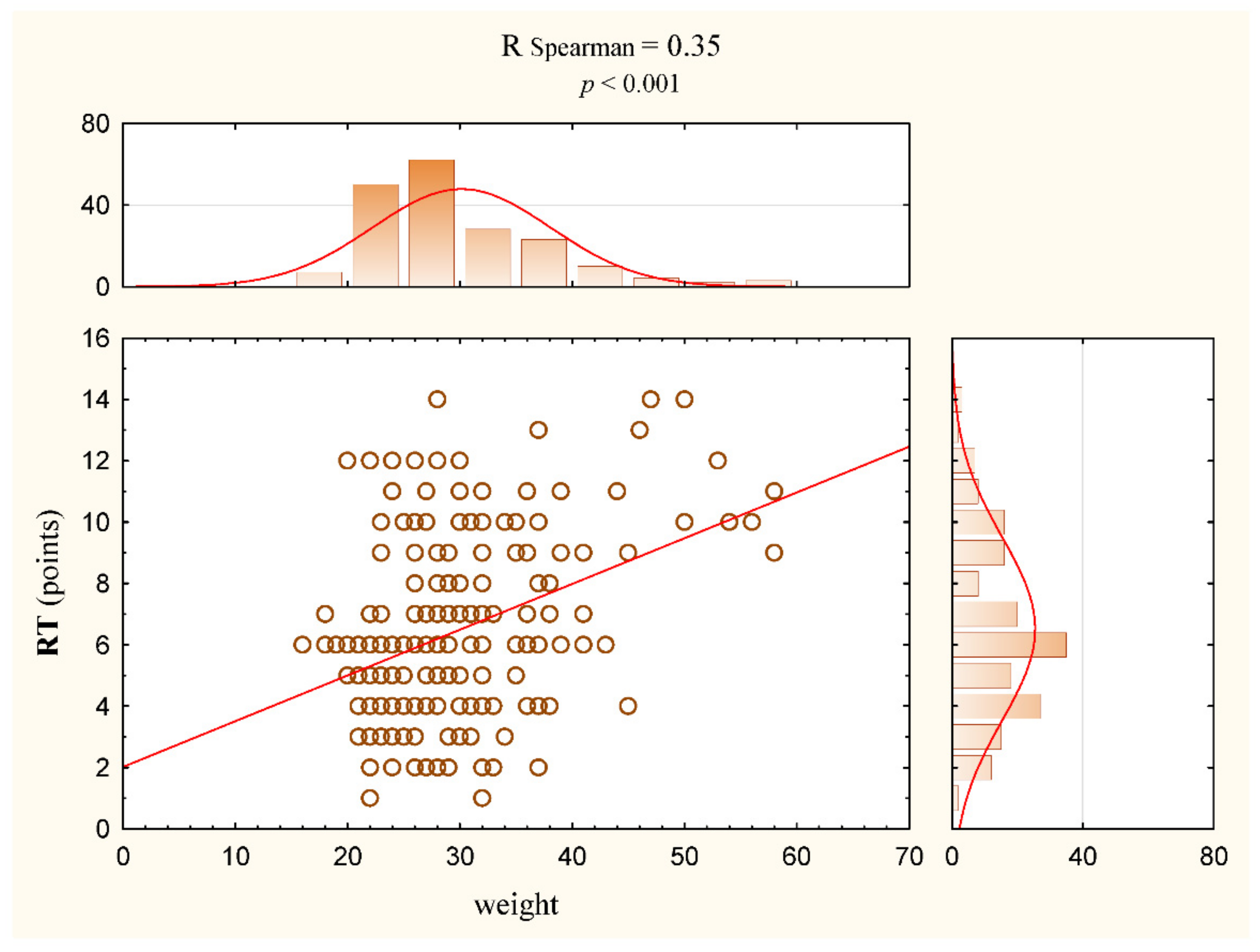
- As body weight increases, body balance disturbance tolerance skills decrease.
- As body weight increases, there is a risk of changes in the anteroposterior curvature of the spine.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yang, L.; Lu, X.; Yan, B.; Huang, Y. Prevalence of Incorrect Posture among Children and Adolescents: Finding from a Large Population-Based Study in China. Iscience 2020, 23, 101043. [Google Scholar] [CrossRef] [PubMed]
- Dalise, S.; Azzollini, V.; Chisari, C. Brain and Muscle: How Central Nervous System Disorders Can Modify the Skeletal Muscle. Diagnostics 2020, 10, 1047. [Google Scholar] [CrossRef] [PubMed]
- Blakemore, S.J.; Choudhury, S. Development of the adolescent brain: Implications for executive function and social cognition. J. Child Psychol. Psychiatry 2006, 47, 296–312. [Google Scholar] [CrossRef] [PubMed]
- Walaszek, R.; Chwała, W.; Walaszek, K.; Burdacki, M. The assessment of the relationships between body posture indices and the Y-Balance Test results in the adolescents. Acta Bioeng. Biomech. 2018, 20, 149–157. [Google Scholar] [PubMed]
- Nowotny, J. The Sense of Positioning and the Body Posture of Children and Adolescents; AWF Publishing: Katowice, Poland, 1986; pp. 34–54. [Google Scholar]
- Ostrowska, B.; Skolimowski, T. Assessment of standing balance in children with lateral idiopathic curvature of the spine. In Spine Dysfunctions Diagnostics and Therapy; Nowotny, J., Ed.; AWF Publishing: Katowice, Poland, 1993. [Google Scholar]
- Janssen, M.M.; Kouwenhoven, J.W.; Schlösser, T.; Viergever, M.A.; Bartels, L.W.; Castelein, R.M.; Vincken, K.L. Analysis of preexistent vertebral rotation in the normal infantile, juvenile, and adolescent spine. Spine 2011, 36, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Levangie, P.K.; Norkin, C.C. Joint Structure and Function: A Comprehensive Analysis; F.A. Davis Company: Philadelphia, PA, USA, 2005. [Google Scholar]
- Claus, A.; Hides, J.A.; Moseley, G.L.; Hodges, P.W. Different ways to balance the spine: Subtle changes in sagittal spinal curves affect regional muscle activity. Spine 2009, 34, 208–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Sullivan, P.B.; Grahamslaw, K.M.; Kendell, M.; Lapenskie, S.C.; Möller, N.E.; Richards, K.V. The effect of different standing and sitting postures on trunk muscle activity in a pain-free population. Spine 2002, 27, 1238–1244. [Google Scholar] [CrossRef] [PubMed]
- Dolphens, M.; Cagnie, B.; Coorevits, P. Sagittal standing posture and its association with spinal pain: A school-based epidemiological study of 1196 Flemish adolescents before age at peak height velocity. Spine 2012, 37, 1657–1666. [Google Scholar] [CrossRef] [PubMed]
- Kratenova, J.; Zejglicova, K.; Maly, M.; Filipova, V. Prevalence and risk factors of poor posture in school children in the Czech Republic. J. Sch. Health 2007, 77, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Wirth, B.; Knecht, C.; Humphreys, K. Spine Day 2012: Spinal pain in Swiss school children—Epidemiology and risk factors. BMC Pediatr. 2013, 13, 159. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H. Effects of forward head posture on static and dynamic balance control. J. Phys. Ther. Sci. 2016, 28, 274–277. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Available online: http://www.cq.com.pl/mora4g.html (accessed on 17 November 2021).
- Kalina, R.M.; Jagiełło, W.; Gliniecka, W. Assessment of the equilibrium level of athletes practicing vaulting. In Selected Issues of Sports Biomechanics; Urbanik, C., Ed.; AWF: Warsaw, Poland, 2001. [Google Scholar]
- Kalina, R.M.; Jagiełło, W.; Barczyński, B. The method to evaluate the body balance disturbation tolerance skills—Validation procedure of the ‘Rotational Test’. Arch. Budo 2013, 9, 59–80. [Google Scholar] [CrossRef]
- Lipowicz, A.; Szurmik, T.; Bugdol, M.N.; Graja, K.; Kurzeja, P.; Mitas, A.W. Relationship between Body Sway and Body Building in Girls and Boys in Developmental Age. In Information Technology in Biomedicine, Proceedings of the International Conference, ITIB 2019, Kamień Śląski, Poland, 18–20 June 2019; Piętka, E., Badura, P., Kawa, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2019; Volume 1011, p. 653. [Google Scholar]
- Ludwig, O.; Kelm, J.; Hammes, A.; Schmitt, E.; Fröhlich, M. Neuromuscular performance of balance and posture control in childhood and adolescence. Heliyon 2020, 6, e04541. [Google Scholar] [CrossRef]
- Reeves, N.P.; Narendra, K.S.; Cholewicki, J. Spine stability: The six blind men and the elephant. Clin. Biomech. 2007, 22, 266–274. [Google Scholar] [CrossRef] [Green Version]
- Ivanenko, Y.; Gurfinkel, V.S. Human Postural Control. Front. Neurosci. 2018, 12, 171. [Google Scholar] [CrossRef]
- Sherrington, C.S. Postural activity of muscle and nerve. Brain 1915, 38, 191–234. [Google Scholar] [CrossRef]
- Nourbakhsh, M.R.; Arab, A.M. Relationship between mechanical factors and incidence of low back pain. J. Orthop. Sports Phys. Ther. 2002, 32, 447–460. [Google Scholar] [CrossRef]
- Buchtelová, E.; Tichy, M.; Vaniková, K. Influence of muscular imbalances on pelvic position and lumbar lordosis: A theoretical basis. J. Nurs. Soc. Stud. Public Health Rehabil. 2013, 1, 25–36. [Google Scholar]
- Alvim, F.C.; Peixoto, J.G.; Vicente, E.J.; Chagas, P.S.; Fonseca, D.S. Influences of the extensor portion of the gluteus maximus muscle on pelvic tilt before and after the performance of a fatigue protocol. Rev. Bras. Fisioter. 2010, 14, 206–213. [Google Scholar] [CrossRef] [Green Version]
- Behm, D.G.; Muehlbauer, T.; Kibele, A.; Granacher, U. Effects of strength training using unstable surfaces on strength, power and balance performance across the lifespan: A systematic review and meta-analysis. Sports Med. 2015, 45, 1645–1669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barczyk-Pawelec, K.; Piechura, J.R.; Dziubek, W.; Rozek, K. Evaluation of isokinetic trunk muscle strength in adolescents with normal and abnormal postures. J. Manip. Physiol. Ther. 2015, 38, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Karaleić, S.; Milenković, V.; Savić, Z. The influence of Physical Education curriculum on the correction of bad body posture and changes of motor status in adolescence period of schoolgirls. Act. Phys. Educ. Sport 2014, 4, 92–94. [Google Scholar]
- Maurer, C.; Peterka, R.J. A new interpretation of spontaneous sway measures based on a simple model of human postural control. J. Neurophysiol. 2005, 93, 189–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winter, D.A.; Patla, A.E.; Frank, J.S. Assessment of balance control in humans. Med. Prog. Technol. 1990, 16, 31–51. [Google Scholar] [PubMed]
- Massion, J. Movement, posture and equilibrium: Interaction and coordination. Prog. Neurobiol. 1992, 38, 35–56. [Google Scholar] [CrossRef]
- Feldman, A.G.; Ilmane, N.; Sangani, S.; Raptis, H. Motor control and position sense: Action-perception coupling. Adv. Exp. Med. Biol. 2014, 826, 17–31. [Google Scholar] [PubMed]
- Sousa, A.S.; Silva, A.; Tavares, J.M. Biomechanical and neurophysiological mechanisms related to postural control and efficiency of movement: A review. Somatosens. Mot. Res. 2012, 29, 131–143. [Google Scholar] [CrossRef] [PubMed]
- Drzal-Grabiec, J.; Rachwal, M.; Podgorska-Bednarz, J.; Rykala, J.; Snela, S.; Truszczynska, A.; Trzaskoma, Z. The effect of spinal curvature on the photogrammetric assessment on static balance in elderly women. BMC Musculoskelet. Disord. 2014, 15, 186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, A.; Silva, D.; Kasuki, L.; Gadelha, M.R.; Camilo, G.B.; Guimarães, F.S. Posture and balance control in patients with acromegaly: Results of a cross-sectional study. Gait Posture 2014, 40, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Willigenburg, N.W.; Kingma, I.; Van Dieën, J.H. Center of pressure trajectories, trunk kinematics and trunk muscle activation during unstable sitting in low back pain patients. Gait Posture 2013, 38, 625–630. [Google Scholar] [CrossRef] [Green Version]
- Nault, M.L.; Allard, P.; Hinse, S.; Le Blanc, R.; Caron, O.; Labelle, H.; Sadeghi, H. Relations between standing stability and body posture parameters in adolescent idiopathic scoliosis. Spine 2002, 27, 1911–1917. [Google Scholar] [CrossRef]
- Stylianides, G.; Dalleau, G.; Begon, M.; Rivard, C.H.; Allard, P. Pelvic morphology, body posture and standing balance characteristics of adolescent able-bodied and idiopathic scoliosis girls. PLoS ONE 2013, 8, e70205. [Google Scholar] [CrossRef]
- Nagymáté, G.; Takács, M.; Kiss, R.M. Does bad posture affect the standing balance? Cogent Med. 2018, 5, 1503778. [Google Scholar] [CrossRef]
- Mrozkowiak, M. Determinants of Selected Parameters Posture of Children and Young People and Their Variability in the Light of the Projection Chamber; Gorzów Wielkopolski AWF: Poznań, Poland, 2010. [Google Scholar]
- Lomas-Vega, R.; Garrido-Jaut, M.V.; Rus, A.; Del-Pino-Casado, R. Effectiveness of Global Postural Re-education for Treatment of Spinal Disorders: A Meta-analysis. Am. J. Phys. Med. Rehabil. 2017, 96, 124–130. [Google Scholar] [CrossRef]
- Lozano-Quijada, C.; Poveda-Pagán, E.J.; Segura-Heras, J.V.; Hernández-Sánchez, S.; Prieto-Castelló, M.J. Changes in Postural Sway After a Single Global Postural Reeducation Session in University Students: A Randomized Controlled Trial. J. Manip. Physiol. Ther. 2017, 40, 467–476. [Google Scholar] [CrossRef]
- De Lima, E.S.; Resende, F.; Vanti, C.; Banchelli, F.; Trani Brandao, J.G.; Amorim, J.B.O.; Villafañe, J.H.; Pillastrini, P. The effect of Global Postural Reeducation on body weight distribution in sitting posture and on musculoskeletal pain. A pilot study. Med. Lav. 2017, 108, 187–196. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All n = 189 x ± SD; M (Min/Max) | Girls n = 85 x ± SD; M (Min/Max) | Boys n = 104 x ± SD; M (Min/Max) |
|---|---|---|---|
| Age (years) | 8.3 ± 0.7; 8.3 (7/9.8) | 8.3 ± 0.7; 8.2 (7/9.8) | 8.3 ± 0.7; 8.3 (7/9.8) |
| Height (cm) | 131.3 ± 7.4; 131 (115/150) | 130.3 ± 7.0; 130 (115/146) | 132.1 ± 7.6; 133 (115/150) |
| Body weight (kg) | 30.0 ± 7.9; 28.0 (16/58) | 29.7 ± 7.9; 28.0 (16/58) | 30.3 ± 7.9; 28.0 (18/58) |
| Variable [°] | All n = 189 x ± SD; M | Girls n = 85 x ± SD; M | Boys n = 104 x ± SD; M |
|---|---|---|---|
| α | 8.8 ± 1.5; 8.8 | 8.8 ± 1.4;8.8 | 8.8 ± 1.6; 8.9 |
| β | 7.9 ± 1.2; 8.0 | 8.0 ± 1.2; 7.9 | 7.8 ± 1.1; 8.0 |
| γ | 10.4 ± 1.5; 10.4 | 10.2 ± 1.6; 10.4 | 10.6 ± 1.3; 10.5 |
| α + β | 16.7 ± 1.8; 16.6 | 16.8 ± 1.7; 16.6 | 16.7 ± 1.9; 16.7 |
| β + γ | 18.3 ± 2.1; 18.3 | 18.3 ± 2.3; 18.3 | 18.4 ± 1.9; 18.3 |
| α + β + γ | 27.2 ± 2.4; 27.0 | 27.1 ± 2.4; 26.8 | 27.2 ± 2.4; 27.1 |
| RT | All n = 189 | Girls n = 85 | Boys n = 104 |
|---|---|---|---|
| x ± SD (pts) | 6.5 ± 2.9 | 6.2 ± 2.6 | 6.7 ± 3.2 |
| M (pts) | 6.0 | 6.0 | 6.0 |
| (min/max) | 1/14 | 2/12 | 1/14 |
| Variable | Rs | p |
|---|---|---|
| Age/RT | −0.13 | 0.07 |
| Weight/RT | 0.35 | <0.001 |
| Height/RT | 0.08 | 0.3 |
| α/RT | 0.15 | 0.04 |
| β/RT | −0.08 | 0.3 |
| γ/RT | −0.09 | 0.2 |
| α + β/RT | 0.07 | 0.4 |
| β + γ/RT | −0.10 | 0.15 |
| α + β + γ/RT | −0.02 | 0.7 |
| α/Weight | 0.30 | <0.001 |
| Variable | Rs | p |
|---|---|---|
| Age/RT | −0.16 | 0.14 |
| Weight/RT | 0.32 | 0.0032 |
| α/RT | 0.26 | 0.015 |
| β + γ/RT | −0.13 | 0.2 |
| Variable | Rs | p |
|---|---|---|
| Age/RT | −0.12 | 0.2 |
| Weight/RT | 0.37 | <0.001 |
| α/RT | 0.06 | 0.5 |
| β + γ/RT | −0.09 | 0.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurzeja, P.; Gąsienica-Walczak, B.; Ogrodzka-Ciechanowicz, K.; Prusak, J. Analysis of the Ability to Tolerate Body Balance Disturbance in Relation to Selected Changes in the Sagittal Plane of the Spine in Early School-Age Children. J. Clin. Med. 2022, 11, 1653. https://doi.org/10.3390/jcm11061653
Kurzeja P, Gąsienica-Walczak B, Ogrodzka-Ciechanowicz K, Prusak J. Analysis of the Ability to Tolerate Body Balance Disturbance in Relation to Selected Changes in the Sagittal Plane of the Spine in Early School-Age Children. Journal of Clinical Medicine. 2022; 11(6):1653. https://doi.org/10.3390/jcm11061653
Chicago/Turabian StyleKurzeja, Piotr, Bartłomiej Gąsienica-Walczak, Katarzyna Ogrodzka-Ciechanowicz, and Jarosław Prusak. 2022. "Analysis of the Ability to Tolerate Body Balance Disturbance in Relation to Selected Changes in the Sagittal Plane of the Spine in Early School-Age Children" Journal of Clinical Medicine 11, no. 6: 1653. https://doi.org/10.3390/jcm11061653
APA StyleKurzeja, P., Gąsienica-Walczak, B., Ogrodzka-Ciechanowicz, K., & Prusak, J. (2022). Analysis of the Ability to Tolerate Body Balance Disturbance in Relation to Selected Changes in the Sagittal Plane of the Spine in Early School-Age Children. Journal of Clinical Medicine, 11(6), 1653. https://doi.org/10.3390/jcm11061653