
A Comparative Study of the Efficacy of an Intervention with a Nutritional Supplement for Patients with Chronic Kidney Disease: A Randomized Trial

 ,
,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
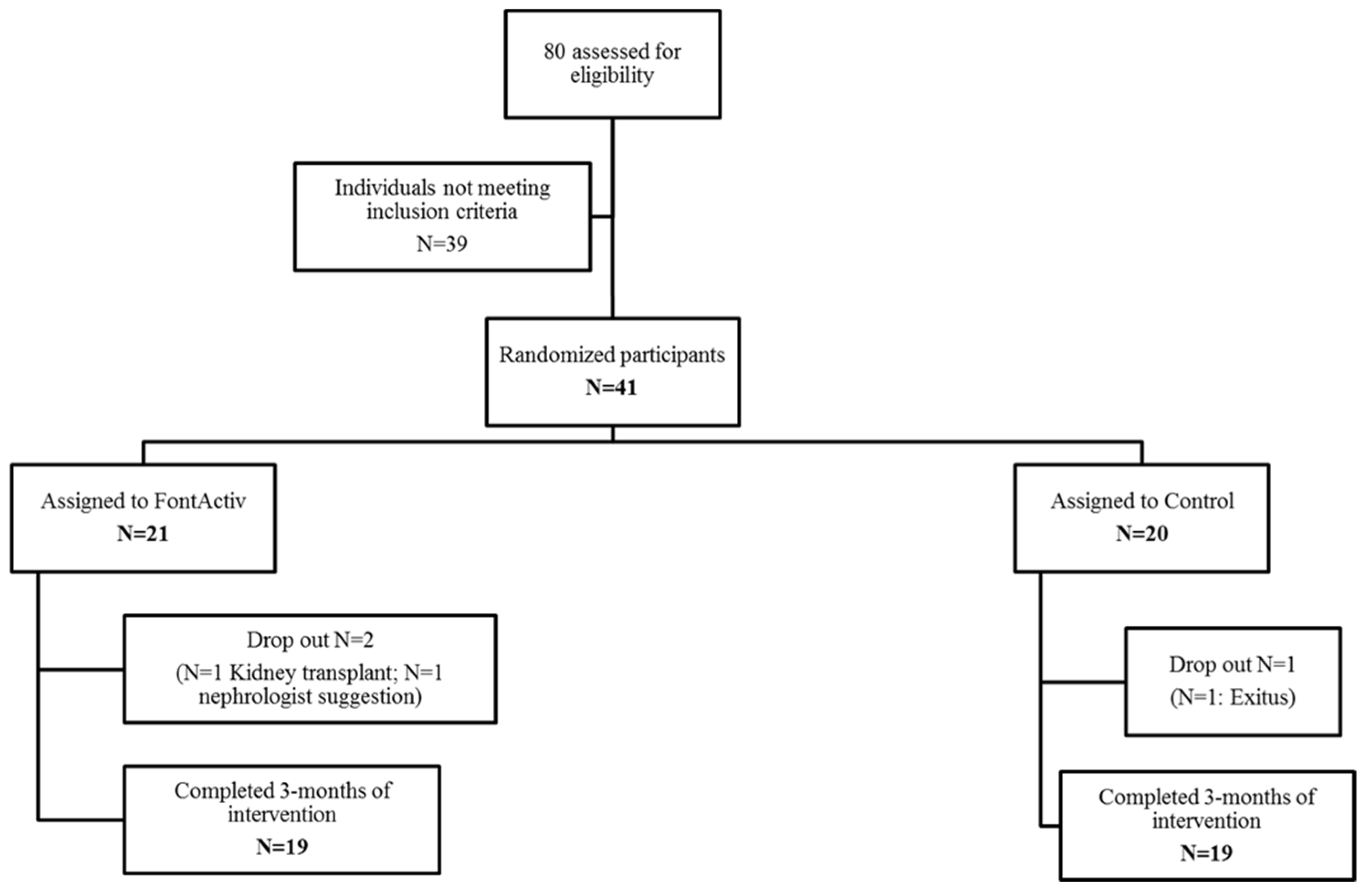
2.1. Study Design
2.2. Study Participants
2.3. Product to Test
2.4. Intervention, Physical Activity, and Clinical Measurements
2.5. Ethics Statement
2.6. Laboratory Measurements
2.7. Statistical Analysis
3. Results
3.1. Tolerance of the Dietary Supplement
3.2. Food, Energy Balance, and Dietary Adherence
3.3. Anthropometric Measurements
3.4. Biochemical Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Salas-Salvadó, J.; I Sanjaume, A.B.; Casañas, R.T.; I Solà, M.E.S.; Peláez, R.B. Nutrición y Dietética Clínica, 4th ed.; Elesvier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Kim, S.M.; Kang, B.C.; Kim, H.J.; Kyung, M.S.; Oh, H.J.; Kim, J.H.; Kwon, O.; Ryu, D.R. Comparison of hemodialysis and peritoneal dialysis patients’ dietary behaviors. BMC Nephrol. 2020, 21, 91. [Google Scholar] [CrossRef] [PubMed]
- Jha, V.; Garcia-Garcia, G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.M.; Yang, C.W. Chronic kidney disease: Global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Mills, K.T.; Xu, Y.; Zhang, W.; Bundy, J.D.; Chen, C.S.; Kelly, T.N.; Chen, J.; He, J. A systematic analysis of worldwide population-based data on the global burden of chronic kidney disease in 2010. Kidney Int. 2015, 88, 950–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorostidi, M.; Sánchez-Martínez, M.; Ruilope, L.M.; Graciani, A.; de la Cruz, J.J.; Santamaría, R.; del Pino, M.D.; Guallar-Castillón, P.; de Álvaro, F.; Rodríguez-Artalejo, F.; et al. Chronic kidney disease in Spain: Prevalence and impact of accumulation of cardiovascular risk factors. Nefrologia 2018, 38, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Naylor, H.L.; Jackson, H.; Walker, G.H.; Macafee, S.; Magee, K.; Hooper, L.; Stewart, L.; Maclaughlin, H.L. British dietetic association evidence-based guidelines for the protein requirements of adults undergoing maintenance haemodialysis or peritoneal dialysis. J. Hum. Nutr. Diet. 2013, 26, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Fiaccadori, E.; Sabatino, A.; Barazzoni, R.; Carrero, J.J.; Cupisti, A.; De Waele, E.; Jonckheer, J.; Singer, P.; Cuerda, C. ESPEN Guideline ESPEN guideline on clinical nutrition in hospitalized patients with acute or chronic kidney disease. Clin. Nutr. 2021, 40, 1644–1668. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.-J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Oquendo, L.G.; Asencio, J.M.M.; de las Nieves, C.B. Contributing factors for therapeutic diet adherence in patients receiving haemodialysis treatment: An integrative review. J. Clin. Nurs. 2017, 26, 3893–3905. [Google Scholar] [CrossRef]
- Sabatino, A.; Piotti, G.; Cosola, C.; Gandolfini, I.; Kooman, J.P.; Fiaccadori, E. Dietary protein and nutritional supplements in conventional hemodialysis. Semin. Dial. 2018, 31, 583–591. [Google Scholar] [CrossRef]
- Ikizler, T.A. Optimal Nutrition in Hemodialysis Patients. Adv. Chronic Kidney Dis. 2013, 20, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Huarte-Loza, E.; Barril-Cuadrado, G.; Cebollada-Muro, J.; Cerezo-Morales, S.; Coronel-Díaz, F.; Doñate-Cubells, T.; Fernández-Giraldez, E.; Izaguirre-Boneta, A.; Lanuza-Luengo, M.; Liébana-Cañada, A.; et al. Nutrición en pacientes en diálisis. Consenso SEDYT. Dial. Traspl. 2006, 27, 138–161. [Google Scholar]
- Juton, C.; Castro-Barquero, S.; Casas, R.; Freitas, T.; Ruiz-León, A.M.; Crovetto, F.; Domenech, M.; Crispi, F.; Vieta, E.; Gratacós, E.; et al. Reliability and Concurrent and Construct Validity of a Food Frequency Questionnaire for Pregnant Women at High Risk to Develop Fetal Growth Restriction. Nutrients 2021, 13, 1629. [Google Scholar] [CrossRef] [PubMed]
- Elosua, R.; Marrugat, J.; Molina, L.; Pons, S.; Pujol, E. Validation of the minnesota leisure time physical activity questionnaire in Spanish men. Am. J. Epidemiol. 1994, 139, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; McKenzie, J.; De Mutsert, R.; Azar, R.; Teta, D.; Plauth, M.; Cano, N.; Fouque, D.; Cano, N.; Plauth, M.; et al. Use of a renal-specific oral supplement by haemodialysis patients with low protein intake does not increase the need for phosphate binders and may prevent a decline in nutritional status and quality of life. Nephrol. Dial. Transplant. 2008, 23, 2902–2910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al de Francisco, M.; Aguilera, L.; Fuster, V. Enfermedad cardiovascular, enfermedad renal y otras enfermedades crónicas. Es necesaria una intervención más temprana en la enfermedad renal crónica. Nefrologia 2009, 29, 6–9. [Google Scholar]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.L.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Kim, Y.; Evangelista, L.S.; Phillips, L.R.; Pavlish, C.; Kopple, J.D. The End-Stage Renal Disease Adherence Questionnaire (ESRD-AQ): Testing the psychometric properties in patients receiving in-center hemodialysis. Nephrol. Nurs. J. 2010, 37, 377–393. [Google Scholar]
- García-Llana, H.; Remor, E.; Selgas, R. Adhesión al tratamiento, estado emocional y calidad de vida en pacientes con insuficiencia renal crónica en tratamiento con diálisis. Psicothema 2013, 25, 79–86. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Ikizler, T.A. Let Them Eat During Dialysis: An Overlooked Opportunity to Improve Outcomes in Maintenance Hemodialysis Patients. J. Ren. Nutr. 2013, 23, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.J.; Ma, F.; Wang, Q.Y.; He, S.L. The effects of oral nutritional supplements in patients with maintenance dialysis therapy: A systematic review and meta-analysis of randomized clinical trials. PLoS ONE 2018, 13, e0203706. [Google Scholar] [CrossRef] [Green Version]
- Riobó Serván, P.; Ortiz Arduan, A. Eficacia de la suplementación oral intradiálisis en pacientes con insuficiencia renal crónica. Endocrinol. Nutr. 2011, 58, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P.; Gillespie, I.A.; Tunks, J.; Addison, J.; Kronenberg, F.; Drueke, T.B.; Marcelli, D.; Schernthaner, G.; Eckardt, K.U.; Floege, J.; et al. Inflammation modifies the paradoxical association between body mass index and mortality in hemodialysis patients. J. Am. Soc. Nephrol. 2016, 27, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Cano, N.; Fiaccadori, E.; Tesinsky, P.; Toigo, G.; Druml, W.; Kuhlmann, M.; Mann, H.; Hörl, W.H. ESPEN Guidelines on Enteral Nutrition: Adult Renal Failure. Clin. Nutr. 2006, 25, 295–310. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Cano, N.J.; Budde, K.; Chazot, C.; Kovesdy, C.P.; Mak, R.H.; Mehrotra, R.; Raj, D.S.; Sehgal, A.R.; Stenvinkel, P.; et al. Diets and enteral supplements for improving outcomes in chronic kidney disease. Nat. Rev. Nephrol. 2011, 7, 369–384. [Google Scholar] [CrossRef]
- Obi, Y.; Mikami, S.; Hamano, T.; Obi, Y.; Tanaka, H.; Shimomura, A.; Rakugi, H.; Inoue, T.; Isaka, Y. Intravenous Vitamin B6 Increases Resistance to Erythropoiesis-Stimulating Agents in Hemodialysis Patients: A Randomized Controlled Trial. J. Ren. Nutr. 2016, 26, 380–390. [Google Scholar] [CrossRef]
- Liakopoulos, V.; Roumeliotis, S.; Bozikas, A.; Eleftheriadis, T.; Dounousi, E. Antioxidant supplementation in renal replacement therapy patients: Is there evidence? Oxid. Med. Cell. Longev. 2019, 2019, 9109473. [Google Scholar] [CrossRef] [Green Version]
- Zachara, B.A.; Gromadzinska, J.; Zbrog, Z.; Swiech, R.; Wasowicz, W.; Twardowska, E.; Jablonska, E.; Sobala, W. Selenium supplementation to chronic kidney disease patients on hemodialysis does not induce the synthesis of plasma glutathione peroxidase. Acta Biochim. Pol. 2009, 56, 183–187. [Google Scholar] [CrossRef]
- Salehi, M.; Sohrabi, Z.; Ekramzadeh, M.; Fallahzadeh, M.K.; Ayatollahi, M.; Geramizadeh, B.; Hassanzadeh, J.; Sagheb, M.M. Selenium supplementation improves the nutritional status of hemodialysis patients: A randomized, double-blind, placebo-controlled trial. Nephrol. Dial. Transplant. 2013, 28, 716–723. [Google Scholar] [CrossRef] [Green Version]
- Bolasco, P. Hemodialysis—nutritional flaws in diagnosis and prescriptions. Could amino acid losses be the sharpest “sword of damocles”? Nutrients 2020, 12, 1773. [Google Scholar] [CrossRef]
- Lau, W.L.; Leaf, E.M.; Hu, M.C.; Takeno, M.; Kuro-O, M.; Moe, O.W.; Giachelli, C.M. Vitamin D receptor agonists increase klotho and osteopontin while decreasing aortic calcification in mice with chronic kidney disease fed a high phosphate diet. Kidney Int. 2012, 12, 1261–1270. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, N.; Brandsch, C.; Kühne, H.; Thiele, A.; Hirche, F.; Stangl, G.I. Vitamin D receptor deficiency and low vitamin D diet stimulate aortic calcification and osteogenic key factor expression in mice. PLoS ONE 2012, 7, e35316. [Google Scholar] [CrossRef] [PubMed]
- Ishimura, E.; Okuno, S.; Kitatani, K.; Tsuchida, T.; Yamakawa, T.; Shioi, A.; Inaba, M.; Nishizawa, Y. Significant association between the presence of peripheral vascular calcification and lower serum magnesium in hemodialysis patients. Clin. Nephrol. 2007, 68, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.L.; Lin, K.P.; Hsu, G.W.; Liu, K.L.; Guo, C.H. Altered Mineral Metabolism and Disequilibrium Between Calcification Promoters and Inhibitors in Chronic Hemodialysis Patients. Biol. Trace Elem. Res. 2020, 193, 14–22. [Google Scholar] [CrossRef]
- Liu, H.; Li, X.; Qin, F.; Huang, K. Selenium suppresses oxidative-stress-enhanced vascular smooth muscle cell calcification by inhibiting the activation of the PI3K/AKT and ERK signaling pathways and endoplasmic reticulum stress. J. Biol. Inorg. Chem. 2014, 19, 375–388. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, F.K.; Smeets, J.S.J.; van der Sande, F.M.; Kooman, J.P.; van Loon, L.J.C. Dietary protein and physical activity interventions to support muscle maintenance in end-stage renal disease patients on hemodialysis. Nutrients 2019, 11, 2972. [Google Scholar] [CrossRef] [Green Version]
- Vlaminck, H.; Maes, B.; Jacobs, A.; Reyntjens, S.; Evers, G. The dialysis diet and fluid non-adherence questionnaire: Validity testing of a self-report instrument for clinical practice. J. Clin. Nurs. 2001, 10, 707–715. [Google Scholar] [CrossRef]
- Hernández-Morante, J.J.; Sánchez-Villazala, A.; Cutillas, R.C.; Fuentes, M.C. Effectiveness of a nutrition education program for the prevention and treatment of malnutrition in end-stage renal disease. J. Ren. Nutr. 2014, 24, 42–49. [Google Scholar] [CrossRef]
- Rattanasompattikul, M.; Molnar, M.Z.; Lee, M.L.; Dukkipati, R.; Bross, R.; Jing, J.; Kim, Y.; Voss, A.C.; Benner, D.; Feroze, U.; et al. Anti-Inflammatory and Anti-Oxidative Nutrition in Hypoalbuminemic Dialysis Patients (AIONID) study: Results of the pilot-feasibility, double-blind, randomized, placebo-controlled trial. J. Cachexia Sarcopenia Muscle 2013, 4, 247–257. [Google Scholar] [CrossRef]

{kind=link}
| Control (n = 19) | FontActiv (n = 19) | p-Value | |
|---|---|---|---|
| Women, n (%) 1 | 9 (47.4) | 11 (57.9) | 0.373 |
| Age (years) | 76.2 (12.6) | 73.6 (17.3) | 0.609 |
| Peritoneal dialysis, n (%) | 4 (21.0) | 3 (15.8) | 0.676 |
| Body weight (kg) | 65.6 (10.2) | 58.3 (10.2) | 0.034 |
| BMI (kg/m2) | 25.3 (3.61) | 21.6 (21.6) | 0.004 |
| Arm circumference (cm) | 28.0 (4.55) | 24.1 (2.63) | 0.003 |
| Calf circumference (cm) | 42.3 (4.51) | 38.6 (8.11) | 0.106 |
| Triceps fold (mm) | 14.0 (5.77) | 10.8 (4.31) | 0.063 |
| MedDiet P17-score (points) | 6.05 (2.25) | 5.00 (1.70) | 0.112 |
| Prealbumin (g/L) | 0.27 (0.08) | 0.23 (0.07) | 0.095 |
| Albumin (g/L) | 37.9 (4.53) | 36.5 (4.54) | 0.340 |
| Total protein (g/L) | 61.9 (6.46) | 60.8 (7.52) | 0.614 |
| 25-hidroxi-vitamin D3 (ng/mL) | 15.7 (10.6) | 11.6 (6.75) | 0.221 |
| HDL-c (mg/dL) | 48.1 (11.0) | 56.7 (20.0) | 0.110 |
| Hemoglobin, g/L | 117.9 (11.6) | 110.7 (17.9) | 0.146 |
| Glycated hemoglobin (%) | 6.21 (1.10) | 5.35 (0.64) | 0.006 |
| Total leukocytes (109/L) | 7.14 (2.67) | 6.16 (1.50) | 0.170 |
| Hematocrit (L/L) | 0.37 (0.04) | 0.35 (0.05) | 0.242 |
| Transferrin saturation | 31.5 (15.7) | 24.1 (11.4) | 0.105 |
| Ferritin (ng/mL) | 387.6 (209.4) | 506.7 (217.7) | 0.094 |
| Control (n = 19) | FontActiv (n = 19) | |||
|---|---|---|---|---|
| Mean | Mean | p-Value between Groups | ||
| Energy (kcal/day) 1 | Baseline 1 | 2392.1 (404) | 2229.2 (454.2) | 0.256 |
| Changes after 3 m. | −164.2 (−335.8, 7.32) | −52.0 (−188.9, 84.8) 3.96) | 0.293 | |
| Carbohydrates (g/day) | Baseline | 233.6 (65.7) | 215.1 (47.1) | 0.334 |
| Changes after 3 m. | −21.5 (−47.0, 3.96) | −14.3 (−29.4, 0.76) | 0.615 | |
| Protein (g/day) | Baseline | 96.6 (21.7) | 88.5 (17.9) | 0.229 |
| Changes after 3 m. | −6.02 (−13.7, 1.64) | −2.29 (−9.22, 4.63) | 0.454 | |
| Total fat (g/day) | Baseline | 118.6 (20.2) | 111.4 (29.9) | 0.397 |
| Changes after 3 m. | −6.16 (−13.1, 0.83) | 1.78 (−8.66, 12.2) | 0.188 | |
| Alcohol (g/day) | Baseline | 0.00 [0.00 to 0.09] | 0.00 [0.00 to 1.64] | 0.916 |
| Changes after 3 m. | 0.00 [0.00 to 0.38] | 0.00 [0.00 to 0.00] | 0.046 | |
| SFAs (g/day) | Baseline | 32.2 (8.48) | 29.7 (9.95) | 0.418 |
| Changes after 3 m. | −3.29 (−5.82, −0.75) * | 0.21 (−2.86, 3.27) | 0.071 | |
| MUFAs (g/day) | Baseline | 60.1 (11.5) | 58.7 (15.0) | 0.753 |
| Changes after 3 m. | −1.93 (−4.82, 0.95) | 1.84 (−3.89, 7.56) | 0.216 | |
| PUFAs (g/day) | Baseline | 17.4 (4.35) | 14.9 (5.18) | 0.124 |
| Changes after 3 m. | −0.38 (−2.05, 1.30) | −0.12 (−1.78, 1.54) | 0.823 | |
| Cholesterol (mg/day) | Baseline | 344.5 (112.3) | 304.8 (84.6) | 0.234 |
| Changes after 3 m. | −21.9 (−50.7, 6.86) | 1.60 (−18.8, 22.0) | 0.174 | |
| Sugar (g/day) | Baseline | 94.9 (28.3) | 86.9 (24.6) | 0.369 |
| Changes after 3 m. | −10.7 (−20.9, −0.57) * | −8.03 (−17.5, 1.43) | 0.685 | |
| Fiber (g/day) | Baseline | 26.7 (8.2) | 22.8 (6.1) | 0.110 |
| Changes after 3m. | −1.16 (−2.96, 0.64) | −1.46 (−3.93, 1.00) | 0.835 | |
| Na (mg/day) | Baseline | 3194 (1050) | 3064 (1053) | 0.710 |
| Changes after 3 m. | −351.9 (−566.6, −137.3) * | −166.5 (−383.2, 50.2) | 0.209 | |
| Fe (mg/day) | Baseline | 13.9 (3.4) | 12.2 (2.7) | 0.103 |
| Changes after 3 m. | −0.58 (−1.62, 0.45) | −0.66 (−1.68, 0.36) | 0.918 | |
| Zn (mg/day) | Baseline | 10.1 (3) | 9.4 (2.2) | 0.491 |
| Changes after 3 m. | −0.61 (−1.49, 0.28) | −0.55 (−1.35, 0.26) | 0.917 | |
| Vitamin A (µg/day) | Baseline | 820.2 [630.2 to 1197] | 630.1 [545.1 to 826.6] | 0.098 |
| Changes after 3 m. | −7.18 [−42.9 to 15.4] | −13.3 [−61.1 to 16.2] | 0.822 | |
| Vitamin D (µg/day) | Baseline | 4.02 (1.80) | 2.93 (1.75) | 0.069 |
| Changes after 3 m. | 0.16 (−0.69, 1.00) | 0.59 (−0.07, 1.26) | 0.403 | |
| Vitamin E (mg/day) | Baseline | 14.5 (2.74) | 12.8 ± 3.92 | 0.144 |
| Changes after 3 m. | 0.13 (−1.14, 1.39) | 0.14 (−1.09, 1.38) | 0.988 | |
| Vitamin B6 (mg/day) | Baseline | 2.25 (0.59) | 2.04 (0.67) | 0.322 |
| Changes after 3 m. | −0.13 (−0.28, 0.02) | −0.05 (−0.27, 0.18) | 0.514 | |
| Vitamin B12 (µg/day) | Baseline | 6.66 (2.85) | 5.75 (2.98) | 0.346 |
| Changes after 3 m. | 0.11 (−0.56, 0.79) | 0.15 (−0.51, 0.82) | 0.928 | |
| Vitamin C (mg/day) | Baseline | 189.2 (89.3) | 153.6 (73.1) | 0.195 |
| Changes after 3 m. | −33.0 (−63.0, −2.91) * | 0.86 (−28.3, 30.0) | 0.098 | |
| K (mg/day) | Baseline | 3564 (1036) | 3250 (806.2) | 0.312 |
| Changes after 3 m. | −277.0 (−611.9, 57.9) | −193.4 (−457.0, 70.1) | 0.685 | |
| Calcium (mg/day) | Baseline | 859.9 (254.6) | 801.2 (285.2) | 0.513 |
| Changes after 3 m. | −94.7 (−199.9, 10.5) | −28.7 (−112.7, 55.2) | 0.313 | |
| Folic acid (µg/day) | Baseline | 391.3 (142.4) | 322.9 (108.2) | 0.110 |
| Changes after 3 m. | −22.0 (−62.7, 18.6) | −19.5 (−51.3, 12.2) | 0.920 |
| Control (n = 19) | FontActiv (n = 19) | |||
|---|---|---|---|---|
| Mean | Mean | p-Value between Groups | ||
| Body weight (kg) | Baseline 1 | 65.6 ± 10.2 | 58.3 ± 10.2 | 0.034 |
| Changes after 3 m. | 0.04 (−0.58, 0.66) | 1.50 (0.88, 2.12) * | 0.002 | |
| BMI (kg/m2) | Baseline | 25.3 ± 3.61 | 21.6 ± 3.77 | 0.004 |
| Changes after 3 m. | 0.05 (−0.18, 0.27) | 0.54 (0.31, 0.77) * | 0.006 | |
| Waist circumference (cm) | Baseline | 94.5 ± 10.3 | 82.1 ± 18.3 | 0.017 |
| Changes after 3 m. | 2.11 (−1.87, 6.08) | 1.69 (−2.17, 5.54) | 0.883 | |
| Hip circumference (cm) | Baseline | 99.1 ± 8.20 | 88.4 ± 17.3 | 0.026 |
| Changes after 3 m. | 1.96 (−1.01, 4.94) | 1.55 (−1.63, 4.73) | 0.853 | |
| Arm circumference (cm) | Baseline | 28.0 ± 4.55 | 24.1 ± 2.63 | 0.003 |
| Changes after 3 m. | −0.48 (−1.35, 0.39) | −0.14 (−0.99, 0.70) | 0.595 | |
| Calf circumference (cm) | Baseline | 42.3 ± 4.51 | 38.6 ± 8.11 | 0.106 |
| Changes after 3 m. | −0.33 (−1.88, 1.22) | 1.09 (−0.37, 2.55) | 0.190 | |
| Triceps fold (mm) | Baseline | 14.0 ± 5.77 | 10.8 ± 4.31 | 0.063 |
| Changes after 3 m. | −0.43 (−1.33, 0.47) | 0.70 (−0.17, 1.58) | 0.079 |
| Control (n = 19) | FontActiv (n = 19) | |||
|---|---|---|---|---|
| Mean | Mean | p-Value | ||
| Prealbumin (g/L) 1 | Baseline 1 | 0.28 (0.20 to 0.33) | 0.22 (0.19 to 0.28) | 0.154 |
| Changes after 3 m. | 0.00 (−0.03 to 0.03) | 0.02 (−0.03 to 0.05) | 0.191 | |
| Albumin (g/L) | Baseline | 39.0 (36.0 to 41.0) | 38.0 (33.0 to 40.0) | 0.297 |
| Changes after 3 m. | 0.00 (−2.00 to 1.00) | 0.00 (0.00 to 3.00) | 0.258 | |
| Total protein (g/L) | Baseline | 61.9 (6.46) | 60.8 (7.52) | 0.614 |
| Changes after 3 m. | 0.10 (−2.01 to 2.21) | 0.58 (−1.52 to 2.69) | 0.743 | |
| HDL (mg/dL) | Baseline | 47.0 (40.0 to 54.0) | 56.0 (40.0 to 66.0) | 0.163 |
| Changes after 3 m. | 0.00 (−7.00 to 7.00) | −5.00 (−12.0 to 5.00) | 0.271 | |
| Hemoglobin (g/L) | Baseline | 119.0 (109.0 to 128.0) | 112.0 (96.0 to 123.0) | 0.172 |
| Changes after 3 m. | −4.00 (−12.0 to 1.00) | 0.00 (−14.0 to 20) | 0.246 | |
| Glycated hemoglobin (%) | Baseline | 5.90 (5.37 to 7.37) | 5.30 (4.80 to 5.50) | 0.010 |
| Changes after 3 m. | 0.00 (−0.45 to 0.30) | 0.00 (−0.52 to 0.30) | 0.782 | |
| Total leukocytes (109/L) | Baseline | 6.44 (5.16 to 7.64) | 6.32 (5.00 to 7.24) | 0.402 |
| Changes after 3 m. | 0.00 (−1.35 to 0.73) | 0.07 (−1.17 to 1.20) | 0.795 | |
| Hematocrit (L/L) | Baseline | 0.37 (0.04) | 0.35 (0.05) | 0.242 |
| Changes after 3 m. | −0.01 (−0.03 to 0.00) | 0.003 (−0.01 to 0.02) | 0.119 | |
| Transferrin saturation (%) | Baseline | 31.5 (15.7) | 24.1 (11.4) | 0.105 |
| Changes after 3 m. | −5.04 (−8.88 to −1.21) * | −3.71 (−7.55 to 0.12) | 0.628 | |
| Ferritin (ng/mL) | Baseline | 393.0 (239.0 to 525.0) | 454.0 (376.0 to 564.0) | 0.109 |
| Changes after 3 m. | 130.4 (−98.0 to 230.0) | 70.0 (−97.0 to 208.0) | 0.525 | |
| PTH (pg/mL) | Baseline | 182.0 (129.0 to 312.0) | 212.0 (99.0 to 350.0) | 0.832 |
| Changes after 3 m. | −1.00 (−38.0 to 54.0) | −25.0 (−117.5 to 69.2) | 0.711 | |
| C-Reactive Protein (mg/dL) | Baseline | 0.40 (0.00 to 0.73) | 0.58 (0.00 to 1.63) | 0.573 |
| Changes after 3 m. | 0.00 (0.00 to 1.16) | 0.00 (−1.00 to 0.63) | 0.165 | |
| Vitamin B1 (ng/mL) | Baseline | 66.0 (50.0 to 93.7) | 63.5 (54.9 to 120.7) | 0.744 |
| Changes after 3 m. | 4.30 (−16.9 to 10.1) | 5.40 (−8.20 to 23.7) | 0.316 | |
| Vitamin B6 (nmol/L) | Baseline | 69.1 (21.1 to 101.1) | 72.4 (24.1 to 94.3) | 0.976 |
| Changes after 3 m. | −6.80 (−76.3 to 21.6) | 9.90 (−18.3 to 59.6) | 0.356 | |
| Intracellular folic acid (ng/mL) | Baseline | 273.5 (74.3) | 252.8 (81.0) | 0.487 |
| Changes after 3 m. | 66.7 (25.3 to 108.2) * | 37.4 (−6.16 to 80.9) | 0.326 | |
| Serum folic acid (ng/mL) | Baseline | 19.6 (6.19 to 24.0) | 10.2 (6.26 to 24.0) | 0.545 |
| Changes after 3 m. | −0.11 (−2.00 to 0.06) | 0.00 (−1.17 to 1.59) | 0.239 | |
| Vitamin B12 (pg/mL) | Baseline | 380.0 (350.0 to 614.0) | 390.0 (313.2 to 517.5) | 0.538 |
| Changes after 3 m. | 21.5 (−115.0 to 57.2) | 14.5 (−9.00 to 78.7) | 0.829 | |
| Retinol (µg/dL) | Baseline | 72.7 (59.2 to 100.8) | 67.5 (55.3 to 86.4) | 0.354 |
| Changes after 3 m. | −7.80 (−23.3 to 10.1) | −2.40 (−10.1 to 8.10) | 0.560 | |
| 25-hydroxyvitamin D(3) (ng/dL) | Baseline | 10.5 (8.10 to 22.2) | 11.8 (6.40 to 15.6) | 0.354 |
| Changes after 3 m. | 3.80 (−5.90 to 4.90) | 8.80 (5.80 to 11.4) * | 0.016 | |
| Alpha-tocoferol (umol/L) | Baseline | 32.1 (6.87) | 32.6 (7.18) | 0.844 |
| Changes after 3 m. | −3.31 (−6.30 to −0.32) * | −2.33 (−5.10 to 0.44) | 0.624 | |
| Ca (mg/dL) | Baseline | 8.64 (0.78) | 8.29 (1.43) | 0.360 |
| Changes after 3 m. | 0.17 (−0.18 to 0.52) | 0.21 (−0.13 to 0.54) | 0.880 | |
| P (mg/dL) | Baseline | 4.50 (1.75) | 4.36 (1.30) | 0.771 |
| Changes after 3 m. | −0.29 (−0.84 to 0.25) | 0.49 (−0.04 to 1.02) | 0.045 | |
| Mg (mg/dL) | Baseline | 2.05 (0.34) | 2.09 (0.43) | 0.779 |
| Changes after 3 m. | −0.05 (−0.17 to 0.06) | 0.02 (−0.11 to 0.16) | 0.376 | |
| Se (µg/dL) | Baseline | 63.5 (16.8) | 60.4 (12.3) | 0.574 |
| Changes after 3 m. | 4.89 (−3.53 to 13.3) | 9.16 (1.37 to 17.0) * | 0.450 | |
| Zn (µg/dL) | Baseline | 77.4 (9.66) | 73.0 (17.0) | 0.400 |
| Changes after 3 m. | 1.91 (−5.78 to 9.60) | −3.06 (−9.93 to 3.81) | 0.333 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castro-Barquero, S.; Arias-Guillén, M.; Pi-Oriol, S.; Sacanella, E.; Romano-Andrioni, B.; Vidal-Lletjós, S.; Ruiz-León, A.M.; Estruch, R.; Casas, R. A Comparative Study of the Efficacy of an Intervention with a Nutritional Supplement for Patients with Chronic Kidney Disease: A Randomized Trial. J. Clin. Med. 2022, 11, 1647. https://doi.org/10.3390/jcm11061647
Castro-Barquero S, Arias-Guillén M, Pi-Oriol S, Sacanella E, Romano-Andrioni B, Vidal-Lletjós S, Ruiz-León AM, Estruch R, Casas R. A Comparative Study of the Efficacy of an Intervention with a Nutritional Supplement for Patients with Chronic Kidney Disease: A Randomized Trial. Journal of Clinical Medicine. 2022; 11(6):1647. https://doi.org/10.3390/jcm11061647
Chicago/Turabian StyleCastro-Barquero, Sara, Marta Arias-Guillén, Sofia Pi-Oriol, Emilio Sacanella, Barbara Romano-Andrioni, Sandra Vidal-Lletjós, Ana María Ruiz-León, Ramon Estruch, and Rosa Casas. 2022. "A Comparative Study of the Efficacy of an Intervention with a Nutritional Supplement for Patients with Chronic Kidney Disease: A Randomized Trial" Journal of Clinical Medicine 11, no. 6: 1647. https://doi.org/10.3390/jcm11061647
APA StyleCastro-Barquero, S., Arias-Guillén, M., Pi-Oriol, S., Sacanella, E., Romano-Andrioni, B., Vidal-Lletjós, S., Ruiz-León, A. M., Estruch, R., & Casas, R. (2022). A Comparative Study of the Efficacy of an Intervention with a Nutritional Supplement for Patients with Chronic Kidney Disease: A Randomized Trial. Journal of Clinical Medicine, 11(6), 1647. https://doi.org/10.3390/jcm11061647