
Prevalence of Opioid Use Disorder among Patients with Cancer-Related Pain: A Systematic Review


 and
and
Abstract
:1. Introduction
2. Materials and Methods
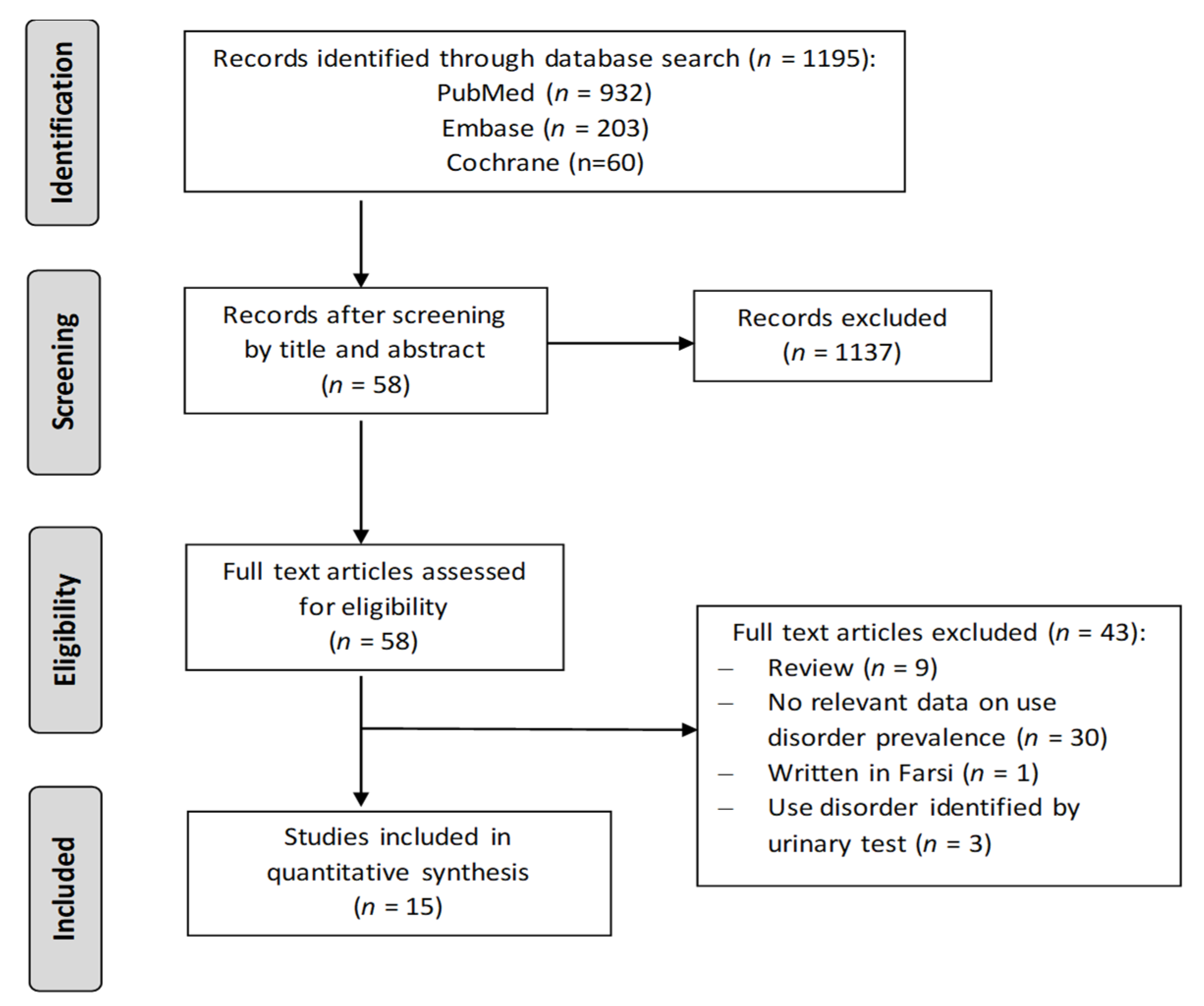
2.1. Search Strategy
2.2. Selection Criteria
2.3. Assessment of Methodological Quality
2.4. Statistical Analysis
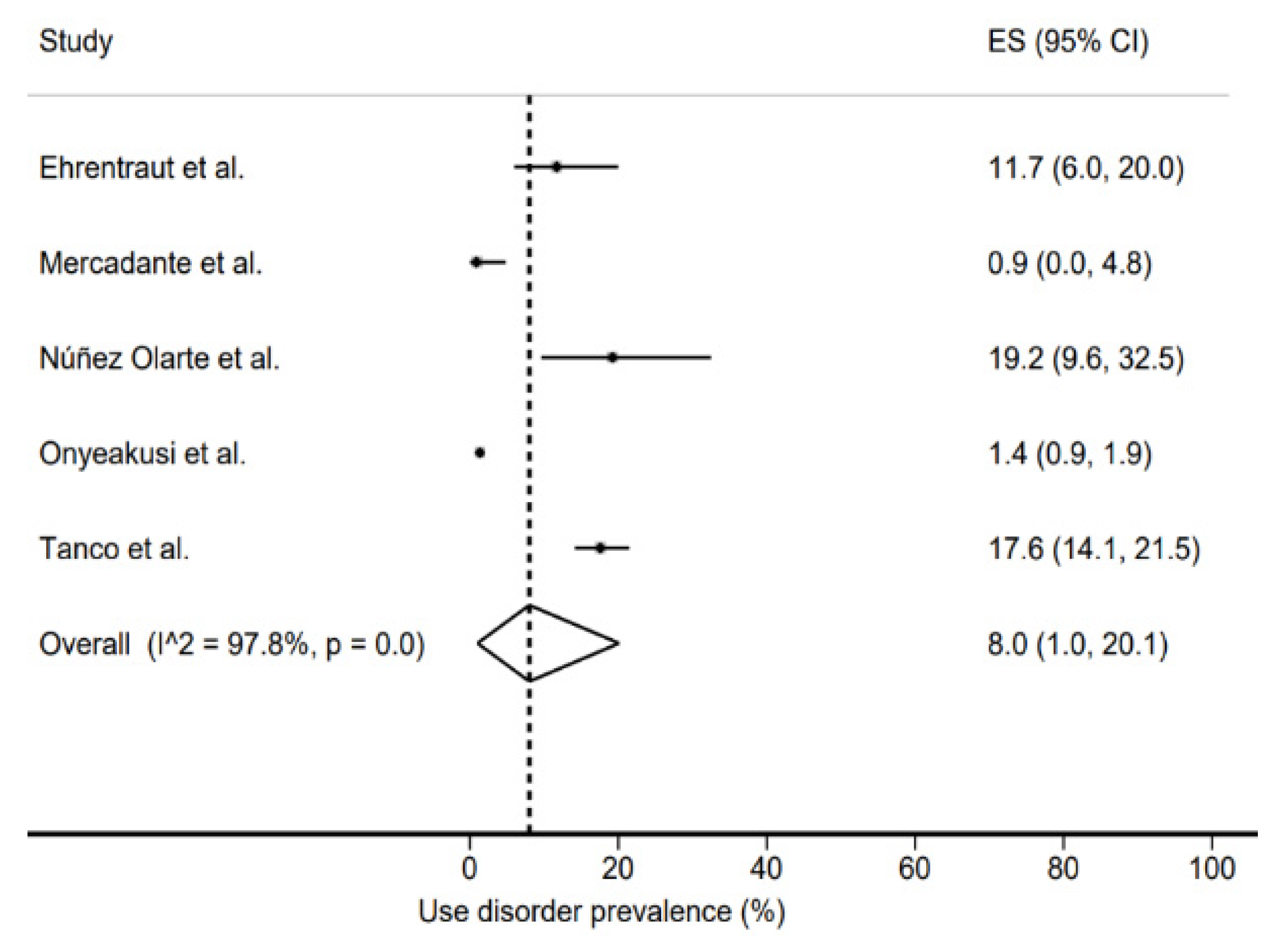
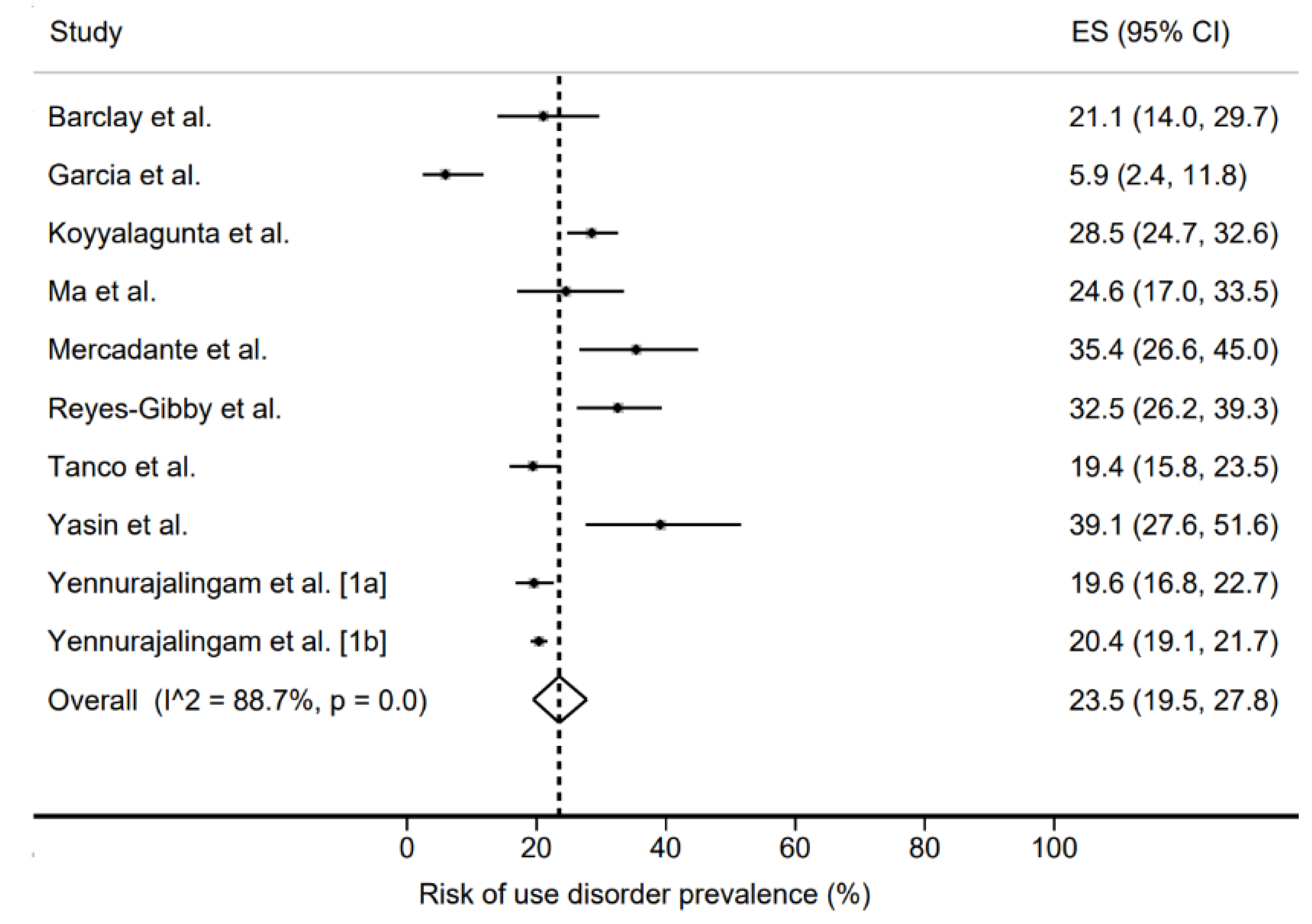
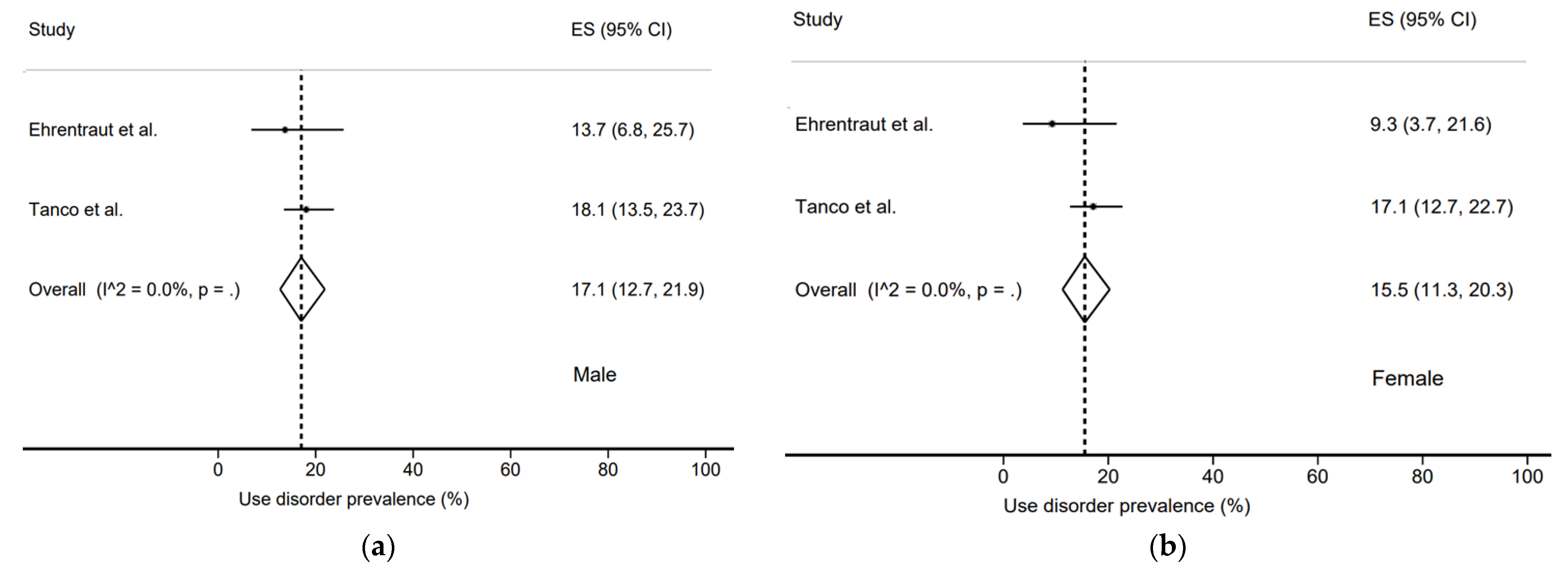
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, X.S.; Cleeland, C.S.; Mendoza, T.R.; Engstrom, M.C.; Liu, S.; Xu, G.; Hao, X.; Wang, Y.; Ren, X.S. The Effects of Pain Severity on Health-Related Quality of Life: A Study of Chinese Cancer Patients. Cancer 1999, 86, 1848–1855. [Google Scholar] [CrossRef]
- Strang, P. Cancer Pain—A Provoker of Emotional, Social and Existential Distress. Acta Oncol. 1998, 37, 641–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents. Available online: https://www.who.int/publications-detail-redirect/9789241550390 (accessed on 19 July 2021).
- Mercadante, S. Potential Strategies to Combat the Opioid Crisis. Expert Opin. Drug Saf. 2019, 18, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Actualité—Antalgiques Opioïdes: L’ANSM Publie un État des Lieux de la Consommation en France—ANSM. Available online: https://ansm.sante.fr/actualites/antalgiques-opioides-lansm-publie-un-etat-des-lieux-de-la-consommation-en-france (accessed on 19 July 2021).
- Christo, P.J.; Manchikanti, L.; Ruan, X.; Bottros, M.; Hansen, H.; Solanki, D.R.; Jordan, A.E.; Colson, J. Urine Drug Testing in Chronic Pain. Pain Physician 2011, 14, 123–143. [Google Scholar] [CrossRef] [PubMed]
- Kaye, A.D. Prescription Opioid Abuse in Chronic Pain: AnUpdated Review of Opioid Abuse Predictorsand Strategies to Curb Opioid Abuse: Part 1. Pain Physician 2017, 2, s93–s109. [Google Scholar] [CrossRef]
- Mercadante, S.; Craig, D.; Giarratano, A. US Food and Drug Administration’s Risk Evaluation and Mitigation Strategy for Extended-Release and Long-Acting Opioids: Pros and Cons, and a European Perspective. Drugs 2012, 72, 2327–2332. [Google Scholar] [CrossRef] [Green Version]
- Savage, S.R. Management of Opioid Medications in Patients with Chronic Pain and Risk of Substance Misuse. Curr. Psychiatry Rep. 2009, 11, 377–384. [Google Scholar] [CrossRef]
- Trouvin, A.-P.; Berenbaum, F.; Perrot, S. The Opioid Epidemic: Helping Rheumatologists Prevent a Crisis. RMD Open 2019, 5, e001029. [Google Scholar] [CrossRef]
- Arthur, J.; Bruera, E. Balancing Opioid Analgesia with the Risk of Nonmedical Opioid Use in Patients with Cancer. Nat. Rev. Clin. Oncol. 2019, 16, 213–226. [Google Scholar] [CrossRef]
- Passik, S.D.; Kirsh, K.L.; McDonald, M.V.; Ahn, S.; Russak, S.M.; Martin, L.; Rosenfeld, B.; Breitbart, W.S.; Portenoy, R.K. A Pilot Survey of Aberrant Drug-Taking Attitudes and Behaviors in Samples of Cancer and AIDS Patients. J. Pain Symptom Manag. 2000, 19, 274–286. [Google Scholar] [CrossRef]
- Bruera, E.; Paice, J.A. Cancer Pain Management: Safe and Effective Use of Opioids. Am. Soc. Clin. Oncol. Educ. Book 2015, e593–e599. [Google Scholar] [CrossRef] [PubMed]
- Checklists. Available online: https://testing36.scot.nhs.uk (accessed on 25 July 2021).
- Hoy, D.; Brooks, P.; Woolf, A.; Blyth, F.; March, L.; Bain, C.; Baker, P.; Smith, E.; Buchbinder, R. Assessing Risk of Bias in Prevalence Studies: Modification of an Existing Tool and Evidence of Interrater Agreement. J. Clin. Epidemiol. 2012, 65, 934–939. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials Revisited. Contemp. Clin. Trials 2015, 45, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onyeakusi, N.E.; Mukhtar, F.; Gbadamosi, S.O.; Oshunbade, A.; Adejumo, A.C.; Olufajo, O.; Owoh, J. Cancer-Related Pain Is an Independent Predictor of In-Hospital Opioid Overdose: A Propensity-Matched Analysis. Pain Med. 2019, 20, 2552–2561. [Google Scholar] [CrossRef]
- Mercadante, S.; Adile, C.; Tirelli, W.; Ferrera, P.; Penco, I.; Casuccio, A. Aberrant Opioid Use Behaviour in Advanced Cancer. BMJ Support. Palliat. Care 2020, 12, 107–113. [Google Scholar] [CrossRef]
- Ehrentraut, J.H.; Kern, K.D.; Long, S.A.; An, A.Q.; Faughnan, L.G.; Anghelescu, D.L. Opioid Misuse Behaviors in Adolescents and Young Adults in a Hematology/Oncology Setting. J. Pediatr. Psychol. 2014, 39, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Núñez Olarte, J.M.; Francisco López, M.D.C.; Conti Jiménez, M.; Sánchez Isac, M.; Pérez Aznar, C.; Solano Garzón, M.L.; Guevara Méndez, S. Management of Aberrant Opioid-Induced Behaviour in an “Early Palliative Care” Outpatient Clinic. Med. Paliativa 2018, 25, 175–183. [Google Scholar] [CrossRef]
- Tanco, K.; Kwon, J.H.; Park, J.C.; Wong, A.; Seo, L.; Liu, D.D.; Chisholm, G.B.; Williams, J.L.; Hui, D.; Bruera, E. Frequency, Predictors and Medical Record Documentation of Chemical Coping among Advanced Cancer Patients. Oncologist 2015, 20, 692–697. [Google Scholar] [CrossRef]
- Yennurajalingam, S.; Edwards, T.; Arthur, J.A.; Lu, Z.; Najera, J.; Nguyen, K.; Manju, J.; Kuriakose, L.; Wu, J.; Liu, D.; et al. Predicting the Risk for Aberrant Opioid Use Behavior in Patients Receiving Outpatient Supportive Care Consultation at a Comprehensive Cancer Center. Cancer 2018, 124, 3942–3949. [Google Scholar] [CrossRef] [Green Version]
- Yennurajalingam, S.; Edwards, T.; Arthur, J.; Lu, Z.; Erdogan, E.; Malik, J.S.; Naqvi, S.M.A.; Wu, J.; Liu, D.D.; Williams, J.L.; et al. The Development of a Nomogram to Determine the Frequency of Elevated Risk for Non-Medical Opioid Use in Cancer Patients. Palliat. Support. Care 2020, 19, 3–10. [Google Scholar] [CrossRef]
- Koyyalagunta, D.; Bruera, E.; Aigner, C.; Nusrat, H.; Driver, L.; Novy, D. Risk Stratification of Opioid Misuse among Patients with Cancer Pain Using the SOAPP-SF. Pain Med. 2013, 14, 667–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, J.D.; Horton, J.M.; Hwang, M.; Atayee, R.S.; Roeland, E.J. A Single-Center, Retrospective Analysis Evaluating the Utilization of the Opioid Risk Tool in Opioid-Treated Cancer Patients. J. Pain Palliat. Care Pharmacother. 2014, 28, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Barclay, J.S.; Owens, J.E.; Blackhall, L.J. Screening for Substance Abuse Risk in Cancer Patients Using the Opioid Risk Tool and Urine Drug Screen. Support. Care Cancer 2014, 22, 1883–1888. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Gibby, C.C.; Anderson, K.O.; Todd, K.H. Risk for Opioid Misuse among Emergency Department Cancer Patients. Acad. Emerg. Med. 2016, 23, 151–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, C.; Lefkowits, C.; Pelkofski, E.; Blackhall, L.; Duska, L.R. Prospective Screening with the Validated Opioid Risk Tool Demonstrates Gynecologic Oncology Patients Are at Low Risk for Opioid Misuse. Gynecol. Oncol. 2017, 147, 456–459. [Google Scholar] [CrossRef]
- Yasin, J.T.; Leader, A.E.; Petok, A.; Garber, G.; Stephens, B.; Worster, B. Validity of the Screener and Opioid Assessment for Patients with Pain-Revised (SOAPP-R) in Patients with Cancer. J. Opioid. Manag. 2019, 15, 272–274. [Google Scholar] [CrossRef] [PubMed]
- Passik, S.D.; Kirsh, K.L.; Donaghy, K.B.; Portenoy, R.K. Pain and Aberrant Drug-Related Behaviors in Medically Ill Patients with and without Histories of Substance Abuse. Clin. J. Pain 2006, 22, 173–181. [Google Scholar] [CrossRef]
- Bashandy, G.; Elfaramawi, M. Prevalence of Aberrant Medication-Related Behaviors in Chronic Cancer Pain Patients in the National Cancer Institute of Egypt. Reg. Anesth. Pain Med. 2016, 41, 296. [Google Scholar]
- Højsted, J.; Sjøgren, P. Addiction to Opioids in Chronic Pain Patients: A Literature Review. Eur. J. Pain 2007, 11, 490–518. [Google Scholar] [CrossRef]
- Jairam, V.; Yang, D.X.; Yu, J.B.; Park, H.S. Emergency Department Visits for Opioid Overdoses among Patients with Cancer. J. Natl. Cancer Inst. 2020, 112, 938–943. [Google Scholar] [CrossRef] [PubMed]
- Madadi, P.; Hildebrandt, D.; Lauwers, A.E.; Koren, G. Characteristics of Opioid-Users Whose Death Was Related to Opioid-Toxicity: A Population-Based Study in Ontario, Canada. PLoS ONE 2013, 8, e60600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Country | Type | ART | Total | Use Disorder Prevalence | Scale | Total Population of Study | Population with Use Disorder | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (Publication Year) | Actual (%) | Risk (%) | Females | Mean Age (SD) | hem/dig/gyn/pn/ mel/hn/genit/br | Females | Mean Age (SD) | hem/dig/gyn/pn/ mel/hn/genit/br | |||||
| Yennurajalingam et al. [23] (2018) | Texas | Rétro. Mono. | 7 | 729 | nr | 143 (19.6%) | SOAPP14 | 382 | 61 (53–69) | nr/nr/nr/nr/ nr/nr/nr/nr | 56 | 61 (54–67) | nr/nr/nr/nr/ nr/nr/nr/nr |
| Onyeakusi et al. [18] (2019) | Ohio | Retro. Multic. | 6 | 2665 | 36 (1.35%) | nr | 1560 | 59.5 (0.26) | nr/nr/nr/nr/ nr/nr/nr/nr | nr/nr/nr/nr/ nr/nr/nr/nr | |||
| Yennurajalingam et al. [24] (2020) | Texas | Rétro. Mono. | 8 | 3588 | nr | 731 (20.4%) | SOAPP14 | 1906 | 62 (52–70) | 178/646/256/573/ 197/572/417/485 | 326 | 61 (51–68) | 30/130/43/132/ 48/130/96/68 |
| Mercadante et al. [19] (2020) | Italy | Prosp. Multic. | 6 | 113 | 0 | 40 (35.4%) | SOAPP14 | 54 | 68 (13) | nr/31/nr/26/ nr/nr/26/13 | nr/nr/nr/nr/ nr/nr/nr/nr | ||
| Passik et al. [31] (2006) | Indiana | Prosp. Multic. | 6 | 100 | nr | nr | 62 | 60.1 (13.87) | nr/nr/nr/nr/ nr/nr/nr/nr | nr/nr/nr/nr/ nr/nr/nr/nr | |||
| Koyyalagunta et al. [25] (2013) | Texas | Prosp. Mono. | 6 | 522 | nr | 149 (28.5%) | SOAPP SF | 271 | 54 | 78/94/nr/57/ nr/78/nr/57 | 70 | 50 (±14) | nr/nr/nr/nr/ nr/nr/nr/nr |
| Ma et al. [26] (2014) | Californie | Rétro. Mono. | 6 | 114 | nr | 28 (24.6%) | ORT | 57 | 53 (14.3) | 21/33/11/4/ nr/8/7/13 | 11 | 52.5 (8.3) | 4/6/4/3/ nr/2/2/3 |
| Barclay et al. [27] (2014) | Virginie | Rétro. Mono. | 5 | 114 | nr | 24 (21%) | ORT | 73 | 53 | 12/13/18/14/ nr/14/2/20 | nr/nr/nr/nr/ nr/nr/nr/nr | ||
| Ehrentraut et al. [20] (2014) | Tennessee | Rétro. Mono. | 6 | 94 | 11 (11.7%) | nr | AOB list | 43 | 16.3 (0.28) | 47/nr/nr/nr/ nr/nr/nr/nr | 4 | 17.4 (2.8) | 7/nr/nr/nr/ nr/nr/nr/nr |
| Reyes-Gibby et al. [28] (2016) | Texas | Prosp. Mono. | 4 | 209 | nr | 68 (32.5%) | SOAPP-R | 102 | 54.2 (13.07) | 53/15/nr/18/ nr/nr/nr/24 | 36 | 52.1 | 19/2/nr/4/ nr/nr/nr/9 |
| Garcia et al. [29] (2017) | Virginie | Prosp. Mono. | 7 | 118 | nr | 7 (6%) | ORT | 118 | 57 | nr/nr/118/nr/ nr/nr/nr/nr | 7 | 47 (42–56) | nr/nr/7/nr/ nr/nr/nr/nr |
| Yasin et al. [30] (2019) | Pennsylvanie | Rétro. Mono. | 5 | 69 | nr | 27 (39.1%) | SOAPP-R | 41 | nr | nr/nr/nr/nr/ nr/nr/nr/nr | nr/nr/nr/nr/ nr/nr/nr/nr | ||
| Núñez Olarte et al. [21] (2018) | Espagne | Rétro. Mono. | 7 | 52 | 10 (19.2%) | nr | nr | nr | nr/nr/nr/nr/ nr/nr/nr/nr | 5 | 58,1 | nr/4/nr/2/ nr/1/1/1 | |
| Bashandy et al. [32] (2016) | Egypte | Prosp. Mono. | Abstr | nr | nr | 76% | COMM | nr | nr | nr/nr/nr/nr/ nr/nr/nr/nr | nr/nr/nr/nr/ nr/nr/nr/nr | ||
| Tanco et al. [22] (2015) | Texas | Rétro. Mono. | 7 | 432 | 76 (18%) | 84 (19.4%) | CAGE | 216 | 57 (49–65) | 26/70/nr/86/ nr/48/nr/60 | 37 | 53 (46–60) | 8/8/nr/15/ nr/14/nr/10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Preux, C.; Bertin, M.; Tarot, A.; Authier, N.; Pinol, N.; Brugnon, D.; Pereira, B.; Guastella, V. Prevalence of Opioid Use Disorder among Patients with Cancer-Related Pain: A Systematic Review. J. Clin. Med. 2022, 11, 1594. https://doi.org/10.3390/jcm11061594
Preux C, Bertin M, Tarot A, Authier N, Pinol N, Brugnon D, Pereira B, Guastella V. Prevalence of Opioid Use Disorder among Patients with Cancer-Related Pain: A Systematic Review. Journal of Clinical Medicine. 2022; 11(6):1594. https://doi.org/10.3390/jcm11061594
Chicago/Turabian StylePreux, Céline, Marion Bertin, Andréa Tarot, Nicolas Authier, Nathalie Pinol, David Brugnon, Bruno Pereira, and Virginie Guastella. 2022. "Prevalence of Opioid Use Disorder among Patients with Cancer-Related Pain: A Systematic Review" Journal of Clinical Medicine 11, no. 6: 1594. https://doi.org/10.3390/jcm11061594
APA StylePreux, C., Bertin, M., Tarot, A., Authier, N., Pinol, N., Brugnon, D., Pereira, B., & Guastella, V. (2022). Prevalence of Opioid Use Disorder among Patients with Cancer-Related Pain: A Systematic Review. Journal of Clinical Medicine, 11(6), 1594. https://doi.org/10.3390/jcm11061594