
Outcomes of COVID-19 Critically Ill Extremely Elderly Patients: Analysis of a Large, National, Observational Cohort

 , , , , ,
, , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
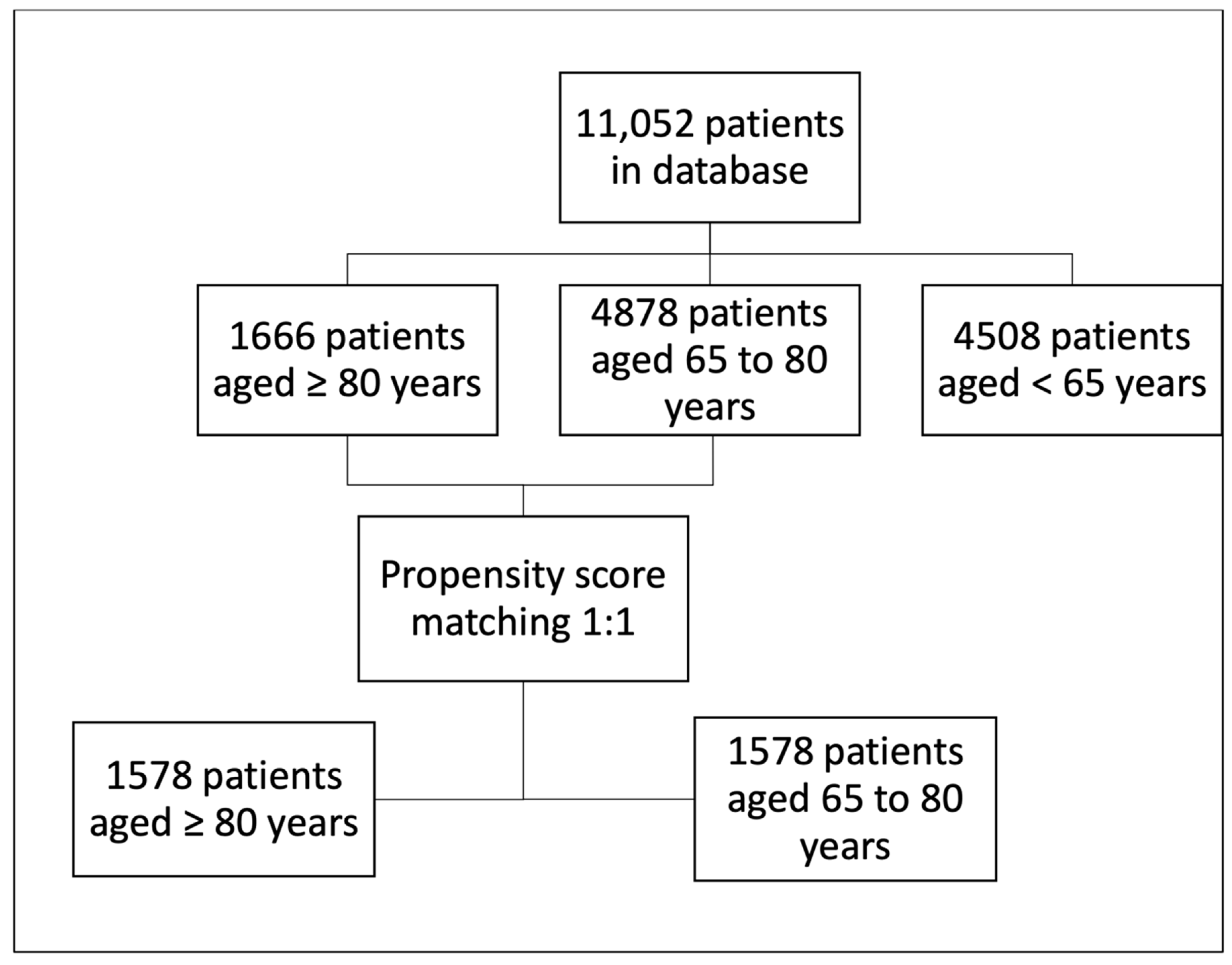
2.1. Study Design, Setting, and Participants
2.2. Variables and Definitions
2.3. Data Sources and Management
2.4. Study Size and Statistical Analyses
2.5. Ethical Aspects
3. Results
3.1. Patients’ Characteristics
3.2. ICU Admission and Management
3.3. ICU Complications
3.4. ICU Mortality and Predictors
3.5. Comparison with Less-Elderly Patients (65 ≤ Age < 80 Years) after Propensity Matching
3.6. The Differential Role of COVID-19 Surges on Corticotherapy Effect
3.7. Evaluation of Interaction Effect between Corticosteroids Administration and Gender and Comorbidities
4. Discussion
4.1. Patients’ Characteristics and ICU Mortality
4.2. Corticosteroid Prescription in Elderly Patients
4.3. Tocilizumab Administration in Elderly Patients
4.4. Elderly Definition Debate
4.5. The Clinical Relevance of Our Results
4.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hennessy, D.; Juzwishin, K.; Yergens, D.; Noseworthy, T.; Doig, C. Outcomes of Elderly Survivors of Intensive Care. Chest 2005, 127, 1764–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaninotto, P.; Falaschetti, E.; Sacker, A. Age trajectories of quality of life among older adults: Results from the English Longitudinal Study of Ageing. Qual. Life Res. 2009, 18, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Ariyo, K.; Canestrini, S.; David, A.S.; Ruck Keene, A.; Wolfrum, S.; Owen, G. Quality of life in elderly ICU survivors before the COVID-19 pandemic: A systematic review and meta-analysis of cohort studies. BMJ Open 2021, 11, e045086. [Google Scholar] [CrossRef] [PubMed]
- Demiselle, J.; Duval, G.; Hamel, J.-F.; Renault, A.; Bodet-Contentin, L.; Martin-Lefèvre, L.; Vivier, D.; Villers, D.; Lefèvre, M.; Robert, R.; et al. Determinants of hospital and one-year mortality among older patients admitted to intensive care units: Results from the multicentric SENIOREA cohort. Ann. Intensive Care 2021, 11, 35. [Google Scholar] [CrossRef]
- Ihra, G.C.; Lehberger, J.; Hochrieser, H.; Bauer, P.; Schmutz, R.; Metnitz, B.; Metnitz, P.G.H. Development of demographics and outcome of very old critically ill patients admitted to intensive care units. Intensive Care Med. 2012, 38, 620–626. [Google Scholar] [CrossRef]
- Aziz, S.; Arabi, Y.M.; Alhazzani, W.; Evans, L.; Citerio, G.; Fischkoff, K.; Salluh, J.; Meyfroidt, G.; Alshamsi, F.; Oczkowski, S.; et al. Managing ICU surge during the COVID-19 crisis: Rapid guidelines. Intensive Care Med. 2020, 46, 1303–1325. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.F.; Korevaar, D.A.; Matczak, S.; Chalumeau, M.; Allali, S.; Toubiana, J. COVID-19–Related Fatalities and Intensive-Care-Unit Admissions by Age Groups in Europe: A Meta-Analysis. Front. Med. 2021, 7, 560685. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected with SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Azzolina, D.; Magnani, C.; Gallo, E.; Ferrante, D.; Gregori, D. Gender and age factors affecting the mortality during the COVID-19 epidemic in Italy. Epidemiol. Prev. 2020, 44, 252–259. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Boccardi, V.; Ruggiero, C.; Mecocci, P. COVID-19: A Geriatric Emergency. Geriatrics 2020, 5, 24. [Google Scholar] [CrossRef] [PubMed]
- Clarfield, A.M.; Dwolatzky, T. Age and Ageing during the COVID-19 Pandemic; Challenges to Public Health and to the Health of the Public. Front. Public Health 2021, 9, 655831. [Google Scholar] [CrossRef] [PubMed]
- Swiss Academy of Medical Sciences. COVID-19 pandemic: Triage for intensive-care treatment under resource scarcity. Swiss Med. Wkly. 2020, 150, w20229. [Google Scholar] [CrossRef]
- Piers, R.; Van Braeckel, E.; Benoit, D.; Van Den Noortgate, N. Early resuscitation orders in hospitalized oldest-old with COVID-19: A multicenter cohort study. Palliat. Med. 2021, 35, 1288–1294. [Google Scholar] [CrossRef] [PubMed]
- Matheny Antommaria, A.H.; Gibb, T.S.; McGuire, A.L.; Wolpe, P.R.; Wynia, M.K.; Applewhite, M.K.; Caplan, A.; Diekema, D.S.; Hester, D.M.; Lehmann, L.S.; et al. Ventilator Triage Policies during the COVID-19 Pandemic at U.S. Hospitals Associated with Members of the Association of Bioethics Program Directors. Ann. Intern. Med. 2020, 173, 188–194. [Google Scholar] [CrossRef]
- van der Veer, T.; van der Sar-van der Brugge, S.; Paats, M.S.; van Nood, E.; de Backer, I.C.; Aerts, J.G.J.V.; van der Eerden, M.M. Do-not-intubate status and COVID-19 mortality in patients admitted to Dutch non-ICU wards. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 2207–2209. [Google Scholar] [CrossRef] [PubMed]
- Flaatten, H.; Guidet, B.; de Lange, D.W.; Beil, M.; Leaver, S.K.; Fjølner, J.; van Heerden, P.V.; Sigal, S.; Szczeklik, W.; Jung, C. The importance of revealing data on limitation of life sustaining therapy in critical ill elderly Covid-19 patients. J. Crit. Care 2022, 67, 147–148. [Google Scholar] [CrossRef]
- Oba, S.; Altınay, M.; Salkaya, A.; Türk, H.Ş. Evaluation of the effect of clinical characteristics and intensive care treatment methods on the mortality of covid-19 patients aged 80 years and older. BMC Anesthesiol. 2021, 21, 291. [Google Scholar] [CrossRef]
- Nabors, C.; Sridhar, A.; Hooda, U.; Lobo, S.; Levine, A.; Frishman, W.; Dhand, A. Characteristics and Outcomes of Patients 80 Years and Older Hospitalized with Coronavirus Disease 2019 (COVID-19). Cardiol. Rev. 2021, 29, 39–42. [Google Scholar] [CrossRef]
- Vrillon, A.; Hourregue, C.; Azuar, J.; Grosset, L.; Boutelier, A.; Tan, S.; Roger, M.; Mourman, V.; Mouly, S.; Sène, D.; et al. COVID-19 in Older Adults: A Series of 76 Patients Aged 85 Years and Older with COVID-19. J. Am. Geriatr. Soc. 2020, 68, 2735–2743. [Google Scholar] [CrossRef] [PubMed]
- COVID 19 Date La Zi—Date Oficiale [Internet]. Available online: https://datelazi.ro/ (accessed on 8 March 2022).
- Andrei, S.; Isac, S.; Jelea, D.; Martac, C.; Stefan, M.-G.; Cotorogea-Simion, M.; Buzatu, C.G.; Ingustu, D.; Abdulkareem, I.; Vasilescu, C.; et al. COVID-19 Pandemic Was Associated with Lower Activity but Not Higher Perioperative Mortality in a Large Eastern European Center. Med. Sci. Monit. 2022; in press. [Google Scholar] [CrossRef]
- Recensământul Populaţiei şi al Locuinţelor—2011 [Internet]. Available online: https://www.recensamantromania.ro/rpl-2011/rezultate-2011/ (accessed on 8 March 2022).
- Guillon, A.; Laurent, E.; Godillon, L.; Kimmoun, A.; Grammatico-Guillon, L. Long-term mortality of elderly patients after intensive care unit admission for COVID-19. Intensive Care Med. 2021, 47, 710–712. [Google Scholar] [CrossRef] [PubMed]
- The COVID-ICU Investigators; Dres, M.; Hajage, D.; Lebbah, S.; Kimmoun, A.; Pham, T.; Béduneau, G.; Combes, A.; Mercat, A.; Guidet, B.; et al. Characteristics, management, and prognosis of elderly patients with COVID-19 admitted in the ICU during the first wave: Insights from the COVID-ICU study: Prognosis of COVID-19 elderly critically ill patients in the ICU. Ann. Intensive Care 2021, 11, 77. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, C.; Mostert, C.; Hentschker, C.; Voshaar, T.; Malzahn, J.; Schillinger, G.; Klauber, J.; Janssens, U.; Marx, G.; Weber-Carstens, S.; et al. Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: An observational study. Lancet Respir. Med. 2020, 8, 853–862. [Google Scholar] [CrossRef]
- Jung, C.; Flaatten, H.; Fjølner, J.; Bruno, R.R.; Wernly, B.; Artigas, A.; Bollen Pinto, B.; Schefold, J.C.; Wolff, G.; Kelm, M.; et al. The impact of frailty on survival in elderly intensive care patients with COVID-19: The COVIP study. Crit. Care 2021, 25, 149. [Google Scholar] [CrossRef] [PubMed]
- Falandry, C.; Malapert, A.; Roche, M.; Subtil, F.; Berthiller, J.; Boin, C.; Dubreuil, J.; Ravot, C.; Bitker, L.; Abraham, P.; et al. Risk factors associated with day-30 mortality in patients over 60 years old admitted in ICU for severe COVID-19: The Senior-COVID-Rea Multicentre Survey protocol. BMJ Open 2021, 11, e044449. [Google Scholar] [CrossRef]
- Becerra-Muñoz, V.M.; Núñez-Gil, I.J.; Eid, C.M.; Aguado, M.G.; Romero, R.; Huang, J.; Mulet, A.; Rametta, F.; Liebetrau, C.; Aparisi, A.; et al. Clinical profile and predictors of in-hospital mortality among older patients admitted for COVID-19. Age Ageing 2021, 33, 326–334. [Google Scholar] [CrossRef]
- Fagard, K.; Gielen, E.; Deschodt, M.; Devriendt, E.; Flamaing, J. Risk factors for severe COVID-19 disease and death in patients aged 70 and over: A retrospective observational cohort study. Acta Clin. Belg. 2021, 1–8. [Google Scholar] [CrossRef]
- Powell, T.; Bellin, E.; Ehrlich, A.R. Older Adults and Covid-19: The Most Vulnerable, the Hardest Hit. Hastings Cent. Rep. 2020, 50, 61–63. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; The Northwell COVID-19 Research Consortium; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052. [Google Scholar] [CrossRef]
- Gkoufa, A.; Maneta, E.; Ntoumas, G.N.; Georgakopoulou, V.E.; Mantelou, A.; Kokkoris, S.; Routsi, C. Elderly adults with COVID-19 admitted to intensive care unit: A narrative review. World J. Crit. Care Med. 2021, 10, 278–289. [Google Scholar] [CrossRef] [PubMed]
- Guillon, A.; Hermetet, C.; Barker, K.A.; Jouan, Y.; Gaborit, C.; Ehrmann, S.; Le Manach, Y.; Dequin, P.-F.; Grammatico-Guillon, L. Long-term survival of elderly patients after intensive care unit admission for acute respiratory infection: A population-based, propensity score-matched cohort study. Crit. Care 2020, 24, 384. [Google Scholar] [CrossRef] [PubMed]
- Hussien, H.; Nastasa, A.; Apetrii, M.; Nistor, I.; Petrovic, M.; Covic, A. Different aspects of frailty and COVID-19: Points to consider in the current pandemic and future ones. BMC Geriatr. 2021, 21, 389. [Google Scholar] [CrossRef] [PubMed]
- Archard, D.; Caplan, A. Is it wrong to prioritise younger patients with covid-19? BMJ 2020, 369, m1509. [Google Scholar] [CrossRef] [Green Version]
- Hewitt, J.; Carter, B.; Vilches-Moraga, A.; Quinn, T.J.; Braude, P.; Verduri, A.; Pearce, L.; Stechman, M.; Short, R.; Price, A.; et al. The effect of frailty on survival in patients with COVID-19 (COPE): A multicentre, European, observational cohort study. Lancet Public Health 2020, 5, e444–e451. [Google Scholar] [CrossRef]
- Medetalibeyoglu, A.; Senkal, N.; Kose, M.; Catma, Y.; Caparali, E.B.; Erelel, M.; Oncul, M.O.; Bahat, G.; Tukek, T. Older Adults Hospitalized with Covid-19: Clinical Characteristics and Early Outcomes from a Single Center in Istanbul, Turkey. J. Nutr. Health Aging 2020, 24, 928–937. [Google Scholar] [CrossRef]
- COVID-19 Monza Team members; Bellelli, G.; Rebora, P.; Valsecchi, M.G.; Bonfanti, P.; Citerio, G. Frailty index predicts poor outcome in COVID-19 patients. Intensive Care Med. 2020, 46, 1634–1636. [Google Scholar] [CrossRef]
- Jung, C.; Wernly, B.; Fjølner, J.; Bruno, R.R.; Dudzinski, D.; Artigas, A.; Bollen Pinto, B.; Schefold, J.C.; Wolff, G.; Kelm, M.; et al. Steroid use in elderly critically ill COVID-19 patients. Eur. Respir. J. 2021, 58, 2100979. [Google Scholar] [CrossRef]
- Recovery Collaborative Group; Abbas, M.; Abbass, H.; Abbott, A.; Abdallah, N.; Abdelaziz, A.; Abdelfattah, M.; Abdelqader, B.; Abdul, B.; Abdul Rasheed, A.; et al. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2021, 397, 1637–1645. [Google Scholar] [CrossRef]
- Spini, A.; Giudice, V.; Brancaleone, V.; Morgese, M.G.; De Francia, S.; Filippelli, A.; Ruggieri, A.; Ziche, M.; Ortona, E.; Cignarella, A.; et al. Sex-tailored pharmacology and COVID-19: Next steps towards appropriateness and health equity. Pharmacol. Res. 2021, 173, 105848. [Google Scholar] [CrossRef]
- POSE Study Group. Peri-interventional outcome study in the elderly in Europe: A 30-day prospective cohort study. Eur. J. Anaesthesiol. 2021. publish ahead of print. Available online: https://journals.lww.com/10.1097/EJA.0000000000001639 (accessed on 8 March 2022).
- Garrouste-Orgeas, M.; Boumendil, A.; Pateron, D.; Aergerter, P.; Somme, D.; Simon, T.; Guidet, B. Selection of intensive care unit admission criteria for patients aged 80 years and over and compliance of emergency and intensive care unit physicians with the selected criteria: An observational, multicenter, prospective study. Crit. Care Med. 2009, 37, 2919–2928. [Google Scholar] [CrossRef] [PubMed]
- Demographic Change in Europe. Country Factsheets: Romania [Internet]. Available online: https://ec.europa.eu/eurostat/documents/10186/10994376/RO-EN.pdf (accessed on 8 March 2022).
- Jordan, R.E.; Adab, P.; Cheng, K.K. Covid-19: Risk factors for severe disease and death. BMJ 2020, 368, m1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ARDS Definition Task Force. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Levey, A.S.; Eckardt, K.U.; Dorman, N.M.; Christiansen, S.L.; Hoorn, E.J.; Ingelfinger, J.R.; Inker, L.A.; Levin, A.; Mehrotra, R.; Palevsky, P.M.; et al. Nomenclature for kidney function and disease: Report of a Kidney Disease: Improving Global Outcomes (KDIGO) Consensus Conference. Kidney Int. 2020, 97, 1117–1129. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]


{kind=link}
| All Cohort n = 1666 | Survivors n = 361 | Non-Survivors n = 1305 | p-Value | Missing n (%) | |
|---|---|---|---|---|---|
| Age (years), median | 83 [81–86] | 83 [81–86] | 83 [81–86] | 0.1 | |
| Male sex, n (%) | 834 (50) | 157 (44) | 677 (52) | 0.005 | |
| Clinical Status on ICU Admission | |||||
| Shiver (yes), n (%) | 239 (14) | 52 (14) | 187 (14) | 0.9 | |
| Headache (yes), n (%) | 177 (11) | 43 (12) | 134 (10) | 0.3 | |
| Myalgia (yes), n (%) | 266 (16) | 63 (18) | 203 (16) | 0.3 | |
| Fever (yes), n (%) | 561 (34) | 100 (28) | 461 (35) | <0.01 | |
| Nausea (yes), n (%) | 88 (5) | 22 (6) | 66 (5) | 0.4 | |
| Cough (yes), n (%) | 876 (53) | 180 (50) | 696 (53) | 0.2 | |
| Diarrhoea (yes), n (%) | 79 (5) | 18 (5) | 61 (5) | 0.8 | |
| Dyspnoea (yes), n (%) | 1288 (77) | 247 (68) | 1041 (80) | <0.001 | |
| SpO2 (%), median | 84 [70–91] | 93 [87–97] | 80 [70–90] | <0.001 | |
| ARDS (yes), n (%) | 595 (36) | 89 (25) | 506 (39) | <0.001 | |
| GCS, median | 12 [6–15] | 15 [13–15] | 12 [4–15] | <0.001 | |
| SOFA | 6 [4–12] | 5 [3–8] | 7 [4–13] | <0.001 | 262 (15.7) |
| Associated Medical History | |||||
| Ischemic heart disease (yes), n (%) | 972 (58) | 204 (57) | 768 (59) | 0.4 | |
| Autoimmune disease (yes), n (%) | 20 (1) | 3 (1) | 17 (1) | 0.4 | |
| Dialysis patient (yes), n (%) | 43 (3) | 14 (4) | 29 (2) | 0.07 | |
| COPD (yes), n (%) | 156 (9) | 42 (12) | 114 (9) | 0.09 | |
| Past or current cancer (yes), n (%) | 151 (9) | 32 (9) | 119 (9) | 0.8 | |
| Chronic kidney disease (yes), n (%) | 448 (27) | 89 (25) | 359 (28) | 0.2 | |
| Diabetes type 1 (yes), n (%) | 18 (1) | 3 (1) | 15 (1) | 0.6 | |
| Diabetes type 2 (yes), n (%) | 509 (31) | 105 (29) | 404 (31) | 0.4 | |
| Heart failure (yes), n (%) | 764 (46) | 171 (47) | 593 (45) | 0.5 | |
| Arterial hypertension (yes), n (%) | 1339 (80) | 294 (81) | 1045 (80) | 0.5 | |
| Variables | All Cohort n = 1666 | Survivors n = 361 | Non-Survivors n = 1305 | p-Value | Missing n (%) |
|---|---|---|---|---|---|
| Maximum SOFA, median | 8 [4–14] | 5 [3–8] | 9 [5–15] | <0.001 | |
| Respiratory management | |||||
| Non-invasive respiratory management | |||||
| HFO2 (yes), n (%) | 698 (42) | 194 (54) | 504 (39) | <0.001 | |
| HFO2 only (yes), n (%) | 225 (14) | 125 (35) | 100 (8) | <0.001 | |
| NIV (yes), n (%) | 729 (44) | 106 (29) | 623 (48) | <0.001 | |
| NIV only (yes), n (%) | 201 (12) | 39 (11) | 162 (12) | 0.406 | |
| HFO2 and NIV (yes), n (%) | 113 (7) | 60 (17) | 53 (4) | <0.001 | |
| Invasive respiratory management | |||||
| Mechanical ventilation (yes), n (%) | 886 (53) | 29 (8) | 857 (66) | <0.001 | |
| MV only (yes), n (%) | 325 (20) | 15 (4) | 310 (24) | <0.001 | |
| HFO2 and MV (yes), n (%) | 146 (9) | 7 (2) | 139 (11) | <0.001 | |
| NIV and MV (yes), n (%) | 201 (12) | 5 (1.5) | 196 (15) | <0.001 | |
| HFO2, NIV, and MV (yes), n (%) | 214 (13) | 2 (1) | 212 (16) | <0.001 | |
| Neuromuscular blockade (yes), n (%) | 162 (10) | 5 (1) | 157 (12) | <0.001 | |
| Maximum PEEP (cm H2O), median | 10 [8–12] | 8 [7–10] | 10 [8–12] | 0.2 | |
| Prone ventilation (yes), n (%) | 175 (11) | 22 (6) | 153 (12) | <0.01 | |
| Treatment | |||||
| Corticosteroids (yes), n (%) | 1295 (78) | 246 (68) | 1049 (80) | <0.001 | |
| Remdesivir (yes), n (%) | 316 (19) | 48 (13) | 268 (21) | <0.01 | |
| Hydroxychloroquine (yes), n (%) | 356 (21) | 84 (23) | 272 (21) | 0.3 | |
| Lopinavir/Ritonavir (yes), n (%) | 385 (23) | 91 (25) | 294 (23) | 0.2 | |
| Tocilizumab (yes), n (%) | 138 (8) | 22 (6) | 116 (9) | 0.08 | |
| Variables | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age (per 1 year), reference 80 years | 1.02 (0.99, 1.05) | 0.1 | - | - |
| Gender (male), reference female | 1.40 (1.10, 1.77) | 0.005 | 1.36 (1.00, 1.85) | 0.049 |
| Past medical history | ||||
| Ischemic Heart Disease (yes) | 1.10 (0.87, 1.39) | 0.4 | - | - |
| Cancer (yes) | 1.03 (0.68, 1.55) | 0.8 | - | - |
| Chronic Kidney Disease (yes) | 1.16 (0.88, 1.51) | 0.2 | - | - |
| Diabetes Type 2 (yes) | 1.09 (0.84, 1.41) | 0.4 | - | - |
| Heart Failure (yes) | 0.92 (0.73, 1.16) | 0.5 | - | - |
| HTA (yes) | 0.91 (0.68, 1.23) | 0.5 | - | - |
| Symptoms on admission | ||||
| Dyspnoea (yes) | 1.82 (1.40, 2.36) | <0.001 | 1.81 (1.27, 2.59) | 0.001 |
| Fever (yes) | 1.43 (1.1, 1.84) | 0.007 | 1.24 (0.89, 1.73) | 0.205 |
| SpO2 < 90% on admission (yes) | 5.30 (4.13, 6.8) | <0.001 | 3.78 (2.76, 5.16) | <0.001 |
| ARDS (yes) | 1.93 (1.48, 2.52) | <0.001 | 1.07 (0.76, 1.51) | 0.7 |
| GCS on admission (each scale point) | 0.75 (0.72, 0.79) | <0.001 | 0.81 (0.76, 0.86) | <0.001 |
| Evolution in ICU | ||||
| SOFA (each score point) | 1.13 (1.10, 1.16) | <0.001 | 1.03 (1.01, 1.07) | 0.017 |
| HFO2 only (yes) * | 0.16 (0.12, 0.21) | <0.001 | 0.37 (0.27, 0.52) | <0.001 |
| HFO2 + NIV only (yes) * | 0.21 (0.14, 0.31) | <0.001 | ||
| HFO2 (yes) | 0.54 (0.43, 0.69) | <0.001 | - | |
| NIV (yes) | 2.19 (1.70, 2.82) | <0.001 | - | - |
| NIV only (yes) | 1.17 (0.81, 1.7) | 0.406 | - | |
| Mechanical ventilation (yes) | 21.90 (14.73, 32.55) | <0.001 | 6.78 (4.27, 10.77) | <0.001 |
| Mechanical ventilation only (yes) | 7.2 (4.22, 12.24) | <0.001 | - | |
| HFO2 and MV (yes), n (%) | 6.03 (2.8, 13) | <0.001 | - | |
| NIV and MV (yes), n (%) | 12.58 (5.14, 30.82) | <0.001 | - | |
| HFO2 and NIV and MV (yes), n (%) | 34.82 (8.6, 140.84) | <0.001 | - | |
| Neuromuscular blockade (yes) | 9.73 (3.96, 23.90) | <0.001 | 1.93 (0.67, 5.54) | 0.222 |
| Prone position (yes) | 0.48 (0.30, 0.77) | 0.002 | 0.77 (0.41,1.46) | 0.426 |
| Treatment | ||||
| Corticosteroids (yes) | 1.91 (1.47, 2.48) | <0.001 | 1.69 (1.18, 2.43) | 0.004 |
| Hydroxychloroquine (yes) | 0.86 (0.65, 1.14) | 0.3 | - | - |
| Lopinavir/Ritonavir (yes) | 0.86 (0.65, 1.13) | 0.2 | - | - |
| Remdesivir (yes) | 1.69 (1.21, 2.35) | 0.002 | 1.28 (0.84, 1.94) | 0.252 |
| Tocilizumab (yes) | 1.50 (0.93, 2.40) | 0.09 | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrei, S.; Valeanu, L.; Stefan, M.G.; Longrois, D.; Popescu, M.; Stefan, G.; Balan, C.; Arafat, R.; Corneci, D.; Droc, G.; et al. Outcomes of COVID-19 Critically Ill Extremely Elderly Patients: Analysis of a Large, National, Observational Cohort. J. Clin. Med. 2022, 11, 1544. https://doi.org/10.3390/jcm11061544
Andrei S, Valeanu L, Stefan MG, Longrois D, Popescu M, Stefan G, Balan C, Arafat R, Corneci D, Droc G, et al. Outcomes of COVID-19 Critically Ill Extremely Elderly Patients: Analysis of a Large, National, Observational Cohort. Journal of Clinical Medicine. 2022; 11(6):1544. https://doi.org/10.3390/jcm11061544
Chicago/Turabian StyleAndrei, Stefan, Liana Valeanu, Mihai Gabriel Stefan, Dan Longrois, Mihai Popescu, Gabriel Stefan, Cosmin Balan, Raed Arafat, Dan Corneci, Gabriela Droc, and et al. 2022. "Outcomes of COVID-19 Critically Ill Extremely Elderly Patients: Analysis of a Large, National, Observational Cohort" Journal of Clinical Medicine 11, no. 6: 1544. https://doi.org/10.3390/jcm11061544
APA StyleAndrei, S., Valeanu, L., Stefan, M. G., Longrois, D., Popescu, M., Stefan, G., Balan, C., Arafat, R., Corneci, D., Droc, G., Bubenek-Turconi, S.-I., & on behalf of the COVATI-RO Collaborative. (2022). Outcomes of COVID-19 Critically Ill Extremely Elderly Patients: Analysis of a Large, National, Observational Cohort. Journal of Clinical Medicine, 11(6), 1544. https://doi.org/10.3390/jcm11061544