
Evaluation of the Proximal Tibia as a Donor Site of Cancellous Bone for Intraoral Grafting Procedures—A Retrospective Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Diagnostics and Pre-Surgical Procedures
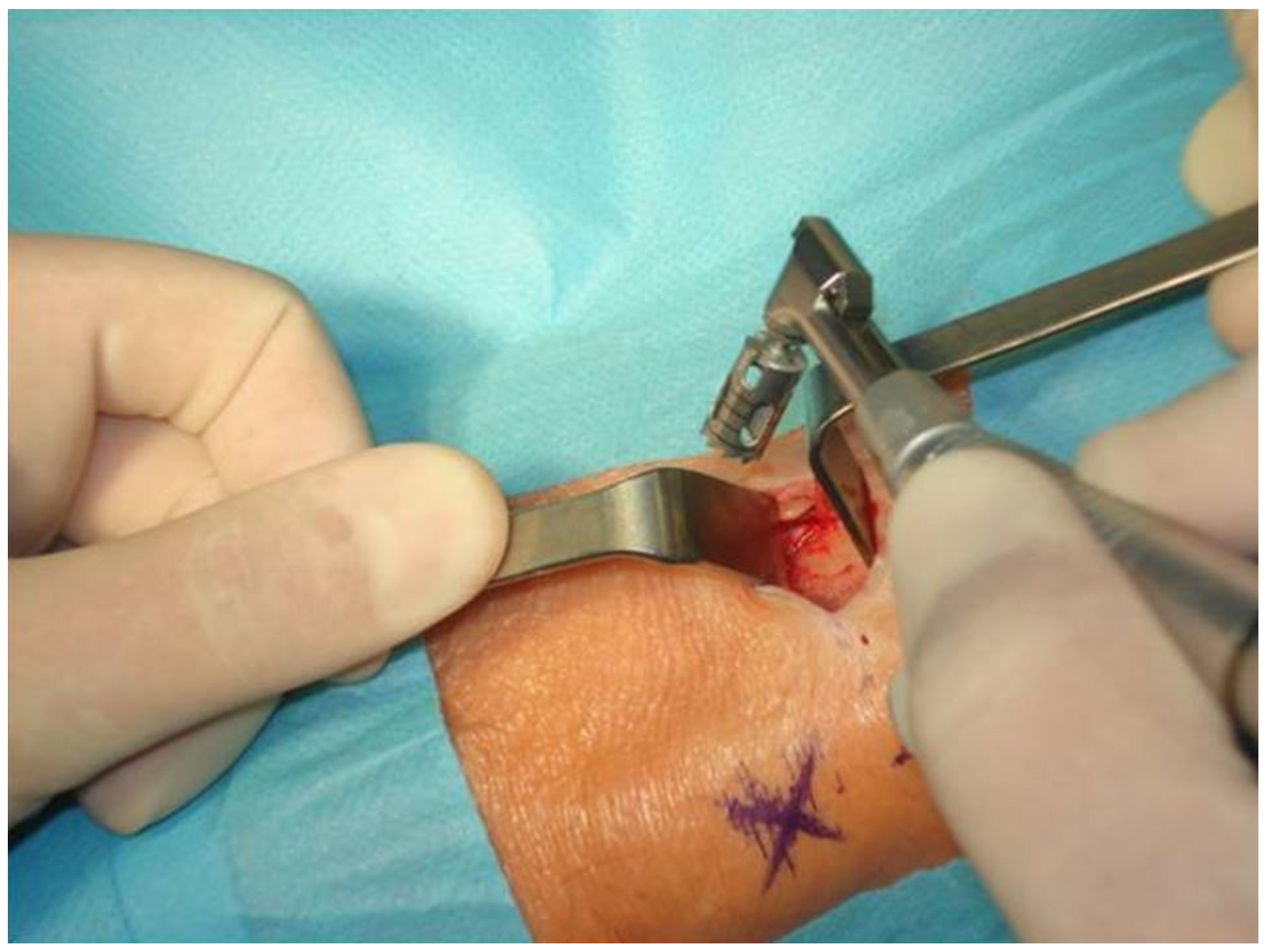
2.3. Surgical Protocol
2.4. Postoperative Care
2.5. Evaluated Parameters and Measurements
- (1)
- Calculation of the Body Mass Index (BMI) of the patients
- (2)
- The length of the skin incision
- (3)
- Surgery time from the skin incision until the end of the skin suturing
- (4)
- Surgery time from the bone opening with a trephine until the beginning of the suturing of the periosteum
- (5)
- A quantity of the harvested cancellous bone
- (6)
- Time from the surgery endpoint until patient mobilization (start of walking)
- (7)
- The number of consecutive days when the patient experienced pain at the donor site requiring the taking of painkillers
- (8)
- The number of consecutive days when the patient s limped
- (9)
- The number of consecutive days when the patient needed a walking aid (a walking stick)
- (10)
- Early complications (excessive and prolonged bleeding, hematoma requiring a surgical intervention, infection, wound dehiscence, wound suppuration)
- (11)
- Late complications (fractures of the tibia, aching, prolonged limping, lengthy healing time, scar, loss of sensation around the scar, swelling, and tenderness)
- (12)
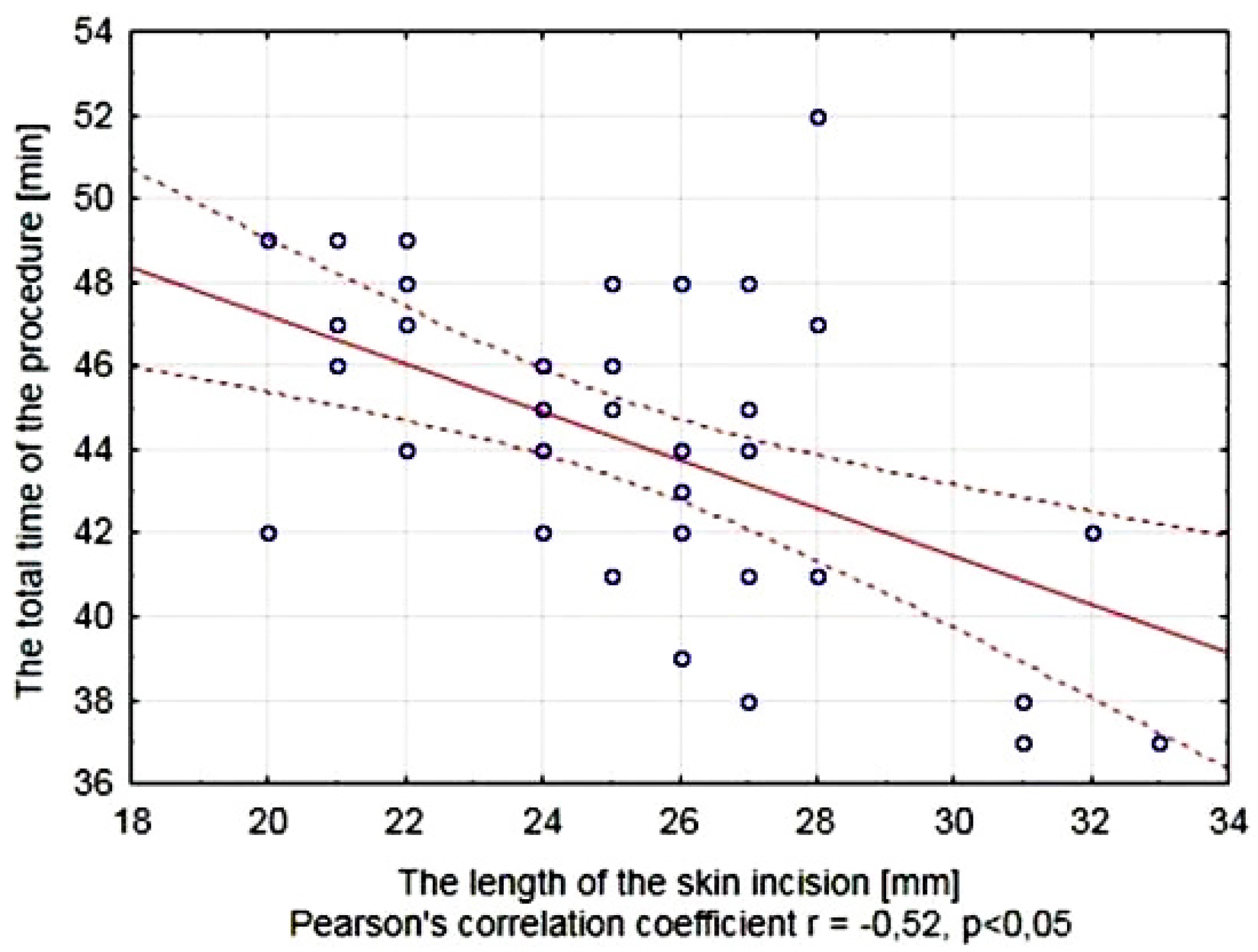
- Possible relationship between the length of the skin incision and the total time of the procedure of the bone harvesting from the proximal tibia
- (13)
- The survival rate of the graft after 6 months assessed on orthopantomograms.
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
- (1)
- The use of the proximal tibia as a donor site enables procurement of large amounts of cancellous bone (15.09 cc in average) and the medial approach to the bone is characterized by a relatively short surgery time (mean 44.12 min), short skin incisions (25.21 mm), and the lack of intraoperative complications.
- (2)
- Harvesting of the cancellous bone from the proximal tibia allows for early patient mobilization after surgery (average 5.4 h after the procedure), although gait disturbances were observed in 72.5% of patients which last for an average of 20.59 days and require the use of walking aids in 25.0% of patients for a mean period of 13.30 days with the use of analgesics for an average of 7.95 days.
- (3)
- The proximal tibia as a donor site for cancellous bone is characterized by a low risk of early and late complications, which include excessive bleeding, wound infection, lengthy healing time, scars, loss of sensation around the scars, aching, a dip in bone, swelling and tenderness.
- (4)
- The ability to obtain large amounts of cancellous bone and a low risk of intra- and postoperative complications make the proximal tibia an attractive donor site for the bone grafting procedures in maxillofacial surgery.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Araújo, M.G.; Lindhe, J. Dimensional Ridge Alterations Following Tooth Extraction. An Experimental Study in the Dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.-X.; Sun, C.-L.; Tian, Y.; Xu, W.-X.; Zhou, C.-L.; Xi, C.-Y.; Yan, J.-L.; Wang, X.-T. A Comparison of Osteocyte Bioactivity in Fine Particulate Bone Powder Grafts vs Larger Bone Grafts in a Rat Bone Repair Model. Acta Histochem. 2014, 116, 1015–1021. [Google Scholar] [CrossRef] [PubMed]
- Ettl, T.; Gosau, M.; Sader, R.; Reichert, T.E. Jaw Cysts—Filling or No Filling after Enucleation? A Review. J. Craniomaxillofac. Surg. 2012, 40, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Pradel, W.; Eckelt, U.; Lauer, G. Bone Regeneration after Enucleation of Mandibular Cysts: Comparing Autogenous Grafts from Tissue-Engineered Bone and Iliac Bone. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-Y.; Lee, J.; Kim, Y.-K. Comparative Analysis of Guided Bone Regeneration Using Autogenous Tooth Bone Graft Material with and without Resorbable Membrane. J. Dent. Sci. 2013, 8, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Castagna, L.; Polido, W.D.; Soares, L.G.; Tinoco, E.M.B. Tomographic Evaluation of Iliac Crest Bone Grafting and the Use of Immediate Temporary Implants to the Atrophic Maxilla. Int. J. Oral Maxillofac. Surg. 2013, 42, 1067–1072. [Google Scholar] [CrossRef]
- Kim, J.-W.; Cho, M.-H.; Kim, S.-J.; Kim, M.-R. Alveolar Distraction Osteogenesis versus Autogenous Onlay Bone Graft for Vertical Augmentation of Severely Atrophied Alveolar Ridges after 12 Years of Long-Term Follow-Up. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 540–549. [Google Scholar] [CrossRef]
- Rawashdeh, M.A.; Telfah, H. Secondary Alveolar Bone Grafting: The Dilemma of Donor Site Selection and Morbidity. Br. J. Oral Maxillofac. Surg. 2008, 46, 665–670. [Google Scholar] [CrossRef]
- Benlidayi, M.E.; Gaggl, A.; Buerger, H.; Kahraman, O.E.; Sencar, L.; Brandtner, C.; Kurkcu, M.; Polat, S.; Borumandi, F. Comparative Study of the Osseous Healing Process Following Three Different Techniques of Bone Augmentation in the Mandible: An Experimental Study. Int. J. Oral Maxillofac. Surg. 2014, 43, 1404–1410. [Google Scholar] [CrossRef]
- Balasundaram, I.; Al-Hadad, I.; Parmar, S. Recent Advances in Reconstructive Oral and Maxillofacial Surgery. Br. J. Oral Maxillofac. Surg. 2012, 50, 695–705. [Google Scholar] [CrossRef]
- Milinkovic, I.; Cordaro, L. Are There Specific Indications for the Different Alveolar Bone Augmentation Procedures for Implant Placement? A Systematic Review. Int. J. Oral Maxillofac. Surg. 2014, 43, 606–625. [Google Scholar] [CrossRef] [PubMed]
- De Freitas, R.M.; Spin-Neto, R.; Marcantonio Junior, E.; Pereira, L.A.V.D.; Wikesjö, U.M.E.; Susin, C. Alveolar Ridge and Maxillary Sinus Augmentation Using RhBMP-2: A Systematic Review. Clin. Implant Dent. Relat. Res. 2015, 17 (Suppl. 1), e192–e201. [Google Scholar] [CrossRef] [PubMed]
- Khojasteh, A.; Behnia, H.; Naghdi, N.; Esmaeelinejad, M.; Alikhassy, Z.; Stevens, M. Effects of Different Growth Factors and Carriers on Bone Regeneration: A Systematic Review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, e405–e423. [Google Scholar] [CrossRef] [PubMed]
- Basyuni, S.; Ferro, A.; Santhanam, V.; Birch, M.; McCaskie, A. Systematic Scoping Review of Mandibular Bone Tissue Engineering. Br. J. Oral Maxillofac. Surg. 2020, 58, 632–642. [Google Scholar] [CrossRef] [PubMed]
- Berstock, J.R.; Blom, A.W.; Beswick, A.D. A Systematic Review and Meta-Analysis of the Standard versus Mini-Incision Posterior Approach to Total Hip Arthroplasty. J. Arthroplast. 2014, 29, 1970–1982. [Google Scholar] [CrossRef]
- Kolomvos, N.; Iatrou, I.; Theologie-Lygidakis, N.; Tzerbos, F.; Schoinohoriti, O. Iliac Crest Morbidity Following Maxillofacial Bone Grafting in Children: A Clinical and Radiographic Prospective Study. J. Craniomaxillofac. Surg. 2010, 38, 293–302. [Google Scholar] [CrossRef]
- Fretwurst, T.; Gad, L.M.; Nelson, K.; Schmelzeisen, R. Dentoalveolar Reconstruction: Modern Approaches. Curr. Opin. Otolaryngol. Head Neck Surg. 2015, 23, 316–322. [Google Scholar] [CrossRef]
- Nikolopoulos, C.E.; Mavrogenis, A.F.; Petrocheilou, G.; Kokkinis, C.; Diamantopoulos, P.; Papagelopoulos, P.J. A Three-Dimensional Medical Imaging Model for Quantitative Assessment of Proximal Tibia vs. Anterior Iliac Crest Cancellous Bone. Knee 2008, 15, 233–237. [Google Scholar] [CrossRef]
- Bents, R.T. Ilioinguinal Neuralgia Following Anterior Iliac Crest Bone Harvesting. Orthopedics 2002, 25, 1389–1390. [Google Scholar] [CrossRef]
- Boyne, N.P.; Lambrianides, A.L.; Pollard, C. Incisional Hernia through Iliac Crest Bone Graft Donor Sites. ANZ J. Surg. 2002, 72, 156–157. [Google Scholar] [CrossRef]
- Danikas, D.; Theodorou, S.J.V.; Stratoulias, C.; Constantinopoulos, G.; Ginalis, E.M. Hernia through an Iliac Crest Bone-Graft Donor Site. Plast. Reconstr. Surg. 2002, 110, 1612–1613. [Google Scholar] [CrossRef] [PubMed]
- Mischkowski, R.A.; Selbach, I.; Neugebauer, J.; Koebke, J.; Zöller, J.E. Lateral Femoral Cutaneous Nerve and Iliac Crest Bone Grafts—Anatomical and Clinical Considerations. Int. J. Oral Maxillofac. Surg. 2006, 35, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Nkenke, E.; Weisbach, V.; Winckler, E.; Kessler, P.; Schultze-Mosgau, S.; Wiltfang, J.; Neukam, F.W. Morbidity of Harvesting of Bone Grafts from the Iliac Crest for Preprosthetic Augmentation Procedures: A Prospective Study. Int. J. Oral Maxillofac. Surg. 2004, 33, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Besly, W.; Ward Booth, P. Technique for Harvesting Tibial Cancellous Bone Modified for Use in Children. Br. J. Oral Maxillofac. Surg. 1999, 37, 129–133. [Google Scholar] [CrossRef]
- Ilankovan, V.; Stronczek, M.; Telfer, M.; Peterson, L.J.; Stassen, L.F.; Ward-Booth, P. A Prospective Study of Trephined Bone Grafts of the Tibial Shaft and Iliac Crest. Br. J. Oral Maxillofac. Surg. 1998, 36, 434–439. [Google Scholar] [CrossRef]
- Hughes, C.W.; Revington, P.J. The Proximal Tibia Donor Site in Cleft Alveolar Bone Grafting: Experience of 75 Consecutive Cases. J. Craniomaxillofac. Surg. 2002, 30, 12–16, discussion 17. [Google Scholar] [CrossRef]
- Miceli, A.L.C.; Pereira, L.C.; da Silva Torres, T.; Calasans-Maia, M.; Louro, R.S. Mandibular Reconstruction with Lateral Tibial Bone Graft: An Excellent Option for Oral and Maxillofacial Surgery. Craniomaxillofac. Trauma Reconstr. 2017, 10, 292–298. [Google Scholar] [CrossRef]
- Thor, A.; Farzad, P.; Larsson, S. Fracture of the Tibia: Complication of Bone Grafting to the Anterior Maxilla. Br. J. Oral Maxillofac. Surg. 2006, 44, 46–48. [Google Scholar] [CrossRef]
- Chen, C.-M.; Chen, P.-L.; Wu, C.-W.; Huang, I.-Y.; Lee, K.-T. Proximal Tibial Bone Harvesting under Local Anesthesia without Intravenous Sedation in the Dental Office: A Case Report. Kaohsiung J. Med. Sci. 2008, 24, 103–106. [Google Scholar] [CrossRef] [Green Version]
- Kirmeier, R.; Payer, M.; Lorenzoni, M.; Wegscheider, W.A.; Seibert, F.J.; Jakse, N. Harvesting of Cancellous Bone from the Proximal Tibia under Local Anesthesia: Donor Site Morbidity and Patient Experience. J. Oral Maxillofac. Surg. 2007, 65, 2235–2241. [Google Scholar] [CrossRef]
- Marchena, J.M.; Block, M.S.; Stover, J.D. Tibial Bone Harvesting under Intravenous Sedation: Morbidity and Patient Experiences. J. Oral Maxillofac. Surg. 2002, 60, 1151–1154. [Google Scholar] [CrossRef] [PubMed]
- de Graaf, I.M.; Oude Rengerink, K.; Wiersma, I.C.; Donker, M.E.; Mol, B.W.; Pajkrt, E. Techniques for Wound Closure at Caesarean Section: A Randomized Clinical Trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 165, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Eskes, A.M.; Brölmann, F.E.; van de Kar, A.L.; Niessen, F.B.; Lindeboom, R.; Ubbink, D.T.; Vermeulen, H. Values of Patients and Caregivers for Donor Site Scars: An Inter-Observer Analysis between Patients and Caregivers and Prediction of Cosmetic Satisfaction. Burns 2012, 38, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Rawashdeh, M.A. Morbidity of Iliac Crest Donor Site Following Open Bone Harvesting in Cleft Lip and Palate Patients. Int. J. Oral Maxillofac. Surg. 2008, 37, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Eufinger, H.; Leppänen, H. Iliac Crest Donor Site Morbidity Following Open and Closed Methods of Bone Harvest for Alveolar Cleft Osteoplasty. J. Craniomaxillofac. Surg. 2000, 28, 31–38. [Google Scholar] [CrossRef]
- Hashemi, H.M. Oblique Use of a Trephine Bur for the Harvesting of Tibial Bone Grafts. Br. J. Oral Maxillofac. Surg. 2008, 46, 690–691. [Google Scholar] [CrossRef]
- Vittayakittipong, P.; Nurit, W.; Kirirat, P. Proximal Tibial Bone Graft: The Volume of Cancellous Bone, and Strength of Decancellated Tibias by the Medial Approach. Int. J. Oral Maxillofac. Surg. 2012, 41, 531–536. [Google Scholar] [CrossRef]
- Noble, P.C.; Pflüger, G.; Junk-Jantsch, S.; Thompson, M.T.; Alexander, J.W.; Mathis, K.B. The Optimal Skin Incision for Minimally Invasive Total Hip Arthroplasty Performed via the Anterolateral Approach. J. Arthroplast. 2012, 27, 901–908. [Google Scholar] [CrossRef]
- Breivik, E.K.; Björnsson, G.A.; Skovlund, E. A Comparison of Pain Rating Scales by Sampling from Clinical Trial Data. Clin. J. Pain 2000, 16, 22–28. [Google Scholar] [CrossRef]
- Kager, A.N.; Marks, M.; Bastrom, T.; Newton, P.O. Morbidity of Iliac Crest Bone Graft Harvesting in Adolescent Deformity Surgery. J. Pediatr. Orthop. 2006, 26, 132–134. [Google Scholar] [CrossRef]
- Soohoo, N.F.; Cracchiolo, A. The Results of Utilizing Proximal Tibial Bone Graft in Reconstructive Procedures of the Foot and Ankle. Foot Ankle Surg. 2008, 14, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Mauffrey, C.; Madsen, M.; Bowles, R.J.; Seligson, D. Bone Graft Harvest Site Options in Orthopaedic Trauma: A Prospective in Vivo Quantification Study. Injury 2012, 43, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Mauffrey, C.P.C.; Seligson, D.; Krikler, S. Surgical Techniques: How I Do It? Bone Graft Harvest from the Proximal Lateral Tibia. Injury 2010, 41, 242–244. [Google Scholar] [CrossRef] [PubMed]
- Herford, A.S.; King, B.J.; Audia, F.; Becktor, J. Medial Approach for Tibial Bone Graft: Anatomic Study and Clinical Technique. J. Oral Maxillofac. Surg. 2003, 61, 358–363. [Google Scholar] [CrossRef] [Green Version]
- Dimitriou, R.; Mataliotakis, G.I.; Angoules, A.G.; Kanakaris, N.K.; Giannoudis, P.V. Complications Following Autologous Bone Graft Harvesting from the Iliac Crest and Using the RIA: A Systematic Review. Injury 2011, 42 (Suppl. 2), S3–S15. [Google Scholar] [CrossRef]
- Fasolis, M.; Boffano, P.; Ramieri, G. Morbidity Associated with Anterior Iliac Crest Bone Graft. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 586–591. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The Whole Group (n = 40) | |||
|---|---|---|---|
| Mean ± SD | Min | Max | |
| The length of the skin incision [mm] | 25.21 ± 3.23 | 20 | 33 |
| Surgery time from the skin incision until the end of the skin suturing [min] | 44.21 ± 3.59 | 37 | 52 |
| Surgery time from the bone opening until the beginning of the suturing [min] | 23.74 ± 3.01 | 19 | 29 |
| Soft tissue management time [min] | 20.47 ± 2.13 | 17 | 25 |
| Quantity of the harvested cancellous bone [cc] | 15.09 ± 3.75 | 8 | 21 |
| Women (n = 26) | Men (n = 14) | ||||||
|---|---|---|---|---|---|---|---|
| Mean ± SD | Min | Max | Mean ± SD | Min | Max | p-Level | |
| The length of the skin incision [mm] | 26.10 ± 3.03 | 21 | 33 | 23.36 ± 2.90 | 20 | 28 | 0.007 a* |
| Surgery time from the skin incision until the end of the skin suturing [min] | 44.17 ± 3.91 | 37 | 52 | 44.29 ± 2.95 | 39 | 49 | 0.924 a |
| Surgery time from the bone opening until the beginning of the suturing [min] | 23.93 ± 3.31 | 19 | 29 | 23.36 ± 2.34 | 20 | 28 | 0.564 a |
| Soft tissue management time [min] | 20.24 ± 1.96 | 18 | 25 | 20.93 ± 2.46 | 17 | 25 | 0.378 b |
| Quantity of the harvested cancellous bone [cc] | 15.28 ± 4.12 | 8 | 21 | 14.71 ± 2.92 | 9 | 20 | 0.337 b |
| The Whole Group (n = 40) | |||
|---|---|---|---|
| Mean ± SD | Min | Max | |
| Time from surgery endpoint until patient mobilization [h] | 5.40 ± 1.14 | 4 | 11 |
| No of days with pain at the donor site requiring pain killers | 7.95 ± 2.55 | 1 | 14 |
| The Whole Group (n = 40) | ||||
|---|---|---|---|---|
| No of Cases (%) | Mean ± SD | Min | Max | |
| No of days with limping | 29 (72.5%) | 20.59 ± 14.76 | 2 | 86 |
| No of days with a walking aid | 10 (25.0%) | 13.30 ± 4.30 | 7 | 21 |
| Problem | No of Cases |
|---|---|
| Excessive bleeding | 3 (7.5%) |
| Wound infection | 1 (2.5%) |
| Problem | No of Cases |
|---|---|
| Lengthy healing time | 1 (2.5%) |
| Scar | 5 (12.5%) |
| Loss of sensation around the scar | 1 (2.5%) |
| Aching | 2 (5.0%) |
| Dip in bone | 1 (2.5%) |
| Swelling and tenderness | 1 (2.5%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malara, P.; von Krockow, N.; Niedzielska, I.; Malara, B. Evaluation of the Proximal Tibia as a Donor Site of Cancellous Bone for Intraoral Grafting Procedures—A Retrospective Study. J. Clin. Med. 2022, 11, 1493. https://doi.org/10.3390/jcm11061493
Malara P, von Krockow N, Niedzielska I, Malara B. Evaluation of the Proximal Tibia as a Donor Site of Cancellous Bone for Intraoral Grafting Procedures—A Retrospective Study. Journal of Clinical Medicine. 2022; 11(6):1493. https://doi.org/10.3390/jcm11061493
Chicago/Turabian StyleMalara, Piotr, Nadine von Krockow, Iwona Niedzielska, and Beata Malara. 2022. "Evaluation of the Proximal Tibia as a Donor Site of Cancellous Bone for Intraoral Grafting Procedures—A Retrospective Study" Journal of Clinical Medicine 11, no. 6: 1493. https://doi.org/10.3390/jcm11061493
APA StyleMalara, P., von Krockow, N., Niedzielska, I., & Malara, B. (2022). Evaluation of the Proximal Tibia as a Donor Site of Cancellous Bone for Intraoral Grafting Procedures—A Retrospective Study. Journal of Clinical Medicine, 11(6), 1493. https://doi.org/10.3390/jcm11061493