
Is a Patient with Paget’s Disease of Bone Suitable for Living Kidney Donation?—Decision-Making in Lack of Clinical Evidence

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. General Approach to Living Kidney Donation Candidates
2.1. Balancing Donor Risks with Recipient Benefits
2.2. Kidney Function Requirements in Living Kidney Donors
2.3. Kidney Function Assessment in Living Kidney Donors
2.4. Beyond-the-Guidelines Requirements for Living Kidney Donation Candidates
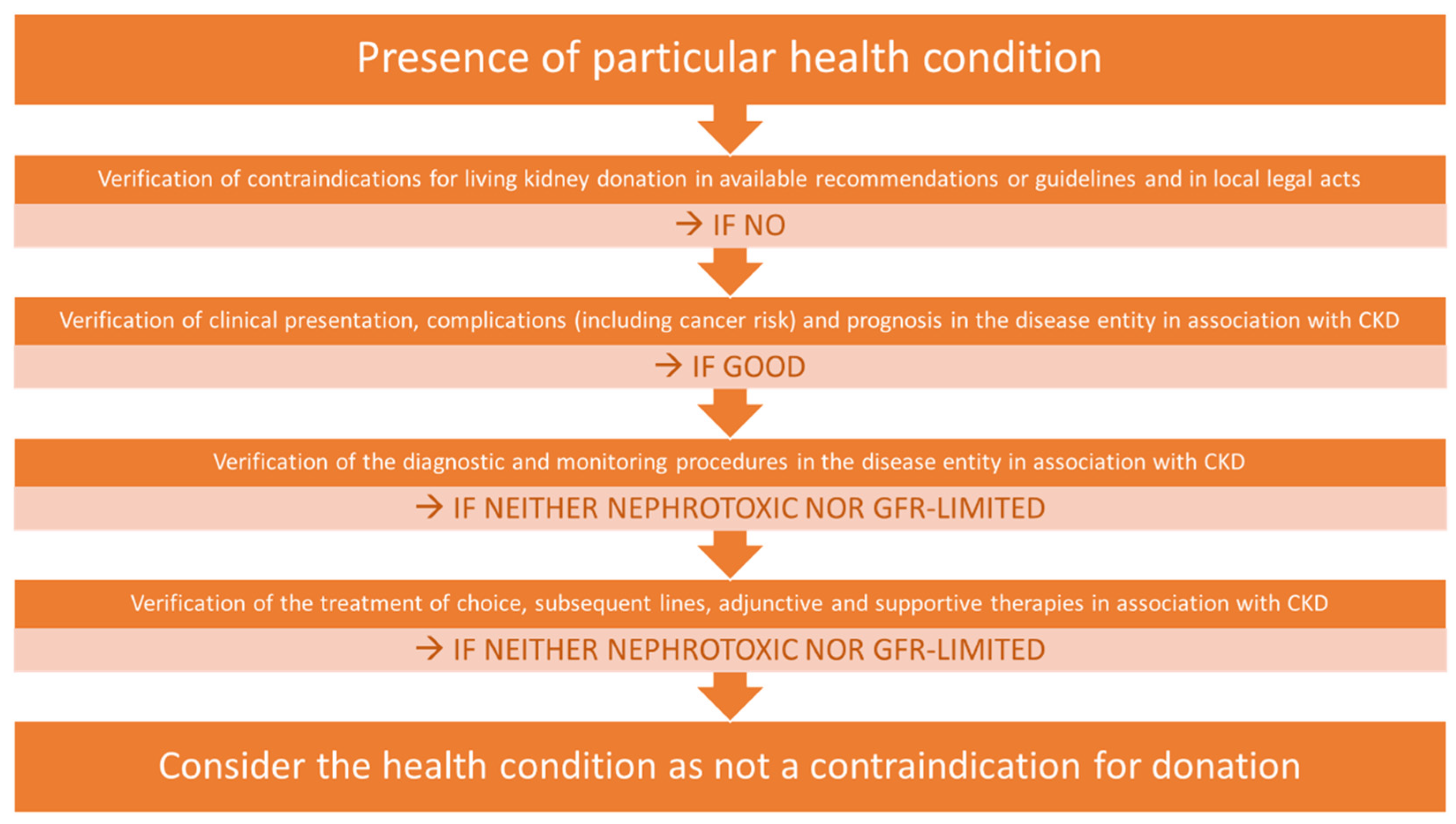
2.5. The Real-World Application of the Algorithm Used for Infrequent Pathologies in Potential Living Donors
3. The Clinical Approach Illustration
3.1. The Clinical Presentation of Paget’s Disease of Bone (PDB)
3.2. Risks Associated with Living Kidney Donation in the Context of PDB
3.3. PDB and Neoplastic Risk
3.4. Metabolic Complication and CKD Overlap
3.5. Further Diagnostics and Monitoring of PDB and CKD
3.6. CKD as an Armamentarium-Limiting Factor in PDB
3.7. Discussions on Kidney Donation from a Donor Suffering from PDB
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Andrews, P.A.; Burnapp, L. British Transplantation Society/Renal Association UK Guidelines for Living Donor Kidney Transplantation 2018: Summary of Updated Guidance. Transplantation 2018, 102, e307. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Kasiske, B.L.; Levey, A.S.; Adams, P.L.; Alberú, J.; Bakr, M.A.; Gallon, L.; Garvey, C.A.; Guleria, S.; Li, P.K.-T.; et al. KDIGO Clinical Practice Guideline on the Evaluation and Care of Living Kidney Donors. Transplantation 2017, 101, S7–S105. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). World Health Organisation Guiding Principles on Human Cell, Tissue and Organ Transplantation; WHO: Geneva, Switzerland, 2010; pp. 1–9. [Google Scholar]
- Lentine, K.L.; Kasiske, B.L.; Levey, A.S.; Adams, P.L.; Alberú, J.; Bakr, M.A.; Gallon, L.; Garvey, C.A.; Guleria, S.; Li, P.K.T.; et al. Summary of Kidney Disease: Improving Global Outcomes (KDIGO) Clinical Practice Guideline on the Evaluation and Care of Living Kidney Donors. Transplantation 2017, 101, 1783–1792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mariat, C.; Mjøen, G.; Watschinger, B.; Sever, M.S.; Crespo, M.; Peruzzi, L.; Oniscu, G.C.; Abramowicz, D.; Hilbrands, L.; Maggiore, U. Assessment of Pre-Donation Glomerular Filtration Rate: Going Back To Basics A Position Paper from the DESCARTES Working Group of the ERA-EDTA. Nephrol. Dial. Transplant. 2021, 37, 430–437. [Google Scholar] [CrossRef] [PubMed]
- The Consensus Statement of the Amsterdam Forum on the Care of the Live Kidney Donor. Transplantation 2004, 78, 491–492. [CrossRef] [PubMed]
- The Authors for the Live Organ Donor Consensus Group. Consensus Statement on the Live Organ Donor. JAMA J. Am. Med. Assoc. 2000, 284, 2919–2926. [Google Scholar] [CrossRef]
- Mandelbrot, D.A.; Reese, P.P.; Garg, N.; Thomas, C.P.; Rodrigue, J.R.; Schinstock, C.; Doshi, M.; Cooper, M.; Friedewald, J.; Naik, A.S.; et al. KDOQI US Commentary on the 2017 KDIGO Clinical Practice Guideline on the Evaluation and Care of Living Kidney Donors. Am. J. Kidney Dis. 2020, 75, 299–316. [Google Scholar] [CrossRef] [Green Version]
- Abramowicz, D.; Cochat, P.; Claas, F.; Dudley, C.; Harden, P.; Heeman, U.; Hourmant, M.; Maggiore, U.; Pascual, J.; Salvadori, M.; et al. Guideline. Nephrol. Dial. Transplant. 2013, 28, ii1–ii71. [Google Scholar] [CrossRef]
- Richardson, R.; Connelly, M.; Dipchand, C.; Garg, A.X.; Ghanekar, A.; Houde, I.; Johnston, O.; Mainra, R.; McCarrell, R.; Mueller, T.; et al. Kidney Paired Donation Protocol for Participating Donors 2014. Transplantation 2015, 99, S1–S88. [Google Scholar] [CrossRef]
- British Transplantation Society. Renal Association Guidelines for Living Donor Kidney Transplantation, 4th ed.; British Transplantation Society: Macclesfield, UK, 2018; Available online: https//bts.org.uk/wp-content/uploads/2018/07/FINAL_LDKT-guidelines_June-2018.pdf (accessed on 2 October 2020).
- Claisse, G.; Gaillard, F.; Mariat, C. Living kidney donor evaluation. Transplantation 2020, 104, 2487–2496. [Google Scholar] [CrossRef]
- Kulkarni, S.; Flescher, A.; Ahmad, M.; Bayliss, G.; Bearl, D.; Biondi, L.; Davis, E.; George, R.; Gordon, E.; Lyons, T.; et al. Ethical analysis examining the prioritisation of living donor transplantation in times of healthcare rationing. J. Med. Ethics 2022. [Google Scholar] [CrossRef] [PubMed]
- Mjøen, G.; Hallan, S.; Hartmann, A.; Foss, A.; Midtvedt, K.; Øyen, O.; Reisæter, A.; Pfeffer, P.; Jenssen, T.; Leivestad, T.; et al. Long-term risks for kidney donors. Kidney Int. 2014, 86, 162–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muzaale, A.D.; Massie, A.B.; Wang, M.C.; Montgomery, R.A.; McBride, M.A.; Wainright, J.L.; Segev, D.L. Risk of end-stage renal disease following live kidney donation. JAMA J. Am. Med. Assoc. 2014, 311, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, Y.; Yagisawa, T.; Sugihara, T.; Hara, K.; Takeshima, S.; Kubo, T.; Shinzato, T.; Shimizu, T.; Suzuki, M.; Maeshima, A.; et al. Clinical outcomes in donors and recipients of kidney transplantations involving medically complex living donors—A retrospective study. Transpl. Int. 2020, 33, 1417–1423. [Google Scholar] [CrossRef] [PubMed]
- Textor, S.C. Medically Complex Living Kidney Donors: Where Are We Now? Kidney Int. Rep. 2020, 5, 4–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiramitsu, T.; Tomosugi, T.; Futamura, K.; Okada, M.; Tsujita, M.; Goto, N.; Ichimori, T.; Narumi, S.; Takeda, A.; Watarai, Y. Preoperative Comorbidities and Outcomes of Medically Complex Living Kidney Donors. Kidney Int. Rep. 2020, 5, 13–27. [Google Scholar] [CrossRef] [Green Version]
- Duda, J. Civil Law Issues of Medical Transplantation, 1st ed.; LEX a Wolters Kluwer Business: Warszawa, Poland, 2011. [Google Scholar]
- Guzik-Makaruk, E.M. Transplantation of Organs, Tissues and Cells in Legal and Criminological Terms, 1st ed.; Temida 2-Wydawnictwo Stowarzyszenia Absolwentów Wydziału Prawa: Bialystok, Poland, 2008. [Google Scholar]
- Grams, M.E.; Sang, Y.; Levey, A.S.; Matsushita, K.; Ballew, S.; Chang, A.R.; Chow, E.K.H.; Kasiske, B.L.; Kovesdy, C.P.; Nadkarni, G.N.; et al. Kidney-Failure Risk Projection for the Living Kidney-Donor Candidate. N. Engl. J. Med. 2016, 374, 411–421. [Google Scholar] [CrossRef]
- Ibrahim, H.N.; Foley, R.N.; Reule, S.A.; Spong, R.; Kukla, A.; Issa, N.; Berglund, D.M.; Sieger, G.K.; Matas, A.J. Renal function profile in white kidney donors: The first 4 decades. J. Am. Soc. Nephrol. 2016, 27, 2885–2893. [Google Scholar] [CrossRef] [Green Version]
- Massie, A.B.; Muzaale, A.D.; Luo, X.; Chow, E.K.H.; Locke, J.E.; Nguyen, A.Q.; Henderson, M.L.; Snyder, J.J.; Segev, D.L. Quantifying postdonation risk of ESRD in living kidney donors. J. Am. Soc. Nephrol. 2017, 28, 2749–2755. [Google Scholar] [CrossRef]
- Ibrahim, H.N.; Foley, R.; Tan, L.; Rogers, T.; Bailey, R.F.; Guo, H.; Gross, C.R.; Matas, A.J. Long-Term Consequences of Kidney Donation. N. Engl. J. Med. 2009, 360, 459–469. [Google Scholar] [CrossRef] [Green Version]
- Fehrman-Ekholm, I.; Elinder, C.-G.; Stenbeck, M.; Tydén, G.; Groth, C.-G. Kidney donors live longer. Transplantation 1997, 64, 976–978. [Google Scholar] [CrossRef] [PubMed]
- Lenihan, C.R.; Busque, S.; Derby, G.; Blouch, K.; Myers, B.D.; Tan, J.C. Longitudinal study of living kidney donor glomerular dynamics after nephrectomy. J. Clin. Investig. 2015, 125, 1311–1318. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.X.; Muirhead, N.; Knoll, G.; Yang, R.C.; Prasad, G.V.R.; Thiessen-Philbrook, H.; Rosas-Arellano, M.P.; Housawi, A.; Boudville, N. Proteinuria and reduced kidney function in living kidney donors: A systematic review, meta-analysis, and meta-regression. Kidney Int. 2006, 70, 1801–1810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soveri, I.; Berg, U.B.; Björk, J.; Elinder, C.G.; Grubb, A.; Mejare, I.; Sterner, G.; Bäck, S.E. Measuring GFR: A systematic review. Am. J. Kidney Dis. 2014, 64, 411–424. [Google Scholar] [CrossRef] [PubMed]
- Szczurowska, A.; Guziński, M.; Krajewski, W.; Kamińska, D.; Kościelska-Kasprzak, K.; Arruza Echevarria, A.; Małkiewicz, B.; Dębinski, P.; Mazanowska, O.; Klinger, M.; et al. Preoperative Computed Tomography Parameters and Deterioration of Remaining Kidney Function in Living Donors. Transplant. Proc. 2018, 50, 1597–1601. [Google Scholar] [CrossRef]
- Rasała, J.; Szczot, M.; Kościelska-Kasprzak, K.; Szczurowska, A.; Poznański, P.; Mazanowska, O.; Małkiewicz, B.; Dębiński, P.; Krajewska, M.; Kamińska, D. Computed Tomography Parameters and Estimated Glomerular Filtration Rate Formulas for Peridonation Living Kidney Donor Assessment. Transplant. Proc. 2020, 52, 2278–2283. [Google Scholar] [CrossRef]
- Gozdowska, J.; Urbanowicz, A.; Sadowska, A.; Bieniasz, M.; Wszoła, M.; Kieszek, R.; Domagała, P.; Kwiatkowski, A.; Chmura, A.; Durlik, M. Glomerular filtration rate estimation in prospective living kidney donors: Preliminary Study. Transplant. Proc. 2014, 46, 2592–2597. [Google Scholar] [CrossRef]
- Mróz, J.; Białek, Ł.; Gozdowska, J.; Sadowska-Jakubowicz, A.; Czerwińska, K.; Durlik, M. Formulas Estimating Glomerular Filtration Rate in the Evaluation of Living Kidney Donor Candidates: Comparison of Different Formulas with Scintigraphy-Measured Glomerular Filtration Rate. Transplant. Proc. 2021, 53, 773–778. [Google Scholar] [CrossRef]
- Braddock, C.H. Supporting Shared Decision Making When Clinical Evidence Is Low. Med. Care Res. Rev. 2013, 70, 129S–140S. [Google Scholar] [CrossRef]
- Josse, R.G.; Hanley, D.A.; Kendler, D.; Ste Marie, L.-G.; Adachi, J.D.; Brown, J. Diagnosis and treatment of Paget’s disease of bone. Clin. Investig. Med. 2007, 30, 210. [Google Scholar] [CrossRef] [Green Version]
- Appelman-Dijkstra, N.M.; Papapoulos, S.E. Paget’s disease of bone. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Miladi, S.; Rouached, L.; Maatallah, K.; Rahmouni, S.; Fazaa, A.; Sellami, M.; Ferjani, H.; Kaffel, D.; Hamdi, W.; Abdelghani, K.B.; et al. Complications of Paget Bone Disease: A Study of 69 Patients. Curr. Rheumatol. Rev. 2021, 17, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Gogas Yavuz, D.; Ayturk, S.; Cetinkalp, S.; Bayraktar, F.; Kulaksizoglu, M.; Hekimsoy, Z.; Aydin, H.; Uygur, M.; Deniz, F.; Ipekci, S.; et al. Clinical and demographic aspects of Paget disease of bone: A multicentric study from Turkey. Eur. J. Rheumatol. 2021, 8, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.; Ralston, S.H. Clinical Presentation of Paget’s Disease: Evaluation of a Contemporary Cohort and Systematic Review. Calcif. Tissue Int. 2014, 95, 385–392. [Google Scholar] [CrossRef]
- Langston, A.L.; Campbell, M.K.; Fraser, W.D.; MacLennan, G.; Selby, P.; Ralston, S.H. Clinical Determinants of Quality of Life in Paget’s Disease of Bone. Calcif. Tissue Int. 2007, 80, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Corral-Gudino, L.; Borao-Cengotita-Bengoa, M.; Del Pino-Montes, J.; Ralston, S. Epidemiology of Paget’s disease of bone: A systematic review and meta-analysis of secular changes. Bone 2013, 55, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Van Staa, T.P.; Selby, P.; Leufkens, H.G.M.; Lyles, K.; Sprafka, J.M.; Cooper, C. Incidence and natural history of paget’s disease of bone in England and Wales. J. Bone Miner. Res. 2002, 17, 465–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanecki, K.; Nitsch-Osuch, A.; Goryński, P.; Bogdan, M.; Tarka, P.; Tyszko, P.Z. Paget disease of bone among hospitalized patients in Poland. Ann. Agric. Environ. Med. 2018, 25, 182–185. [Google Scholar] [CrossRef]
- Singer, F.R.; Bone, H.G.; Hosking, D.J.; Lyles, K.W.; Murad, M.H.; Reid, I.R.; Siris, E.S. Paget’s disease of bone: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2014, 99, 4408–4422. [Google Scholar] [CrossRef] [Green Version]
- Okumura, K.; Yamanaga, S.; Tanaka, K.; Kinoshita, K.; Kaba, A.; Fujii, M.; Ogata, M.; Hidaka, Y.; Toyoda, M.; Uekihara, S.; et al. Prediction model of compensation for contralateral kidney after living-donor donation. BMC Nephrol. 2019, 20, 283. [Google Scholar] [CrossRef] [Green Version]
- Lentine, K.L.; Lam, N.N.; Segev, D.L. Risks of living kidney donation: Current state of knowledge on outcomes important to donors. Clin. J. Am. Soc. Nephrol. 2019, 14, 597–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Małyszko, J.; Kozłowska, K.; Kozłowski, L.; Małyszko, J. Nephrotoxicity of anticancer treatment. Nephrol. Dial. Transplant. 2017, 32, 924–936. [Google Scholar] [CrossRef] [PubMed]
- Rendina, D.; De Filippo, G.; Merlotti, D.; Di Stefano, M.; Mingiano, C.; Giaquinto, A.; Evangelista, M.; Bo, M.; Arpino, S.; Faraonio, R.; et al. Increased Prevalence of Nephrolithiasis and Hyperoxaluria in Paget Disease of Bone. J. Clin. Endocrinol. Metab. 2020, 105, e4430–e4438. [Google Scholar] [CrossRef]
- Kumar, A.; Dash, A.; Kumar, P.; Prakash, M.; Tewari, V.; Sahni, H. Paget′s disease diagnosed on bone scintigraphy: Case report and literature review. Indian J. Nucl. Med. 2013, 28, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, Y.C.; Lu, C.L.; Lu, K.C. Mineral bone disorders in chronic kidney disease. Nephrology 2018, 23, 88–94. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.S.; Lee, D.H.; Youn, H.J. Calcium-phosphorus product concentration is a risk factor of coronary artery disease in metabolic syndrome. Atherosclerosis 2013, 229, 253–257. [Google Scholar] [CrossRef]
- Kasiske, B.L.; Kumar, R.; Kimmel, P.L.; Pesavento, T.E.; Kalil, R.S.; Kraus, E.S.; Rabb, H.; Posselt, A.M.; Anderson-Haag, T.L.; Steffes, M.W.; et al. Abnormalities in biomarkers of mineral and bone metabolism in kidney donors. Kidney Int. 2016, 90, 861–868. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Eum, S.H.; Ko, E.J.; Cho, H.J.; Yang, C.W.; Chung, B.H. Alterations in the Mineral Bone Metabolism of Living Kidney Donors After Uni-Nephrectomy: Prospective Observational Study. Front. Med. 2021, 8, 741944. [Google Scholar] [CrossRef]
- Young, A.; Hodsman, A.B.; Boudville, N.; Geddes, C.; Gill, J.; Goltzman, D.; Jassal, S.V.; Klarenbach, S.; Knoll, G.; Muirhead, N.; et al. Bone and Mineral Metabolism and Fibroblast Growth Factor 23 Levels After Kidney Donation. Am. J. Kidney Dis. 2012, 59, 761–769. [Google Scholar] [CrossRef]
- Naylor, K.L.; Garg, A.X. Bone health in living kidney donors. Curr. Opin. Urol. 2014, 24, 624–628. [Google Scholar] [CrossRef]
- Rotés-Sala, D.; Monfort, J.; Solano, A.; Miralles, E.; Vila, J.; Carbonell, J. The clover and heart signs in vertebral scintigraphic images are highly specific of Paget’s disease of bone. Bone 2004, 34, 605–608. [Google Scholar] [CrossRef] [PubMed]
- Love, C.; Din, A.S.; Tomas, M.B.; Kalapparambath, T.P.; Palestro, C.J. Radionuclide Bone Imaging: An Illustrative Review. RadioGraphics 2003, 23, 341–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherian, R.A.; Haddaway, M.J.; Davie, M.W.J.; McCall, I.W.; Cassar-Pullicino, V.N. Effect of Paget’s disease of bone on areal lumbar spine bone mineral density measured by DXA, and density of cortical and trabecular bone measured by quantitative CT. Br. J. Radiol. 2000, 73, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Davenport, M.S.; Perazella, M.A.; Yee, J.; Dillman, J.R.; Fine, D.; McDonald, R.J.; Rodby, R.A.; Wang, C.L.; Weinreb, J.C. Use of Intravenous Iodinated Contrast Media in Patients with Kidney Disease: Consensus Statements from the American College of Radiology and the National Kidney Foundation. Kidney Med. 2020, 2, 85–93. [Google Scholar] [CrossRef] [Green Version]
- Weinreb, J.C.; Rodby, R.A.; Yee, J.; Wang, C.L.; Fine, D.; McDonald, R.J.; Perazella, M.A.; Dillman, J.R.; Davenport, M.S. Use of Intravenous Gadolinium-Based Contrast Media in Patients with Kidney Disease: Consensus Statements from the American College of Radiology and the National Kidney Foundation. Kidney Med. 2021, 3, 142–150. [Google Scholar] [CrossRef]
- Woolen, S.A.; Shankar, P.R.; Gagnier, J.J.; MacEachern, M.P.; Singer, L.; Davenport, M.S. Risk of Nephrogenic Systemic Fibrosis in Patients with Stage 4 or 5 Chronic Kidney Disease Receiving a Group II Gadolinium-Based Contrast Agent: A Systematic Review and Meta-analysis. JAMA Intern. Med. 2020, 180, 223–230. [Google Scholar] [CrossRef]
- Lange, S.; Mędrzycka-Dąbrowska, W.; Zorena, K.; Dąbrowski, S.; Ślęzak, D.; Malecka-Dubiela, A.; Rutkowski, P. Nephrogenic systemic fibrosis as a complication after gadolinium-containing contrast agents: A rapid review. Int. J. Environ. Res. Public Health 2021, 18, 3000. [Google Scholar] [CrossRef]
- Schieda, N.; Blaichman, J.I.; Costa, A.F.; Glikstein, R.; Hurrell, C.; James, M.; Jabehdar Maralani, P.; Shabana, W.; Tang, A.; Tsampalieros, A.; et al. Gadolinium-Based Contrast Agents in Kidney Disease: Comprehensive Review and Clinical Practice Guideline Issued by the Canadian Association of Radiologists. Can. Assoc. Radiol. J. 2018, 69, 136–150. [Google Scholar] [CrossRef] [Green Version]
- Ralston, S.H.; Corral-Gudino, L.; Cooper, C.; Francis, R.M.; Fraser, W.D.; Gennari, L.; Guañabens, N.; Javaid, M.K.; Layfield, R.; O’Neill, T.W.; et al. Diagnosis and Management of Paget’s Disease of Bone in Adults: A Clinical Guideline. J. Bone Miner. Res. 2019, 34, 579–604. [Google Scholar] [CrossRef]
- Huvos, A.G. Osteogenic sarcoma of bones and soft tissues in older persons. A clinicopathologic analysis of 117 patients older than 60 years. Cancer 1986, 57, 1442–1449. [Google Scholar] [CrossRef]
- Singer, F.R. The evaluation and treatment of Paget’s disease of bone. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101506. [Google Scholar] [CrossRef] [PubMed]
- Ajh, T.; Pino-Montes, J.; Sh, R.; Corral-Gudino, L.; Tan, A.J.H.; Pino-Montes, J.; Ralston, S.H. Bisphosphonates for Paget’s disease of bone in adults (Review) Bisphosphonates for Paget’s disease of bone in adults. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef]
- Nairn, C.; Ralston, S.H. Paget’s disease of bone: When and why to refer to specialist care. Br. J. Gen. Pract. 2020, 70, 561–562. [Google Scholar] [CrossRef]
- Zhang, Y.; Gao, P.; Yan, S.; Zhang, Q.; Wang, O.; Jiang, Y.; Xing, X.; Xia, W.; Li, M. Clinical, Biochemical, Radiological, and Genetic Analyses of a Patient with VCP Gene Variant-Induced Paget’s Disease of Bone. Calcif. Tissue Int. 2021. [Google Scholar] [CrossRef] [PubMed]
- Reid, I.R.; Lyles, K.; Su, G.; Brown, J.P.; Walsh, J.P.; del Pino-Montes, J.; Miller, P.D.; Fraser, W.D.; Cafoncelli, S.; Bucci-Rechtweg, C.; et al. A single infusion of zoledronic acid produces sustained remissions in Paget disease: Data to 6.5 years. J. Bone Miner. Res. 2011, 26, 2261–2270. [Google Scholar] [CrossRef]
- Merlotti, D.; Gennari, L.; Martini, G.; Valleggi, F.; De Paola, V.; Avanzati, A.; Nuti, R. Comparison of Different Intravenous Bisphosphonate Regimens for Paget’s Disease of Bone. J. Bone Miner. Res. 2007, 22, 1510–1517. [Google Scholar] [CrossRef] [Green Version]
- Walsh, J.; Ward, L.; Stewart, G.; Will, R.; Criddle, R.; Prince, R.; Stuckey, B.G.; Dhaliwal, S.; Bhagat, C.; Retallack, R.; et al. A randomized clinical trial comparing oral alendronate and intravenous pamidronate for the treatment of Paget’s disease of bone. Bone 2004, 34, 747–754. [Google Scholar] [CrossRef]
- Tan, A.; Goodman, K.; Walker, A.; Hudson, J.; MacLennan, G.S.; Selby, P.L.; Fraser, W.D.; Ralston, S.H. Long-Term Randomized Trial of Intensive Versus Symptomatic Management in Paget’s Disease of Bone: The PRISM-EZ Study. J. Bone Miner. Res. 2017, 32, 1165–1173. [Google Scholar] [CrossRef]
- Rodríguez-Olleros Rodríguez, C.; Blanes Jacquart, D.; Arboiro Pinel, R.; de la Piedra Gordo, C.; Moro Álvarez, M.J.; Díaz Curiel, M. Long term effects on biochemical bone markers of a single infusion of zoledronic acid in Paget disease of bone. J. Orthop. Sci. 2020, 25, 715–718. [Google Scholar] [CrossRef]
- Marongiu, G.; Contini, A.; Lepri, A.C.; Donadu, M.; Verona, M.; Capone, A. The treatment of acute diaphyseal long-bones fractures with orthobiologics and pharmacological interventions for bone healing enhancement: A systematic review of clinical evidence. Bioengineering 2020, 7, 22. [Google Scholar] [CrossRef] [Green Version]
- Koch, F.P.; Wunsch, A.; Merkel, C.; Ziebart, T.; Pabst, A.; Said Yekta, S.; Blessmann, M.; Smeets, R. The influence of bisphosphonates on human osteoblast migration and integrin aVb3/tenascin C gene expression in vitro. Head Face Med. 2011, 7, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ott, S.M. Pharmacology of Bisphosphonates in Patients with Chronic Kidney Disease. Semin. Dial. 2015, 28, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.D. The kidney and bisphosphonates. Bone 2011, 49, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Ungprasert, P.; Cheungpasitporn, W.; Crowson, C.S.; Matteson, E.L. Individual non-steroidal anti-inflammatory drugs and risk of acute kidney injury: A systematic review and meta-analysis of observational studies. Eur. J. Intern. Med. 2015, 26, 285–291. [Google Scholar] [CrossRef]
- Lucas, G.N.C.; Leitão, A.C.C.; Alencar, R.L.; Xavier, R.M.F.; Daher, E.D.F.; Silva Junior, G.B. da Pathophysiological aspects of nephropathy caused by non-steroidal anti-inflammatory drugs. J. Bras. Nefrol. 2019, 41, 124–130. [Google Scholar] [CrossRef] [Green Version]
- Baker, M.; Perazella, M.A. NSAIDs in CKD: Are They Safe? Am. J. Kidney Dis. 2020, 76, 546–557. [Google Scholar] [CrossRef]
- Camin, R.M.G.; Cols, M.; Chevarria, J.L.; Osuna, R.G.; Carreras, M.; Lisbona, J.M.; Coderch, J. Acute kidney injury secondary to a combination of renin-angiotensin system inhibitors, diuretics and NSAIDS: “The Triple Whammy”. Nefrologia 2015, 35, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Lucas, G.J.; Riches, P.L.; Hocking, L.J.; Cundy, T.; Nicholson, G.C.; Walsh, J.P.; Ralston, S.H. Identification of a Major Locus for Paget’s Disease on Chromosome 10p13 in Families of British Descent. J. Bone Miner. Res. 2007, 23, 58–63. [Google Scholar] [CrossRef]
- Layfield, R. The molecular pathogenesis of Paget disease of bone. Expert Rev. Mol. Med. 2007, 9, 1–13. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Authors | Outcomes | Predonation Variables | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Predonation ESRD | Postdonation ESRD | Postdonation eGFR | Postdonation Proteinuria | Age | Gender | Race | Recipient Relation | Diabetes in Donor | Diabetes in Recipient | eGFR | Blood Pressure | Hypertension Meds | BMI | Smoking | UACR | Glycemia | |
| Grams et al. [22] | • | • | • | • | • | • | • | • | • | • | • | ||||||
| Ibrahim et al. [23] | • | • | • | • | • | • | • | • | • | • | • | • | |||||
| Massie et al. [24] | • | • | • | • | • | • | |||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poznański, P.; Lepiesza, A.; Jędrzejuk, D.; Mazanowska, O.; Bolanowski, M.; Krajewska, M.; Kamińska, D. Is a Patient with Paget’s Disease of Bone Suitable for Living Kidney Donation?—Decision-Making in Lack of Clinical Evidence. J. Clin. Med. 2022, 11, 1485. https://doi.org/10.3390/jcm11061485
Poznański P, Lepiesza A, Jędrzejuk D, Mazanowska O, Bolanowski M, Krajewska M, Kamińska D. Is a Patient with Paget’s Disease of Bone Suitable for Living Kidney Donation?—Decision-Making in Lack of Clinical Evidence. Journal of Clinical Medicine. 2022; 11(6):1485. https://doi.org/10.3390/jcm11061485
Chicago/Turabian StylePoznański, Paweł, Agnieszka Lepiesza, Diana Jędrzejuk, Oktawia Mazanowska, Marek Bolanowski, Magdalena Krajewska, and Dorota Kamińska. 2022. "Is a Patient with Paget’s Disease of Bone Suitable for Living Kidney Donation?—Decision-Making in Lack of Clinical Evidence" Journal of Clinical Medicine 11, no. 6: 1485. https://doi.org/10.3390/jcm11061485
APA StylePoznański, P., Lepiesza, A., Jędrzejuk, D., Mazanowska, O., Bolanowski, M., Krajewska, M., & Kamińska, D. (2022). Is a Patient with Paget’s Disease of Bone Suitable for Living Kidney Donation?—Decision-Making in Lack of Clinical Evidence. Journal of Clinical Medicine, 11(6), 1485. https://doi.org/10.3390/jcm11061485