
Effects of Anatomical or Non-Anatomical Resection of Hepatocellular Carcinoma on Survival Outcome


Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Surgical Technique and Decision Regarding the Extent of Resection
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. Patient Demographics and Clinical Characteristics
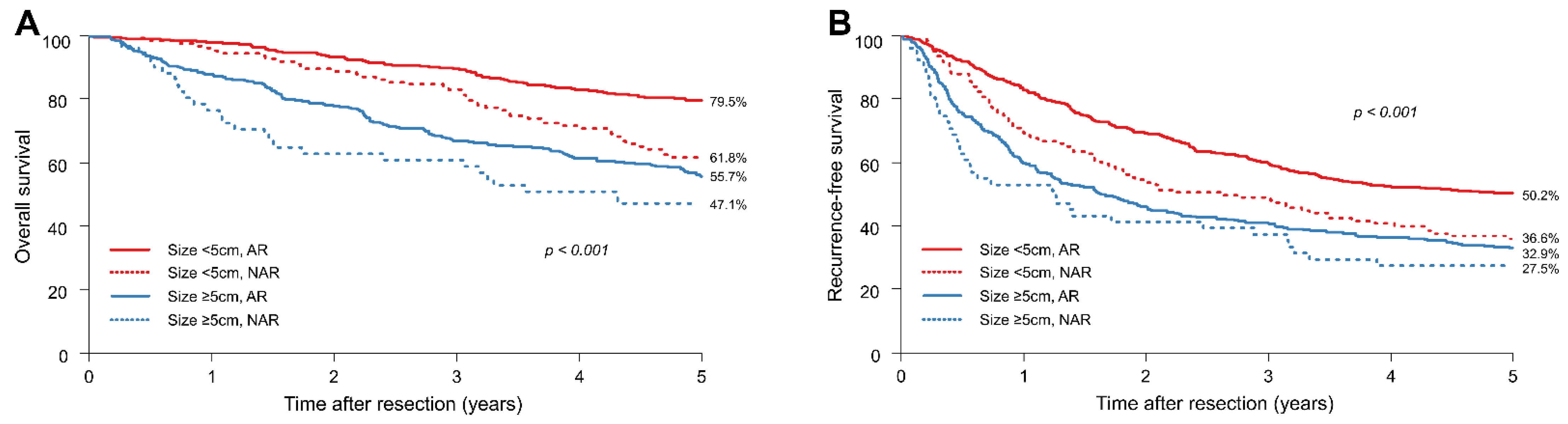
3.2. Survival Outcomes of the Entire Study Population
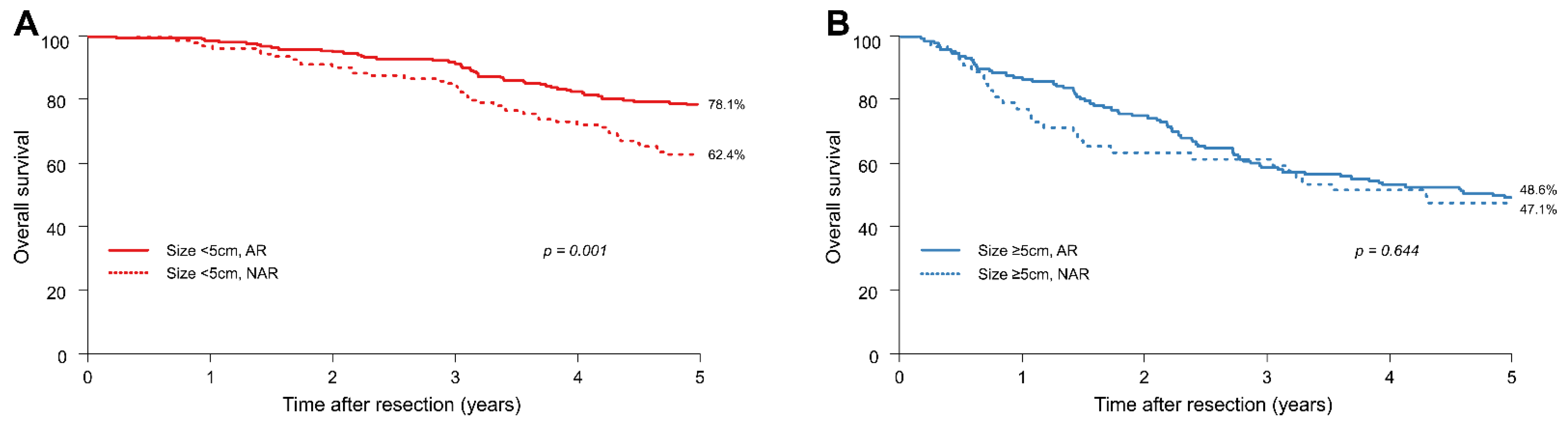
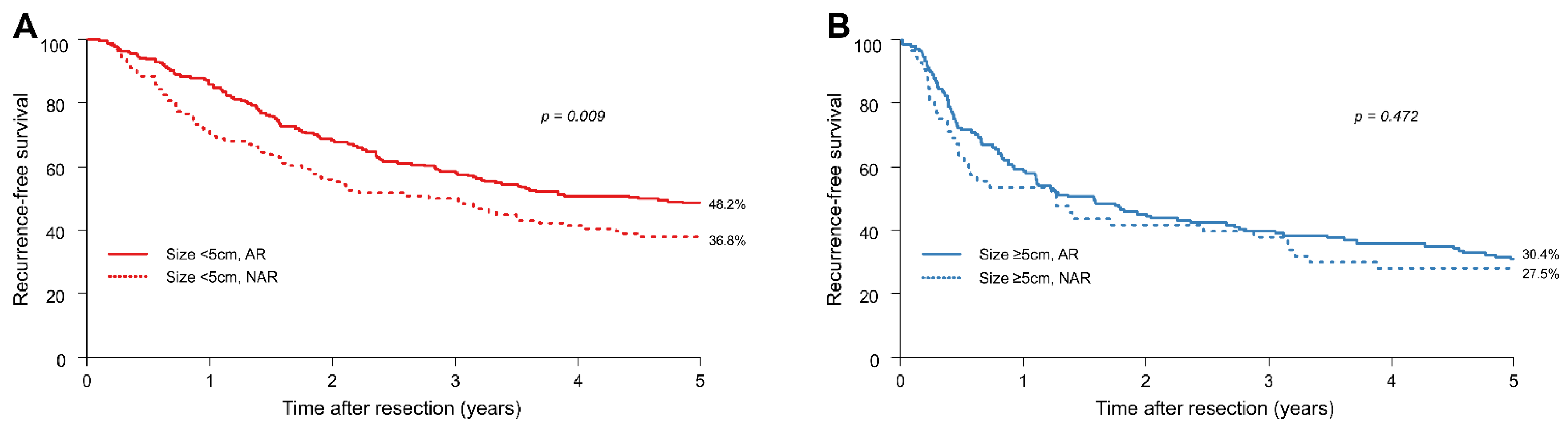
3.3. Survival Outcomes after PSM
3.4. Risk Factors for Survival Outcomes and Recurrence of HCC
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Global Burden of Disease Cancer Collaboration. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2017: A systematic analysis for the global burden of disease study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singal, A.G.; Lampertico, P.; Nahon, P. Epidemiology and surveillance for hepatocellular carcinoma: New trends. J. Hepatol. 2020, 72, 250–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American association for the study of liver diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kudo, M.; Kawamura, Y.; Hasegawa, K.; Tateishi, R.; Kariyama, K.; Shiina, S.; Toyoda, H.; Imai, Y.; Hiraoka, A.; Ikeda, M.; et al. Management of hepatocellular carcinoma in Japan: JSH consensus statements and recommendations 2021 update. Liver Cancer 2021, 10, 181–223. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, K.; Kokudo, N.; Imamura, H.; Matsuyama, Y.; Aoki, T.; Minagawa, M.; Sano, K.; Sugawara, Y.; Takayama, T.; Makuuchi, M. Prognostic impact of anatomic resection for hepatocellular carcinoma. Ann. Surg. 2005, 242, 252–259. [Google Scholar] [CrossRef]
- Takasaki, K. Glissonean pedicle transection method for hepatic resection: A new concept of liver segmentation. J. Hepatobiliary Pancreat. Surg. 1998, 5, 286–291. [Google Scholar] [CrossRef]
- Cucchetti, A.; Cescon, M.; Ercolani, G.; Bigonzi, E.; Torzilli, G.; Pinna, A.D. A comprehensive meta-regression analysis on outcome of anatomic resection versus nonanatomic resection for hepatocellular carcinoma. Ann. Surg. Oncol. 2012, 19, 3697–3705. [Google Scholar] [CrossRef]
- Jiao, S.; Li, G.; Zhang, D.; Xu, Y.; Liu, J.; Li, G. Anatomic versus non-anatomic resection for hepatocellular carcinoma, do we have an answer: A meta-analysis. Int. J. Surg. 2020, 80, 243–255. [Google Scholar] [CrossRef]
- Moris, D.; Tsilimigras, D.I.; Kostakis, I.D.; Ntanasis-Stathopoulos, I.; Shah, K.N.; Felekouras, E.; Pawlik, T.M. Anatomic versus non-anatomic resection for hepatocellular carcinoma: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2018, 44, 927–938. [Google Scholar] [CrossRef]
- Tan, Y.; Zhang, W.; Jiang, L.; Yang, J.; Yan, L. Efficacy and safety of anatomic resection versus nonanatomic resection in patients with hepatocellular carcinoma: A systemic review and meta-analysis. PLoS ONE 2017, 12, e0186930. [Google Scholar] [CrossRef]
- Zhou, Y.; Xu, D.; Wu, L.; Li, B. Meta-analysis of anatomic resection versus nonanatomic resection for hepatocellular carcinoma. Langenbecks Arch. Surg. 2011, 396, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Su, C.M.; Chou, C.C.; Yang, T.H.; Lin, Y.J. Comparison of anatomic and non-anatomic resections for very early-stage hepatocellular carcinoma: The importance of surgical resection margin width in non-anatomic resection. Surg. Oncol. 2021, 36, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Okamura, Y.; Ito, T.; Sugiura, T.; Mori, K.; Uesaka, K. Anatomic versus nonanatomic hepatectomy for a solitary hepatocellular carcinoma: A case-controlled study with propensity score matching. J. Gastrointest. Surg. 2014, 18, 1994–2002. [Google Scholar] [CrossRef] [PubMed]
- Marubashi, S.; Gotoh, K.; Akita, H.; Takahashi, H.; Ito, Y.; Yano, M.; Ishikawa, O.; Sakon, M. Anatomical versus non-anatomical resection for hepatocellular carcinoma. Br. J. Surg. 2015, 102, 776–784. [Google Scholar] [CrossRef]
- Lin, Y.J.; Ho, C.M. Is the rationale of anatomical liver resection for hepatocellular carcinoma universally adoptable: A hypothesis-driven review. Medicina 2021, 57, 131. [Google Scholar] [CrossRef]
- Li, S.Q.; Huang, T.; Shen, S.L.; Hua, Y.P.; Hu, W.J.; Kuang, M.; Peng, B.G.; Liang, L.J. Anatomical versus non-anatomical liver resection for hepatocellular carcinoma exceeding Milan criteria. Br. J. Surg. 2017, 104, 118–127. [Google Scholar] [CrossRef]
- Kang, K.J.; Ahn, K.S. Anatomical resection of hepatocellular carcinoma: A critical review of the procedure and its benefits on survival. World J. Gastroenterol. 2017, 23, 1139–1146. [Google Scholar] [CrossRef]
- Ju, M.; Yopp, A.C. The utility of anatomical liver resection in hepatocellular carcinoma: Associated with improved outcomes or lack of supportive evidence? Cancers 2019, 11, 1441. [Google Scholar] [CrossRef] [Green Version]
- Huang, S.W.; Chu, P.Y.; Ariizumi, S.; Lin, C.C.; Wong, H.P.; Chou, D.A.; Lee, M.T.; Wu, H.J.; Yamamoto, M. Anatomical versus non-anatomical resection for hepatocellular carcinoma, a propensity-matched analysis between Taiwanese and Japanese patients. In Vivo 2020, 34, 2607–2612. [Google Scholar] [CrossRef]
- Hidaka, M.; Eguchi, S.; Okuda, K.; Beppu, T.; Shirabe, K.; Kondo, K.; Takami, Y.; Ohta, M.; Shiraishi, M.; Ueno, S.; et al. Impact of anatomical resection for hepatocellular carcinoma with microportal invasion (vp1): A multi-institutional study by the Kyushu study group of liver surgery. Ann. Surg. 2020, 271, 339–346. [Google Scholar] [CrossRef] [Green Version]
- Kang, C.M.; Choi, G.H.; Kim, D.H.; Choi, S.B.; Kim, K.S.; Choi, J.S.; Lee, W.J. Revisiting the role of nonanatomic resection of small (<or = 4 cm) and single hepatocellular carcinoma in patients with well-preserved liver function. J. Surg. Res. 2010, 160, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Makuuchi, M.; Hasegawa, H.; Yamazaki, S. Ultrasonically guided subsegmentectomy. Surg. Gynecol. Obstet. 1985, 161, 346–350. [Google Scholar] [PubMed]
- Rahbari, N.N.; Garden, O.J.; Padbury, R.; Brooke-Smith, M.; Crawford, M.; Adam, R.; Koch, M.; Makuuchi, M.; Dematteo, R.P.; Christophi, C.; et al. Posthepatectomy liver failure: A definition and grading by the international study group of liver surgery (ISGLS). Surgery 2011, 149, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Centonze, L.; De Carlis, R.; Vella, I.; Carbonaro, L.; Incarbone, N.; Palmieri, L.; Sgrazzutti, C.; Ficarelli, A.; Valsecchi, M.G.; Dello Iacono, U.; et al. From LI-RADS Classification to HCC Pathology: A Retrospective Single-Institution Analysis of Clinico-Pathological Features Affecting Oncological Outcomes after Curative Surgery. Diagnostics 2022, 12, 160. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| NAR (n = 174) | AR (n = 812) | p-Value | |
|---|---|---|---|
| Age (years) | 54 (49–61) | 54 (47–61) | 0.296 |
| Sex | 0.081 | ||
| Male | 145 (83.3) | 628 (77.3) | |
| Female | 29 (16.7) | 184 (22.7) | |
| Child–Turcotte–Pugh class | 0.145 | ||
| A | 172 (98.9) | 810 (99.8) | |
| B | 2 (1.1) | 2 (0.2) | |
| Primary liver disease | 0.016 | ||
| HBV | 136 (78.2) | 642 (79.1) | |
| HCV | 17 (9.8) | 38 (4.7) | |
| NBNC | 21 (12.1) | 132 (16.3) | |
| ASA PS classification | 0.100 | ||
| Ⅰ | 21 (12.1) | 114 (14.0) | |
| Ⅱ | 127 (73.0) | 616 (75.9) | |
| Ⅲ | 26 (14.9) | 82 (10.1) | |
| Preoperative TACE | 44 (25.3) | 169 (20.8) | 0.193 |
| Preoperative laboratory result | |||
| AFP (ng/mL) | 30.0 (8.0–484.0) | 50.0 (6.0–657.0) | 0.591 |
| Platelet (×103/uL) | 135.50 (100.0–177.8) | 152.00 (119.0–195.3) | <0.001 |
| AST (IU/L) | 36.00 (29.0–50.8) | 36.00 (27.0–52.0) | 0.897 |
| ALT (IU/L) | 32.00 (22.0–43.0) | 33.00 (22.0–51.0) | 0.229 |
| Total bilirubin (mg/dL) | 0.90 (0.80–1.20) | 0.90 (0.70–1.10) | 0.008 |
| Albumin (g/dL) | 3.70 (3.5–4.0) | 3.80 (3.5–4.1) | 0.019 |
| PT (%) | 87.45 (78.2–95.9) | 90.40 (83.0–98.9) | <0.001 |
| PT (INR) | 1.08 (1.03–1.16) | 1.06 (1.01–1.11) | <0.001 |
| ICG R15 | 13.12 (8.5–19.1) | 11.38 (7.8–15.9) | 0.004 |
| Operation time (min) | 171.00 (135.0–215.0) | 180.00 (150.0–225.3) | 0.003 |
| Postoperative hospital stay (days) | 13.00 (12.0–16.0) | 14.00 (12.0–17.0) | 0.306 |
| Postoperative complication | 21 (12.1) | 99 (12.2) | 0.964 |
| Pathology | |||
| Maximum tumour size (cm) | 3.5 (2.4–5.0) | 4.2 (2.8–7.0) | <0.001 |
| Number of tumours | 0.215 | ||
| Solitary | 147 (84.5) | 714 (87.9) | |
| Multiple | 27 (15.5) | 98 (12.1) | |
| Edmondson–Steiner grade | 0.093 | ||
| I–II | 78 (44.8) | 421 (51.8) | |
| III–IV | 96 (55.2) | 391 (48.2) | |
| Macrovascular invasion | 19 (10.9) | 114 (14.0) | 0.274 |
| Microvascular invasion | 25 (14.4) | 150 (18.5) | 0.198 |
| Total Set | Matched Set * | ||||||
|---|---|---|---|---|---|---|---|
| Tumour Size < 5 cm | NAR Group | AR Group | p-Value | SMD | NAR Group | AR Group | SMD |
| n = 123 | n = 478 | n = 117 | n = 224 | ||||
| Age | |||||||
| <50 years | 31 (25.2) | 149 (31.2) | 0.433 | 0.133 | 31 (26.5) | 68 (30.4) | 0.100 |
| 50–60 years | 59 (48.0) | 209 (43.7) | 56 (47.9) | 97 (43.3) | |||
| >60 years | 33 (26.8) | 120 (25.1) | 30 (25.6) | 59 (26.3) | |||
| Sex (male/female) | 103 (83.7%)/20 | 368 (77.0%)/110 | 0.105 | 0.171 | 97 (82.9%)/20 | 180 (80.4%)/44 | 0.066 |
| Primary liver disease | |||||||
| HBV | 92 (74.8) | 395 (82.6) | 0.032 | 0.241 | 89 (76.1) | 175 (78.1) | 0.051 |
| HCV | 15 (12.2) | 27 (5.6) | 13 (11.1) | 22 (9.8) | |||
| NBNC | 16 (13.0) | 56 (11.7) | 15 (12.8) | 27 (12.1) | |||
| Preoperative TACE | 27 (22.0) | 97 (20.3) | 0.685 | 0.041 | 24 (20.5) | 55 (24.6) | 0.097 |
| AFP (ng/mL) | |||||||
| <100 | 80 (65.0) | 294 (61.5) | 0.771 | 0.073 | 76 (65.0) | 139 (62.1) | 0.062 |
| 100–1000 | 27 (22.0) | 116 (24.3) | 25 (21.4) | 51 (22.8) | |||
| >1000 | 16 (13.0) | 68 (14.2) | 16 (13.7) | 34 (15.2) | |||
| Platelet | |||||||
| <150 | 77 (62.6) | 290 (60.7) | 0.695 | 0.040 | 73 (62.4) | 131 (58.5) | 0.080 |
| ≥150 | 46 (37.4) | 188 (39.3) | 44 (37.6) | 93 (41.5) | |||
| Log-transformed AST | 3.62 ± 0.45 | 3.59 ± 0.42 | 0.498 | 0.067 | 3.62 ± 0.45 | 3.61 ± 0.43 | 0.025 |
| Total bilirubin | |||||||
| <1.5 | 110 (89.4) | 444 (92.9) | 0.203 | 0.122 | 106 (90.6) | 207 (92.4) | 0.065 |
| ≥1.5 | 13 (10.6) | 34 (7.1) | 11 (9.4) | 17 (7.6) | |||
| Albumin | 3.70 ± 0.41 | 3.80 ± 0.39 | 0.008 | 0.265 | 3.73 ± 0.38 | 3.76 ± 0.38 | 0.073 |
| PT (INR) | 1.10 ± 0.10 | 1.28 ± 4.43 | 0.669 | 0.055 | 1.10 ± 0.09 | 1.09 ± 0.09 | 0.057 |
| ICG R15 | |||||||
| <15 | 74 (60.2) | 341 (71.3) | 0.017 | 0.237 | 74 (63.2) | 144 (64.3) | 0.022 |
| ≥15 | 49 (39.8) | 137 (28.7) | 43 (36.8) | 80 (35.7) | |||
| Number of tumours | |||||||
| Solitary | 107 (87.0) | 428 (89.5) | 0.420 | 0.079 | 104 (88.9) | 191 (85.3) | 0.108 |
| Multiple | 16 (13.0) | 50 (10.5) | 13 (11.1) | 33 (14.7) | |||
| Macrovascular invasion | 9 (7.3) | 34 (7.1) | 0.938 | 0.008 | 8 (6.8) | 13 (5.8) | 0.043 |
| Microvascular invasion | 11 (8.9) | 47 (9.8) | 0.766 | 0.031 | 10 (8.5) | 20 (8.9) | 0.014 |
| Edmondson–Steiner grade | |||||||
| I–II | 60 (48.8) | 273 (57.1) | 0.097 | 0.168 | 58 (49.6) | 112 (50.0) | 0.009 |
| III–IV | 63 (51.2) | 205 (42.9) | 59 (50.4) | 112 (50.0) | |||
| Total Set | Matched Set * | ||||||
|---|---|---|---|---|---|---|---|
| Tumour Size ≥ 5 cm | NAR Group | AR Group | p-Value | SMD | NAR Group | AR Group | SMD |
| n = 51 | n = 334 | n = 51 | n = 148 | ||||
| Age | |||||||
| <50 years | 16 (31.4) | 117 (35.0) | 0.711 | 0.123 | 16 (31.4) | 46 (31.1) | 0.033 |
| 50–60 years | 22 (43.1) | 124 (37.1) | 22 (43.1) | 66 (44.6) | |||
| >60 years | 13 (25.5) | 93 (27.8) | 13 (25.5) | 36 (24.3) | |||
| Sex (male/female) | 42 (82.4%)/9 | 260 (77.8%)/74 | 0.466 | 0.113 | 42 (82.4%)/9 | 119 (80.4%)/29 | 0.050 |
| Primary liver disease | |||||||
| HBV | 44 (86.3) | 247 (74.0) | 0.107 | 0.356 | 44 (86.3) | 127 (85.8) | 0.041 |
| HCV | 2 (3.9) | 11 (3.3) | 2 (3.9) | 7 (4.7) | |||
| NBNC | 5 (9.8) | 76 (22.8) | 5 (9.8) | 14 (9.5) | |||
| Preoperative TACE | 17 (33.3) | 72 (21.6) | 0.063 | 0.266 | 17 (33.3) | 50 (33.8) | 0.010 |
| AFP (ng/mL) | |||||||
| <100 | 28 (54.9) | 163 (48.8) | 0.054 | 0.384 | 28 (54.9) | 80 (54.1) | 0.070 |
| 100–1000 | 14 (27.5) | 60 (18.0) | 14 (27.5) | 38 (25.7) | |||
| >1000 | 9 (17.6) | 111 (33.2) | 9 (17.6) | 30 (20.3) | |||
| Platelet | |||||||
| <150 | 27 (52.9) | 109 (32.6) | 0.005 | 0.419 | 27 (52.9) | 71 (48.0) | 0.099 |
| ≥150 | 24 (47.1) | 225 (67.4) | 24 (47.1) | 77 (52.0) | |||
| Log-transformed AST | 3.77 (0.50) | 3.77 (0.57) | 0.988 | 0.002 | 3.77 (0.50) | 3.80 (0.59) | 0.055 |
| Total bilirubin | |||||||
| <1.5 | 49 (96.1) | 311 (93.1) | 0.424 | 0.131 | 49 (96.1) | 140 (94.6) | 0.070 |
| ≥1.5 | 2 (3.9) | 23 (6.9) | 2 (3.9) | 8 (5.4) | |||
| Albumin | 3.67 (0.45) | 3.74 (0.44) | 0.344 | 0.140 | 3.67 (0.45) | 3.66 (0.46) | 0.042 |
| PT (INR) | 1.08 (0.09) | 1.06 (0.09) | 0.052 | 0.286 | 1.08 (0.09) | 1.08 (0.09) | 0.022 |
| ICG R15 | |||||||
| <15 | 32 (62.7) | 235 (70.4) | 0.272 | 0.162 | 32 (62.7) | 90 (60.8) | 0.040 |
| ≥15 | 19 (37.3) | 99 (29.6) | 19 (37.3) | 58 (39.2) | |||
| Number of tumours | |||||||
| Solitary | 40 (78.4) | 286 (85.6) | 0.184 | 0.188 | 40 (78.4) | 121 (81.8) | 0.083 |
| Multiple | 11 (21.6) | 48 (14.4) | 11 (21.6) | 27 (18.2) | |||
| Macrovascular invasion | 10 (19.6) | 80 (24.0) | 0.495 | 0.105 | 10 (19.6) | 28 (18.9) | 0.017 |
| Microvascular invasion | 14 (27.5) | 103 (30.8) | 0.624 | 0.075 | 14 (27.5) | 44 (29.7) | 0.050 |
| Edmondson–Steiner grade | |||||||
| I–II | 18 (35.3) | 148 (44.3) | 0.226 | 0.185 | 18 (35.3) | 51 (34.5) | 0.018 |
| III–IV | 33 (64.7) | 186 (55.7) | 33 (64.7) | 97 (65.5) | |||
| Tumour Size < 5 cm | Tumour Size ≥ 5 cm | ||||
|---|---|---|---|---|---|
| Multivariate Cox Analysis | Multivariate Cox Analysis | ||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| AR | 0.54 (0.37–0.77) | 0.001 | 0.84 (0.53–1.32) | 0.439 | |
| Age (years) | 50–60 years | 0.88 (0.57–1.34) | 0.540 | 0.73 (0.49–1.08) | 0.115 |
| >60 years | 1.28 (0.79–2.09) | 0.319 | 0.84 (0.54–1.29) | 0.421 | |
| Sex | Female | 0.77 (0.49–1.21) | 0.251 | 0.78 (0.52–1.16) | 0.219 |
| Primary disease | HCV | 1.35 (0.74–2.45) | 0.322 | 1.59 (0.75–3.37) | 0.227 |
| NBNC | 0.91 (0.51–1.62) | 0.746 | 0.90 (0.58–1.41) | 0.642 | |
| Preoperative TACE | Yes | 1.43 (0.96–2.11) | 0.076 | 1.20 (0.83–1.73) | 0.332 |
| AFP (ng/mL) | 100–1000 | 1.36 (0.90–2.06) | 0.147 | 0.96 (0.62–1.50) | 0.856 |
| >1000 | 1.39 (0.86–2.24) | 0.180 | 1.07 (0.71–1.61) | 0.735 | |
| Platelet | ≥150 | 0.78 (0.53–1.14) | 0.190 | 0.74 (0.54–1.02) | 0.07 |
| Log-transformed AST | 1.88 (1.29–2.76) | 0.001 | 1.24 (0.90–1.69) | 0.185 | |
| Total bilirubin | ≥1.5 | 1.29 (0.73–2.30) | 0.382 | 1.73 (0.99–3.01) | 0.053 |
| Albumin | 0.62 (0.39–0.99) | 0.044 | 0.81 (0.55–1.19) | 0.276 | |
| PT (INR) | 0.96 (0.80–1.15) | 0.636 | 0.61 (0.08–4.70) | 0.632 | |
| ICG R15 | ≥15 | 1.06 (0.72–1.56) | 0.774 | 1.20 (0.83–1.72) | 0.337 |
| Number of tumours | Multiple | 2.23 (1.46–3.41) | <0.001 | 2.25 (1.54–3.28) | <0.001 |
| Macrovascular invasion | 2.00 (0.72–5.60) | 0.186 | 1.13 (0.61–2.07) | 0.7 | |
| Microvascular invasion | 1.61 (0.62–4.15) | 0.327 | 1.77 (0.98–3.20) | 0.058 | |
| Edmondson–Steiner grade | III–IV | 1.57 (1.11–2.21) | 0.011 | 1.26 (0.88–1.79) | 0.203 |
| Tumour Size < 5 cm | Tumour Size ≥ 5 cm | ||||
|---|---|---|---|---|---|
| Multivariate Cox Analysis | Multivariate Cox Analysis | ||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| AR | 0.69 (0.53–0.90) | 0.006 | 0.93 (0.64–1.35) | 0.707 | |
| Age (years) | 50–60 years | 0.86 (0.65–1.15) | 0.312 | 0.77 (0.55–1.06) | 0.106 |
| >60 years | 1.26 (0.90–1.75) | 0.173 | 0.89 (0.62–1.27) | 0.518 | |
| Sex | Female | 0.53 (0.38–0.73) | <0.001 | 0.69 (0.50–0.96) | 0.030 |
| Primary disease | HCV | 1.04 (0.67–1.61) | 0.857 | 2.07 (1.14–3.76) | 0.016 |
| NBNC | 0.73 (0.49–1.10) | 0.135 | 0.74 (0.52–1.06) | 0.104 | |
| Preoperative TACE | Yes | 1.29 (0.98–1.70) | 0.068 | 1.14 (0.84–1.55) | 0.384 |
| AFP (ng/mL) | 100–1000 | 1.25 (0.95–1.65) | 0.110 | 0.91 (0.62–1.32) | 0.608 |
| >1000 | 0.98 (0.69–1.40) | 0.915 | 1.14 (0.82–1.58) | 0.426 | |
| Platelet | ≥150 | 0.80 (0.62–1.03) | 0.078 | 0.66 (0.51–0.86) | 0.002 |
| Log-transformed AST | 1.48 (1.13–1.94) | 0.005 | 1.48 (1.14–1.91) | 0.003 | |
| Total bilirubin | ≥1.5 | 0.94 (0.62–1.42) | 0.778 | 1.50 (0.91–2.49) | 0.112 |
| Albumin | 0.56 (0.41–0.77) | <0.001 | 0.82 (0.59–1.14) | 0.227 | |
| PT (INR) | 0.96 (0.84–1.09) | 0.503 | 0.13 (0.02–0.71) | 0.019 | |
| ICG R15 | ≥15 | 1.00 (0.77–1.29) | 0.981 | 1.22 (0.89–1.66) | 0.214 |
| Number of tumours | Multiple | 1.48 (1.08–2.04) | 0.015 | 2.20 (1.58–3.06) | <0.001 |
| Macrovascular invasion | 1.53 (0.71–3.30) | 0.282 | 1.24 (0.71–2.16) | 0.448 | |
| Microvascular invasion | 1.40 (0.70–2.82) | 0.340 | 1.17 (0.69–1.99) | 0.554 | |
| Edmondson–Steiner grade | III–IV | 1.21 (0.96–1.52) | 0.112 | 1.06 (0.80–1.41) | 0.661 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, J.H.; Lee, J.-W.; Lee, J.W.; Lee, Y.J. Effects of Anatomical or Non-Anatomical Resection of Hepatocellular Carcinoma on Survival Outcome. J. Clin. Med. 2022, 11, 1369. https://doi.org/10.3390/jcm11051369
Kwon JH, Lee J-W, Lee JW, Lee YJ. Effects of Anatomical or Non-Anatomical Resection of Hepatocellular Carcinoma on Survival Outcome. Journal of Clinical Medicine. 2022; 11(5):1369. https://doi.org/10.3390/jcm11051369
Chicago/Turabian StyleKwon, Jae Hyun, Jung-Woo Lee, Jong Woo Lee, and Young Joo Lee. 2022. "Effects of Anatomical or Non-Anatomical Resection of Hepatocellular Carcinoma on Survival Outcome" Journal of Clinical Medicine 11, no. 5: 1369. https://doi.org/10.3390/jcm11051369
APA StyleKwon, J. H., Lee, J.-W., Lee, J. W., & Lee, Y. J. (2022). Effects of Anatomical or Non-Anatomical Resection of Hepatocellular Carcinoma on Survival Outcome. Journal of Clinical Medicine, 11(5), 1369. https://doi.org/10.3390/jcm11051369