Testing for Vitamin D in High-Risk COPD in Outpatient Clinics in Spain: A Cross-Sectional Analysis of the VITADEPOC Study

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
Variable Selection
3. Results
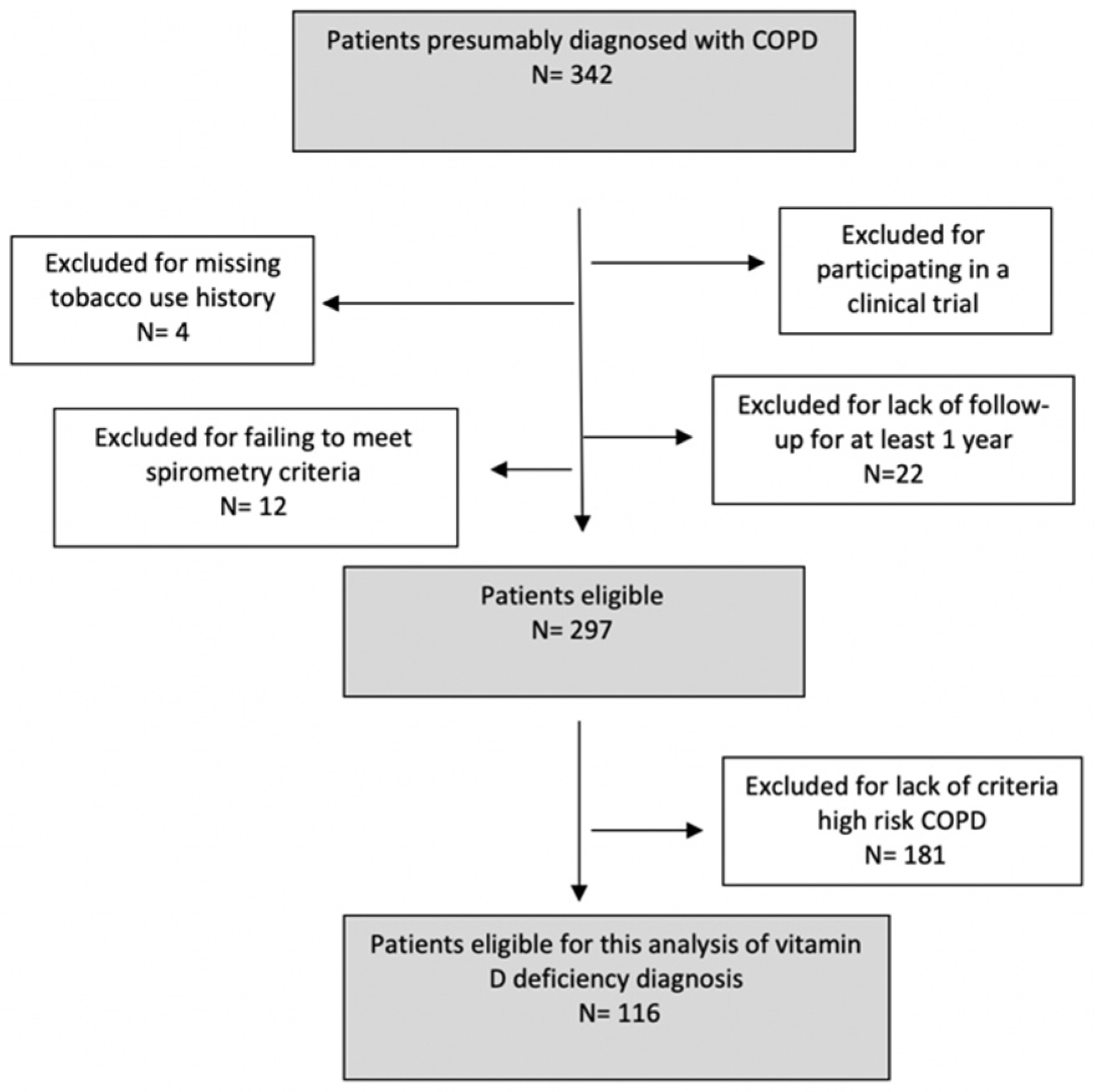
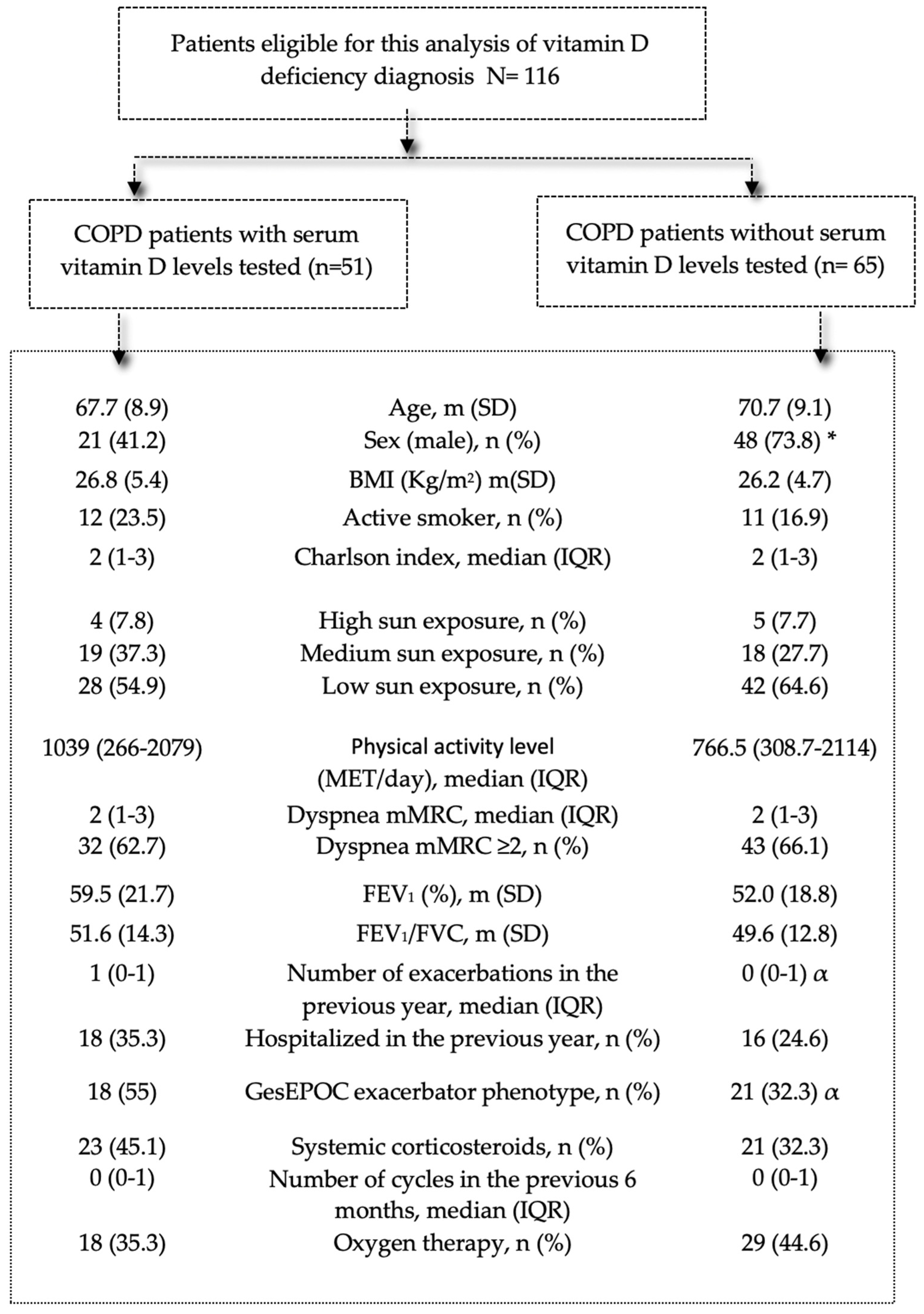
3.1. Population
3.2. Vitamin D Testing in Patients with High-Risk COPD
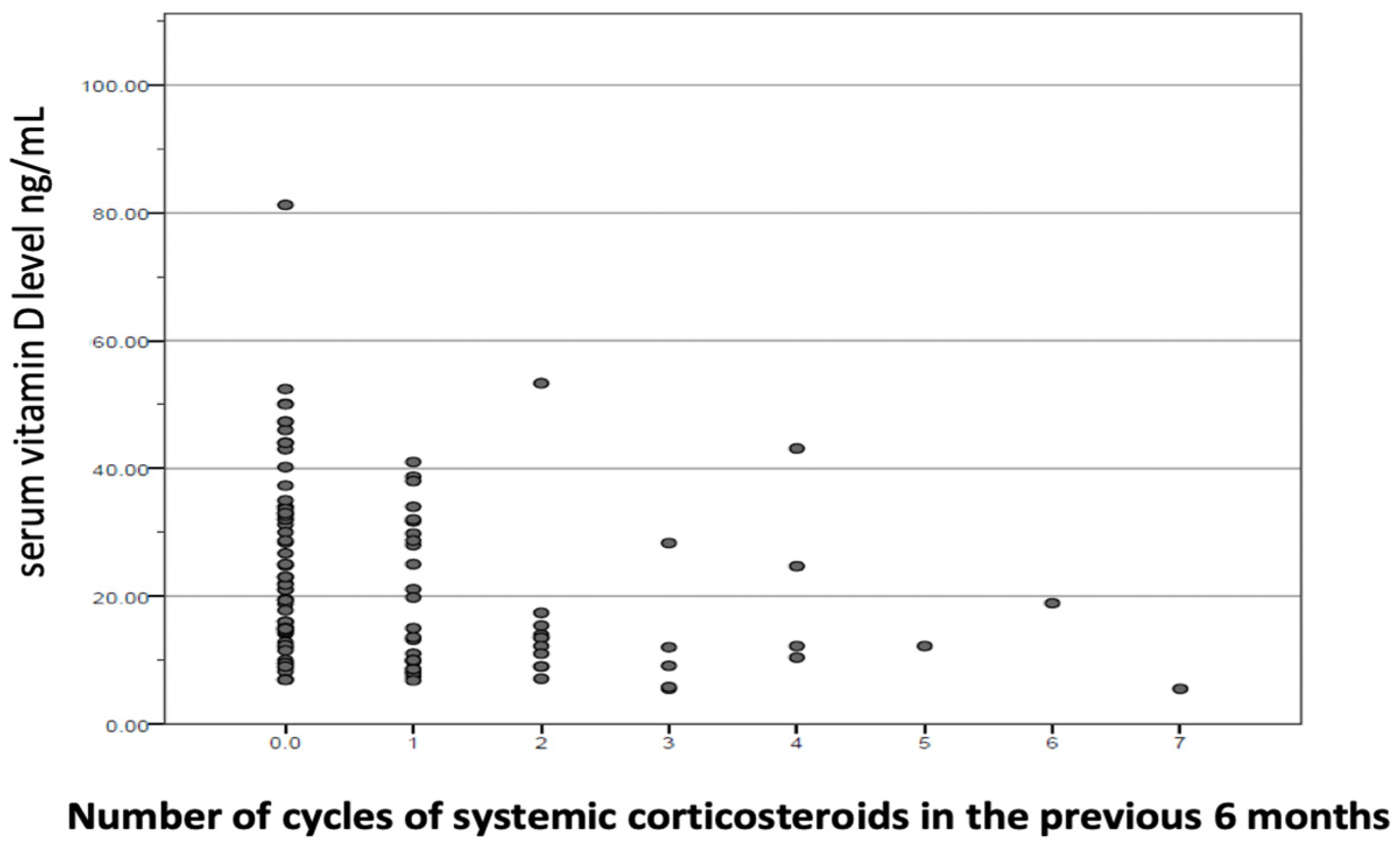
3.3. Vitamin D Deficiency and High-Risk COPD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blasi, F.; Cesana, G.; Conti, S.; Chiodini, V.; Aliberti, S.; Fornari, C. The clinical and economic impact of exacerbations of chronic obstructive pulmonary disease: A cohort of hospitalized patients. PLoS ONE 2014, 9, e101228. [Google Scholar] [CrossRef] [PubMed]
- Wageck, B.; Cox, N.S.; Holland, A.E. Recovery Following Acute Exacerbations of Chronic Obstructive Pulmonary Disease—A Review. COPD 2019, 16, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Seemungal, T.A.; Wedzicha, J.A. Exacerbation frequency and FEV1 decline of COPD: Is it geographic? Eur. Respir. J. 2014, 43, 1220–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, G.; Mushnikov, V.; Bäckström, T.; Engström, A.; Khalid, J.M.; Wall, J. Exacerbations and healthcare resource utilization among COPD patients in a Swedish registry-based nation-wide study. BMC Pulm. Med. 2018, 18, 17. [Google Scholar] [CrossRef] [Green Version]
- Soriano, J.B.; Rojas-Rueda, D.; Alonso, J.; Antó, J.M.; Cardona, P.J.; Fernández, E. Colaboradores de GBD en España; Lista de colaboradores de GBD en España. The burden of disease in Spain: Results from the Global Burden of Disease 2016. Med. Clin. 2018, 151, 171–190. [Google Scholar] [CrossRef]
- Assessing National Capacity for the Prevention and Control of Noncommunicable Diseases: Report of the 2019 Global Survey. Ginebra: Organización Mundial de la Salud. 2020. Licencia: CC BY-NC-SA 3.0 IGO. Disponible en. 2020. Available online: https://www.who.int/teams/ncds/surveillance/monitoring-capacity/ncdccs (accessed on 30 December 2021).
- Miravitlles, M.; Calle, M.; Molina, J.; Almagro, P.; Gómez, J.T.; Trigueros, J.A.; Cosío, B.G.; Casanova, C.; López-Campos, J.L.; Riesco, J.A.; et al. Spanish COPD Guidelines (GesEPOC) 2021, Updated Pharmacological treatment of stable COPD. Arch. Bronconeumol. 2021, 58, 69–81. [Google Scholar] [CrossRef]
- Calle Rubio, M.; Rodríguez Hermosa, J.L.; Soler-Cataluña, J.J.; López-Campos, J.L.; Alcázar Navarrete, B.; Soriano, J.B. Medical Care According to Risk Level and Adaptation to Spanish COPD Guidelines (Gesepoc): The Epoconsul Study. Arch. Bronconeumol. 2018, 54, 270–279. [Google Scholar] [CrossRef]
- Miravitlles, M.; Calle, M.; Soler-Cataluña, J.J. GesEPOC 2021, One More Step towards Personalized Treatment of COPD. Arch. Bronconeumol. 2021, 57, 9–10. [Google Scholar] [CrossRef]
- Adams, J.S.; Hewison, M. Update in vitamin D. J. Clin. Endocrinol. Metab. 2010, 95, 471–478. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Baldrick, F.R.; Elborn, J.S.; Woodside, J.V. Vitamin D status in chronic obstructive pulmonary disease. Proc. Nutr. Soc. 2012, 71, E98. [Google Scholar] [CrossRef] [Green Version]
- Reid, I.R.; Bolland, M.J.; Grey, A. Effects of vitamin D supplements on bone mineral density: A systematic review and meta-analysis. Lancet 2014, 383, 146–155. [Google Scholar] [CrossRef]
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080S–1086S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prietl, B.; Treiber, G.; Pieber, T.R.; Amrein, K. Vitamin D and immune function. Nutrients 2013, 5, 2502–2521. [Google Scholar] [CrossRef] [PubMed]
- Janssens, W.; Lehouck, A.; Carremans, C.; Bouillon, R.; Mathieu, C.; Decramer, M. Vitamin D beyond bones in chronic obstructive pulmonary disease: Time to act. Am. J. Respir. Crit. Care Med. 2009, 179, 630–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginde, A.A.; Mansbach, J.M.; Camargo, C.A., Jr. Association between serum 25-hydroxyvitamin D level and upper respiratory tract infection in the Third National Health and Nutrition Examination Survey. Arch. Intern. Med. 2009, 169, 384–390. [Google Scholar] [CrossRef] [Green Version]
- Hurst, J.R.; Vestbo, J.; Anzueto, A.; Locantore, N.; Müllerova, H.; Tal-Singer, R. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N. Engl. J. Med. 2010, 363, 1128–1138. [Google Scholar] [CrossRef] [Green Version]
- Zhu, M.; Wang, T.; Wang, C.; Ji, Y. The association between vitamin D and COPD risk, severity, and exacerbation: An updated systematic review and meta-analysis. Int. J. Chron. Obstruct. Pulmon. Dis. 2016, 11, 2597–2607. [Google Scholar] [CrossRef] [Green Version]
- Burkes, R.M.; Ceppe, A.S.; Doerschuk, C.M.; Couper, D.; Hoffman, E.A.; Comellas, A.P. Associations Among 25-Hydroxyvitamin D Levels Lung Function, and Exacerbation Outcomes in COPD: An Analysis of the SPIROMICS Cohort. Chest 2020, 157, 856–865. [Google Scholar] [CrossRef]
- Alavi Foumani, A.; Mehrdad, M.; Jafarinezhad, A.; Nokani, K.; Jafari, A. Impact of vitamin D on spirometry findings and quality of life in patients with chronic obstructive pulmonary disease: A randomized, double-blinded, placebo-controlled clinical trial. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 1495–1501. [Google Scholar] [CrossRef] [Green Version]
- Jolliffe, D.A.; Greenberg, L.; Hooper, R.L.; Mathyssen, C.; Rafiq, R.; de Jongh, R.T. Vitamin D to prevent exacerbations of COPD: Systematic review and meta-analysis of individual participant data from randomised controlled trials. Thorax 2019, 74, 337–345. [Google Scholar] [CrossRef] [Green Version]
- López-Campos, J.L.; Almagro, P.; Gómez, J.T.; Chiner, E.; Palacios, L.; Hernández, C. En nombre del equipo de trabajo de GesEPOC2021. Spanish COPD Guideline(GesEPOC) Update: Comorbidities, Self-Managementand Palliative Care. Arch. Bronconeumol. 2021. [Google Scholar] [CrossRef]
- Bestall, J.C.; Paul, E.A.; Garrod, R.; Garnham, R.; Jones, P.W.; Wedzicha, J.A. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax 1999, 54, 581–586. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Brown, W.J.; Trost, S.G.; Bauman, A.; Mummery, K.; Owen, N. Test-retest reliability of four physical activity measures used in population surveys. J. Sci. Med. Sport 2004, 7, 205–215. [Google Scholar] [CrossRef]
- Jones, P.W.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.H.; Kline Leidy, N. Development and first validation of the COPD Assessment Test. Eur. Respir. J. 2009, 34, 648–654. [Google Scholar] [CrossRef] [Green Version]
- Miravitlles, M.; Soler-Cataluña, J.J.; Calle, M.; Molina, J.; Almagro, P.; Quintano, J.A. Spanish COPD guidelines (GesEPOC) 2017. Pharmacological treatment of stable chronic obstructive pulmonary diseare. Arch. Bronconeumol. 2017, 53, 324–335. [Google Scholar] [CrossRef]
- Mekov, E.; Slavova, Y. Vitamin D deficiency and insufficiency in patients with COPD—A systematic review. Thorac. Med. 2014, 6, 18–32. [Google Scholar]
- Casado, E.; Quesada, J.M.; Naves, M.; Peris, P.; Jódar, E.; Giner, M. Recomendaciones de la SEIOMM en la prevención y tratamiento del déficit de vitamina D. Rev. Osteoporos Metab. Miner. 2021, 13, 84–97. [Google Scholar]
- Janssens, W. Vitamin D deficiency is highly prevalent in COPD and correlates with variants in the vitamin D-binding gene. Thorax 2010, 65, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Shaheen, S.O.; Jameson, K.A.; Robinson, S.M.; Boucher, B.J.; Syddall, H.E.; Sayer, A.A. Relationship of vitamin D status to adult lung function and COPD. Thorax 2011, 66, 692–698. [Google Scholar] [CrossRef] [Green Version]
- Salinas, M.; López-Garrigós, M.; Flores, E.; Leiva-Salinas, C. Temporal and regional variability in the request of Vitamin D from general practitioners in Spain. Clin. Chem. Lab. Med. 2017, 55, 1754–1760. [Google Scholar] [CrossRef]
- Petrilli, C.M.; Henderson, J.; Keedy, J.M.; Dibble, E.R.; Wei, M.Y.; Prussack, J.K. Reducing Unnecessary Vitamin D Screening in an Academic Health System: What Works and When. Am. J. Med. 2018, 131, 1444–1448. [Google Scholar] [CrossRef]
- LeFevre, M.L.; LeFevre, N.M. Vitamin D Screening and Supplementation in Community-Dwelling Adults: Common Questions and Answers. Am. Fam. Physician 2018, 97, 254–260. [Google Scholar]
- Rockwell, M.; Kraak, V.; Hulver, M.; Epling, J. Clinical management of low vitamin D: A scoping review of physicians’ practices. Nutrients 2018, 10, 493. [Google Scholar] [CrossRef] [Green Version]
- Fraser, W.D.; Milan, A.M. Vitamin D assays: Past and present debates, difficulties, and developments. Calcif. Tissue Int. 2013, 92, 118–127. [Google Scholar] [CrossRef]
- Mekov, E. Vitamin D Deficiency and Insufficiency in Hospitalized COPD Patients. PLoS ONE 2015, 10, e0129080. [Google Scholar] [CrossRef] [Green Version]
- Lukert, B.P.; Raisz, L.G. Glucocorticoid-induced osteoporosis: Pathogenesis and management. Ann. Intern. Med. 1990, 112, 352–364. [Google Scholar] [CrossRef]
- Dhawan, P.; Christakos, S. Novel regulation of 25-hydroxyvitamin D3 24-hydroxylase (24(OH)ase) transcription by glucocorticoids: Cooperative effects of the glucocorticoid receptor, C/EBP beta, and the Vitamin D receptor in 24(OH)ase transcription. J. Cell Biochem. 2010, 110, 1314–1323. [Google Scholar] [CrossRef]
- Skversky, A.L.; Kumar, J.; Abramowitz, M.K.; Kaskel, F.J.; Melamed, M.L. Association of glucocorticoid use and low 25-hydroxyvitamin D levels: Results from the National Health and Nutrition Examination Survey (NHANES): 2001–2006. J. Clin. Endocrinol. Metab. 2011, 96, 3838–3845. [Google Scholar] [CrossRef] [Green Version]
- Martineau, A.R.; James, W.Y.; Hooper, R.L.; Barnes, N.C.; Jolliffe, D.A.; Greiller, C.L. Vitamin D3 supplementation in patients with chronic obstructive pulmonary disease (ViDiCO): A multicentre, double-blind, randomized controlled trial. Lancet Respir. Med. 2015, 3, 120–130. [Google Scholar] [CrossRef]
- Jorde, I.; Stegemann-Koniszewski, S.; Papra, K.; Föllner, S.; Lux, A.; Schreiber, J. Association of serum vitamin D levels with disease severity, systemic inflammation, prior lung function loss and exacerbations in a cohort of patients with chronic obstructive pulmonary disease (COPD). J. Thorac. Dis. 2021, 13, 3597–3609. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis Prior to Vitamin D | All | Received Vitamin D Supplementation | Did Not Receive Vitamin D Supplementation | p |
|---|---|---|---|---|
| (n = 51) | (n = 33) | (n = 18) | ||
| Age, m (SD) | 67.7 (8.9) | 66.9 (8.5) | 69.3 (9.8) | 0.368 |
| Sex (male), n (%) | 21 (41.2) | 9 (27.3) | 12 (66.7) | 0.006 |
| BMI (Kg/m2), m (SD) | 26.8 (5.4) | 27.1 (5.9) | 26.4 (4.6) | 0.666 |
| Pack-years, median (IQR) | 40 (24–60) | 49 (21–71) | 40 (28.5–50) | 0.185 |
| Active smoker, n (%) | 12 (23.5) | 8 (24.2) | 4 (22.2) | 1 |
| Charlson index, median (IQR) | 2 (1–3) | 2 (1–3) | 2 (2–3) | 0.199 |
| Predisposing comorbidities, n (%) | 10 (19.6) | 8 (24.2) | 2 (11.1) | 0.462 |
| 4 (7.8) | 1 (3) | 3 (16.7) | 0.12 |
| Sun exposure | 4 (7.8) | 2 (6.1) | 2 (11.1) | 0.537 |
| 19 (37.3) | 14 (42.4) | 5 (27.8) | |
| 28 (54.9) | 17 (51.5) | 11 (61.1) | ||
| Physical activity level | 1039 (266–2079) | 1386 (288–2079) | 656.5 (256.5–1559) | 0.413 |
| (MET), median (IQR) | ||||
| Physical activity level | 7 (13.7) | 5 (15.2) | 2 (11.1) | 0.476 |
| 22 (43.1) | 15 (45.5) | 7 (38.9) | |
| 22 (43.1) | 13 (39.4) | 9 (50) | ||
| Previous vitamin D level, median (IQR) | 13.4 (8.5–17.8) | 11.9 (8.6–17.5) | 17.3 (14.3–21.8) | 0.003 |
| Dyspnea mMRC, median (IQR) | 2 (1–3) | 2 (1–3) | 2 (1–3) | 0.766 |
| ≥2, n (%) | 32 (62.7) | 20 (60.6) | 12 (66.7) | 0.767 |
| CAT, m (SD) | 14.1 (9.0) | 13.5 (8.4) | 15.2 (10.1) | 0.664 |
| CAT ≥10, n (%) | 31 (60.8) | 20 (60.6) | 11 (61.1) | 1 |
| FEV1 (mL), median (IQR) | 1290 (1090–1860) | 1230 (1040–1780) | 1525 (1047–1927) | 0.364 |
| FEV1 (%), m (SD) | 59.5 (21.7) | 60.7 (21.2) | 57.2 (23.1) | 0.597 |
| FVC ml, median (IQR) | 2550 (2130–3060) | 2420 (2105–2920) | 2860 (2197–3517) | 0.104 |
| FVC %, m (SD) | 92.0 (19.5) | 93.7 (18.9) | 88.8 (20.7) | 0.397 |
| FEV1/FVC, m (SD) | 51.6 (14.3) | 52.4 (14.4) | 50.2 (14.3) | 0.597 |
| Number of exacerbations in previous year, m (SD) | 1 (0–1) | 1 (1.7) | 1.1 (1.2) | 0.272 |
| Hospitalizations | 18 (35.3) | 7 (21.2) | 11 (61.1) | 0.004 |
| GesEPOC exacerbator phenotype, n (%) | 18 (55) | 17 (51.5) | 11 (61.1) | 0.548 |
| Treatment, n (%) | 3 (5.9) | 1 (3) | 1 (5.6) | 0.344 |
| 28 (54.9) | 15 (45.5) | 13 (72.2) | |
| 1 (2) | 1 (3) | 0 | ||
| 19 (37.3) | 15 845.5) | 4 (22.2) | ||
| Systemic corticosteroids, n (%) | 23 (45.1) | 12 (36.4) | 11 (61.1) | 0.141 |
| Number of cycles, median (IQR) | 0 (0–1) | 0 (0–1) | 1 (0–2) | 0.061 |
| Oxygen therapy, n (%) | 18 (35.3) | 12 (36.4) | 6 (33.3) | 1 |
| All | Vitamin D Levels <20 ng/mL | Vitamin D Levels ≥20 ng/mL | p | |
|---|---|---|---|---|
| (n= 116) | (n = 63) | (n= 53) | ||
| Male, n (%) | 69 (59.5) | 40 (63.5) | 29 (54.7) | 0.338 |
| Age, m (SD) | 69.4 (9.1) | 70.2 (8.6) | 68.4 (68.5) | 0.316 |
| BMI (kg/m2), m (SD) | 26.5 (5.0) | 25.9 (4.5) | 27.1 (5.5) | 0.202 |
| Pack-years, median (IQR) | 45 (30–60) | 50 (34–65) | 42 (30–50) | 0.078 |
| Employment status | 0.909 | |||
| Active | 12 (10.3) | 7 (11.1) | 5 (9.4) | |
| Retired | 78 (67.2) | 43 (68.3) | 35 (66) | |
| Low/inability to work | 21 (18.1) | 10 (15.9) | 11 (20.8) | |
| Unemployed | 5 (4.3) | 3 (4.8) | 2 (3.8) | |
| Level of studies | 0.059 | |||
| High | 27 (23.3) | 11 (17.5) | 16 (30.2) | |
| Average | 53 (45.7) | 35 (55.6) | 18 (34) | |
| No studies | 36 (31) | 17 (27) | 19 (35.8) | |
| Living situation | 0.353 | |||
| Single | 30 (25.9) | 14 (22.2) | 16 (30.2) | |
| Partner | 85 (73.3) | 48 (76.2) | 37 (69.8) | |
| Residence | 1 (0.9) | 1 (1.6) | 0 | |
| Charlson index, median (IQR) | 2 (1- 3) | 2 (1–3) | 2 (1–3) | 0.677 |
| Predisposing comorbidities, n (%) | ||||
| Osteoporosis Chronic renal failure | 14 (12.1) | 2 (1–3) | 2 (1–3) | 0.667 |
| 4 (3.4) | 8 (12.7) | 6 (11.3) | 0.821 | |
| Active smoker, n (%) | 23 (19.8) | 9 (14.3) | 14 (26.4) | 0.103 |
| Vitamin D levels al visit, m (SD) | 18.8 (11.6–32) | 12.11 (3.92) | 34.54 (11.08) | <0.001 |
| Vitamin D >30, n (%) | 32 (27.6) | 32 (60.3) | ||
| Vitamin D ≤30 and ≥20, n (%) | 21 (18.1) | 21 (39.6) | ||
| Vitamin D <20 and ≥12, n (%) | 34 (29.3) | 34 (54) | ||
| Vitamin D <12, n (%) | 29 (25) | 29 (46) | ||
| Physical activity level (MET), median (IQR) | 880 (288–2079) | 422 (242.5–1181) | 1740 (714.5–2772) | <0.001 |
| Physical activity level | ||||
| High, n (%) Medium, n (%) Low, n (%) | 16 (13.8) | 4 (6.6) | 12 (22.6) | <0.001 |
| 51 (43.9) | 21 (34.4) | 30 (56.6) | ||
| 47 (40.5) | 36 (59) | 11 (20.8) | ||
| Sun exposure | 0.253 | |||
| High exposure, n (%) Medium exposure, n (%) Low exposure, n (%) | 9 (7.8) | 5 (7.9) | 4 (7.5) | |
| 37 (31.9) | 16 (25.4) | 21 (39.7) | ||
| 70 (60.3) | 42 (66.7) | 28 (52.8) | ||
| FEV1 mL, median (IQR) | 1290 (957–1800) | 1260 (900–1860) | 1350 (1110–1730) | 0.24 |
| FEV1 (%), m (SD) | 55.3 (20.4) | 50.6 (21.3) | 60.7 (17.9) | 0.007 |
| FVC ml, median (IQR) | 2725 (2235–3325) | 2790 (2210–3380) | 2580 (2280–3320) | 0.816 |
| FVC %, m (SD) | 90.6 (19.5) | 89.6 (70.3–104.6) | 92.2 (18.5) | 0.421 |
| FEV1/FVC, m (SD) | 50.5 (13.5) | 49 (39.3–60.8) | 52.3 (12.6) | 0.189 |
| Dyspnea mMRC, median (IQR) | 2 (1–3) | 2 (1–3) | 2 (1–2) | 0.072 |
| ≥2, n (%) | 75 (64.6) | 45 (71.4) | 30 (56.6) | 0.096 |
| CAT, median (IQR) | 13.5 (7–20.7) | 16 (9–22) | 10 (6.5–18.5) | 0.033 |
| GesEPOC exacerbator phenotype, n (%) | 56 (48.3) | 37 (58.7) | 13 (24.5) | <0.001 |
| Number of exacerbations in previous year, median (IQR) | 0 (0–1) | 1 (0–2) | 0 (0–1) | 0.003 |
| 0–1, n (%) | ||||
| ≥2, n (%) | 93 (80.2) | 44 (69.8) | 49 (92.5) | 0.002 |
| 23 (19.8) | 19 (30.2) | 4 (7.5) | ||
| Hospitalized in the previous year, n (%) | 34 (29.3) | 32 (50.8) | 2 (3.8) | <0.001 |
| Required systemic corticosteroids in the previous 6 months, n (%) | 44 (37.9) | 35 (55.6) | 9 (17) | 0.003 |
| Number of corticosteroid cycles, median (IQR) | 0 | |||
| 0 (0–1) | 1 (0–2) | 0 (0–0) | ||
| Treatment, n (%) | 0.04 | |||
| LAMA LAMA + LABA LABA + ICS LAMA + LABA + ICS | 7 (6) | 1 (1.6) | 6 (11.5) | |
| 71 (61.2) | 41 (67.2) | 30 (57.7) | ||
| 1 (0.9) | 0 | 1 (1.9) | ||
| 34 (29.3) | 19 (31.1) | 15 (28.8) | ||
| Oxygen therapy, n (%) | 47 (40.5) | 32 (50.8) | 15 (28.3) | 0.014 |
| Diagnostic procedures conducted for COPD evaluation | ||||
| COPD patients with serum vitamin D levels tested during follow-up | 51 (44) | 26 (41.3) | 25 (47.2) | 0.576 |
| COPD patients with vitamin D deficiency who received vitamin D supplementation | 33 (28.4) | 12 (19) | 21 (39.6) | 0.021 |
| Variable | OR (95% CI) | p |
|---|---|---|
| Activity level | ||
| Medium-high (ref) | ||
| Low | 3.840 (1.541–9.567) | 0.004 |
| Inhaled corticosteroids | ||
| No (ref) | ||
| Yes | 3.210 (1.230–8.317) | 0.016 |
| Number of systemic corticosteroid cycles | ||
| No (ref) | ||
| Yes | 2.149 (1.330–3.473) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calle Rubio, M.; Álvarez-Sala, J.L.; Vargas Centanaro, G.; Navarro, A.M.H.; Hermosa, J.L.R. Testing for Vitamin D in High-Risk COPD in Outpatient Clinics in Spain: A Cross-Sectional Analysis of the VITADEPOC Study. J. Clin. Med. 2022, 11, 1347. https://doi.org/10.3390/jcm11051347
Calle Rubio M, Álvarez-Sala JL, Vargas Centanaro G, Navarro AMH, Hermosa JLR. Testing for Vitamin D in High-Risk COPD in Outpatient Clinics in Spain: A Cross-Sectional Analysis of the VITADEPOC Study. Journal of Clinical Medicine. 2022; 11(5):1347. https://doi.org/10.3390/jcm11051347
Chicago/Turabian StyleCalle Rubio, Myriam, José Luis Álvarez-Sala, Gianna Vargas Centanaro, Ana María Humanes Navarro, and Juan Luis Rodríguez Hermosa. 2022. "Testing for Vitamin D in High-Risk COPD in Outpatient Clinics in Spain: A Cross-Sectional Analysis of the VITADEPOC Study" Journal of Clinical Medicine 11, no. 5: 1347. https://doi.org/10.3390/jcm11051347
APA StyleCalle Rubio, M., Álvarez-Sala, J. L., Vargas Centanaro, G., Navarro, A. M. H., & Hermosa, J. L. R. (2022). Testing for Vitamin D in High-Risk COPD in Outpatient Clinics in Spain: A Cross-Sectional Analysis of the VITADEPOC Study. Journal of Clinical Medicine, 11(5), 1347. https://doi.org/10.3390/jcm11051347