
Echocardiographic and Electrocardiographic Determinants of Atrial Cardiomyopathy Identify Patients with Atrial Fibrillation at Risk for Left Atrial Thrombogenesis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Patient Population
2.2. Transthoracic Echocardiography (TTE)
2.3. Transesophageal Echocardiography (TEE)
2.4. Amplified Sinus-P-Wave Duration (APWD)
3. Statistical Analysis
4. Results
4.1. Baseline Characteristics
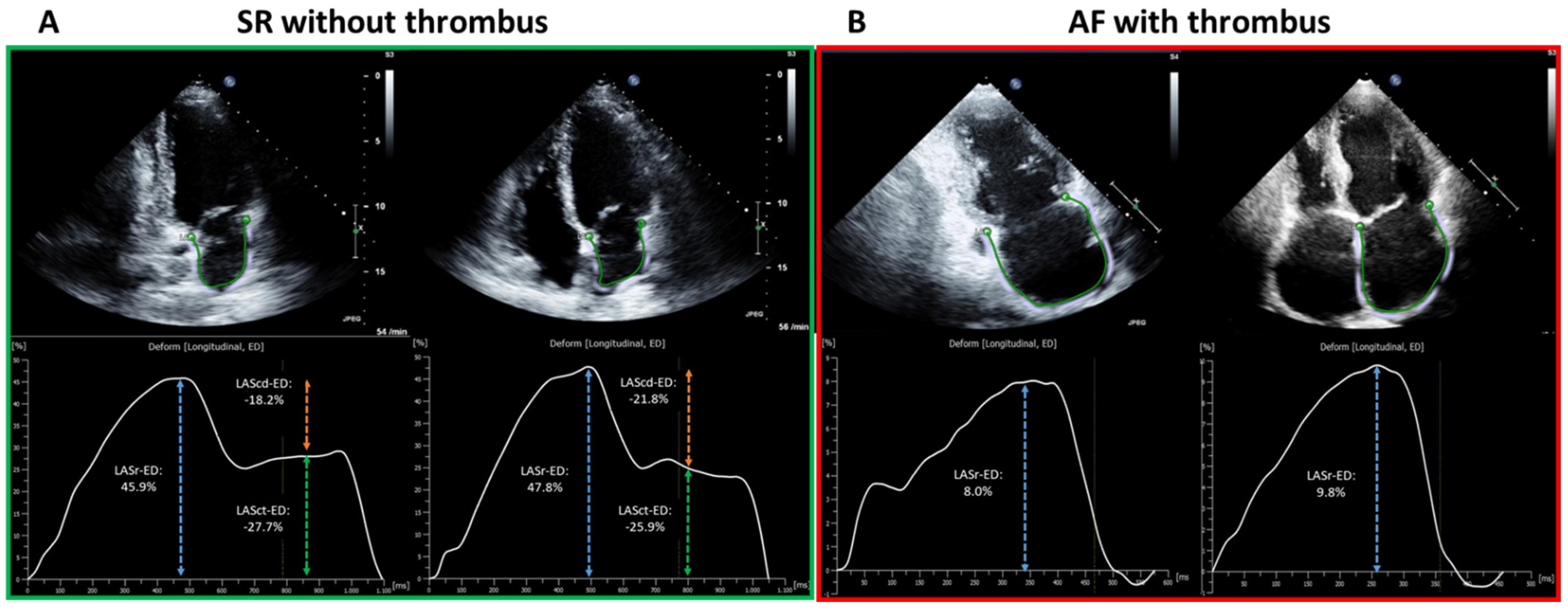
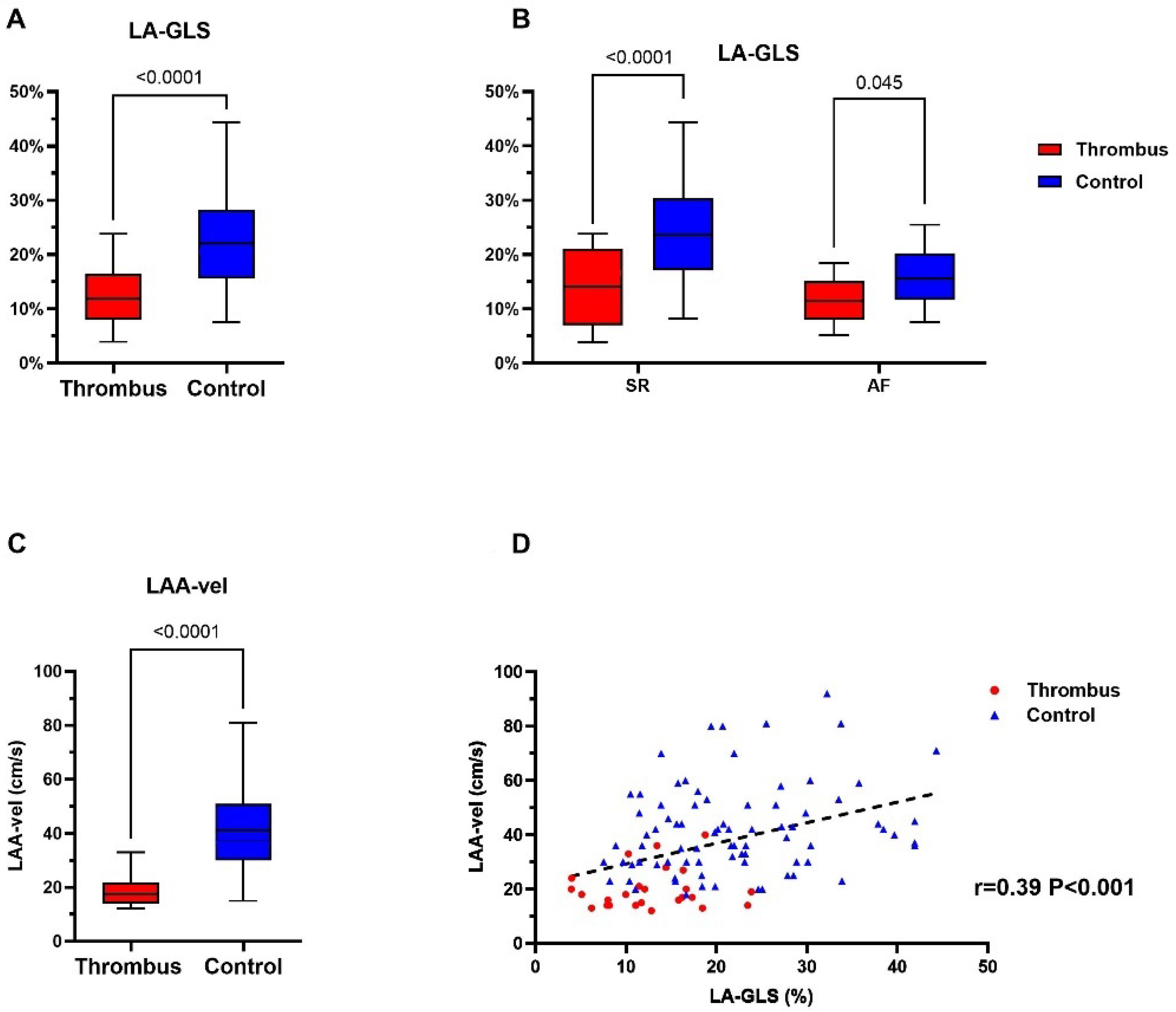
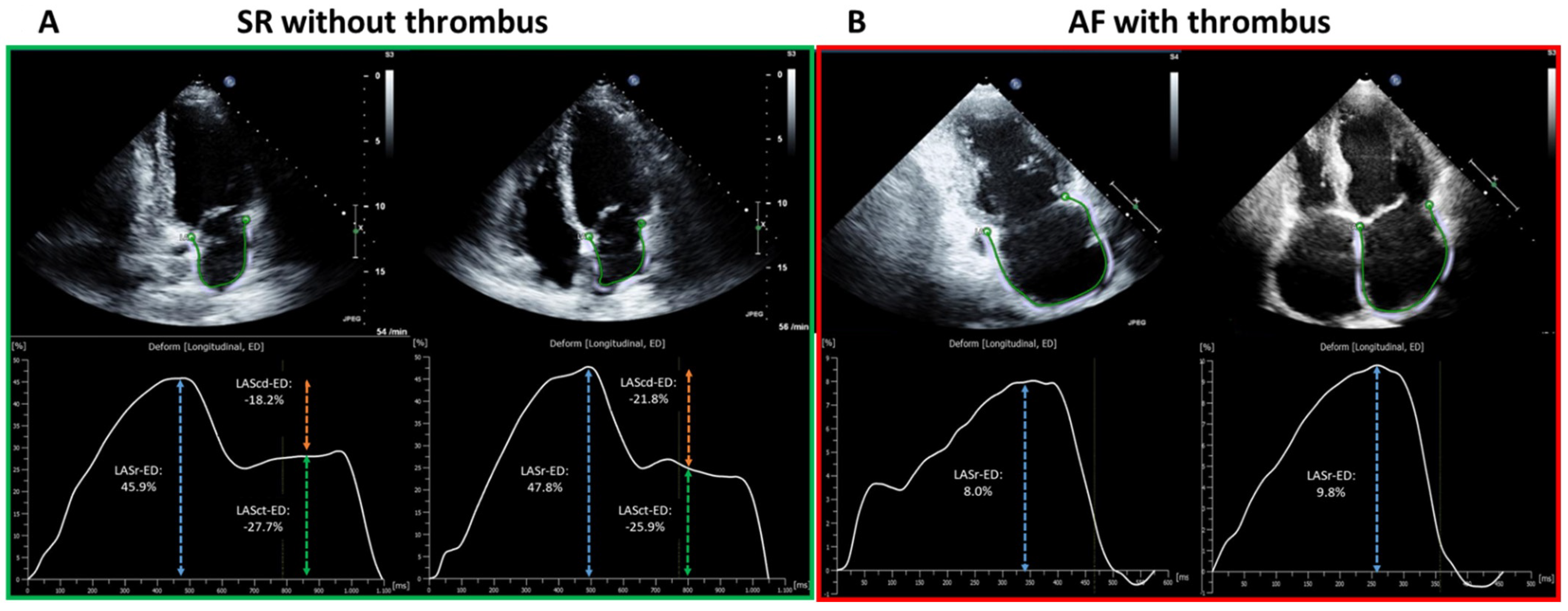
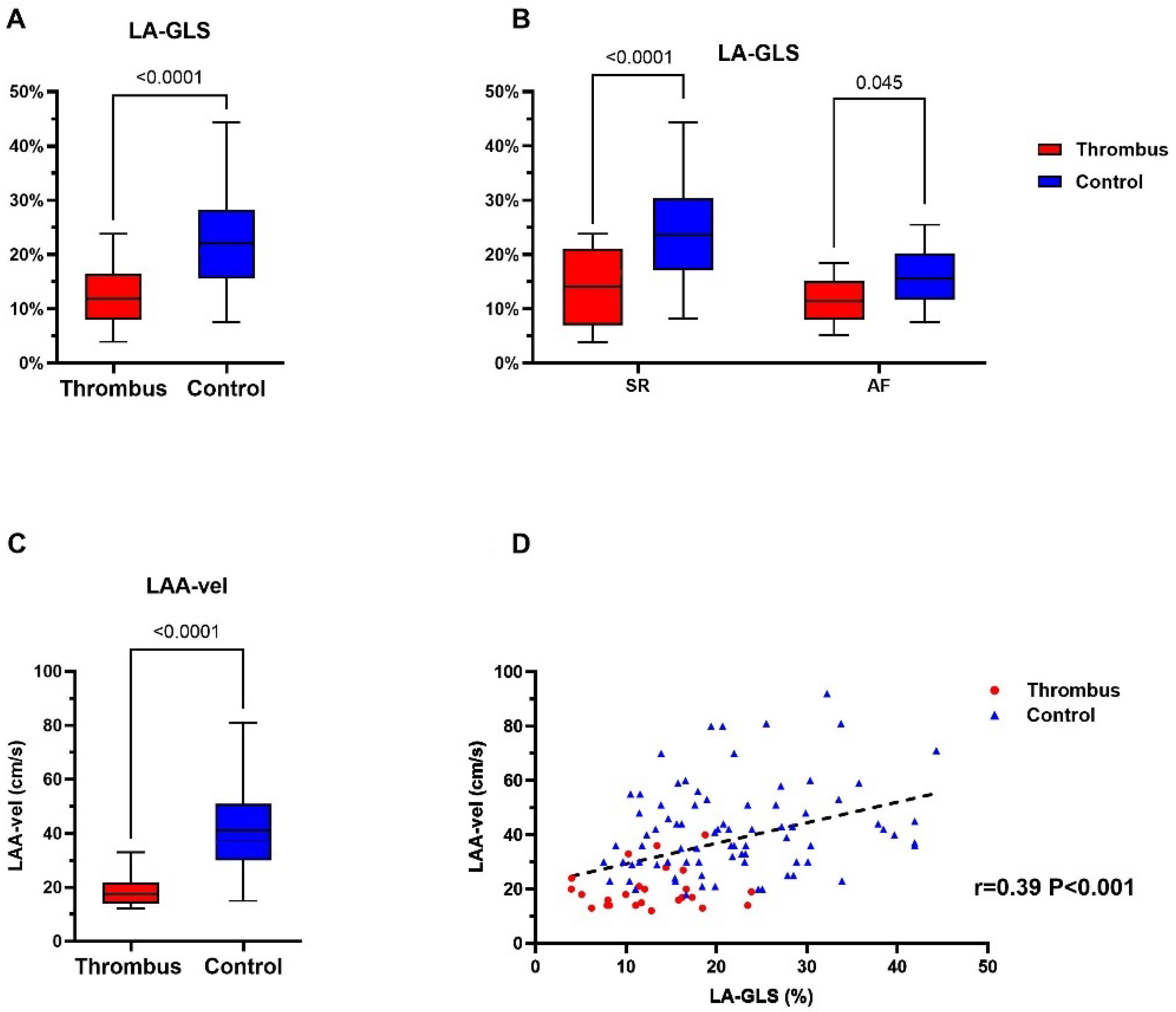
4.2. Left Atrial Appendage Thrombus Is Associated with Impaired Mechanical Function
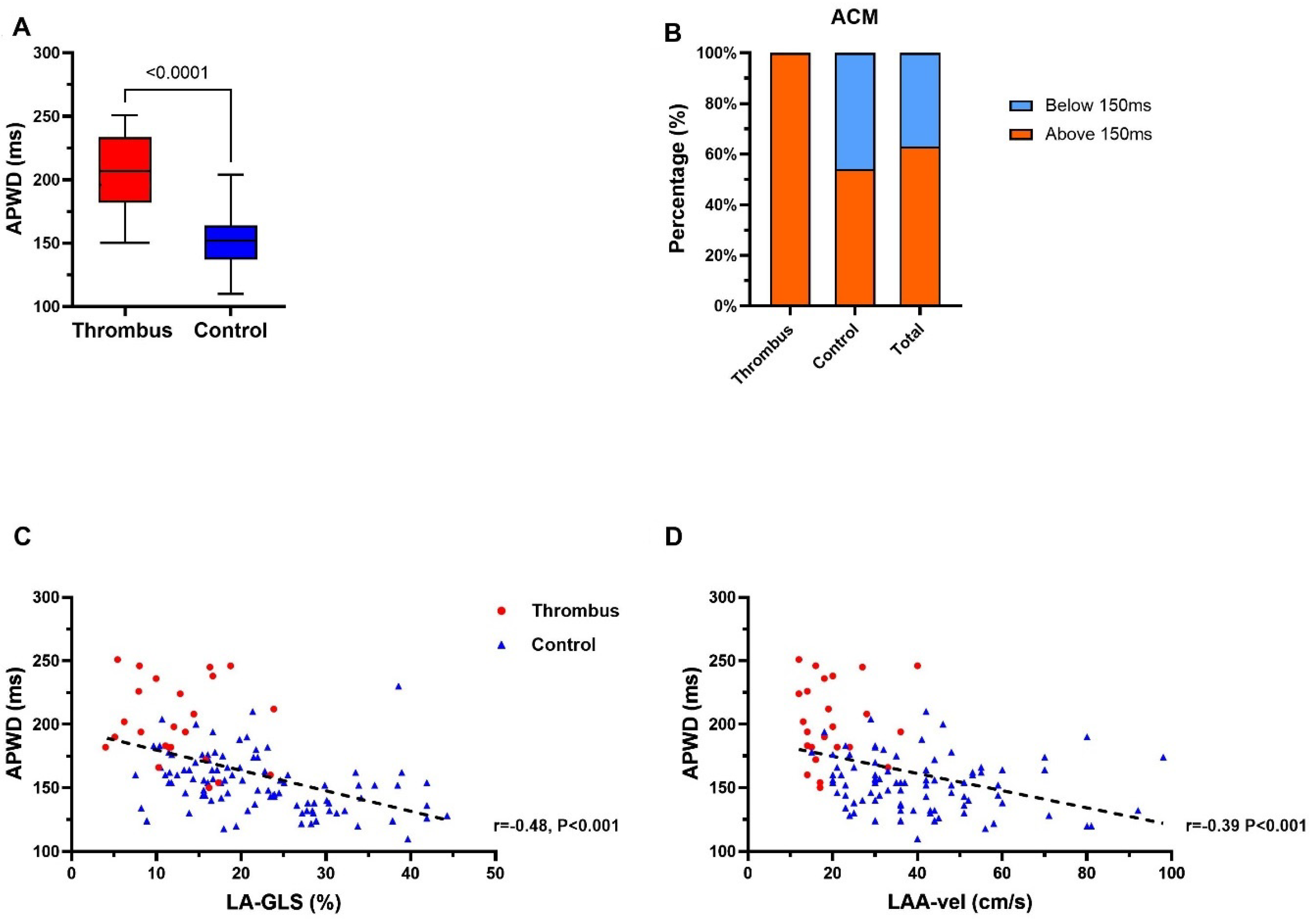
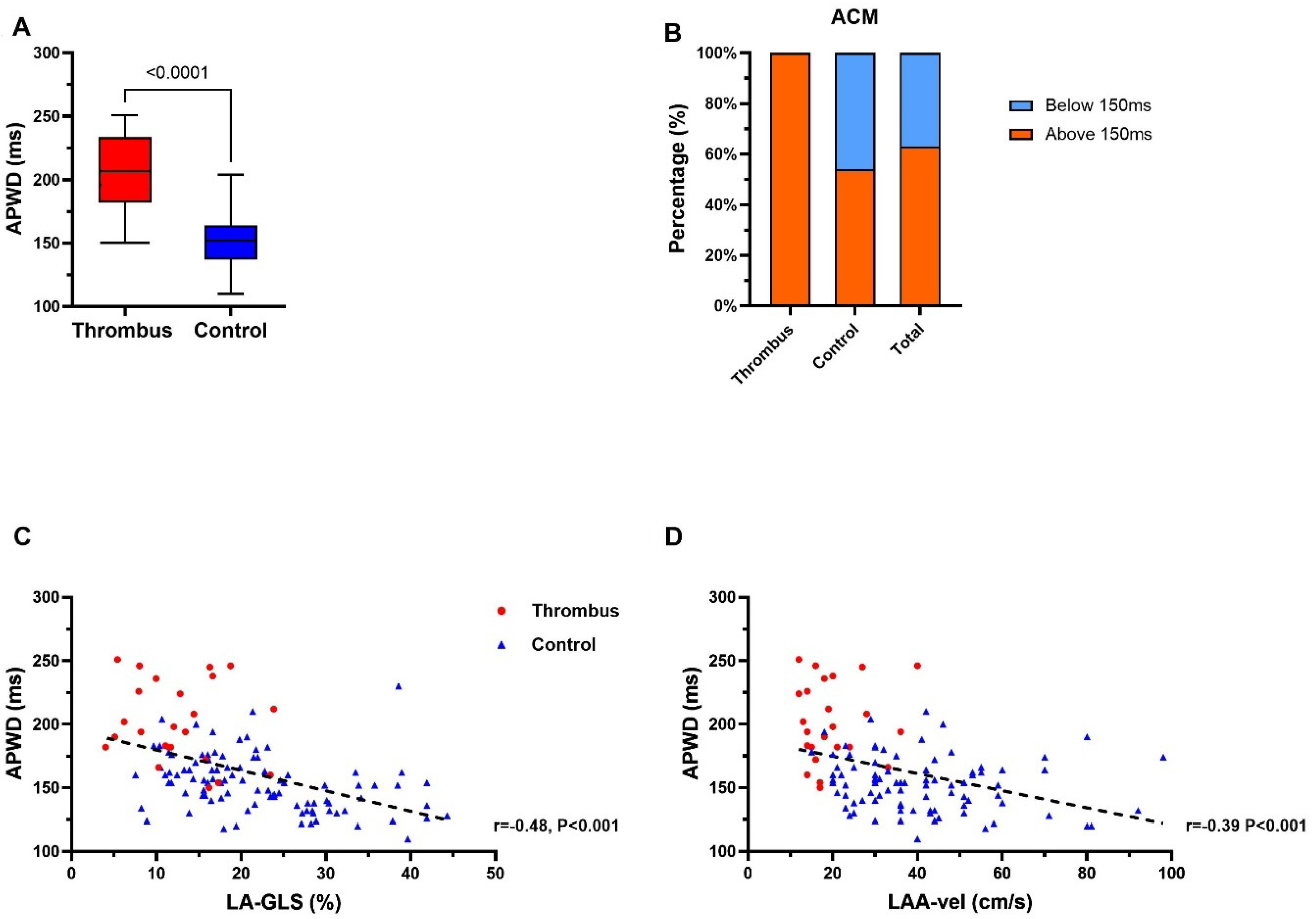
4.3. APWD Identifies Patients with LAA-Thrombus with Left Atrial Contractile Dysfunction
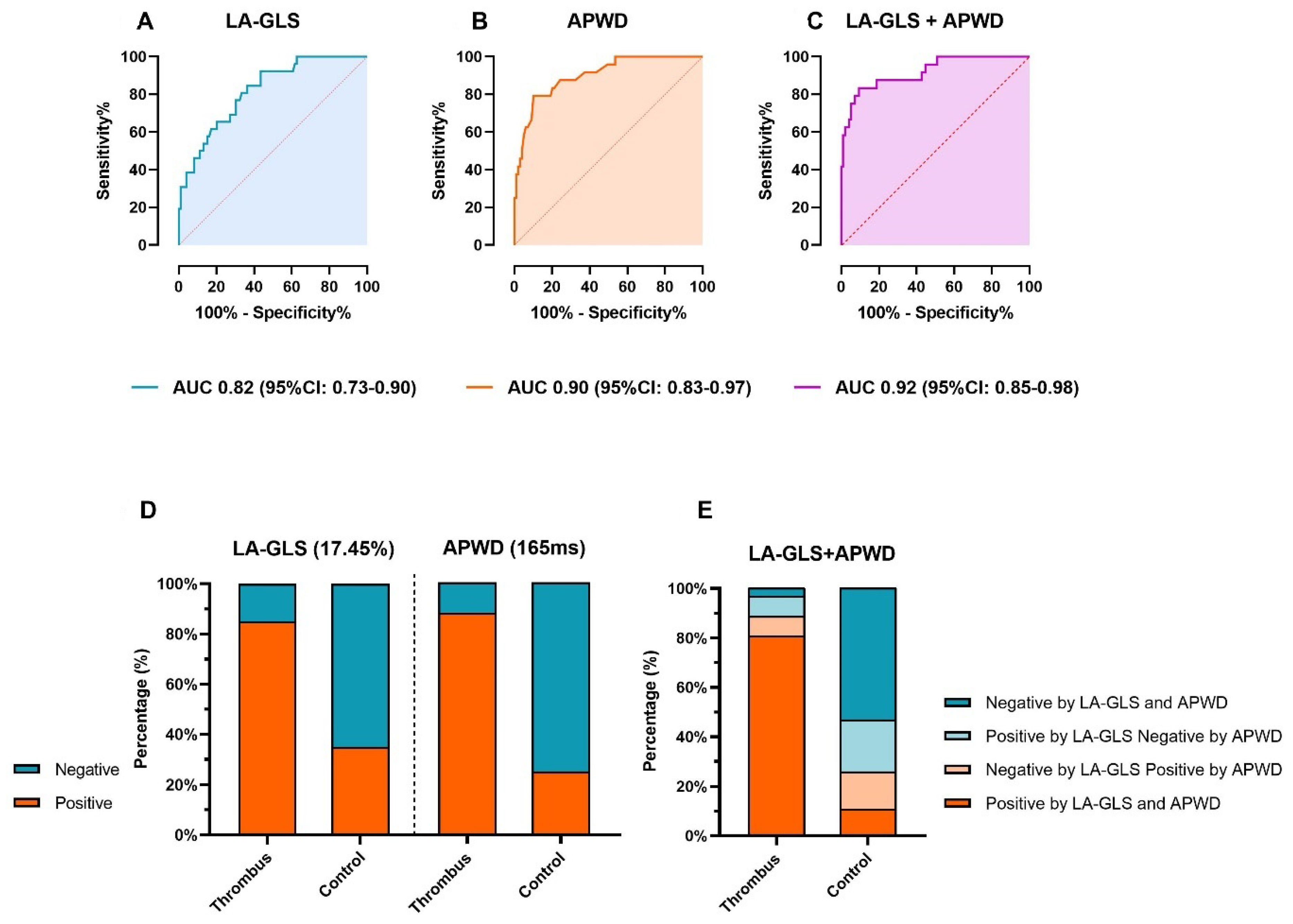
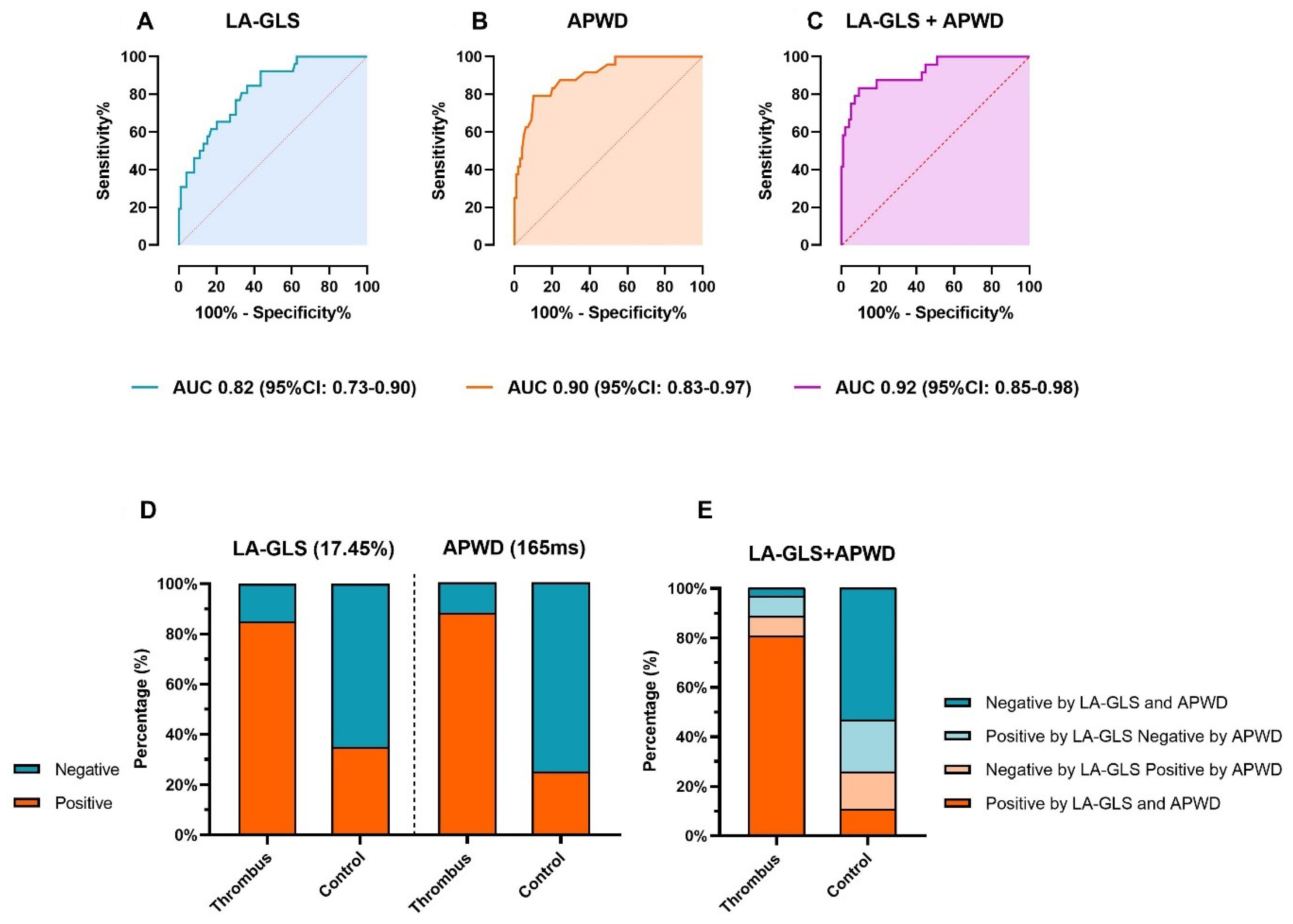
4.4. Diagnostic Value of LA-GLS and APWD for Identification of Patients at Risk for LAA-Thrombus
5. Discussion
5.1. Atrial Cardiomyopathy and Atrial Thrombogenesis
5.2. General and Rhythm-Specific LA-GLS Thresholds for Left-Atrial Appendage Thrombus
5.3. Combination of Echocardiographic and Electrocardiographic Markers
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goette, A.; Kalman, J.M.; Aguinaga, L.; Akar, J.; Cabrera, J.A.; Chen, S.A.; Chugh, S.S.; Corradi, D.; d’Avila, A.; Dobrev, D.; et al. EHRA/HRS/APHRS/SOLAECE expert consensus on atrial cardiomyopathies: Definition, characterization, and clinical implication. EP Eur. 2016, 18, 1455–1490. [Google Scholar] [CrossRef] [PubMed]
- Platonov, P.G.; Mitrofanova, L.B.; Orshanskaya, V.; Ho, S.Y. Structural abnormalities in atrial walls are associated with presence and persistency of atrial fibrillation but not with age. J. Am. Coll. Cardiol. 2011, 58, 2225–2232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolf, S.; Kircher, S.; Arya, A.; Eitel, C.; Sommer, P.; Richter, S.; Gaspar, T.; Bollmann, A.; Altmann, D.; Piedra, C.; et al. Tailored atrial substrate modification based on low-voltage areas in catheter ablation of atrial fibrillation. Circ. Arrhythmia Electrophysiol. 2014, 7, 825–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, B.J.; Zhao, J.; Csepe, T.A.; Moore, B.T.; Li, N.; Jayne, L.A.; Kalyanasundaram, A.; Lim, P.; Bratasz, A.; Powell, K.A.; et al. Atrial fibrillation driven by micro-anatomic intramural re-entry revealed by simultaneous sub-epicardial and sub-endocardial optical mapping in explanted human hearts. Eur. Heart J. 2015, 36, 2390–2401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagishita, A.; Sparano, D.; Cakulev, I.; Gimbel, J.R.; Phelan, T.; Mustafa, H.; de Oliveira, S.; Mackall, J.; Arruda, M. Identification and electrophysiological characterization of early left atrial structural remodeling as a predictor for atrial fibrillation recurrence after pulmonary vein isolation. J. Cardiovasc. Electrophysiol. 2017, 28, 642–650. [Google Scholar]
- Zhang, Q.; Yip, G.W.; Yu, C.M. Approaching regional left atrial function by tissue Doppler velocity and strain imaging. Europace 2008, 10 (Suppl. 3), iii62–iii69. [Google Scholar] [CrossRef] [PubMed]
- Goldman, M.E.; Pearce, L.A.; Hart, R.G.; Zabalgoitia, M.; Asinger, R.W.; Safford, R.; Halperin, J.L. Pathophysiologic correlates of thromboembolism in nonvalvular atrial fibrillation: I. Reduced flow velocity in the left atrial appendage (The Stroke Prevention in Atrial Fibrillation [SPAF-III] study). J. Am. Soc. Echocardiogr. 1999, 12, 1080–1087. [Google Scholar] [CrossRef]
- Muller-Edenborn, B.; Chen, J.; Allgeier, J.; Didenko, M.; Moreno-Weidmann, Z.; Neumann, F.J.; Lehrmann, H.; Weber, R.; Arentz, T.; Jadidi, A. Amplified sinus-P-wave reveals localization and extent of left atrial low-voltage substrate: Implications for arrhythmia freedom following pulmonary vein isolation. Europace 2020, 22, 240–249. [Google Scholar] [CrossRef]
- Jadidi, A.; Müller-Edenborn, B.; Chen, J.; Keyl, C.; Weber, R.; Allgeier, J.; Moreno-Weidmann, Z.; Trenk, D.; Neumann, F.-J.; Lehrmann, H.; et al. The Duration of the Amplified Sinus-P-Wave Identifies Presence of Left Atrial Low Voltage Substrate and Predicts Outcome after Pulmonary Vein Isolation in Patients with Persistent Atrial Fibrillation. JACC Clin. Electrophysiol. 2018, 4, 531–543. [Google Scholar] [CrossRef]
- Eichenlaub, M.; Mueller-Edenborn, B.; Minners, J.; Jander, N.; Allgeier, M.; Lehrmann, H.; Schoechlin, S.; Allgeier, J.; Trenk, D.; Neumann, F.-J.; et al. Left Atrial Hypertension, Electrical Conduction Slowing, and Mechanical Dysfunction—The Pathophysiological Triad in Atrial Fibrillation-Associated Atrial Cardiomyopathy. Front. Physiol. 2021, 12, 670527. [Google Scholar] [CrossRef] [PubMed]
- Eichenlaub, M.; Mueller-Edenborn, B.; Minners, J.; Allgeier, M.; Lehrmann, H.; Allgeier, J.; Trenk, D.; Neumann, F.-J.; Jander, N.; Arentz, T.; et al. Echocardiographic diagnosis of atrial cardiomyopathy allows outcome prediction following pulmonary vein isolation. Clin. Res. Cardiol. 2021, 110, 1770–1780. [Google Scholar] [CrossRef] [PubMed]
- Jadidi, A.S.; Lehrmann, H.; Keyl, C.; Sorrel, J.; Markstein, V.; Minners, J.; Park, C.-I.; Denis, A.; Jaïs, P.; Hocini, M.; et al. Ablation of Persistent Atrial Fibrillation Targeting Low-Voltage Areas with Selective Activation Characteristics. Circ. Arrhythmia Electrophysiol. 2016, 9, e002962. [Google Scholar] [CrossRef] [PubMed]
- Yagishita, A.; Gimbel, J.R.; de Oliveira, S.; Manyam, H.; Sparano, D.; Cakulev, I.; Mackall, J.; Arruda, M. Long-Term Outcome of Left Atrial Voltage-Guided Substrate Ablation during Atrial Fibrillation: A Novel Adjunctive Ablation Strategy. J. Cardiovasc. Electrophysiol. 2017, 28, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Liao, J.-N.; Chao, T.-F.; Kuo, J.-Y.; Sung, K.-T.; Tsai, J.-P.; Lo, C.-I.; Lai, Y.-H.; Su, C.-H.; Hung, C.-L.; Yeh, H.-I. Global Left Atrial Longitudinal Strain Using 3-Beat Method Improves Risk Prediction of Stroke over Conventional Echocardiography in Atrial Fibrillation. Circ. Cardiovasc. Imaging 2020, 13, e010287. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; d’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.; Makimoto, H.; Dietrich, J.W.; Fochler, F.; Nentwich, K.; Krug, J.; Duncker, D.; Blockhaus, C.; Kelm, M.; Fürnkranz, A.; et al. Association of left atrial low-voltage area and thromboembolic risk in patients with atrial fibrillation. Europace 2018, 20, f359–f365. [Google Scholar] [CrossRef] [PubMed]
- Akoum, N.; Fernandez, G.; Wilson, B.; McGann, C.; Kholmovski, E.; Marrouche, N. Association of atrial fibrosis quantified using LGE-MRI with atrial appendage thrombus and spontaneous contrast on transesophageal echocardiography in patients with atrial fibrillation. J. Cardiovasc. Electrophysiol. 2013, 24, 1104–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; E Dilaveris, P.; et al. ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 128) | Thrombus (n = 26) | Control (n = 102) | p Value | |
|---|---|---|---|---|
| Age (years) | 65.8 (10.2) | 70.9 (9.2) | 64.5 (10.1) | 0.004 |
| Sinus rhythm, n (%) | 82 (64.1) | 9 (34.6) | 73 (71.6) | <0.001 |
| Persistent AF, n (%) | 101 (78.9) | 26 (100) | 75 (73.5) | 0.003 |
| Male, n (%) | 86 (67.2) | 18 (69.2) | 68 (66.7) | 0.804 |
| BMI, kg/m2 | 27.8 (4.1) | 18.0 (4.6) | 27.7 (4.0) | 0.784 |
| Hypertension, n (%) | 94 (73.4) | 22 (84.6) | 72 (70.6) | 0.148 |
| Diabetes, n (%) | 16 (12.5) | 5 (19.2) | 8 (7.8) | 0.110 |
| History of Stroke/TIA, n (%) | 9 (7.0) | 5 (19.2) | 4 (3.9) | 0.017 |
| CHD, n (%) | 32 (25) | 14 (53.8) | 18 (17.6) | <0.001 |
| CHA2DS2-VASc-score | 2.6 (1.7) | 4.2 (1.5) | 2.3 (1.5) | <0.001 |
| LAD, mm | 44.8 (5.7) | 48.8 (6.2) | 43.8 (5.2) | <0.001 |
| LAV, mL | 90.2 (25.4) | 105.6 (17.0) | 88.4 (25.6) | 0.027 |
| LVEDD, mm | 52.8 (6.7) | 56.3 (8.6) | 51.9 (5.9) | 0.003 |
| LVESD, mm | 35.7 (9.1) | 43.8 (12.0) | 33.6 (6.8) | <0.001 |
| LVEF (%) | 44.0 (14.9) | 29.4 (15.9) | 47.9 (11.9) | <0.001 |
| LAA-vel, cm/s | 36.9 (17.5) | 20.0 (7.5) | 42.1 (16.4) | <0.001 |
| Amiodaron, n (%) | 39 (30.5) | 7 (26.9) | 32 (31.4) | 0.660 |
| Flecanid, n (%) | 11 (8.6) | 0 (0) | 11 (10.8) | 0.022 |
| Sotalol, n (%) | 7 (5.5) | 0 (0) | 7 (6.9) | 0.070 |
| Propafenon, n (%) | 1 (0.8) | 0 (0) | 1 (1.0) | 0.499 |
| Beta-Blocker, n (%) | 90 (70.3) | 22 (84.6) | 68 (66.7) | 0.074 |
| SR Thrombus (n = 9) | SR Control (n = 73) | AF Thrombus (n = 17) | AF Control (n = 29) | p Value | |
|---|---|---|---|---|---|
| Age (years) | 66.4 (8) | 65.0 (10) | 68.2 (9) | 68.0 (8) | 0.06 |
| Male, n (%) | 9 (100) | 47 (64.4) | 9 (47.1) | 8 (72.7) | 0.09 |
| Persistent AF, n (%) | 9 (100) | 48 (65.8) | 17 (100) | 27 (93.1) | <0.001 |
| BMI, kg/m2 | 29.3 (4.0) | 27.8 (3.9) | 27.3 (4.5) | 25.3 (2.5) | 0.146 |
| Hypertension, n (%) | 7 (77.8) | 52 (71.2) | 15 (88.2) | 20 (69.0) | 0.422 |
| Diabetes, n (%) | 2 (22.2) | 8 (11.0) | 3 (17.6) | 3 (10.3) | 0.041 |
| History of Stroke/TIA, n (%) | 3 (33.3) | 3 (4.1) | 2 (11.8) | 1 (3.4) | 0.05 |
| CHD, n (%) | 3 (33.3) | 14 (19.2) | 11 (64.7) | 4 (13.8) | 0.001 |
| CHA2DS2-VASc-score, n (%) | 3.44 (1.5) | 2.38 (1.5) | 4.59 (1.4) | 1.9 (1.2) | <0.001 |
| LAD, mm | 50.4 (5.8) | 43.4 (5.6) | 48 (6.4) | 44.8 (3.9) | <0.001 |
| LAV, mm | 115.3 (9.5) | 88.6 (28.1) | 99.8 (18.7) | 88.0 (21.8) | 0.262 |
| LVEDD, mm | 61.1 (7.4) | 52.7 (5.8) | 53.8 (8.3) | 49.8 (5.6) | <0.001 |
| LVESD, mm | 49.0 (12.4) | 33.9 (7.4) | 41.1 (11.1) | 32.9 (5.2) | <0.001 |
| LVEF(%) | 31.2 (17.3) | 47.9 (11.8) | 28.5 (15.7) | 47.7 (12.5) | <0.001 |
| LAA-Vel, cm/s | 22.4 (7.5) | 41.9 (16.1) | 18.6 (7.3) | 42.6 (17.5) | <0.001 |
| Amiodaron, n (%) | 5 (55.6) | 25 (34.2) | 2 (11.8) | 7 (24.1) | 0.078 |
| Flecanid, n (%) | 0 (0) | 7 (9.6) | 0 (0) | 4 (13.8) | 0.132 |
| Sotalol, n (%) | 0 (0) | 5 (6.8) | 0 (0) | 2 (6.9) | 0.350 |
| Propafenon, n (%) | 0 (0) | 1 (1.4) | 0 (0) | 0 (0) | 0.770 |
| Beta-Blocker, n (%) | 6 (66.7) | 47 (64.4) | 16 (94.1) | 21 (72.4) | 0.418 |
| Value, % | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|
| LA-GLS (17.45%) | 84.6 | 63.6 | 37.9 | 94.3 |
| APWD (165 ms) | 88.5 | 75.5 | 47.9 | 96.2 |
| Patients, n (%) | Negative by LA-GLS and APWD | Negative by LA-GLS Positive by APWD | Positive by LA-GLS Negative by APWD | Positive by LA-GLS and APWD |
|---|---|---|---|---|
| Thrombus group, (n = 26) | 1 (3.8) | 2 (7.7) | 2 (7.7) | 21 (80.8) |
| Control group, (n = 102) | 55 (53.9) | 15 (14.7) | 21 (20.6) | 11 (10.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, T.; Patrick, S.; Mayer, L.K.; Müller-Edenborn, B.; Eichenlaub, M.; Allgeier, M.; Allgeier, J.; Lehrmann, H.; Ahlgrim, C.; Bohnen, M.; et al. Echocardiographic and Electrocardiographic Determinants of Atrial Cardiomyopathy Identify Patients with Atrial Fibrillation at Risk for Left Atrial Thrombogenesis. J. Clin. Med. 2022, 11, 1332. https://doi.org/10.3390/jcm11051332
Huang T, Patrick S, Mayer LK, Müller-Edenborn B, Eichenlaub M, Allgeier M, Allgeier J, Lehrmann H, Ahlgrim C, Bohnen M, et al. Echocardiographic and Electrocardiographic Determinants of Atrial Cardiomyopathy Identify Patients with Atrial Fibrillation at Risk for Left Atrial Thrombogenesis. Journal of Clinical Medicine. 2022; 11(5):1332. https://doi.org/10.3390/jcm11051332
Chicago/Turabian StyleHuang, Taiyuan, Schurr Patrick, Louisa Katharina Mayer, Björn Müller-Edenborn, Martin Eichenlaub, Martin Allgeier, Jürgen Allgeier, Heiko Lehrmann, Christoph Ahlgrim, Marius Bohnen, and et al. 2022. "Echocardiographic and Electrocardiographic Determinants of Atrial Cardiomyopathy Identify Patients with Atrial Fibrillation at Risk for Left Atrial Thrombogenesis" Journal of Clinical Medicine 11, no. 5: 1332. https://doi.org/10.3390/jcm11051332
APA StyleHuang, T., Patrick, S., Mayer, L. K., Müller-Edenborn, B., Eichenlaub, M., Allgeier, M., Allgeier, J., Lehrmann, H., Ahlgrim, C., Bohnen, M., Schoechlin, S., Trenk, D., Jander, N., Neumann, F. J., Arentz, T., & Jadidi, A. (2022). Echocardiographic and Electrocardiographic Determinants of Atrial Cardiomyopathy Identify Patients with Atrial Fibrillation at Risk for Left Atrial Thrombogenesis. Journal of Clinical Medicine, 11(5), 1332. https://doi.org/10.3390/jcm11051332