
Bridge of Tunneled Cuffed Catheter as a Risk for Future Arteriovenous Fistulae Failure


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Research Samples
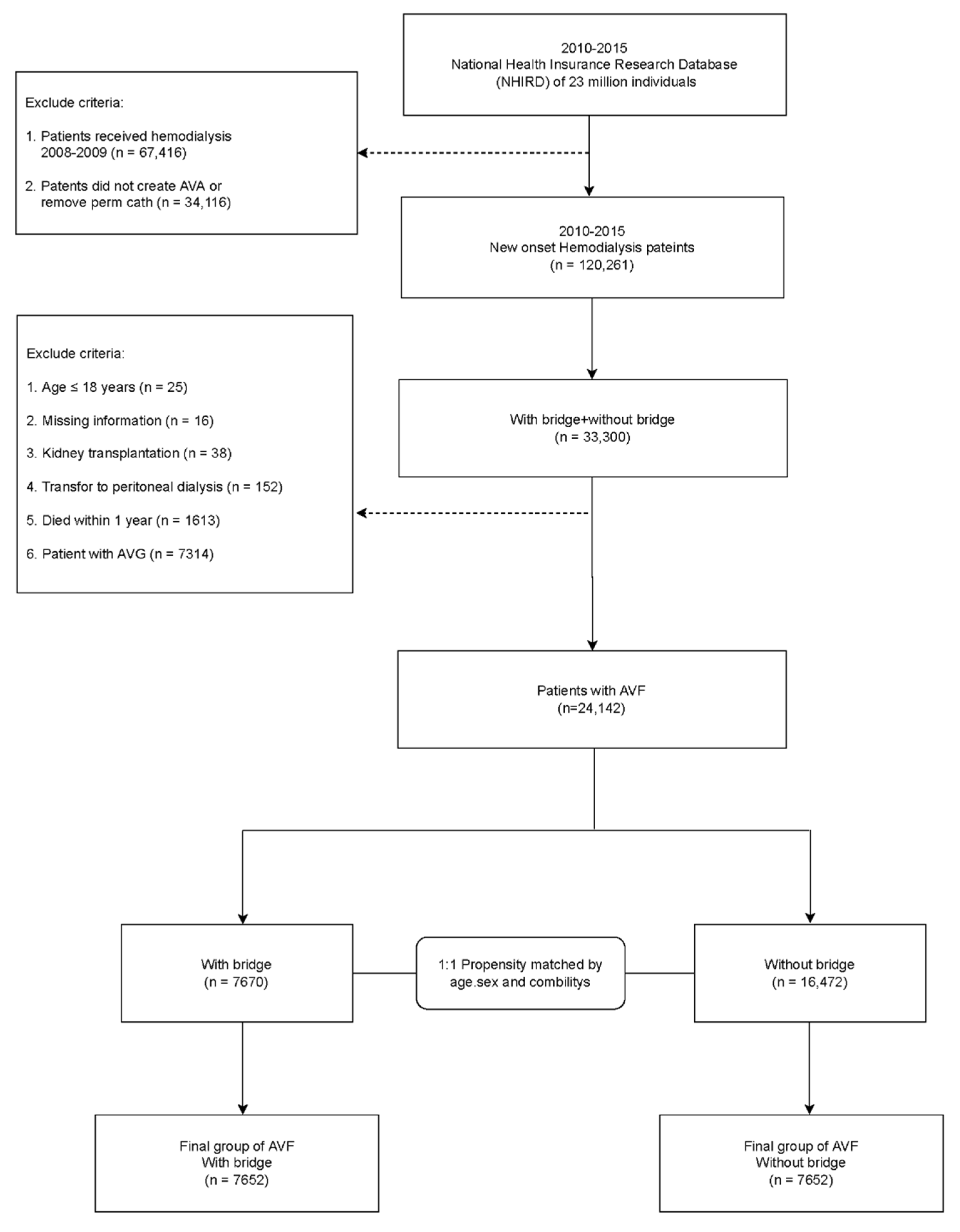
2.2. Study Population and Exclusion Criteria
2.3. Statistical Analyses
3. Results
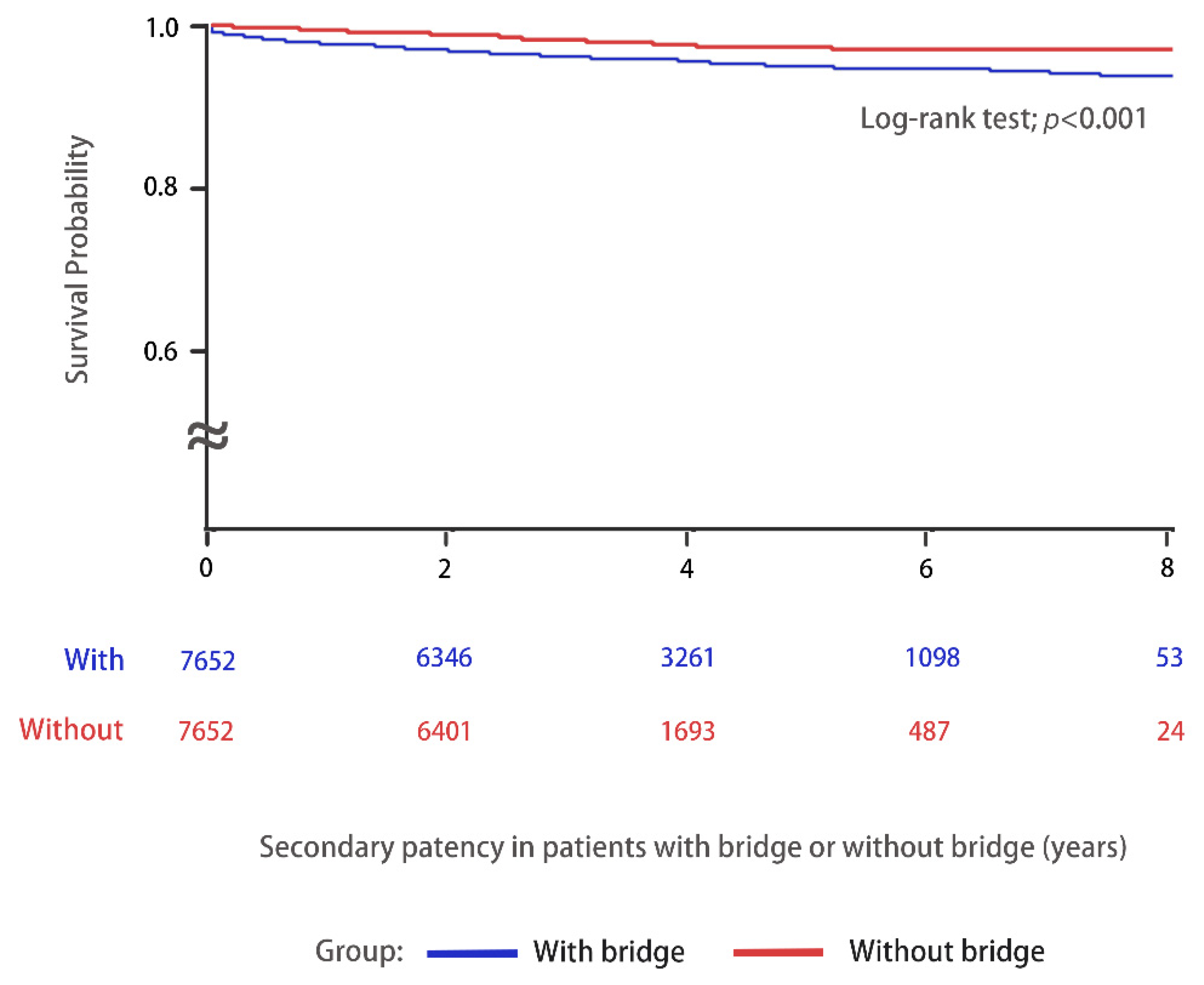
Comparisons of Vascular Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lok, C.E.; Huber, T.S.; Lee, T.; Shenoy, S.; Yevzlin, A.S.; Abreo, K.; Allon, M.; Asif, A.; Astor, B.C.; Glickman, M.H.; et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. Am. J. Kidney Dis. 2020, 75, S1–S164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almasri, J.; Alsawas, M.; Mainou, M.; Mustafa, R.A.; Wang, Z.; Woo, K.; Cull, D.L.; Murad, M.H. Outcomes of vascular access for hemodialysis: A systematic review and meta-analysis. J. Vasc. Surg. 2016, 64, 236–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celik, S.; Gok, O.E.; Ulusal, O.G.; Selen, T.; Ayli, M.D. The impact of arteriovenous fistulas and tunneled cuffed venous catheters on morbidity and mortality in hemodialysis patients: A single center experience. Int. J. Artif. Organs. 2021, 44, 229–236. [Google Scholar] [CrossRef]
- Shechter, S.M.; Skandari, M.R.; Zalunardo, N. Timing of arteriovenous fistula creation in patients With CKD: A decision analysis. Am. J. Kidney Dis. 2014, 63, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Schmidli, J.; Widmer, M.K.; Basile, C.; de Donato, G.; Gallieni, M.; Gibbons, C.P.; Haage, P.; Hamilton, G.; Hedin, U.; Kamper, L.; et al. Editor’s Choice—Vascular Access: 2018 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2018, 55, 757–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vassalotti, J.A.; Jennings, W.C.; Beathard, G.A.; Neumann, M.; Caponi, S.; Fox, C.H.; Spergel, L.M. Fistula First Breakthrough Initiative Community Education Committee. Fistula first breakthrough initiative: Targeting catheter last in fistula first. Semin. Dial. 2012, 25, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Lee, T. Fistula First Initiative: Historical Impact on Vascular Access Practice Patterns and Influence on Future Vascular Access Care. Cardiovasc. Eng. Technol. 2017, 8, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Society of Nephrology. Annual Report on Kidney Disease in Taiwan; Taiwan Society of Nephrology: Taipei, Taiwan, 2019. [Google Scholar]
- Canaud, B.; Tong, L.; Tentori, F.; Akiba, T.; Karaboyas, A.; Gillespie, B.; Akizawa, T.; Pisoni, R.L.; Bommer, J.; Port, F.K. Clinical practices and outcomes in elderly hemodialysis patients: Results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Clin. J. Am. Soc. Nephrol. 2011, 6, 1651–1662. [Google Scholar] [CrossRef] [Green Version]
- Al-Jaishi, A.A.; Oliver, M.J.; Thomas, S.M.; Lok, C.E.; Zhang, J.C.; Garg, A.X.; Kosa, S.D.; Quinn, R.R.; Moist, L.M. Patency rates of the arteriovenous fistula for hemodialysis: A systematic review and meta-analysis. Am. J. Kidney Dis. 2014, 63, 464–478. [Google Scholar] [CrossRef]
- Lazarides, M.K.; Georgiadis, G.S.; Antoniou, G.A.; Staramos, D.N. A meta-analysis of dialysis access outcome in elderly patients. J. Vasc. Surg. 2007, 45, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Ye, D.; Yang, L.; Ye, W.; Zhan, D.; Zhang, L.; Xiao, J.; Zeng, Y.; Chen, Q. A meta-analysis of the association between diabetic patients and AVF failure in dialysis. Ren. Fail. 2018, 40, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Sedlacek, M.; Teodorescu, V.; Falk, A.; Vassalotti, J.A.; Uribarri, J. Hemodialysis access placement with preoperative noninvasive vascular mapping: Comparison between patients with and without diabetes. Am. J. Kidney Dis. 2001, 38, 560–564. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Chang, J.M.; Hwang, S.J.; Tsai, J.C.; Wang, C.S.; Mai, H.C.; Lin, F.H.; Su, H.M.; Chen, H.C. Significant correlation between ankle-brachial index and vascular access failure in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2009, 4, 128–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Work, J. Hemodialysis catheters and ports. Semin. Nephrol. 2002, 22, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Poinen, K.; Quinn, R.R.; Clarke, A.; Ravani, P.; Hiremath, S.; Miller, L.M.; Blake, P.G.; Oliver, M.J. Complications from tunneled hemodialysis catheters: A Canadian observational cohort study. Am. J. Kidney Dis. 2019, 73, 467–475. [Google Scholar] [CrossRef]
- Agarwal, A.K.; Patel, B.M.; Haddad, N.J. Central vein stenosis: A nephrologist’s perspective. Semin. Dial. 2007, 20, 53–62. [Google Scholar] [CrossRef]
- MacRae, J.M.; Ahmed, A.; Johnson, N.; Levin, A.; Kiaii, M. Central vein stenosis: A common problem in patients on hemodialysis. ASAIO J. 2005, 51, 77–81. [Google Scholar] [CrossRef]
- Forauer, A.R.; Theoharis, C. Histologic changes in the human vein wall adjacent to indwelling central venous catheters. J. Vasc. Interv. Radiol. 2003, 14, 1163–1168. [Google Scholar] [CrossRef]
- Shingarev, R.; Barker-Finkel, J.; Allon, M. Association of hemodialysis central venous catheter use with ipsilateral arteriovenous vascular access survival. Am. J. Kidney Dis. 2012, 60, 983–989. [Google Scholar] [CrossRef] [Green Version]
- Rayner, H.C.R.; Pisoni, R.L.; Gillespie, B.W.; Goodkin, D.A.; Akiba, T.; Akizawa, T.; Saito, A.; Young, E.W.; Port, F.K. Creation, cannulation and survival of arteriovenous fistulae: Data from the Dialysis Outcomes and Practice Patterns Study. Kidney Int. 2003, 63, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Pisoni, R.L.; Young, E.W.; Dykstra, D.M.; Greenwood, R.N.; Hecking, E.; Gillespie, B.; Wolfe, R.A.; Goodkin, D.A.; Held, P.J. Vascular access use in Europe and the United States: Results from the DOPPS. Kidney Int. 2002, 61, 305–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, T.; Ullah, A.; Allon, M.; Succop, P.; El-Khatib, M.; Munda, R.; Roy-Chaudhury, P. Decreased cumulative access survival in arteriovenous fistulas requiring interventions to promote maturation. Clin. J. Am. Soc. Nephrol. 2011, 6, 575–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elkassaby, M.; Elsaadany, N.; Mowaphy, K.; Soliman, M. Balloon-assisted maturation of autogenous arteriovenous fistulae: A randomized controlled prospective study. Vascular 2021, 29, 776–783. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, S.A.; Usoh, F.; Hingorani, A.; Iadgarova, E.; Boniscavage, P.; Eisenberg, J.; Ascher, E.; Marks, N. The clinical efficacy of balloon-assisted maturation of autogenous arteriovenous fistulae. Ann. Vasc. Surg. 2017, 41, 41–45. [Google Scholar] [CrossRef]
- Peterson, W.J.; Barker, J.; Allon, M. Disparities in fistula maturation persist despite preoperative vascular mapping. Clin. J. Am. Soc. Nephrol. 2008, 3, 437–441. [Google Scholar] [CrossRef] [Green Version]
- Monroy-Cuadros, M.; Yilmaz, S.; Salazar-Bañuelos, A.; Doig, C. Risk factors associated with patency loss of hemodialysis vascular access within 6 months. Clin. J. Am. Soc. Nephrol. 2010, 5, 1787–1792. [Google Scholar] [CrossRef] [Green Version]
- Li, H.L.; Chan, Y.C.; Cui, D.; Liu, J.; Wang, M.; Li, N.; Pai, P.; Cheng, S.W. Predictors of primary functional maturation of autogenous radiocephalic arteriovenous fistula in a cohort of Asian patients. Ann. Vasc. Surg. 2020, 66, 326–333. [Google Scholar] [CrossRef]
- Bashar, K.; Conlon, P.J.; Kheirelseid, E.A.; Aherne, T.; Walsh, S.R.; Leahy, A. Arteriovenous fistula in dialysis patients: Factors implicated in early and late AVF maturation failure. Surgeon 2016, 14, 294–300. [Google Scholar] [CrossRef]
- Masengu, A.; McDaid, J.; Maxwell, A.P.; Hanko, J.B. Preoperative radial artery volume flow is predictive of arteriovenous fistula outcomes. J. Vasc. Surg. 2016, 63, 429–435. [Google Scholar] [CrossRef] [Green Version]
- Weber, C.L.; Djurdjev, O.; Levin, A.; Kiaii, M. Outcomes of vascular access creation prior to dialysis: Building the case for early referral. ASAIO J. 2009, 55, 355–360. [Google Scholar] [CrossRef]
- Lindhard, K.; Rix, M.; Heaf, J.G.; Hansen, H.P.; Pedersen, B.L.; Jensen, B.L.; Hansen, D. Effect of far infrared therapy on arteriovenous fistula maturation, survival and stenosis in hemodialysis patients, a randomized, controlled clinical trial: The FAITH on fistula trial. BMC Nephrol. 2021, 22, 283. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| AVF | ||||||
|---|---|---|---|---|---|---|
| Variables | Before Matching | p | After Matching | p | ||
| With Bridge (N = 7670) | Without Bridge (N = 16,472) | With Bridge (N = 7652) | Without Bridge (N = 7652) | |||
| Gender | ||||||
| Male | 4486 (58.49) | 9453 (57.39) | 0.107 | 4472 (58.44) | 4492 (58.70) | 0.742 |
| Female | 3184 (41.51) | 7019 (42.61) | 3180 (41.56) | 3160 (41.30) | ||
| Age stratified, y | 62.79 ± 13.42 | 64.45 ± 12.58 | <0.001 | 62.81 ± 13.42 | 62.89 ± 12.97 | 0.702 |
| Age group | ||||||
| <50 | 1207 (15.74) | 1972 (11.97) | <0.001 | 1203 (15.72) | 1147 (14.99) | 0.390 |
| 50–64 | 2865 (37.35) | 5982 (36.32) | 2851 (37.26) | 2907 (37.99) | ||
| ≥65 | 3598 (46.91) | 8518 (51.71) | 3598 (47.02) | 3598 (47.02) | ||
| Comorbidities | ||||||
| Hypertension | 4270 (55.67) | 8884 (53.93) | 0.011 | 4259 (55.66) | 4320 (56.46) | 0.320 |
| Diabetes mellitus | 4807 (62.67) | 8687 (52.74) | <0.001 | 4789 (62.58) | 4819 (62.98) | 0.615 |
| Hyperlipidemia | 2469 (32.19) | 4547 (27.60) | <0.001 | 2454 (32.07) | 2404 (31.42) | 0.385 |
| CAD | 3611 (47.08) | 6403 (38.87) | <0.001 | 3593 (46.96) | 3644 (47.62) | 0.409 |
| Stroke | 2224 (29.00) | 3793 (23.03) | <0.001 | 2208 (28.86) | 2231 (29.16) | 0.682 |
| PVD | 1630 (21.25) | 2549 (15.47) | <0.001 | 1612 (21.07) | 1656 (21.64) | 0.385 |
| COPD | 2057 (26.82) | 3319 (20.15) | <0.001 | 2041 (26.67) | 1972 (25.77) | 0.204 |
| Cancer | 49 (0.64) | 130 (0.79) | 0.204 | 49 (0.64) | 51 (0.67) | 0.841 |
| CCIS stratified | ||||||
| 0–2 | 261 (3.40) | 952 (5.78) | <0.001 | 261 (3.41) | 338 (4.41) | <0.001 |
| 3–5 | 2421 (31.56) | 5541 (33.64) | 2421 (31.63) | 2167 (28.32) | ||
| ≥6 | 4988 (65.03) | 9979 (60.58) | 4970 (64.95) | 5147 (67.26) | ||
| Before Matching | ||||
| Variables | With Bridge (N = 7670) | Without Bridge (N = 16,472) | Crude HR (95% CI) | Adjusted HR (95% CI) |
| IR | ||||
| New AVF creation | 0.338 | 0.138 | 2.54 (2.15–3.00) *** | 2.50 (2.12–2.96) *** |
| New AVG creation | 0.146 | 0.041 | 1.69 (1.35–2.12) *** | 1.65 (1.32–2.07) *** |
| After Matching | ||||
| Variables | With Bridge (N = 7652) | Without Bridge (N = 7652) | Crude HR (95% CI) | Adjusted HR (95% CI) |
| IR | ||||
| New AVF creation | 0.334 | 0.119 | 2.17 (1.77–2.66) *** | 2.17 (1.77–2.67) *** |
| New AVG creation | 0.147 | 0.036 | 1.51 (1.15–1.98) ** | 1.52 (1.15–1.99) ** |
| New AVF Creation | New AVG Creation | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variables (Years) | With Bridge (N = 7661) | Without Bridge (N = 7661) | p-Value | With Bridge (N = 7661) | Without Bridge (N = 7661) | p-Value | ||||
| n | PY | n | PY | n | PY | n | PY | |||
| 0 ≤ Follow up time < 1 | 72 | 7.849 | 14 | 8.492 | <0.001 | 44 | 14.967 | 18 | 9.218 | 0.143 |
| 1 ≤ Follow up time < 2 | 20 | 31.663 | 12 | 17.215 | 0.787 | 26 | 39.961 | 13 | 18.436 | 0.812 |
| 2 ≤ Follow up time < 3 | 17 | 41.590 | 12 | 28.807 | 0.959 | 16 | 39.148 | 13 | 31.181 | 0.957 |
| Follow up time ≥ 3 | 19 | 79.808 | 6 | 25.032 | 0.988 | 25 | 107.356 | 10 | 40.301 | 0.865 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-K.; Huang, Y.-C.; Lin, C.-H.; Chen, M. Bridge of Tunneled Cuffed Catheter as a Risk for Future Arteriovenous Fistulae Failure. J. Clin. Med. 2022, 11, 1289. https://doi.org/10.3390/jcm11051289
Wu C-K, Huang Y-C, Lin C-H, Chen M. Bridge of Tunneled Cuffed Catheter as a Risk for Future Arteriovenous Fistulae Failure. Journal of Clinical Medicine. 2022; 11(5):1289. https://doi.org/10.3390/jcm11051289
Chicago/Turabian StyleWu, Chung-Kuan, Yen-Chun Huang, Chia-Hsun Lin, and Mingchih Chen. 2022. "Bridge of Tunneled Cuffed Catheter as a Risk for Future Arteriovenous Fistulae Failure" Journal of Clinical Medicine 11, no. 5: 1289. https://doi.org/10.3390/jcm11051289
APA StyleWu, C.-K., Huang, Y.-C., Lin, C.-H., & Chen, M. (2022). Bridge of Tunneled Cuffed Catheter as a Risk for Future Arteriovenous Fistulae Failure. Journal of Clinical Medicine, 11(5), 1289. https://doi.org/10.3390/jcm11051289