
Disease Severity and Risk Factors of 30-Day Hospital Readmission in Pediatric Hospitalizations for Pneumonia

 ,
, 
Abstract
:1. Introduction
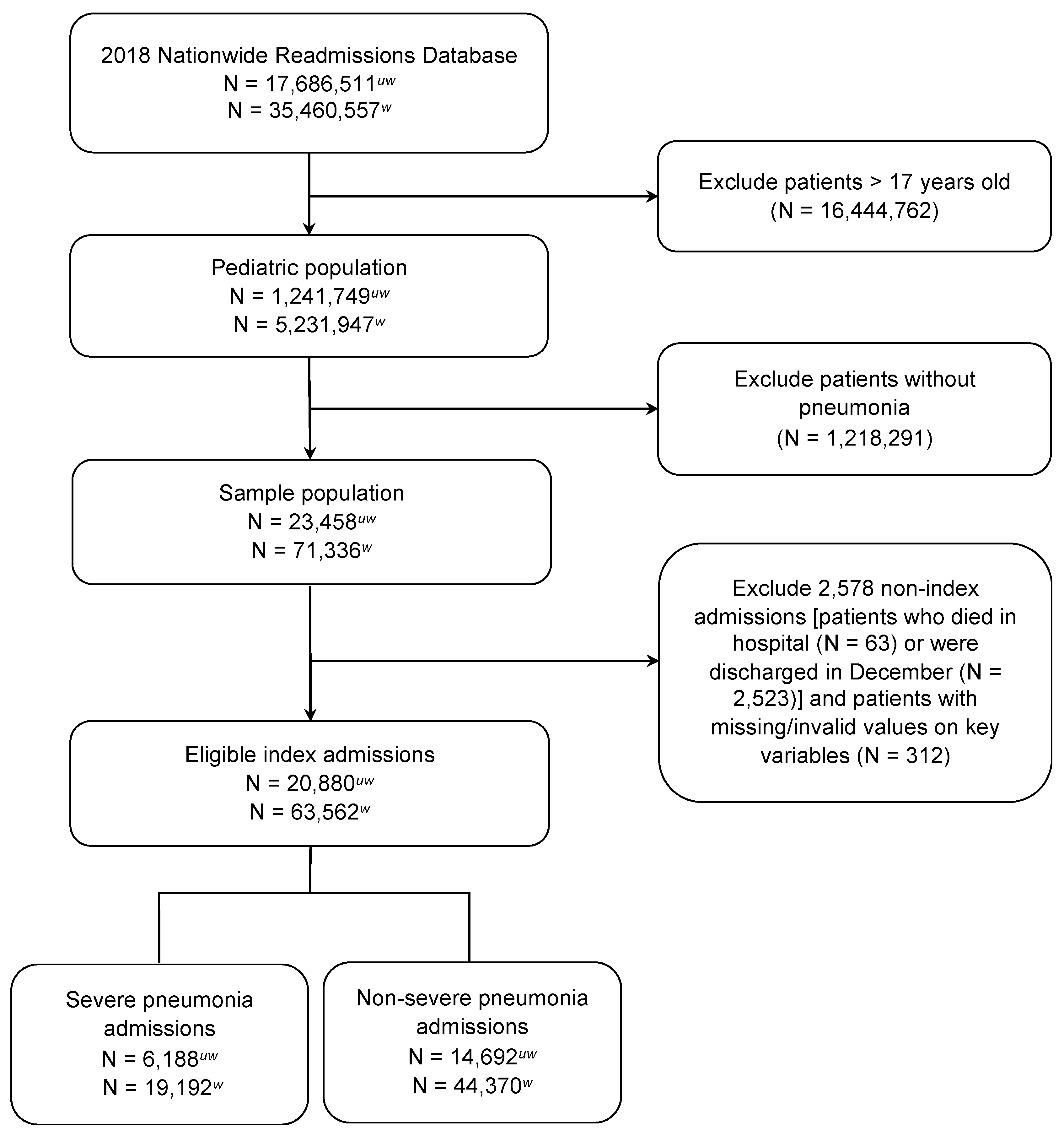
2. Materials and Methods
3. Results
3.1. Readmissions and Related Clinical and Economic Burden
3.2. Risk Factors for Readmission
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDermott, K.W.; Jiang, H.J. Characteristics and costs of potentially preventable inpatient stays, 2017: Statistical brief #259. In Healthcare Cost and Utilization Project (HCUP) Statistical Briefs; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2006. [Google Scholar]
- Toomey, S.L.; Peltz, A.; Loren, S.; Tracy, M.; Williams, K.; Pengeroth, L.; Marie, A.S.; Onorato, S.; Schuster, M.A. Potentially preventable 30-day hospital readmissions at a children’s hospital. Pediatrics 2016, 138, e20154182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payne, N.R.; Flood, A. Preventing pediatric readmissions: Which ones and how? J. Pediatr. 2015, 166, 519–520. [Google Scholar] [CrossRef] [PubMed]
- Fontanarosa, P.B.; McNutt, R.A. Revisiting hospital readmissions. J. Am. Med. Assooc. 2013, 309, 398–400. [Google Scholar] [CrossRef]
- Joynt, K.E.; Jha, A.K. Thirty-Day readmissions—Truth and consequences. N. Engl. J. Med. 2012, 366, 1366–1369. [Google Scholar] [CrossRef] [Green Version]
- Kocher, R.P.; Adashi, E.Y. Hospital readmissions and the affordable care act: Paying for coordinated quality care. J. Am. Med. Assooc. 2011, 306, 1794–1795. [Google Scholar] [CrossRef] [PubMed]
- AHRQ. Pediatric 30-Day Lower Respiratory Infection Readmission Measure; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2021. Available online: https://www.ahrq.gov/pqmp/measures/pediatric-respiratory-infection-readmissions.html (accessed on 31 January 2022).
- Witt, W.P.; Weiss, A.J.; Elixhauser, A. Overview of hospital stays for children in the United States, 2012: Statistical brief #187. In Healthcare Cost and Utilization Project (HCUP) Statistical Briefs; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2006. [Google Scholar]
- Black, R.E.; Cousens, S.; Johnson, H.L.; Lawn, J.; Rudan, I.; Bassani, D.; Jha, P.; Campbell, H.; Walker, C.F.; Cibulskis, R.; et al. Global, regional, and national causes of child mortality in 2008: A systematic analysis. Lancet 2010, 375, 1969–1987. [Google Scholar] [CrossRef]
- Liang, L.; Moore, B.; Soni, A. National inpatient hospital costs: The most expensive conditions by payer, 2017: Statistical brief #261. In Healthcare Cost and Utilization Project (HCUP) Statistical Briefs; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2006. [Google Scholar]
- Dean, P.; Florin, T. Factors associated with pneumonia severity in children: A systematic review. J. Pediatr. Infect. Dis. Soc. 2018, 7, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.J.; Zhu, Y.; Grijalva, C.G.; Self, W.H.; Harrell, F.E.; Reed, C.; Stockmann, C.; Arnold, S.R.; Ampofo, K.K.; Anderson, E.J.; et al. Predicting severe pneumonia outcomes in children. Pediatrics 2016, 138, e20161019. [Google Scholar] [CrossRef] [Green Version]
- De Benedictis, F.M.; Kerem, E.; Chang, A.B.; Colin, A.A.; Zar, H.J.; Bush, A. Complicated pneumonia in children. Lancet 2020, 396, 786–798. [Google Scholar] [CrossRef]
- Auger, K.A.; Harris, J.M.; Gay, J.C.; Teufel, R.; McClead, R.E.; Neuman, M.I.; Agrawal, R.; Simon, H.K.; Peltz, A.; Tejedor-Sojo, J.; et al. Progress (?) toward reducing pediatric readmissions. J. Hosp. Med. 2019, 14, 618–621. [Google Scholar] [CrossRef] [Green Version]
- Zar, H.J.; Andronikou, S.; Nicol, M. Advances in the diagnosis of pneumonia in children. Br. Med. J. 2017, 358, j2739. [Google Scholar] [CrossRef] [PubMed]
- Gereige, R.S.; Laufer, P.M. Pneumonia. Pediatr. Rev. 2013, 34, 438–456. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Williams, D.J.; Arnold, S.R.; Ampofo, K.; Bramley, A.M.; Reed, C.; Stockmann, C.; Anderson, E.J.; Grijalva, C.G.; Self, W.H.; et al. Community-acquired pneumonia requiring hospitalization among U.S. children. N. Engl. J. Med. 2015, 372, 835–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffin, M.R.; Zhu, Y.; Moore, M.R.; Whitney, C.G.; Grijalva, C.U.S. hospitalizations for pneumonia after a decade of pneumococcal vaccination. N. Engl. J. Med. 2013, 369, 155–163. [Google Scholar] [CrossRef] [Green Version]
- HCUP Nationwide Readmissions Database (NRD). Healthcare Cost and Utilization Project (HCUP). Available online: https://www.hcup-us.ahrq.gov/nrdoverview.jsp (accessed on 31 January 2022).
- Whittle, J.; Fine, M.J.; Joyce, D.Z.; Lave, J.R.; Young, W.W.; Hough, L.J.; Kapoor, W.N. Community-acquired pneumonia: Can it be defined with claims data? Am. J. Med. Qual. 1997, 12, 187–193. [Google Scholar] [CrossRef]
- Barber, C.; Lacaille, D.; Fortin, P.R. Systematic review of validation studies of the use of administrative data to identify serious infections. Arthritis Care Res. 2013, 65, 1343–1357. [Google Scholar] [CrossRef] [Green Version]
- Olasupo, O.; Xiao, H.; Brown, J.D. Relative clinical and cost burden of community-acquired pneumonia hospitalizations in older adults in the United States—A cross-sectional analysis. Vaccines 2018, 6, 59. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.J.; Shah, S.S.; Myers, A.; Hall, M.; Auger, K.; Queen, M.A.; Jerardi, K.E.; McClain, L.; Wiggleton, C.; Tieder, J.S. Identifying pediatric community-acquired pneumonia hospitalizations: Accuracy of administrative billing codes. JAMA Pediatr. 2013, 167, 851–858. [Google Scholar] [CrossRef] [Green Version]
- Florin, T.A.; Brokamp, C.; Mantyla, R.; DePaoli, B.; Ruddy, R.; Shah, S.S.; Ambroggio, L. Validation of the pediatric infectious diseases society–infectious diseases society of America severity criteria in children with community-acquired pneumonia. Clin. Infect. Dis. 2018, 67, 112–119. [Google Scholar] [CrossRef]
- Harris, M.; Clark, J.; Coote, N.; Fletcher, P.; Harnden, A.; Mckean, M.; Thomson, A. British Thoracic Society guidelines for the management of community acquired pneumonia in children: Update 2011. Thorax 2011, 66, ii1. [Google Scholar] [CrossRef] [Green Version]
- HCUP. Elixhauser Comorbidity Software Refined for ICD-10-CM; Version 2021.1; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2021. Available online: https://www.hcup-us.ahrq.gov/toolssoftware/comorbidityicd10/comorbidity_icd10.jsp (accessed on 31 January 2022).
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity measures for use with administrative data. Med. Care 1998, 36, 8–27. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, S.M.; DeLong, E.R.; Peterson, E.D. Impact of case volume on hospital performance assessment. Arch. Intern. Med. 2008, 168, 1277–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- HCUP. Cost-to-Charge Ratio (CCR) for the Nationwide Readmissions Database (NRD); Agency for Healthcare Research and Quality: Rockville, MD, USA, 2021. Available online: https://www.hcup-us.ahrq.gov/db/ccr/ip-ccr/ip-ccr.jsp (accessed on 31 January 2022).
- Neuman, M.I.; Hall, M.; Gay, J.C.; Blaschke, A.J.; Williams, D.J.; Parikh, K.; Hersh, A.L.; Brogan, T.V.; Gerber, J.S.; Grijalva, C.; et al. Readmissions among children previously hospitalized with pneumonia. Pediatrics 2014, 134, 100–109. [Google Scholar] [CrossRef] [Green Version]
- Faverio, P.; Compagnoni, M.M.; Della Zoppa, M.; Pesci, A.; Cantarutti, A.; Merlino, L.; Luppi, F.; Corrao, G. Rehospitalization for pneumonia after first pneumonia admission: Incidence and predictors in a population-based cohort study. PLoS ONE 2020, 15, e0235468. [Google Scholar] [CrossRef] [PubMed]
- Berry, J.G.; Toomey, S.L.; Zaslavsky, A.M.; Jha, A.K.; Nakamura, M.M.; Klein, D.J.; Feng, J.Y.; Shulman, S.; Chiang, V.W.; Kaplan, W.; et al. Pediatric readmission prevalence and variability across hospitals. J. Am. Med. Assooc. 2013, 309, 372–380. [Google Scholar] [CrossRef] [Green Version]
- Shorr, A.F.; Zilberberg, M.D.; Reichley, R.; Kan, J.; Hoban, A.; Hoffman, J.; Micek, S.T.; Kollef, M.H. Readmission following hospitalization for pneumonia: The impact of pneumonia type and its implication for hospitals. Clin. Infect. Dis. 2013, 57, 362–367. [Google Scholar] [CrossRef] [Green Version]
- Weinreich, M.; Nguyen, O.K.; Wang, D.; Mayo, H.; Mortensen, E.; Halm, E.A.; Makam, A.N. Predicting the risk of readmission in pneumonia. A systematic review of model performance. Ann. Am. Thorac. Soc. 2016, 13, 1607–1614. [Google Scholar] [CrossRef] [Green Version]
- Leyenaar, J.K.; Lagu, T.; Shieh, M.-S.; Pekow, P.S.; Lindenauer, P.K. Management and outcomes of pneumonia among children with complex chronic conditions. Pediatr. Infect. Dis. J. 2014, 33, 907–911. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, M.M.; Zaslavsky, A.M.; Toomey, S.L.; Petty, C.R.; Bryant, M.C.; Geanacopoulos, A.T.; Jha, A.K.; Schuster, M.A. Pediatric readmissions after hospitalizations for lower respiratory infections. Pediatrics 2017, 140, e20160938. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Feng, Z.; Shuai, J.; Liu, J.; Li, G. Risk factors of 90-day rehospitalization following discharge of pediatric patients hospitalized with mycoplasma Pneumoniae pneumonia. BMC Infect. Dis. 2019, 19, 966. [Google Scholar] [CrossRef]
- Ambroggio, L.; Herman, H.; Fain, E.; Huang, G.; Florin, T.A. Clinical risk factors for revisits for children with community-acquired pneumonia. Hosp. Pediatr. 2018, 8, 718–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, C.J.; Porter, J.J.; Lipsett, S.C.; Monuteaux, M.C.; Hirsch, A.W.; Neuman, M.I. Variation in management and outcomes of children with complicated pneumonia. Hosp. Pediatr. 2021, 11, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Gay, J.C.; Hall, M.; Markham, J.; Bettenhausen, J.L.; Doupnik, S.K.; Berry, J.G. Association of extending hospital length of stay with reduced pediatric hospital readmissions. JAMA Pediatr. 2019, 173, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Brogan, T.V.; Hall, M.; Williams, D.J.; Neuman, M.I.; Grijalva, C.; Farris, R.W.; Shah, S.S. Variability in processes of care and outcomes among children hospitalized with community-acquired pneumonia. Pediatr. Infect. Dis. J. 2012, 31, 1036–1041. [Google Scholar] [CrossRef] [Green Version]
- McCabe, C.; Kirchner, C.; Zhang, H.; Daley, J.; Fisman, D.N. Guideline-concordant therapy and reduced mortality and length of stay in adults with community-acquired pneumonia: Playing by the rules. Arch. Intern. Med. 2009, 169, 1525–1531. [Google Scholar] [CrossRef] [Green Version]
- Gohil, S.K.; Datta, R.; Cao, C.; Phelan, M.J.; Nguyen, V.; Rowther, A.A.; Huang, S.S. Impact of hospital population case-mix, including poverty, on hospital all-cause and infection-related 30-day readmission rates. Clin. Infect. Dis. 2015, 61, 1235–1243. [Google Scholar] [CrossRef] [Green Version]
- Brittan, M.; Shah, S.S.; Auger, K.A. Preventing pediatric readmissions: How does the hospital fit in? Pediatrics 2016, 138, e20161643. [Google Scholar] [CrossRef] [Green Version]
- Dejong, N.A.; Kimple, K.S.; Morreale, M.C.; Hang, S.; Davis, D.; Steiner, M.J. A quality improvement intervention bundle to reduce 30-day pediatric readmissions. Pediatr. Qual. Saf. 2020, 5, e264. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, M.M.; Toomey, S.L.; Zaslavsky, A.M.; Berry, J.G.; Lorch, S.A.; Jha, A.K.; Bryant, M.C.; Geanacopoulos, A.T.; Loren, S.S.; Pain, D.; et al. Measuring pediatric hospital readmission rates to drive quality improvement. Acad. Pediatr. 2014, 14, S39–S46. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total Sample N = 20,880 (100%) | Non-Severe Pneumonia N = 14,692 (70.4%) | Severe Pneumonia N = 6188 (29.6%) | p-Value |
|---|---|---|---|---|
| Patient Demographic Characteristics | ||||
| Age group | <0.01 | |||
| <1 year | 2450 (11.7) | 1622 (11.0) | 828 (13.4) | |
| 1–4 years | 9782 (46.9) | 6807 (46.3) | 2975 (48.1) | |
| 5–12 years | 6504 (31.2) | 4747 (32.3) | 1757 (28.4) | |
| 13–17 years | 2144 (10.3) | 1516 (10.3) | 628 (10.2) | |
| Female | 9882 (47.3) | 6956 (47.4) | 2926 (47.3) | 0.94 |
| Income quartile | <0.01 | |||
| 0–25th percentile | 7271 (34.8) | 5293 (36.0) | 1978 (32.0) | |
| 26th–50th percentile (median) | 5955 (28.5) | 4090 (27.8) | 1865 (30.1) | |
| 51st–75th percentile | 4678 (22.4) | 3267 (22.24) | 1411 (22.8) | |
| 76th–100th percentile | 2976 (14.3) | 2042 (13.9) | 934 (15.1) | |
| Patient location | <0.01 | |||
| Large central metro | 5548 (26.6) | 3905 (26.6) | 1643 (26.7) | |
| Large fringe metro | 4519 (21.6) | 3081 (21.0) | 1438 (23.2) | |
| Medium metro | 4373 (20.9) | 2964 (20.2) | 1409 (22.8) | |
| Small metro | 2405 (11.5) | 1768 (12.0) | 637 (10.3) | |
| Micropolitan | 2276 (10.9) | 1651 (11.2) | 625 (10.1) | |
| Non-metro or micropolitan | 1759 (8.4) | 1323 (9.0) | 436 (7.1) | |
| In-state resident | 19,883 (95.2) | 14,058 (95.7) | 5825 (94.1) | <0.01 |
| Emergency department | 15,559 (74.5) | 10,916 (74.3) | 4644 (75.1) | 0.25 |
| Admitted on weekend | 5209 (25.0) | 3650 (24.8) | 1559 (25.2) | 0.59 |
| Season | 0.19 | |||
| Winter | 6292 (30.1) | 4437 (30.2) | 1855 (30.0) | |
| Spring | 6238 (29.9) | 4337 (29.5) | 1901 (30.7) | |
| Summer | 3084 (14.8) | 2161 (14.7) | 923 (14.9) | |
| Fall | 5266 (25.2) | 3757 (25.6) | 1509 (24.4) | |
| Expected primary payer | <0.01 | |||
| Medicare | 125 (0.6) | 82 (0.6) | 43 (0.7) | |
| Medicaid | 12,567 (60.2) | 8728 (59.4) | 3839 (62.0) | |
| Private insurance | 7193 (34.5) | 5141 (35.0) | 2052 (33.2) | |
| Self-pay | 440 (2.1) | 336 (2.3) | 104 (1.7) | |
| No charge | 555 (2.7) | 405 (2.8) | 150 (2.4) | |
| Patient Clinical Characteristics | ||||
| Respiratory conditions | ||||
| Asthma | 7244 (34.7) | 5001 (34.0) | 2243 (36.3) | <0.01 |
| Acute bronchitis/bronchiolitis | 2805 (13.4) | 1579 (10.8) | 1226 (19.8) | <0.01 |
| Chronic pulmonary disease | 7399 (35.4) | 5111 (34.8) | 2288 (37.0) | <0.01 |
| Immunosuppressive conditions | ||||
| Cancer, any type | 187 (0.9) | 134 (0.9) | 53 (0.9) | 0.70 |
| Cystic fibrosis | 466 (2.2) | 434 (3.0) | 32 (0.5) | <0.01 |
| Sickle cell disease | 280 (1.3) | 257 (1.8) | 23 (0.4) | <0.01 |
| HCUP severity class | <0.01 | |||
| Minor | 6199 (29.7) | 5556 (37.8) | 643 (10.4) | |
| Moderate | 8199 (39.3) | 6754 (46.0) | 1445 (23.4) | |
| Major | 4177 (20.0) | 1860 (12.7) | 2317 (37.4) | |
| Extreme | 2305 (11.0) | 522 (3.6) | 1783 (28.8) | |
| Hospital Characteristics | ||||
| Hospital size | <0.01 | |||
| Small | 3142 (15.1) | 2318 (15.8) | 824 (13.3) | |
| Medium | 4406 (21.1) | 3413 (23.2) | 993 (16.1) | |
| Large | 13,332 (63.9) | 8961 (61.0) | 4371 (70.6) | |
| Hospital urban-rural designation | <0.01 | |||
| Large metropolitan | 11,234 (53.8) | 7636 (52.0) | 3598 (58.1) | |
| Small metropolitan | 7352 (35.2) | 5153 (35.1) | 2199 (35.5) | |
| Micropolitan | 1609 (7.7) | 1293 (8.8) | 316 (5.1) | |
| Non-urban | 685 (3.3) | 610 (4.2) | 75 (1.2) | |
| Hospital teaching status | <0.01 | |||
| Metro non-teaching | 1790 (8.6) | 1465 (10.0) | 325 (5.3) | |
| Metro teaching | 16,796 (80.4) | 11,324 (77.0) | 5472 (88.4) | |
| Non-metro hospital | 22.94 (11.0) | 1903 (13.0) | 391 (6.3) | |
| Hospital case volume | <0.01 | |||
| 0–25th percentile | 5347 (25.6) | 4341 (29.5) | 1006 (16.3) | |
| 26th–50th percentile (median) | 5154 (24.7) | 3750 (25.5) | 1404 (22.7) | |
| 51st–75th percentile | 5165 (24.7) | 3567 (24.3) | 1598 (25.8) | |
| 76th–100th percentile | 5214 (25.0) | 3034 (20.7) | 2180 (35.2) | |
| Outcome | Total Sample N = 20,880 (100%) | Non-Severe Pneumonia N = 14,692 (70.4%) | Severe Pneumonia N = 6188 (29.6%) | p-Value |
|---|---|---|---|---|
| 30-day readmission, all-cause | 1225 (5.9) | 687 (4.7) | 538 (8.7) | <0.01 |
| 30-day readmission, pneumonia-specific | 348 (1.7) | 210 (1.4) | 138 (2.2) | <0.01 |
| Index hospitalization | ||||
| Length of stay (days), mean ± SD | 3.8 (4.1) | 3.0 (2.9) | 5.7 (5.7) | <0.01 |
| Daily cost (USD), mean ± SD | 2341 (1823) | 2120 (1363) | 2865 (2533) | <0.01 |
| Sum of total costs (USD) | 205,400,992 | 93,869,832 | 111,531,160 | <0.01 |
| 30-day readmission | ||||
| Length of stay (days), mean ± SD | 5.9 (5.9) | 5.4 (5.5) | 6.5 (6.4) | <0.01 |
| Daily cost (USD), mean ± SD | 2928 (1963) | 2679 (1978) | 3246 (1898) | <0.01 |
| Sum of total costs (USD) | 22,036,400 | 10,340,098 | 11,696,302 | <0.01 |
| Principal Diagnosis | N (%) |
|---|---|
| Pneumonia (except that caused by tuberculosis) | 291 (23.8) |
| Respiratory failure, insufficiency, or arrest | 144 (11.8) |
| Acute bronchitis | 94 (7.7) |
| Asthma | 83 (6.8) |
| Influenza | 48 (3.9) |
| Epilepsy or convulsions | 44 (3.6) |
| Septicemia | 43 (3.5) |
| Other specified upper respiratory infections | 36 (2.9) |
| Aspiration pneumonitis | 33 (2.7) |
| Respiratory signs and symptoms (e.g., epistaxis, hemorrhage, cough, dyspnea, shortness of breath, etc.) | 30 (2.5) |
| Covariate | Adjusted Odds Ratio (95% CI) |
|---|---|
| Severe pneumonia | 1.44 (1.26, 1.65) * |
| Age group | |
| <1 year | Reference |
| 1–4 years | 0.81 (0.67, 0.98) * |
| 5–12 years | 0.88 (0.72, 1.08) |
| 13–17 years | 1.25 (0.99, 1.58) |
| Female | 0.99 (0.88, 1.12) |
| Expected primary payer | |
| Private insurance | Reference |
| Medicare | 2.17 (1.20, 3.95) * |
| Medicaid | 1.20 (1.05, 1.37) * |
| Self-pay | 0.44 (0.22, 0.86) * |
| No charge | 1.40 (0.98, 1.98) |
| Length of stay | 1.04 (1.03, 1.06) * |
| Daily cost | |
| 0–25th percentile | Reference |
| 26th–50th percentile (median) | 1.15 (0.95, 1.38) |
| 51st–75th percentile | 1.29 (1.07, 1.55) * |
| 76th–100th percentile | 1.40 (1.16, 1.69) * |
| Asthma | 0.78 (0.68, 0.90) * |
| Cancer, any type | 4.82 (3.43, 6.77) * |
| Cystic fibrosis | 0.89 (0.62, 1.27) |
| Sickle cell disease | 2.14 (1.45, 3.16) * |
| Hospital size | |
| Small | Reference |
| Medium | 1.00 (0.81, 1.24) |
| Large | 1.13 (0.95, 1.35) |
| Hospital teaching status | |
| Non-metropolitan hospital | Reference |
| Metropolitan non-teaching | 0.84 (0.57, 1.23) |
| Metropolitan teaching | 1.48 (1.12, 1.97) * |
| Hospital case volume | |
| 0–25th percentile | Reference |
| 26th–50th percentile (median) | 1.33 (1.08, 1.64) * |
| 51st–75th percentile | 1.40 (1.13, 1.74) * |
| 76th–100th percentile | 1.50 (1.22, 1.86) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lewis, M.O.; Tran, P.T.; Huang, Y.; Desai, R.A.; Shen, Y.; Brown, J.D. Disease Severity and Risk Factors of 30-Day Hospital Readmission in Pediatric Hospitalizations for Pneumonia. J. Clin. Med. 2022, 11, 1185. https://doi.org/10.3390/jcm11051185
Lewis MO, Tran PT, Huang Y, Desai RA, Shen Y, Brown JD. Disease Severity and Risk Factors of 30-Day Hospital Readmission in Pediatric Hospitalizations for Pneumonia. Journal of Clinical Medicine. 2022; 11(5):1185. https://doi.org/10.3390/jcm11051185
Chicago/Turabian StyleLewis, Motomori O., Phuong T. Tran, Yushi Huang, Raj A. Desai, Yun Shen, and Joshua D. Brown. 2022. "Disease Severity and Risk Factors of 30-Day Hospital Readmission in Pediatric Hospitalizations for Pneumonia" Journal of Clinical Medicine 11, no. 5: 1185. https://doi.org/10.3390/jcm11051185
APA StyleLewis, M. O., Tran, P. T., Huang, Y., Desai, R. A., Shen, Y., & Brown, J. D. (2022). Disease Severity and Risk Factors of 30-Day Hospital Readmission in Pediatric Hospitalizations for Pneumonia. Journal of Clinical Medicine, 11(5), 1185. https://doi.org/10.3390/jcm11051185