
Nonalcoholic Fatty Liver Disease Is a Precursor of New-Onset Metabolic Syndrome in Metabolically Healthy Young Adults

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
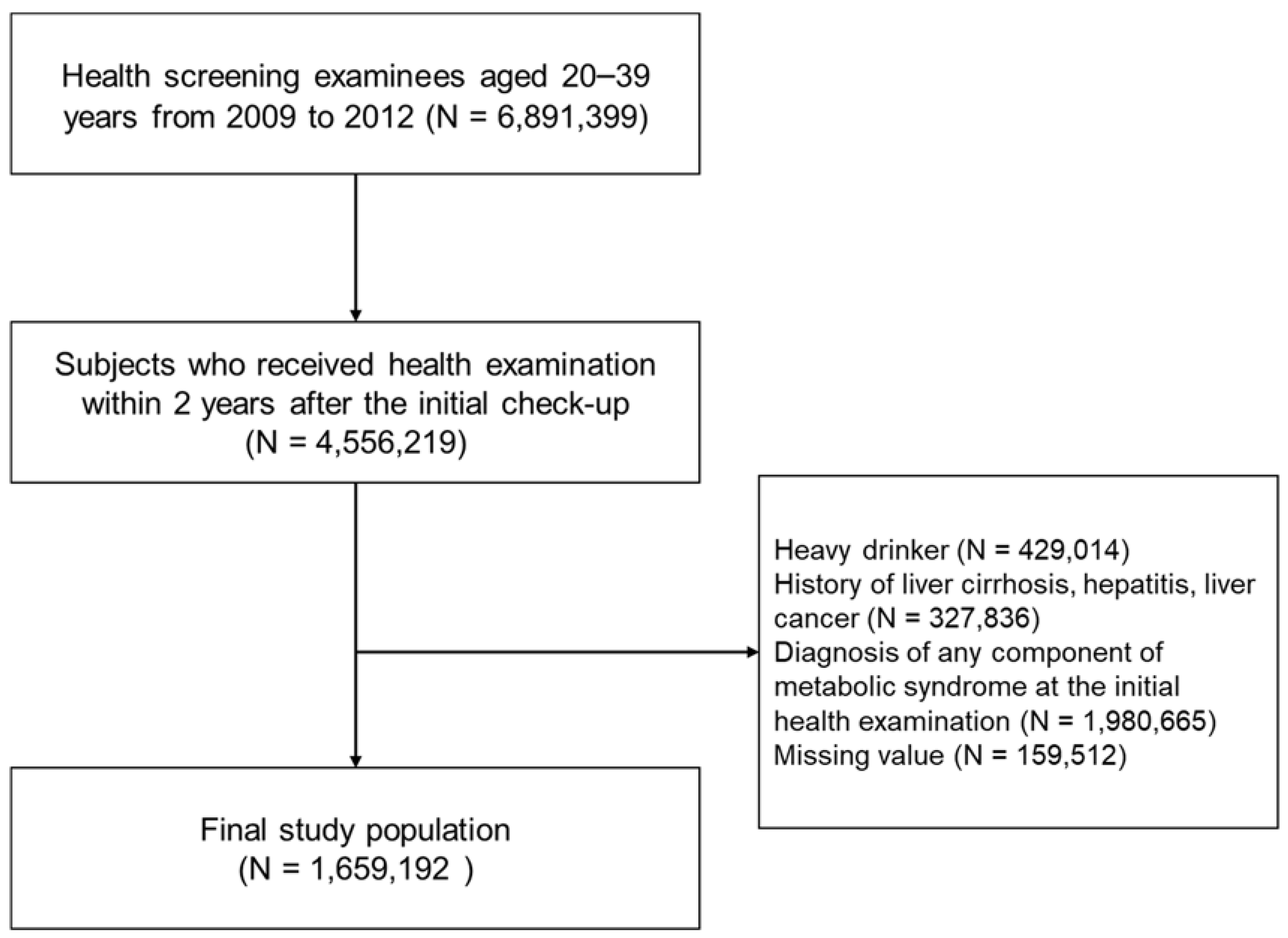
2.2. Study Population
2.3. Data Collection
2.4. Definition of NAFLD
× ln (triglyceride) + 0.139 × BMI + 0.718 × ln (gamma-glutamyl transferase) + 0.053 × WC − 15.745) × 100
2.5. Study Outcome
2.6. Statistical Analyses
3. Results
3.1. Baseline Characteristics of the Study Population
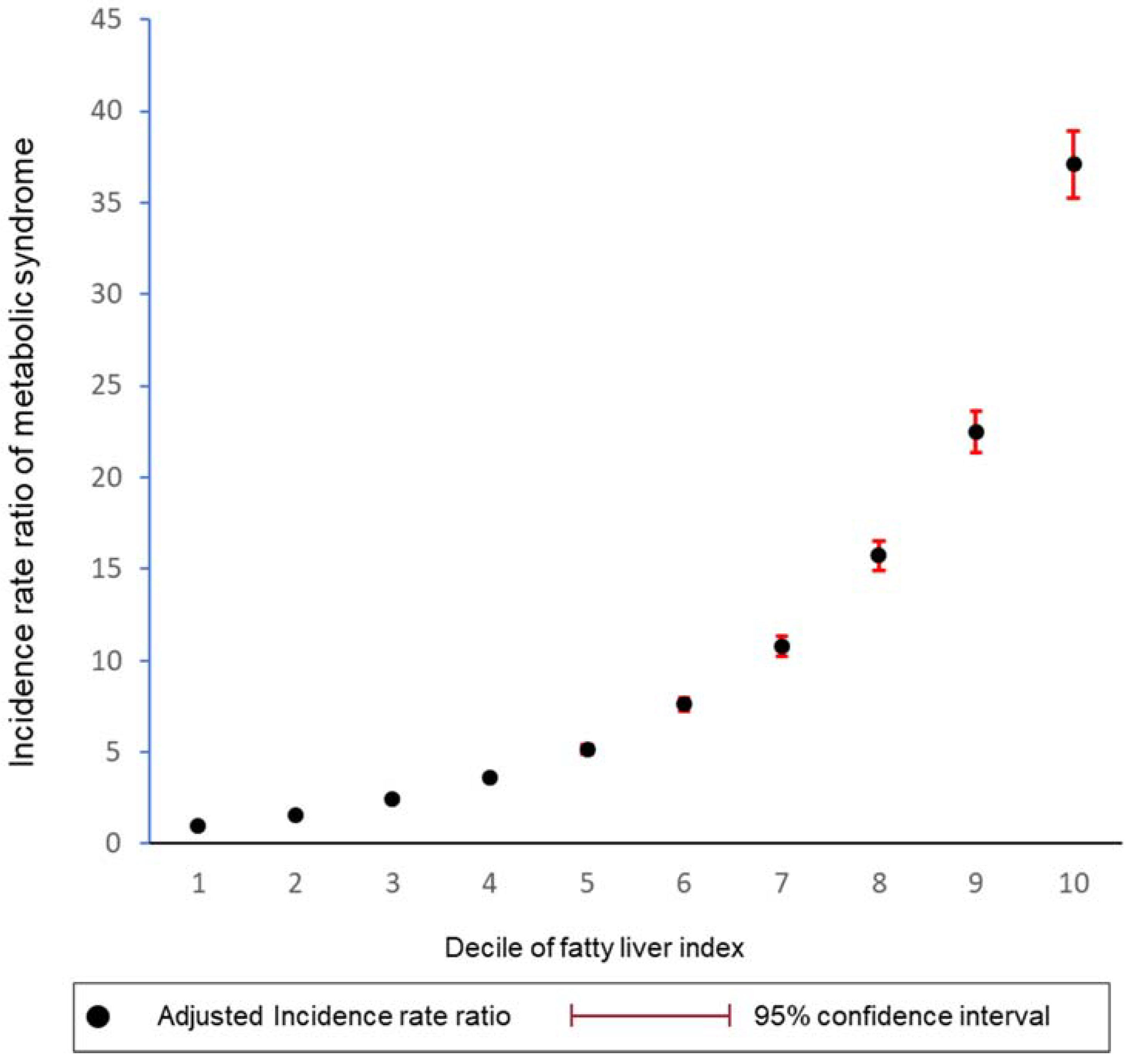
3.2. Incidence of Metabolic Syndrome and Its Component According to the Degree of Hepatic Steatosis
3.3. Stratified Analysis According to Various Subgroups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chan, T.T.; Tse, Y.K.; Lui, R.N.; Wong, G.L.; Chim, A.M.; Kong, A.P.; Woo, J.; Yeung, D.K.; Abrigo, J.M.; Chu, W.C.; et al. Fatty Pancreas Is Independently Associated with Subsequent Diabetes Mellitus Development: A 10-Year Prospective Cohort Study. Clin. Gastroenterol Hepatol. 2021; in press. [Google Scholar] [CrossRef]
- Godoy-Matos, A.F.; Silva Junior, W.S.; Valerio, C.M. NAFLD as a continuum: From obesity to metabolic syndrome and diabetes. Diabetol. Metab. Syndr. 2020, 12, 60. [Google Scholar] [CrossRef] [PubMed]
- Milovanovic, T.; Pantic, I.; Dragasevic, S.; Lugonja, S.; Dumic, I.; Rajilic-Stojanovic, M. The Interrelationship Among Non-Alcoholic Fatty Liver Disease, Colonic Diverticulosis and Metabolic Syndrome. J. Gastrointestin. Liver Dis. 2021, 30, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Gastaldelli, A. Fatty liver disease: The hepatic manifestation of metabolic syndrome. Hypertens. Res. Off. J. Jpn. Soc. Hypertens. 2010, 33, 546–547. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Haring, H.U. The metabolically benign and malignant fatty liver. Diabetes 2011, 60, 2011–2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balkau, B.; Lange, C.; Vol, S.; Fumeron, F.; Bonnet, F.; Study Group D.E.S.I.R. Nine-year incident diabetes is predicted by fatty liver indices: The French D.E.S.I.R. study. BMC Gastroenterol. 2010, 10, 56. [Google Scholar] [CrossRef]
- Chang, Y.; Jung, H.S.; Yun, K.E.; Cho, J.; Cho, Y.K.; Ryu, S. Cohort study of non-alcoholic fatty liver disease, NAFLD fibrosis score, and the risk of incident diabetes in a Korean population. Am. J. Gastroenterol. 2013, 108, 1861–1868. [Google Scholar] [CrossRef]
- Kasturiratne, A.; Weerasinghe, S.; Dassanayake, A.S.; Rajindrajith, S.; de Silva, A.P.; Kato, N.; Wickremasinghe, A.R.; de Silva, H.J. Influence of non-alcoholic fatty liver disease on the development of diabetes mellitus. J. Gastroenterol. Hepatol. 2013, 28, 142–147. [Google Scholar] [CrossRef]
- Lonardo, A.; Ballestri, S.; Marchesini, G.; Angulo, P.; Loria, P. Nonalcoholic fatty liver disease: A precursor of the metabolic syndrome. Dig. Liver Dis. 2015, 47, 181–190. [Google Scholar] [CrossRef] [Green Version]
- Friis-Liby, I.; Aldenborg, F.; Jerlstad, P.; Rundstrom, K.; Bjornsson, E. High prevalence of metabolic complications in patients with non-alcoholic fatty liver disease. Scand. J. Gastroenterol. 2004, 39, 864–869. [Google Scholar] [CrossRef]
- Hanley, A.J.; Williams, K.; Festa, A.; Wagenknecht, L.E.; D’Agostino, R.B., Jr.; Haffner, S.M. Liver markers and development of the metabolic syndrome: The insulin resistance atherosclerosis study. Diabetes 2005, 54, 3140–3147. [Google Scholar] [CrossRef] [Green Version]
- Ryoo, J.H.; Choi, J.M.; Moon, S.Y.; Suh, Y.J.; Shin, J.Y.; Shin, H.C.; Park, S.K. The clinical availability of non alcoholic fatty liver disease as an early predictor of the metabolic syndrome in Korean men: 5-year’s prospective cohort study. Atherosclerosis 2013, 227, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Paschos, P.; Paletas, K. Non alcoholic fatty liver disease and metabolic syndrome. Hippokratia 2009, 13, 9–19. [Google Scholar]
- Diehl, A.M. Fatty liver, hypertension, and the metabolic syndrome. Gut 2004, 53, 923–924. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.G.; Roelstraete, B.; Khalili, H.; Hagstrom, H.; Ludvigsson, J.F. Mortality in biopsy-confirmed nonalcoholic fatty liver disease: Results from a nationwide cohort. Gut 2020, 70, 1375–1382. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort Profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- Cho, E.J.; Han, K.; Lee, S.P.; Shin, D.W.; Yu, S.J. Liver enzyme variability and risk of heart disease and mortality: A nationwide population-based study. Liver Int. 2020, 40, 1292–1302. [Google Scholar] [CrossRef]
- Cho, Y.; Cho, E.J.; Yoo, J.J.; Chang, Y.; Chung, G.E.; Jeong, S.M.; Park, S.H.; Han, K.; Shin, D.W.; Yu, S.J. Association between Lipid Profiles and the Incidence of Hepatocellular Carcinoma: A Nationwide Population-Based Study. Cancers 2021, 13, 1599. [Google Scholar] [CrossRef]
- Yoo, J.J.; Cho, E.J.; Han, K.; Heo, S.S.; Kim, B.Y.; Shin, D.W.; Yu, S.J. Glucose variability and risk of hepatocellular carcinoma in diabetic patients: A nationwide population-based study. Cancer Epidemiol. Biomark. Prev. 2021, 30, 974–981. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. Diabetologia 2016, 59, 1121–1140. [Google Scholar] [CrossRef] [Green Version]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Koehler, E.M.; Schouten, J.N.; Hansen, B.E.; Hofman, A.; Stricker, B.H.; Janssen, H.L. External validation of the fatty liver index for identifying nonalcoholic fatty liver disease in a population-based study. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2013, 11, 1201–1204. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Park, S.K.; Ryoo, J.H.; Kim, M.G.; Shin, J.Y. Association of serum ferritin and the development of metabolic syndrome in middle-aged Korean men: A 5-year follow-up study. Diabetes Care 2012, 35, 2521–2526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hui, A.Y.; Wong, V.W.; Chan, H.L.; Liew, C.T.; Chan, J.L.; Chan, F.K.; Sung, J.J. Histological progression of non-alcoholic fatty liver disease in Chinese patients. Aliment. Pharm. 2005, 21, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R.; Fisch, G.; Teague, B.; Tamborlane, W.V.; Banyas, B.; Allen, K.; Savoye, M.; Rieger, V.; Taksali, S.; Barbetta, G.; et al. Prevalence of impaired glucose tolerance among children and adolescents with marked obesity. N. Engl. J. Med. 2002, 346, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.; Bremer, A.A.; Lustig, R.H. What is metabolic syndrome, and why are children getting it? Ann. N. Y. Acad. Sci. 2013, 1281, 123–140. [Google Scholar] [CrossRef] [Green Version]
- Lara-Castro, C.; Garvey, W.T. Intracellular lipid accumulation in liver and muscle and the insulin resistance syndrome. Endocrinol. Metab. Clin. N. Am. 2008, 37, 841–856. [Google Scholar] [CrossRef] [Green Version]
- Chait, A.; den Hartigh, L.J. Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease. Front. Cardiovasc. Med. 2020, 7, 22. [Google Scholar] [CrossRef] [Green Version]
- Tangvarasittichai, S. Oxidative stress, insulin resistance, dyslipidemia and type 2 diabetes mellitus. World J. Diabetes 2015, 6, 456–480. [Google Scholar] [CrossRef]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuniga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef]
- Jornayvaz, F.R.; Samuel, V.T.; Shulman, G.I. The role of muscle insulin resistance in the pathogenesis of atherogenic dyslipidemia and nonalcoholic fatty liver disease associated with the metabolic syndrome. Annu. Rev. Nutr. 2010, 30, 273–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albhaisi, S.; Chowdhury, A.; Sanyal, A.J. Non-alcoholic fatty liver disease in lean individuals. JHEP Rep. Innov. Hepatol. 2019, 1, 329–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, Q.; Liu, W.; Baker, S.S.; Li, H.; Chen, C.; Liu, Q.; Tang, S.; Guan, L.; Tsompana, M.; Kozielski, R.; et al. Multi-targeting therapeutic mechanisms of the Chinese herbal medicine QHD in the treatment of non-alcoholic fatty liver disease. Oncotarget 2017, 8, 27820–27838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, V.W.S.; Wong, G.L.H.; Woo, J.; Abrigo, J.M.; Chan, C.K.M.; Shu, S.S.T.; Leung, J.K.Y.; Chim, A.M.L.; Kong, A.P.S.; Lui, G.C.Y. Impact of the New Definition of Metabolic Associated Fatty Liver Disease on the Epidemiology of the Disease. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2020, 19, 2161–2171. [Google Scholar] [CrossRef]
- Kang, S.H.; Cho, Y.; Jeong, S.W.; Kim, S.U.; Lee, J.W.; Korean, N.S.G. From nonalcoholic fatty liver disease to metabolic-associated fatty liver disease: Big wave or ripple? Clin. Mol. Hepatol. 2021, 27, 257–269. [Google Scholar] [CrossRef]
- Boland, B.B.; Rhodes, C.J.; Grimsby, J.S. The dynamic plasticity of insulin production in beta-cells. Mol. Metab. 2017, 6, 958–973. [Google Scholar] [CrossRef]
- Kurtoglu, S.; Akin, L.; Kendirci, M.; Hatipoglu, N.; Elmali, F.; Mazicioglu, M. The absence of insulin resistance in metabolic syndrome definition leads to underdiagnosing of metabolic risk in obese patients. Eur. J. Pediatr. 2012, 171, 1331–1337. [Google Scholar] [CrossRef]
- Boisvenue, J.J.; Oliva, C.U.; Manca, D.P.; Johnson, J.A.; Yeung, R.O. Feasibility of identifying and describing the burden of early-onset metabolic syndrome in primary care electronic medical record data: A cross-sectional analysis. CMAJ Open 2020, 8, E779–E787. [Google Scholar] [CrossRef]
- Sekgala, M.D.; Monyeki, K.D.; Mogale, A.; McHiza, Z.J.; Parker, W.; Choma, S.R.; Makgopa, H.M. The risk of metabolic syndrome as a result of lifestyle among Ellisras rural young adults. J. Hum. Hypertens. 2018, 32, 572–584. [Google Scholar] [CrossRef] [Green Version]
- Feng, R.N.; Du, S.S.; Wang, C.; Li, Y.C.; Liu, L.Y.; Guo, F.C.; Sun, C.H. Lean-non-alcoholic fatty liver disease increases risk for metabolic disorders in a normal weight Chinese population. World J. Gastroenterol. 2014, 20, 17932–17940. [Google Scholar] [CrossRef]
- Yang, B.L.; Wu, W.C.; Fang, K.C.; Wang, Y.C.; Huo, T.I.; Huang, Y.H.; Yang, H.I.; Su, C.W.; Lin, H.C.; Lee, F.Y.; et al. External validation of fatty liver index for identifying ultrasonographic fatty liver in a large-scale cross-sectional study in Taiwan. PLoS ONE 2015, 10, e0120443. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | FLI < 30 | 30 ≤ FLI < 60 | FLI ≥ 60 | p-Value |
|---|---|---|---|---|
| (n = 1,585,018) | (n = 71,642) | (n = 2532) | ||
| Age, years | 29.2 ± 4.6 | 31.4 ± 4.0 | 31.8 ± 3.8 | <0.001 |
| 20–29 y | 880,059 (55.5) | 24,361 (34.0) | 769 (30.4) | <0.001 |
| 30–39 y | 704,959 (44.5) | 47,281 (66.0) | 1763 (69.6) | |
| Male | 686,261 (43.3) | 68,680 (95.9) | 2452 (96.8) | <0.001 |
| Body mass index, kg/m2 | 21.1 ± 2.4 | 25.6 ± 1.9 | 27.8 ± 7.2 | <0.001 |
| <18.5 | 208,844 (13.2) | 5 (0.01) | 0 (0) | |
| 18.5–23 | 1,033,206 (65.2) | 4672 (6.5) | 29 (1.2) | |
| 23–25 | 247,216 (15.6) | 21,440 (29.9) | 222 (8.8) | |
| 25–30 | 94,898 (6.0) | 44,233 (61.7) | 1974 (78.0) | |
| ≥30 | 854 (0.05) | 1292 (1.8) | 307 (12.1) | |
| Low-income status | 234,208 (14.8) | 6607 (9.2) | 242 (9.6) | <0.001 |
| Dyslipidemia | 34,692 (2.19) | 5821 (8.1) | 338 (13.4) | <0.001 |
| Smoking | <0.001 | |||
| Non-smoker | 1,103,436 (69.6) | 23,765 (33.2) | 749 (29.6) | |
| Ex-smoker | 120,225 (7.6) | 10,752 (15.0) | 374 (14.8) | |
| Current smoker | 361,357 (22.8) | 37,125 (51.8) | 1409 (55.7) | |
| Alcohol consumption | <0.001 | |||
| None | 705,868 (44.5) | 17,595 (24.6) | 520 (20.5) | |
| Mild-to-moderate * | 879,150 (55.5) | 54,047 (75.4) | 2012 (79.5) | |
| Regular exercise | 188,503 (11.9) | 10,212 (14.3) | 352 (13.9) | <0.001 |
| Waist circumference, cm | 71.9 ± 7.1 | 84.5 ± 3.4 | 86.3 ± 3.0 | <0.001 |
| Systolic blood pressure, mm Hg | 110.9 ± 9.1 | 116.1 ± 7.3 | 116.7 ± 6.9 | <0.001 |
| Diastolic blood pressure, mm Hg | 69.6 ± 7.21 | 73.2 ± 6.3 | 74.1 ± 6.1 | <0.001 |
| Fasting glucose, mg/dL | 85.5 ± 7.8 | 87.4 ± 7.6 | 87.9 ± 7.9 | <0.001 |
| Total cholesterol, mg/dL | 176.3 ± 28.6 | 196.0 ± 34.6 | 206.1 ± 31.4 | <0.001 |
| HDL cholesterol, mg/dL | 62.6 ± 19.7 | 54.6 ± 32.0 | 55.4 ± 18.5 | <0.001 |
| LDL cholesterol, mg/dL | 116.2 ± 348.8 | 124.2 ± 163.5 | 128.3 ± 67.1 | <0.001 |
| Triglyceride, mg/dL | 68.4 (68.4–68.5) | 112.8 (112.6–113.0) | 124.3 (123.5–125.1) | <0.001 |
| Fatty liver index | 7.1 ± 6.5 | 38.9 ± 7.2 | 65.8 ± 5.3 | <0.001 |
| Number | Duration (Person-Year) | Events | Incidence Rate (Per 1000 p-y) | Model 1 * | Model 2 † | Model 3 § | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| IRR (95% CI) | p | IRR (95% CI) | p | IRR (95% CI) | p | |||||
| Total | ||||||||||
| FLI < 30 | 1,585,018 | 6,450,322 | 86,006 | 13.33 | 1 (ref) | <0.001 | 1 (ref) | <0.001 | 1 (ref) | <0.001 |
| 30–60 | 71,642 | 242,083 | 22,116 | 91.36 | 6.9 (6.8–7.0) | 4.1 (4.1–4.2) | 2.1 (2.1–2.2) | |||
| ≥60 | 2532 | 7056 | 1117 | 158.30 | 11.9 (11.2–12.6) | 7.1 (6.7–7.6) | 2.9 (2.8–3.1) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, J.-J.; Cho, E.J.; Chung, G.E.; Chang, Y.; Cho, Y.; Park, S.-H.; Jeong, S.-M.; Kim, B.-Y.; Shin, D.W.; Kim, Y.J.; et al. Nonalcoholic Fatty Liver Disease Is a Precursor of New-Onset Metabolic Syndrome in Metabolically Healthy Young Adults. J. Clin. Med. 2022, 11, 935. https://doi.org/10.3390/jcm11040935
Yoo J-J, Cho EJ, Chung GE, Chang Y, Cho Y, Park S-H, Jeong S-M, Kim B-Y, Shin DW, Kim YJ, et al. Nonalcoholic Fatty Liver Disease Is a Precursor of New-Onset Metabolic Syndrome in Metabolically Healthy Young Adults. Journal of Clinical Medicine. 2022; 11(4):935. https://doi.org/10.3390/jcm11040935
Chicago/Turabian StyleYoo, Jeong-Ju, Eun Ju Cho, Goh Eun Chung, Young Chang, Yuri Cho, Sang-Hyun Park, Su-Min Jeong, Bo-Yeon Kim, Dong Wook Shin, Yun Joon Kim, and et al. 2022. "Nonalcoholic Fatty Liver Disease Is a Precursor of New-Onset Metabolic Syndrome in Metabolically Healthy Young Adults" Journal of Clinical Medicine 11, no. 4: 935. https://doi.org/10.3390/jcm11040935
APA StyleYoo, J.-J., Cho, E. J., Chung, G. E., Chang, Y., Cho, Y., Park, S.-H., Jeong, S.-M., Kim, B.-Y., Shin, D. W., Kim, Y. J., Yoon, J.-H., Han, K., & Yu, S. J. (2022). Nonalcoholic Fatty Liver Disease Is a Precursor of New-Onset Metabolic Syndrome in Metabolically Healthy Young Adults. Journal of Clinical Medicine, 11(4), 935. https://doi.org/10.3390/jcm11040935