
Against All Odds? Addiction History Associated with Better Viral Hepatitis Care: A Dutch Nationwide Claims Data Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Outcomes and Clustering Healthcare Activities
2.4. Statistical Analyses
3. Results
3.1. Study Population
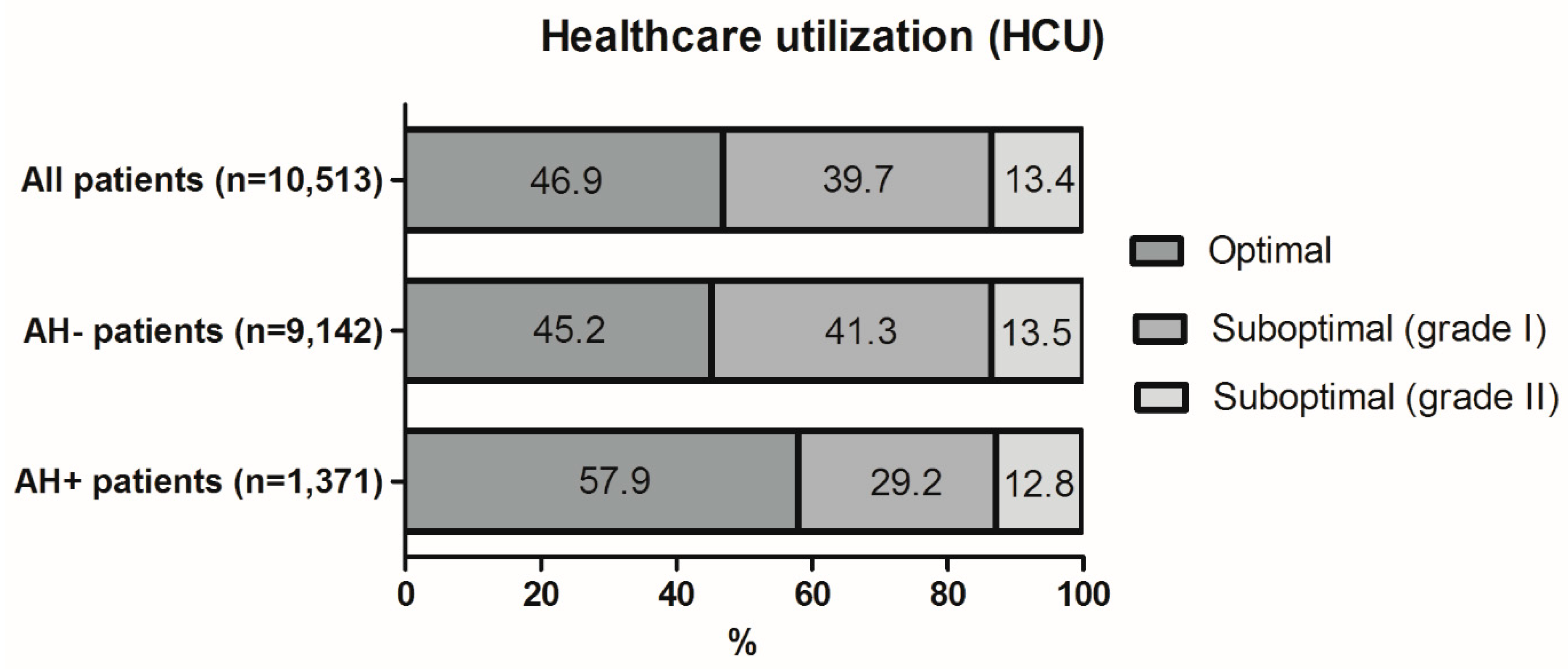
3.2. Healthcare Utilization (HCU)
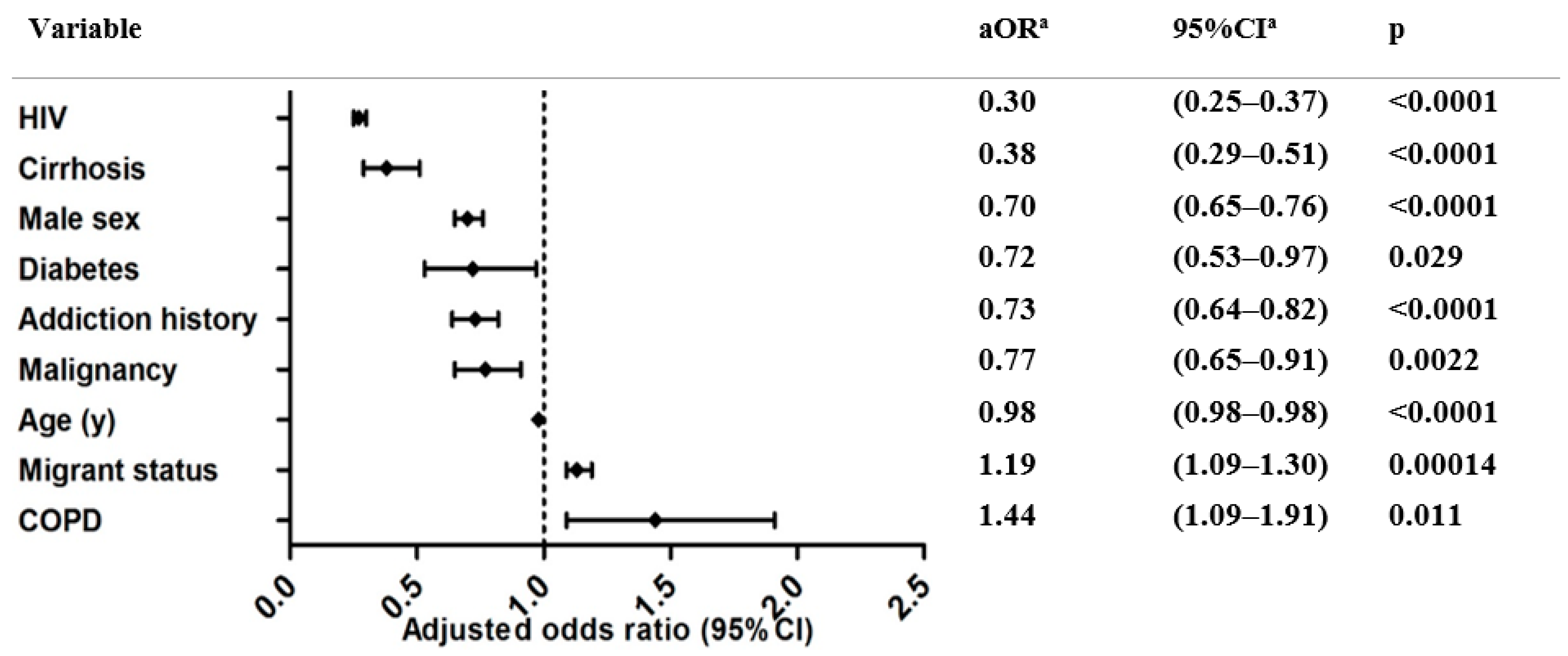
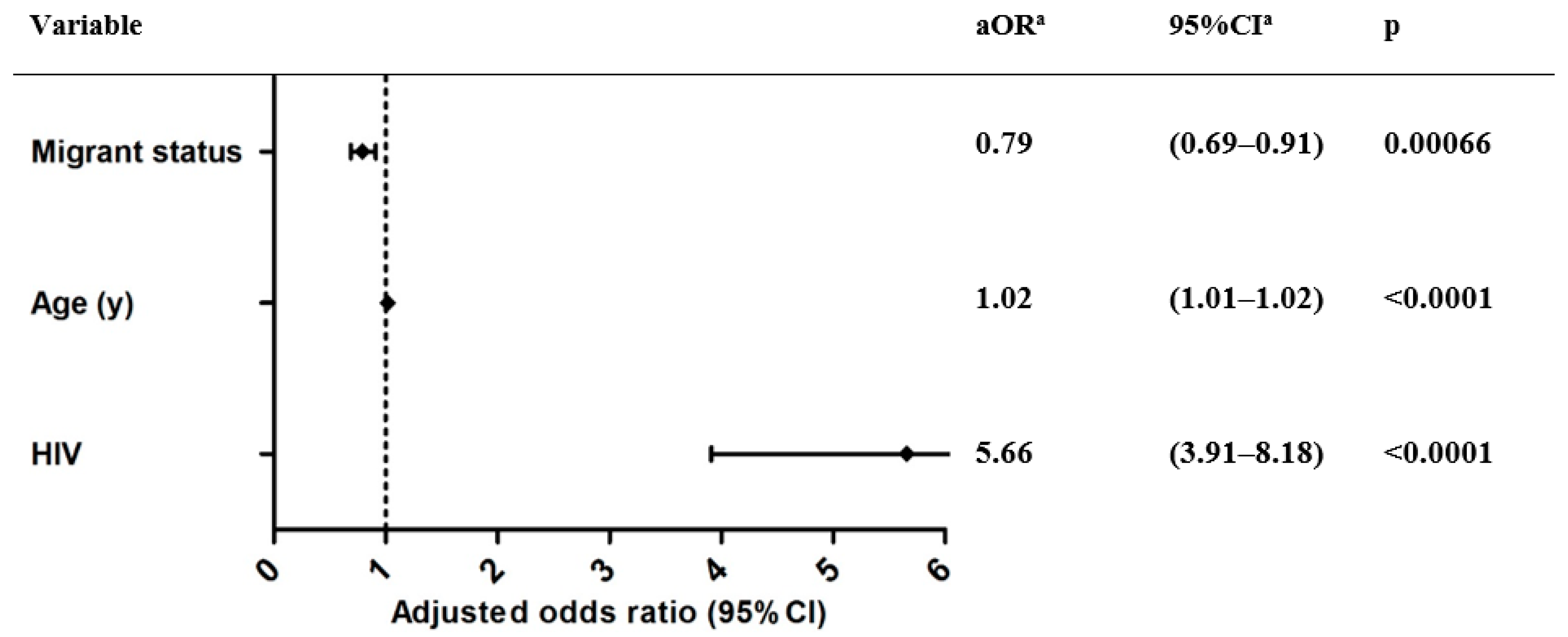
3.3. Exploratory Model
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Association for the Study of the Liver. EASL Recommendations on Treatment of Hepatitis C 2018. J. Hepatol. 2018, 69, 461–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razavi, H. Global Epidemiology of Viral Hepatitis. Gastroenterol. Clin. N. Am. 2020, 49, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Koopsen, J.; van Steenbergen, J.E.; Richardus, J.H.; Prins, M.; Op de Coul, E.L.M.; Heil, J.; Zuure, F.R.; Veldhuijzen, I.K. Chronic hepatitis B and C infections in the Netherlands: Estimated prevalence in risk groups and the general population. Epidemiol. Infect. 2019, 147, e147. [Google Scholar] [CrossRef] [Green Version]
- WHO. Combating Hepatitis B and C to Reach Elimination by 2030; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- van Dijk, M.; Brakenhoff, S.M.; Isfordink, C.J.; Cheng, W.-H.; Blokzijl, H.; Boland, G.; Dofferhoff, A.S.M.; van Hoek, B.; Nieuwkoop, C.; Sonneveld, M.J.; et al. The Netherlands Is on Track to Meet the World Health Organization Hepatitis C Elimination Targets by 2030. J. Clin. Med. 2021, 10, 4562. [Google Scholar] [CrossRef]
- Kracht, P.A.M.; Arends, J.E.; van Erpecum, K.J.; Urbanus, A.; Willemse, J.A.; Hoepelman, A.I.M. Strategies for achieving viral hepatitis C micro-elimination in the Netherlands. Hepatol. Med. Policy 2018, 3, 12. [Google Scholar] [CrossRef]
- Nitulescu, R.; Young, J.; Saeed, S.; Cooper, C.; Cox, J.; Martel-Laferriere, V.; Hull, M.; Walmsley, S.; Tyndall, M.; Wong, A.; et al. Variation in hepatitis C virus treatment uptake between Canadian centres in the era of direct-acting antivirals. Int. J. Drug Policy 2019, 65, 41–49. [Google Scholar] [CrossRef]
- Solund, C.; Hallager, S.; Pedersen, M.S.; Fahnoe, U.; Ernst, A.; Krarup, H.B.; Roger, B.T.; Christensen, P.B.; Laursen, A.L.; Gerstoft, J.; et al. Direct acting antiviral treatment of chronic hepatitis C in Denmark: Factors associated with and barriers to treatment initiation. Scand. J. Gastroenterol. 2018, 53, 849–856. [Google Scholar] [CrossRef]
- van Dijk, M.; Drenth, J.P.H.; HepNed Study Group. Loss to follow-up in the hepatitis C care cascade: A substantial problem but opportunity for micro-elimination. J. Viral Hepat. 2020, 27, 1270–1283. [Google Scholar] [CrossRef]
- Hajarizadeh, B.; Cunningham, E.B.; Reid, H.; Law, M.; Dore, G.J.; Grebely, J. Direct-acting antiviral treatment for hepatitis C among people who use or inject drugs: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2018, 3, 754–767. [Google Scholar] [CrossRef]
- Shiha, G.; Soliman, R.; Serwah, A.; Mikhail, N.N.H.; Asselah, T. A same day ‘test and treat’ model for chronic HCV and HBV infection: Results from two community-based pilot studies in Egypt. J. Viral Hepat. 2020, 27, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.H.; Wong, G.; Gane, E.; Kao, J.-H.; Dusheiko, G. Hepatitis B Virus: Advances in Prevention, Diagnosis, and Therapy. Clin. Microbiol. Rev. 2020, 33, e00046-19. [Google Scholar] [CrossRef] [PubMed]
- Allain, J.P.; Opare-Sem, O. Screening and diagnosis of HBV in low-income and middle-income countries. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 643–653. [Google Scholar] [CrossRef] [PubMed]
- Locarnini, S.; Hatzakis, A.; Chen, D.-S.; Lok, A. Strategies to control hepatitis B: Public policy, epidemiology, vaccine and drugs. J. Hepatol. 2015, 62 (Suppl. S1), S76–S86. [Google Scholar] [CrossRef]
- Falade-Nwulia, O.; Ward, K.M.; McCormick, S.; Mehta, S.H.; Pitts, S.R.; Katzs, S.; Chander, G.; Thomas, D.L.; Sulkowski, M.; Latkin, C.A. Network-based recruitment of people who inject drugs for hepatitis C testing and linkage to care. J. Viral Hepat. 2020, 27, 663–670. [Google Scholar] [CrossRef]
- Benitez, T.M.; Fernando, S.M.; Amini, C.; Saab, S. Geographically Focused Collocated Hepatitis C Screening and Treatment in Los Angeles’s Skid Row. Dig. Dis. Sci. 2020, 65, 3023–3031. [Google Scholar] [CrossRef]
- Grebely, J.; Tyndall, M.W. Management of HCV and HIV infections among people who inject drugs. Curr. Opin. HIV AIDS 2011, 6, 501–507. [Google Scholar] [CrossRef]
- Grebely, J.; Oser, M.; Taylor, L.E.; Dore, G.J. Breaking down the barriers to hepatitis C virus (HCV) treatment among individuals with HCV/HIV coinfection: Action required at the system, provider, and patient levels. J. Infect. Dis. 2013, 207 (Suppl. S1), S19–S25. [Google Scholar] [CrossRef] [Green Version]
- Bajis, S.; Grebely, J.; Cooper, L.; Smith, J.; Owen, G.; Chudleigh, A.; Hajarizadeh, B.; Martinello, M.; Adey, S.; Read, P.; et al. Hepatitis C virus testing, liver disease assessment and treatment uptake among people who inject drugs pre- and post-universal access to direct-acting antiviral treatment in Australia: The LiveRLife study. J. Viral Hepat. 2019, 27, 281–293. [Google Scholar] [CrossRef]
- Treloar, C.; Newland, J.; Rance, J.; Hopwood, M. Uptake and delivery of hepatitis C treatment in opiate substitution treatment: Perceptions of clients and health professionals. J. Viral Hepat. 2010, 17, 839–844. [Google Scholar] [CrossRef]
- Cuomo, G.; Borghi, V.; Andreone, P.; Massari, M.; Villa, E.; Pietrangelo, A.; Verucchi, G.; Ferrari, C. Missed treatment in an Italian HBV infected patients cohort: HBV RER. Dig. Liver Dis. 2016, 48, 1346–1350. [Google Scholar] [CrossRef] [PubMed]
- Schreuder, I.; van der Sande, M.A.; de Wit, M.; Bongaerts, M.; Boucher, C.A.; Croes, E.A.; van Veen, M.G. Seroprevalence of HIV, hepatitis b, and hepatitis c among opioid drug users on methadone treatment in The Netherlands. Harm. Reduct. J. 2010, 7, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statistics Netherlands (CBS). Available online: https://www.cbs.nl/en-gb/onze-diensten/customised-services-microdata/microdata-conducting-your-own-research (accessed on 29 July 2021).
- Mszsubtrajectentab: Gesloten DBC Subtrajecten. Available online: https://www.cbs.nl/nl-nl/onze-diensten/maatwerk-en-microdata/microdata-zelf-onderzoek-doen/microdatabestanden/mszsubtrajectentab-gesloten-dbc-subtrajecten (accessed on 29 July 2021).
- Mszprestatiesvekttab: Geopende Diagnose Behandeling. Available online: https://www.cbs.nl/nl-nl/onze-diensten/maatwerk-en-microdata/microdata-zelf-onderzoek-doen/microdatabestanden/mszprestatiesvekttab-geopende-diagnose-behandeling (accessed on 29 July 2021).
- The Netherlands Health System Review. Nivel Health Systems in Transition 2010. Available online: https://edit-ggz-acc.azurewebsites.net/getmedia/a2213618-e5c0-42ea-9a39-20e7e9a56f2d/nivel_health-systems-in-transition_2010.pdf (accessed on 30 July 2021).
- Result of Negotiations between the Dutch Government, De Nederlandse ggz and Eight Other Stakeholders. Administrative Agreement on the Future of Mental Health Care 2013–2014. 2013. Available online: https://edit-ggz-acc.azurewebsites.net/getmedia/b8ce998f-67af-4d43-a376-694a0e469379/ggznl_National-Agreement-on-the-Future-of-Mental-Health-Care_18062012.pdf (accessed on 30 July 2021).
- Brusselaers, N.; Lagergren, J. The Charlson Comorbidity Index in Registry-based Research. Methods Inf. Med. 2017, 56, 401–406. [Google Scholar] [PubMed]
- Grebely, J.; Hajarizadeh, B.; Lazarus, J.V.; Bruneau, J.; Treloar, C.; International Network on Hepatitis in Substance Users. Elimination of hepatitis C virus infection among people who use drugs: Ensuring equitable access to prevention, treatment, and care for all. Int. J. Drug Policy 2019, 72, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Grebely, J.; Tran, L.; Degenhardt, L.; Dowell-Day, A.; Santo, T., Jr.; Larney, S.; Hickman, M.; Vickerman, P.; French, C.; Butler, K.; et al. Association between opioid agonist therapy and testing, treatment uptake, and treatment outcomes for hepatitis C infection among people who inject drugs: A systematic review and meta-analysis. Clin. Infect. Dis. 2020, 73, e107–e118. [Google Scholar] [CrossRef]
- Graf, C.; Mücke, M.M.; Dultz, G.; Peiffer, K.-H.; Kubesch, A.; Ingiliz, P.; Zeuzem, S.; Herrmann, E.; Vermehren, J. Efficacy of Direct-acting Antivirals for Chronic Hepatitis C Virus Infection in People Who Inject Drugs or Receive Opioid Substitution Therapy: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2020, 70, 2355–2365. [Google Scholar] [CrossRef]
- Van Den Berg, C.; Smit, C.; Van Brüssel, G.; Coutinho, R.; Prins, M. Full participation in harm reduction programmes is associated with decreased risk for human immunodeficiency virus and hepatitis C virus: Evidence from the Amsterdam Cohort Studies among drug users. Addiction 2007, 102, 1454–1462. [Google Scholar] [CrossRef] [Green Version]
- Seedat, F.; Hargreaves, S.; Nellums, L.B.; Ouyang, J.; Brown, M.; Friedland, J.S. How effective are approaches to migrant screening for infectious diseases in Europe? A systematic review. Lancet Infect. Dis. 2018, 18, e259–e271. [Google Scholar] [CrossRef]
- Kim, J.U.; Ingiliz, P.; Shimakawa, Y.; Lemoine, M. Improving care of migrants is key for viral hepatitis elimination in Europe. Bull. World Health Organ. 2021, 99, 280–286. [Google Scholar] [CrossRef]
- Health Insurance Numbers. Available online: https://www.zorgwijzer.nl/faq/cijfers-zorgverzekering (accessed on 13 August 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n (%) | AH+ n (%) | AH− n (%) | |
|---|---|---|---|
| Total | 10,513 | 1371 (13.0) | 9142 (87.0) |
| Male | 6521 (62.0) | 1090 (79.5) | 5431 (59.4) |
| Age at diagnosis (y) (SD) | 47.49 (13.6) | 50.48 (9.0) | 47.04 (14.1) |
| Comorbid conditions (any): | 2190 (20.8) | 360 (26.3) | 1830 (20.0) |
| 282 (2.7) | 65 (4.7) | 217 (2.4) |
| 677 (6.4) | 86 (6.3) | 591 (6.5) |
| 552 (5.3) | 85 (6.2) | 467 (5.1) |
| 217 (2.1) | 95 (6.9) | 122 (1.3) |
| 198 (1.9) | 17 (1.2) | 181 (2.0) |
| Migrant status: * | 6636 (63.1) | 441 (32.2) | 6195 (68.0) |
| 235 (3.5) | 59 (13.4) | 176 (2.8) |
| 132 (2.0) | 26 (5.9) | 106 (1.7) |
| 273 (4.1) | 52 (11.8) | 221 (3.6) |
| 1014 (15.3) | 88 (20.0) | 926 (14.9) |
| 1656 (25.0) | 62 (14.1) | 1594 (25.7) |
| 2603 (39.2) | 65 (14.7) | 2538 (41.0) |
| 723 (10.9) | 89 (20.2) | 634 (10.2) |
| Type of viral hepatitis | |||
| 4105 (39.0) | 992 (72.4) | 3113 (34.1) |
| 2978 (28.3) | 56 (4.1) | 2922 (32.0) |
| 285 (2.7) | 28 (2.0) | 257 (2.8) |
| 3145 (29.9) | 295 (21.5) | 2850 (31.2) |
| Category | Total Median (IQR) | AH+ Median (IQR) | AH− Median (IQR) |
|---|---|---|---|
| Outpatient visits | 3 (2–6) | 4 (2–6) | 3 (2–6) |
| Venipunctures | 2 (1–4) | 2 (1–4) | 2 (1–4) |
| Lab tests | 19 (4–42) | 24 (6–46) | 19 (4–41) |
| Radiology(abdominal) * | 63.9% | 67.5% | 63.4% |
| Other interventions (i.e., endoscopy) * | 9.5% | 13.6% | 8.9% |
| Pathology * | 3.2% | 3.0% | 3.2% |
| (A) | ||||||
| Factor | OR a (Univariate) | 95% CI a | p | aOR ab (Multivariate) | 95% CI | p |
| Addiction history | 0.60 | (0.54, 0.67) | <0.0001 | 0.73 | (0.64–0.82) | <0.0001 |
| (B) | ||||||
| Factor | OR a (Univariate) | 95% CI a | p | aOR ab (Multivariate) | 95% CI | p |
| Addiction history | 1.35 | (1.12, 1.63) | 0.0020 | 1.15 | (0.94–1.40) | 0.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Von den Hoff, D.W.; Berden, F.A.C.; Atsma, F.; Schellekens, A.F.A.; Drenth, J.P.H. Against All Odds? Addiction History Associated with Better Viral Hepatitis Care: A Dutch Nationwide Claims Data Study. J. Clin. Med. 2022, 11, 1146. https://doi.org/10.3390/jcm11041146
Von den Hoff DW, Berden FAC, Atsma F, Schellekens AFA, Drenth JPH. Against All Odds? Addiction History Associated with Better Viral Hepatitis Care: A Dutch Nationwide Claims Data Study. Journal of Clinical Medicine. 2022; 11(4):1146. https://doi.org/10.3390/jcm11041146
Chicago/Turabian StyleVon den Hoff, Daan W., Floor A. C. Berden, Femke Atsma, Arnt F. A. Schellekens, and Joost P. H. Drenth. 2022. "Against All Odds? Addiction History Associated with Better Viral Hepatitis Care: A Dutch Nationwide Claims Data Study" Journal of Clinical Medicine 11, no. 4: 1146. https://doi.org/10.3390/jcm11041146
APA StyleVon den Hoff, D. W., Berden, F. A. C., Atsma, F., Schellekens, A. F. A., & Drenth, J. P. H. (2022). Against All Odds? Addiction History Associated with Better Viral Hepatitis Care: A Dutch Nationwide Claims Data Study. Journal of Clinical Medicine, 11(4), 1146. https://doi.org/10.3390/jcm11041146