
Acetylcholine Use in Modern Cardiac Catheterization Laboratories: A Systematic Review

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Methods
3. Results
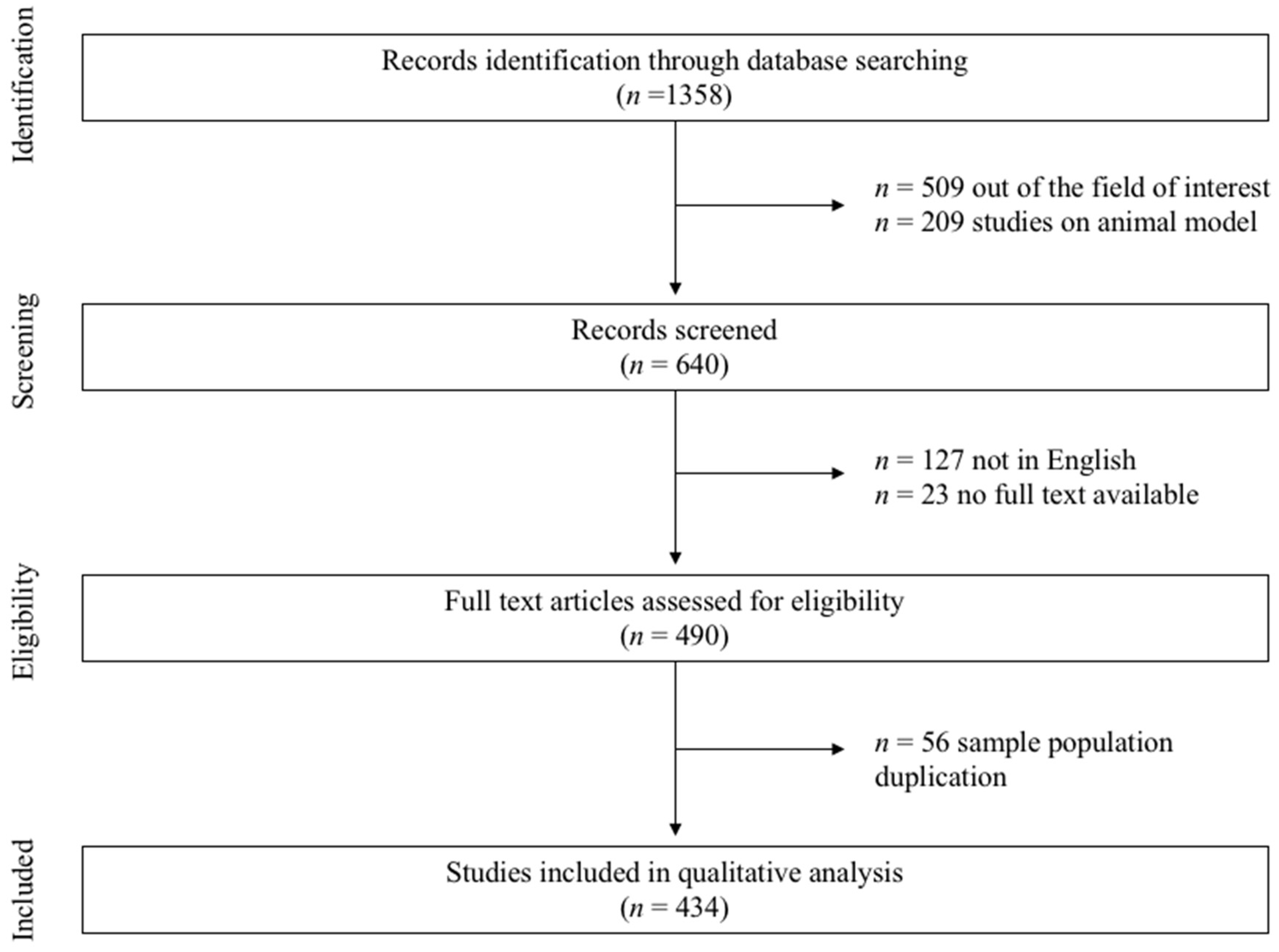
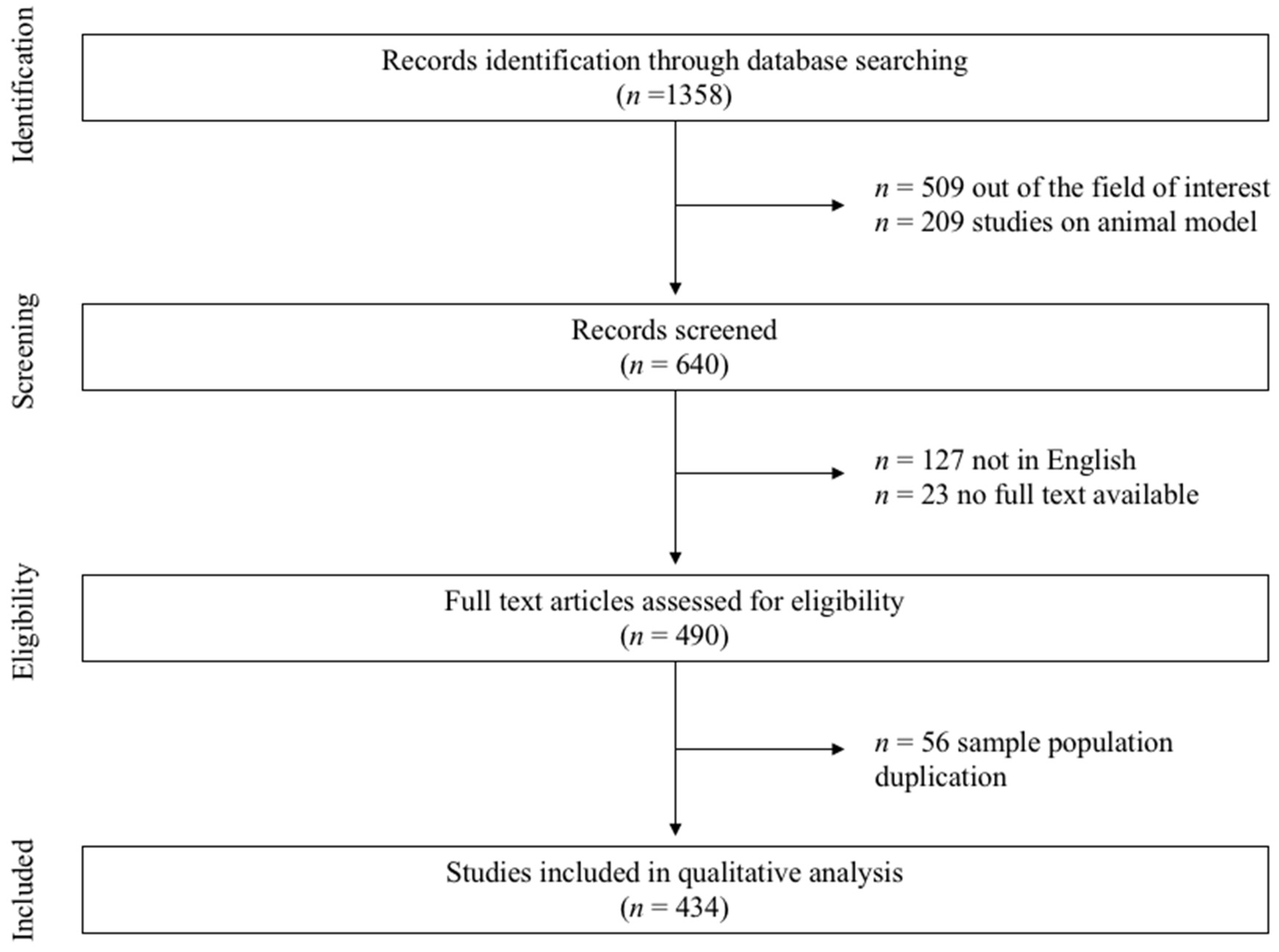
3.1. Search Strategy
3.2. Adverse Events Related to ACh Administration
3.3. INOCA vs. MINOCA
4. Discussion
- The intracoronary use of ACh has been tested in a wide number of studies (specifically, 434).
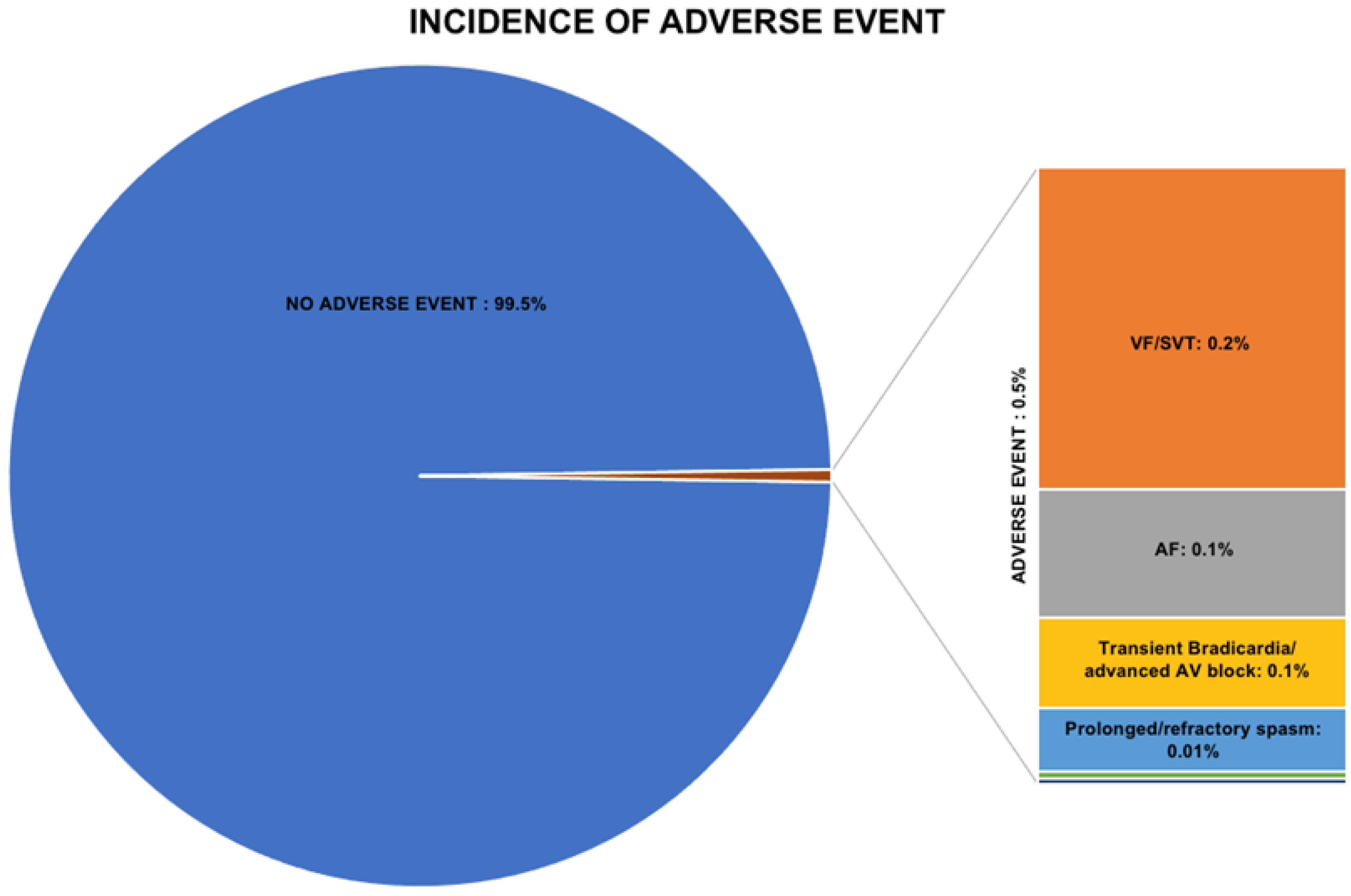
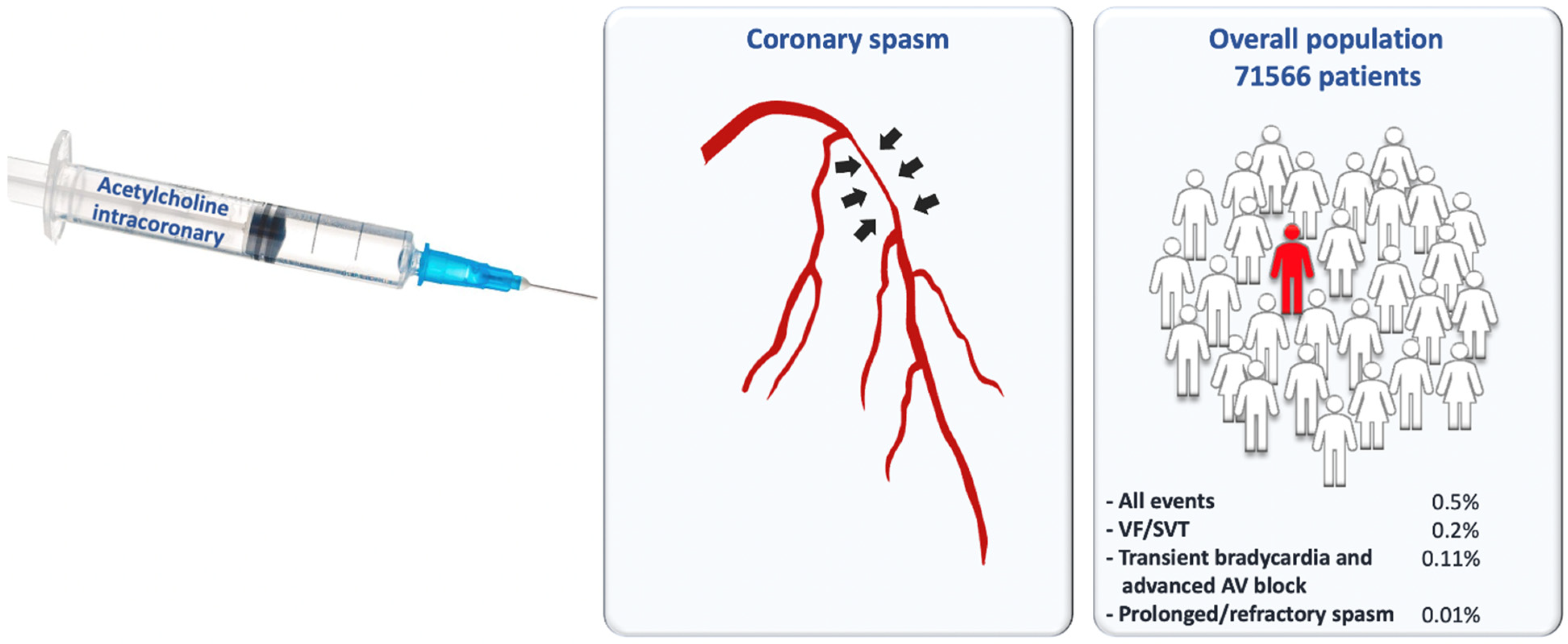
- The total number of reported side effects is low, occurring in 0.5% of the patients included.
- The most frequent side effects are arrhythmic events (VF/SVT and AF occurring in 0.2% and 0.15% of the overall population, respectively).
- Ach-related death has never been described.
- Patients with MINOCA have a significantly lower number of events than INOCA patients when assessed for ACh.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beltrame, J.F.; Crea, F.; Kaski, J.C.; Ogawa, H.; Ong, P.; Sechtem, U.; Shimokawa, H.; Merz, C.N.B.; on behalf of the Coronary Vasomotion Disorders International Study Group (COVADIS). The Who, What, Why, When, How and Where of Vasospastic Angina. Circ. J. 2016, 80, 289–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, T.J.; Corcoran, D.; Berry, C. Stable coronary syndromes: Pathophysiology, diagnostic advances and therapeutic need. Heart 2017, 104, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, Y.; Tamura, Y.; Suzuki, K.; Tanabe, Y.; Yamaguchi, T.; Fujita, T.; Yamazoe, M.; Aizawa, Y.; Shibata, A. Coronary artery spasm is a major cause of sudden cardiac arrest in survivors without underlying heart disease. Coron. Artery Dis. 1993, 4, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Abdu, F.A.; Mohammed, A.-Q.; Liu, L.; Xu, Y.; Che, W. Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA): A Review of the Current Position. Cardiology 2020, 145, 543–552. [Google Scholar] [CrossRef]
- Igarashi, Y.; Tamura, Y.; Tanabe, Y.; Fujita, T.; Yamazoe, M.; Shibata, A. Angina-linked syncope and lack of calcium antagonist therapy predict cardiac arrest before definitive diagnosis of vasospastic angina. Coron. Artery Dis. 1994, 5, 881–887. [Google Scholar]
- Beltrame, J.F.; Crea, F.; Kaski, J.C.; Ogawa, H.; Ong, P.; Sechtem, U.; Shimokawa, H.; Merz, C.N.B. International standardization of diagnostic criteria for vasospastic angina. Eur. Heart J. 2015, 38, 2565–2568. [Google Scholar] [CrossRef] [Green Version]
- Ford, T.; Ong, P.; Sechtem, U.; Beltrame, J.; Camici, P.G.; Crea, F.; Kaski, J.-C.; Merz, C.N.B.; Pepine, C.J.; Shimokawa, H.; et al. Assessment of Vascular Dysfunction in Patients Without Obstructive Coronary Artery Disease. JACC Cardiovasc. Interv. 2020, 13, 1847–1864. [Google Scholar] [CrossRef]
- JCS Joint Working Group. Guidelines for Diagnosis and Treatment of Patients with Vasospastic Angina (Coronary Spastic Angina) (JCS 2013). Circ. J. 2014, 78, 2779–2801. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Cook, D.J.; Eastwood, S.; Olkin, I.; Rennie, D.; Stroup, D.F. Improving the quality of reports of meta-analyses of randomized controlled trials: The QUOROM statement. Lancet 1999, 354, 1896–1900. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epi-demiology: A proposal for reporting. Meta-Analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration, 2009. Available online: https://handbook.cochrane.org (accessed on 18 November 2021).
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Ford, T.; Stanley, B.; Good, R.; Rocchiccioli, P.; McEntegart, M.; Watkins, S.; Eteiba, H.; Shaukat, A.; Lindsay, M.; Robertson, K.; et al. Stratified Medical Therapy Using Invasive Coronary Function Testing in Angina. J. Am. Coll. Cardiol. 2018, 72, 2841–2855. [Google Scholar] [CrossRef]
- Gomez-Lara, J.; Brugaletta, S.; Ortega-Paz, L.; Vandeloo, B.; Moscarella, E.; Salas, M.; Romaguera, R.; Roura, G.; Ferreiro, J.L.; Teruel, L.; et al. Long-Term Coronary Functional Assessment of the Infarct-Related Artery Treated with Everolimus-Eluting Bioresorbable Scaffolds or Everolimus-Eluting Metallic Stents. JACC Cardiovasc. Interv. 2018, 11, 1559–1571. [Google Scholar] [CrossRef]
- Corcoran, D.; Young, R.; Cialdella, P.; McCartney, P.; Bajrangee, A.; Hennigan, B.; Collison, D.; Carrick, D.; Shaukat, A.; Good, R.; et al. The effects of remote ischaemic preconditioning on coronary artery function in patients with stable coronary artery disease. Int. J. Cardiol. 2018, 252, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Aoki, Y.; Ishikawa, K.; Miura, K.; Sugimoto, K.; Nakayama, T.; Fujimoto, Y.; Kobayashi, Y. Protective effect of angiotensin II receptor blocker and calcium channel blocker on endothelial vasomotor function after everolimus-eluting stent implantation. J. Cardiol. 2015, 67, 236–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mischie, A.N.; Nazzaro, M.S.; Fiorilli, R.; De Felice, F.; Musto, C.; Confessore, P.; Parma, A.; Boschetti, C.; Violini, R. Head-to-head comparison of sirolimus-eluting stent versus bare metal stent evaluation of the coronary endothelial dysfunction in the same patient presenting with multiple coronary artery lesions: The CREDENTIAL study. Catheter. Cardiovasc. Interv. 2013, 82, E184–E191. [Google Scholar] [CrossRef] [PubMed]
- Belkacemi, A.; Agostoni, P.; Nathoe, H.M.; Voskuil, M.; Shao, C.; VAN Belle, E.; Wildbergh, T.; Politi, L.; Doevendans, P.A.; Sangiorgi, G.; et al. First Results of the DEB-AMI (Drug Eluting Balloon in Acute ST-Segment Elevation Myocardial Infarction) Trial: A Multicenter Randomized Comparison of Drug-Eluting Balloon Plus Bare-Metal Stent Versus Bare-Metal Stent Versus Drug-Eluting Stent in Primary Percutaneous Coronary Intervention With 6-Month Angiographic, Intravascular, Functional, and Clinical Outcomes. J. Am. Coll. Cardiol. 2012, 59, 2327–2337. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Seo, H.S.; Park, J.H.; Na, J.O.; Choi, C.U.; Lim, H.E.; Kim, E.J.; Rha, S.-W.; Park, C.G.; Oh, D.J. A Prospective, Randomized, 6-Month Comparison of the Coronary Vasomotor Response Associated with a Zotarolimus- Versus a Sirolimus-Eluting Stent: Differential Recovery of Coronary Endothelial Dysfunction. J. Am. Coll. Cardiol. 2009, 53, 1653–1659. [Google Scholar] [CrossRef] [Green Version]
- Lüscher, T.F.; Pieper, M.; Tendera, M.; Vrolix, M.; Rutsch, W.; Branden, F.V.D.; Gil, R.; Bischoff, K.-O.; Haude, M.; Fischer, D.; et al. A randomized placebo-controlled study on the effect of nifedipine on coronary endothelial function and plaque formation in patients with coronary artery disease: The ENCORE II study. Eur. Heart J. 2009, 30, 1590–1597. [Google Scholar] [CrossRef] [Green Version]
- Yasue, H.; Mizuno, Y.; Harada, E.; Itoh, T.; Nakagawa, H.; Nakayama, M.; Ogawa, H.; Tayama, S.; Honda, T.; Hokimoto, S.; et al. Effects of a 3-Hydroxy-3-Methylglutaryl Coenzyme A Reductase Inhibitor, Fluvastatin, on Coronary Spasm After Withdrawal of Calcium-Channel Blockers. J. Am. Coll. Cardiol. 2008, 51, 1742–1748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ENCORE Investigators. Effect of nifedipine and cerivastatin on coronary endothelial function in patients with coronary artery disease: The ENCORE I Study (Evaluation of Nifedipine and Cerivastatin On Recovery of coronary Endothelial function). Circulation 2003, 107, 422–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azevedo, E.R.; Schofield, A.M.; Kelly, S.; Parker, J.D. Nitroglycerin withdrawal increases endothelium-dependent vasomotor response to acetylcholine. J. Am. Coll. Cardiol. 2001, 37, 505–509. [Google Scholar] [CrossRef] [Green Version]
- Hambrecht, R.; Wolf, A.; Gielen, S.; Linke, A.; Hofer, J.; Erbs, S.; Schoene, N.; Schuler, G. Effect of Exercise on Coronary Endothelial Function in Patients with Coronary Artery Disease. N. Engl. J. Med. 2000, 342, 454–460. [Google Scholar] [CrossRef]
- Lerman, A.; Burnett, J.J.C.; Higano, S.T.; McKinley, L.J.; Holmes, J.D.R. Long-term l -Arginine Supplementation Improves Small-Vessel Coronary Endothelial Function in Humans. Circulation 1998, 97, 2123–2128. [Google Scholar] [CrossRef] [Green Version]
- Treasure, C.B.; Klein, J.L.; Weintraub, W.S.; Talley, J.D.; Stillabower, M.E.; Kosinski, A.S.; Zhang, J.; Boccuzzi, S.J.; Cedarholm, J.C.; Alexander, R.W. Beneficial Effects of Cholesterol-Lowering Therapy on the Coronary Endothelium in Patients with Coronary Artery Disease. N. Engl. J. Med. 1995, 332, 481–487. [Google Scholar] [CrossRef]
- Yasue, H.; Horio, Y.; Nakamura, N.; Fujii, H.; Imoto, N.; Sonoda, R.; Kugiyama, K.; Obata, K.; Morikami, Y.; Kimura, T. Induction of coronary artery spasm by acetylcholine in patients with variant angina: Possible role of the parasympathetic nervous system in the pathogenesis of coronary artery spasm. Circulation 1986, 74, 955–963. [Google Scholar] [CrossRef]
- Scalone, G.; Niccoli, G.; Crea, F. Editor’s Choice- Pathophysiology, diagnosis and management of MINOCA: An update. Eur. Heart J. Acute Cardiovasc. Care 2018, 8, 54–62. [Google Scholar] [CrossRef]
- Ciliberti, G.; Seshasai, S.R.K.; Ambrosio, G.; Kaski, J.C. Safety of intracoronary provocative testing for the diagnosis of coronary artery spasm. Int. J. Cardiol. 2017, 244, 77–83. [Google Scholar] [CrossRef]
- Yasue, H.; Kugiyama, K. Coronary Spasm: Clinical Features and Pathogenesis. Intern. Med. 1997, 36, 760–765. [Google Scholar] [CrossRef] [Green Version]
- Isogai, T.; Yasunaga, H.; Matsui, H.; Tanaka, H.; Ueda, T.; Horiguchi, H.; Fushimi, K. Serious Cardiac Complications in Coronary Spasm Provocation Tests Using Acetylcholine or Ergonovine: Analysis of 21512 Patients from the Diagnosis Procedure Combination Database in Japan. Clin. Cardiol. 2015, 38, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Ong, P.; Athanasiadis, A.; Borgulya, G.; Mahrholdt, H.; Kaski, J.C.; Sechtem, U. High Prevalence of a Pathological Response to Acetylcholine Testing in Patients with Stable Angina Pectoris and Unobstructed Coronary Arteries: The ACOVA Study (Abnormal COronary VAsomotion in patients with stable angina and unobstructed coronary arteries). J. Am. Coll. Cardiol. 2012, 59, 655–662. [Google Scholar] [CrossRef] [Green Version]
- Takagi, Y.; Yasuda, S.; Takahashi, J.; Tsunoda, R.; Ogata, Y.; Seki, A.; Sumiyoshi, T.; Matsui, M.; Goto, T.; Tanabe, Y.; et al. Clinical implications of provocation tests for coronary artery spasm: Safety, arrhythmic complications, and prognostic impact: Multicentre Registry Study of the Japanese Coronary Spasm Association. Eur. Heart J. 2012, 34, 258–267. [Google Scholar] [CrossRef] [Green Version]
- Sueda, S.; Saeki, H.; Otani, T.; Mineoi, K.; Kondou, T.; Yano, K.; Ochi, T.; Ochi, N.; Hayashi, Y.; Tsuruoka, T.; et al. Major complications during spasm provocation tests with an intracoronary injection of acetylcholine. Am. J. Cardiol. 2000, 85, 391–394. [Google Scholar] [CrossRef]
- Sato, K.; Kaikita, K.; Nakayama, N.; Horio, E.; Yoshimura, H.; Ono, T.; Ohba, K.; Tsujita, K.; Kojima, S.; Tayama, S.; et al. Coronary vasomotor response to intracoronary acetylcholine injection, clinical features, and long-term prognosis in 873 consecutive patients with coronary spasm: Analysis of a single-center study over 20 years. J. Am. Heart Assoc. 2013, 2, e000227. [Google Scholar] [CrossRef] [Green Version]
- Sueda, S.; Kohno, H.; Miyoshi, T.; Sakaue, T.; Sasaki, Y.; Habara, H. Maximal acetylcholine dose of 200 μg into the left coronary artery as a spasm provocation test: Comparison with 100 μg of acetylcholine. Heart Vessel. 2014, 30, 771–778. [Google Scholar] [CrossRef]
- Montalescot, G.; Sechtem, U.; Achenbach, S.; Andreotti, F.; Arden, C.; Budaj, A.; Bugiardini, R.; Crea, F.; Cuisset, T.; Di Mario, C. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur. Heart J. 2013, 34, 2949–3003. [Google Scholar]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey, D.E.; Ganiats, T.G.; Holmes, D.R.; Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Non–ST-Elevation Acute Coronary Syndromes. Circulation 2014, 130, e344–e426. [Google Scholar] [CrossRef]
- Aziz, A.; Hansen, H.S.; Sechtem, U.; Prescott, E.; Ong, P. Sex-Related Differences in Vasomotor Function in Patients with Angina and Unobstructed Coronary Arteries. J. Am. Coll. Cardiol. 2017, 70, 2349–2358. [Google Scholar] [CrossRef]
- Pargaonkar, V.S.; Lee, J.H.; Chow, E.K.; Nishi, T.; Ball, R.L.; Kobayashi, Y.; Kimura, T.; Lee, D.P.; Stefanick, M.L.; Fearon, W.F.; et al. Dose-Response Relationship Between Intracoronary Acetylcholine and Minimal Lumen Diameter in Coronary Endothelial Function Testing of Women and Men with Angina and No Obstructive Coronary Artery Disease. Circ. Cardiovasc. Interv. 2020, 13, e008587. [Google Scholar] [CrossRef]
- Nishigaki, K.; Inoue, Y.; Yamanouchi, Y.; Fukumoto, Y.; Yasuda, S.; Sueda, S.; Urata, H.; Shimokawa, H.; Minatoguchi, S. Prognostic Effects of Calcium Channel Blockers in Patients with Vasospastic Angina—A Meta-Analysis. Circ. J. 2010, 74, 1943–1950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishii, M.; Kaikita, K.; Sato, K.; Yamanaga, K.; Miyazaki, T.; Akasaka, T.; Tabata, N.; Arima, Y.; Sueta, D.; Sakamoto, K.; et al. Impact of Statin Therapy on Clinical Outcome in Patients with Coronary Spasm. J. Am. Heart Assoc. 2016, 5, e003426. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| First Author | Year of Publication | Type of Study | Study Population | Diagnosis | ACh Route of Administration | ACh Dosage | Side Effects, n of Patients | Kinds of Side Effect, Type (n) |
|---|---|---|---|---|---|---|---|---|
| Ford, T.J. [14] | 2018 | RCT | 151 | INOCA | Intracoronary | Incremental doses of 10−6, 10−5, and 10−4 mol/L | 9 | Persistent AF (1); paroxysmal AF (8). |
| Gomez-Lara, J. [15] | 2018 | RCT | 63 | CCS | Intracoronary | Incremental doses of 10−6 M and 10−4 M | 0 | 0 |
| Corcoran, D. [16] | 2018 | RCT | 75 | CCS | Intracoronary | 10−6, 10−5, and 10−4 mol/L | 0 | 0 |
| Aoki, Y. [17] | 2016 | RCT | 40 | CCS | Intracoronary | Incremental doses of ACh at 10−8 and 10−7 mol/L f | 0 | 0 |
| Mischie, A.N. [18] | 2013 | RCT | 24 | CCS | Intracoronary | 10−5 mol/L | 2 | Temporary asystole (less than 5 s) that recovered spontaneously (2). |
| Belkacemi, A. [19] | 2012 | RCT | 150 | CCS | Intracoronary | Incremental doses of 10−6, 10−5, and 10−4 mol/L/mL | 0 | 0 |
| Kim, J.W. [20] | 2009 | RCT | 55 | CCS | Intracoronary | Incremental doses of 10 μg, 20 μg, 50 μg, and 100 μg | 0 | 0 |
| Lüscher, T.F. [21] | 2009 | RCT | 454 | CCS | Intracoronary | 10−6 to 10−4 | 2 | Diffuse coronary vasoconstriction with marked hemodynamic consequences requiring resuscitation (1); MI (1). |
| Yasue, H. [22] | 2008 | RCT | 78 | INOCA | Intracoronary | Incremental doses of 50 and 100 μg in LCA, 50 μg in RCA | 0 | 0 |
| ENCORE investigators [23] | 2003 | RCT | 343 | CCS | Intracoronary | 2 mL/min for 3 min acetylcholine 0.36, 3.6, and 18 mcg/mL | 2 | Diffuse vasoconstriction with hemodynamic consequences requiring resuscitation, in both cases without sequelae (2). |
| Azevedo, E.R. [24] | 2001 | RCT | 20 | CCS | Intracoronary | 10−4 mol/L | 2 | Bradycardia/2nd degree AV block requiring no temporary pacing or atropine. |
| Hambrecht, R. [25] | 2000 | RCT | 19 | CCS | Intracoronary | Increasing doses of 0.072, 0.72, and 7.2 mcg | 0 | 0 |
| Lerman, A. [26] | 1998 | RCT | 26 | Non obstructive CAD | Intracoronary | 10−6 to 10−4 mol/L) | 0 | 0 |
| Treasure, C.B. [27] | 1995 | RCT | 23 | CCS | Intracoronary | Incremental doses of 10−9 M, 10−8 M, 10−7 M, and 10−6 M | 0 | 0 |
| Adverse Event | RCT, n = 1521 Patients n, (%) | Observational Studies, n = 70,045 Patients n, (%) | Overall Population, n = 71,566 Patients n, (%) |
|---|---|---|---|
| All events | 17, (1.12) | 365, (0.5) | 382, (0.5) |
| VF/SVT | 0, (0) | 148, (0.21) | 148, (0.20) |
| AF | 9, (0.59) | 102, (0.14) | 111, (0.15) |
| Transient bradycardia and advanced AV block | 4, (0.26) | 78, (0.11) | 82, (0.11) |
| Prolonged/refractory spasm | 3, (0.19) | 9, (0.01) | 12, (0.01) |
| NSVT | 0, (0) | 10, (0.01) | 10, (0.01) |
| Hypotension | 0, (0) | 8, (0.01) | 8, (0.01) |
| Shock | 0, (0) | 6, (<0.01) | 6, (<0.01) |
| MI | 1, (0.06) | 4, (<0.01) | 5, (<0.01) |
| Death | 0, (0) | 0, (0) | 0, (0) |
| Society | Recommendations | Class and Level of Evidence |
|---|---|---|
| 2015 COVADIS [1]. | Suspected history of VSA without documented episode, especially if nitrate-responsive rest angina, and/or marked diurnal variation in symptom onset/exercise tolerance, and/or rest angina without obstructive coronary artery disease. Unresponsive to empiric therapy. Acute coronary syndrome presentation in the absence of a culprit lesion. Unexplained resuscitated cardiac arrest. Unexplained syncope with antecedent chest pain. Recurrent rest angina following angiographically successful PCI. | I |
| Invasive testing for non-invasive diagnosed patients unresponsive to drug therapy. Documented spontaneous episode of VSA to determine the ‘site and mode’ of spasm. | IIa | |
| Invasive testing for non-invasive diagnosed patients responsive to drug therapy. | IIb | |
| Emergent acute coronary syndrome. Severe fixed multi-vessel coronary artery disease including left main stenosis. Severe myocardial dysfunction (Class IIb if symptoms suggestive of vasospasm). Patients without any symptoms suggestive of VSA. | III | |
| 2013 JCS [8]. | ACh provocation test during coronary angiography performed in patients in whom vasospastic angina is suspected based on symptoms, but who have not been diagnosed with coronary spasm by non-invasive evaluation. | I |
| ACh provocation test during coronary angiography performed in patients who have been diagnosed with coronary spasm by non-invasive evaluation, and in whom medical treatment is ineffective or insufficiently effective. | IIa | |
| ACh provocation test during coronary angiography performed in patients who have been diagnosed with coronary spasm by non-invasive evaluation, and in whom medical treatment has been proven to be effective. | IIb | |
| ACh provocation test during coronary angiography performed in patients without symptoms suggestive of vasospastic angina. ACh provocation test during coronary angiography performed in patients who are considered at high risk of suffering a life-threatening complication of induced coronary spasm (e.g., patients with left main coronary trunk lesions; those with multivessel coronary lesions, including obstructive lesions; those with severe cardiac dysfunction; those with untreated congestive heart failure). However, in cases in which the onset of severe cardiac dysfunction or congestive heart failure may be a consequence of coronary spasm, the criteria for Class IIb apply). ACh provocation test during emergent coronary angiography performed in patients with acute coronary syndrome. | III | |
| 2013 ESC Stable coronary CAD [38] | Intracoronary provocative testing should be considered to identify coronary spasm in patients with normal findings or non-obstructive lesions on coronary arteriography and the clinical picture of coronary spasm to diagnose the site and mode of spasm. | IIa, C |
| 2014 AHA/ACC, NSTE-ACS [39] | Provocative testing during invasive coronary angiography may be considered in patients with suspected vasospastic angina when clinical criteria and non-invasive testing fail to establish the diagnosis. | IIb, B |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marrone, A.; Pavasini, R.; Scollo, E.; Gibiino, F.; Pompei, G.; Caglioni, S.; Biscaglia, S.; Campo, G.; Tebaldi, M. Acetylcholine Use in Modern Cardiac Catheterization Laboratories: A Systematic Review. J. Clin. Med. 2022, 11, 1129. https://doi.org/10.3390/jcm11041129
Marrone A, Pavasini R, Scollo E, Gibiino F, Pompei G, Caglioni S, Biscaglia S, Campo G, Tebaldi M. Acetylcholine Use in Modern Cardiac Catheterization Laboratories: A Systematic Review. Journal of Clinical Medicine. 2022; 11(4):1129. https://doi.org/10.3390/jcm11041129
Chicago/Turabian StyleMarrone, Andrea, Rita Pavasini, Ennio Scollo, Federico Gibiino, Graziella Pompei, Serena Caglioni, Simone Biscaglia, Gianluca Campo, and Matteo Tebaldi. 2022. "Acetylcholine Use in Modern Cardiac Catheterization Laboratories: A Systematic Review" Journal of Clinical Medicine 11, no. 4: 1129. https://doi.org/10.3390/jcm11041129
APA StyleMarrone, A., Pavasini, R., Scollo, E., Gibiino, F., Pompei, G., Caglioni, S., Biscaglia, S., Campo, G., & Tebaldi, M. (2022). Acetylcholine Use in Modern Cardiac Catheterization Laboratories: A Systematic Review. Journal of Clinical Medicine, 11(4), 1129. https://doi.org/10.3390/jcm11041129