
Ideal Depth of Endotracheal Intubation at the Vocal Cord Level in Pediatric Patients Considering Racial Differences in Tracheal Length



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol and Patients
2.2. Retrospective Observational Study to Determine a Formula to Predict the Tracheal Length in Pediatric Patients
2.3. Statistical Analyses
3. Results
3.1. Parameters Showing the Strongest Correlation with Tracheal Length in Cardiac Pediatric Patients (Germany)
3.2. Validity of Tracheal Length Measurements in the Supine Position (Germany)
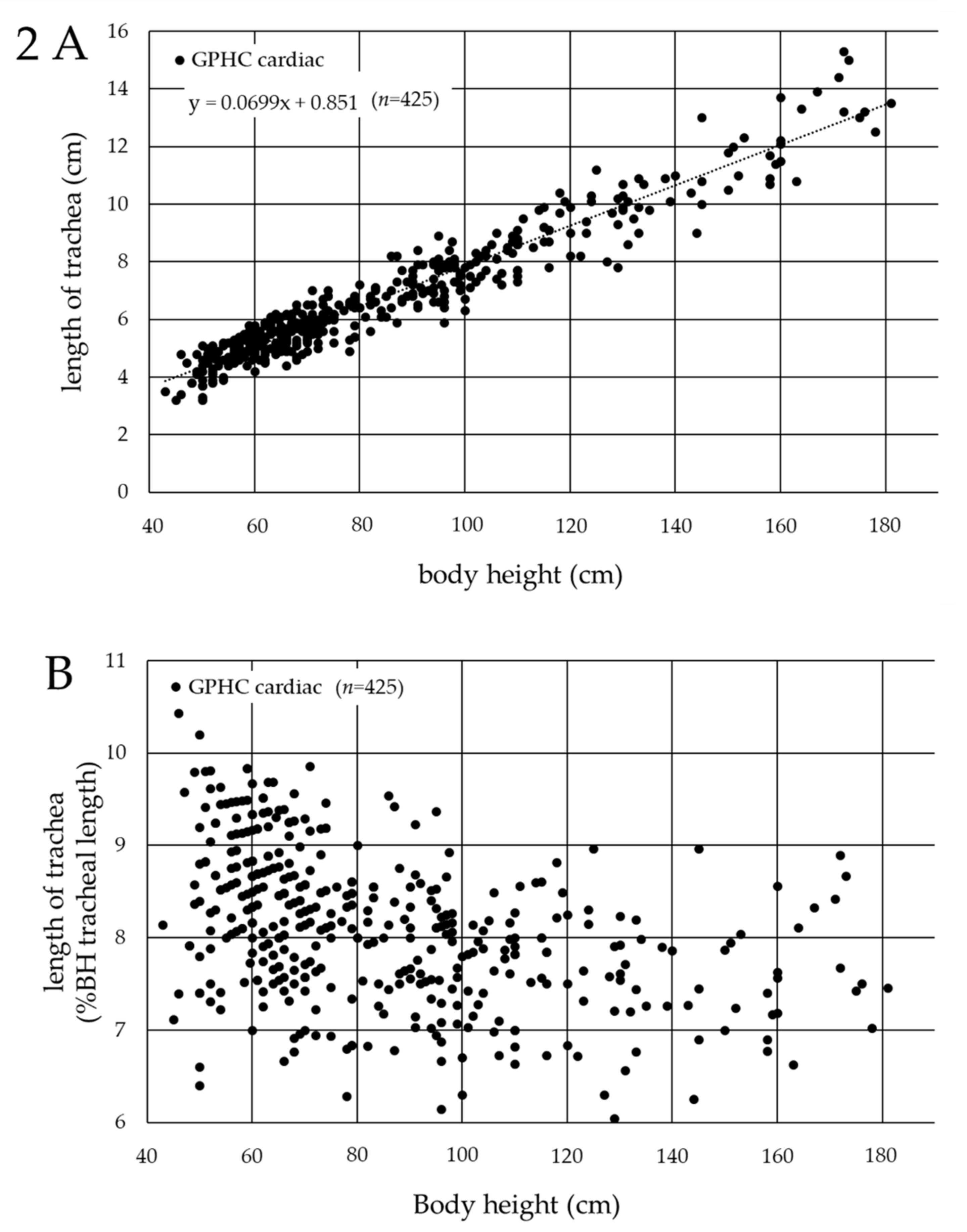
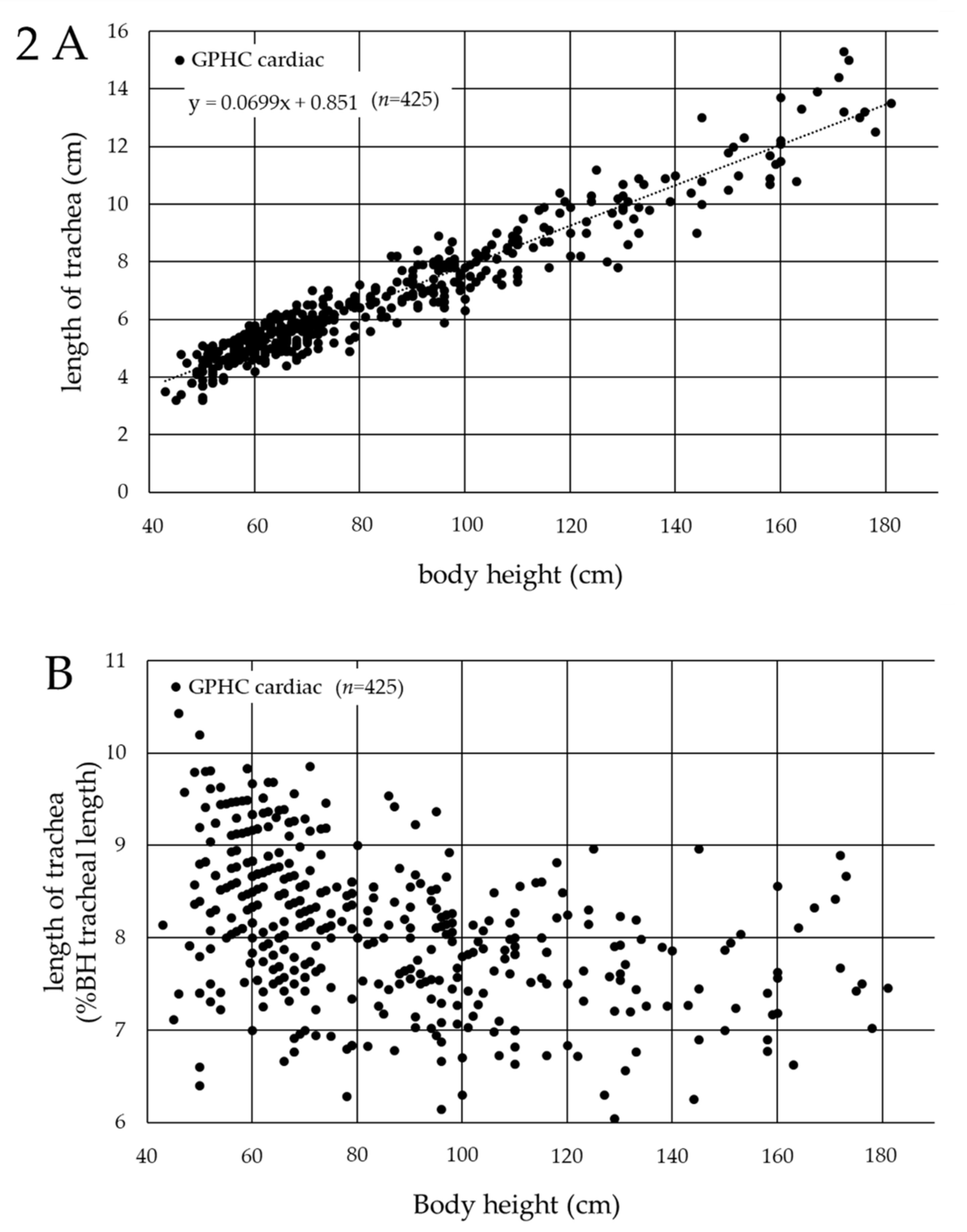
3.3. Association between Tracheal Length and Body Height in Cardiac Pediatric Patients in Germany
3.4. Association between Tracheal Length and Body Height in Cardiac Pediatric Patients in Japan
3.5. Comparison of the Tracheal Length in Cardiac Pediatric Patients between Germany and Japan
3.6. Comparison of the Diameters of the Trachea and Bronchi (Japan)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Weiss, M.; Dullenkopf, A.; Gysin, C.; Dillier, C.M.; Gerber, A.C. Shortcomings of cuffed paediatric tracheal tubes. Br. J. Anaesth. 2004, 92, 78–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivera, R.; Tibballs, J. Complications of endotracheal intubation and mechanical ventilation in infants and children. Crit. Care Med. 1992, 20, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Bloch, E.C.; Ossey, K.; Ginsberg, B. Tracheal intubation in children: A new method for assuring correct depth of tube placement. Anesth. Analg. 1988, 67, 590–592. [Google Scholar] [CrossRef] [PubMed]
- Mariano, E.R.; Ramamoorthy, C.; Chu, L.F.; Chen, M.; Hammer, G.B. A comparison of three methods for estimating appropriate tracheal tube depth in children. Paediatr. Anaesth. 2005, 15, 846–851. [Google Scholar] [CrossRef]
- Cole, F. Pediatric formulas for the anesthesiologist. AMA J. Dis. Child. 1957, 94, 672–673. [Google Scholar] [CrossRef]
- Khine, H.H.; Corddry, D.H.; Kettrick, R.G.; Martin, T.M.; McCloskey, J.J.; Rose, J.B.; Theroux, M.C.; Zagnoev, M. Comparison of cuffed and uncuffed endotracheal tubes in young children during general anesthesia. Anesthesiology 1997, 86, 627–631. [Google Scholar] [CrossRef]
- American Heart Association. 2005 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) of pediatric and neonatal patients: Pediatric basic life support. Pediatrics 2006, 117, e989–e1004. [Google Scholar] [CrossRef]
- Phipps, L.M.; Thomas, N.J.; Gilmore, R.K.; Raymond, J.A.; Bittner, T.R.; Orr, R.A.; Robertson, C.L. Prospective assessment of guidelines for determining appropriate depth of endotracheal tube placement in children. Pediatr. Crit. Care Med. 2005, 6, 519–522. [Google Scholar] [CrossRef]
- Techanivate, A.; Kumwilaisak, K.; Samranrean, S. Estimation of the proper length of orotracheal intubation by Chula formula. J. Med. Assoc. Thai. 2005, 88, 1838–1846. [Google Scholar]
- Techanivate, A.; Kumwilaisak, K.; Worasawate, W.; Tanyong, A. Estimation of the proper length of nasotracheal intubation by Chula formula. J. Med. Assoc. Thai. 2008, 91, 173–180. [Google Scholar]
- Kim, K.O.; Um, W.S.; Kim, C.S. Comparative evaluation of methods for ensuring the correct position of the tracheal tube in children undergoing open heart surgery. Anaesthesia 2003, 58, 889–893. [Google Scholar] [CrossRef] [PubMed]
- Weiss, M.; Knirsch, W.; Kretschmar, O.; Dullenkopf, A.; Tomaske, M.; Balmer, C.; Stutz, K.; Gerber, A.C.; Berger, F. Tracheal tube-tip displacement in children during head-neck movement—A radiological assessment. Br. J. Anaesth. 2006, 96, 486–491. [Google Scholar] [CrossRef] [Green Version]
- Jing, B.S. Roentgen examination of the larynx and hypopharynx. Radiol. Clin. N. Am. 1970, 8, 361–386. [Google Scholar] [PubMed]
- Ferro, P.S.; North, L.B. Roentgenological appearance of lesions of the larynx. CRC Crit. Rev. Diagn. Imaging 1979, 11, 335–382. [Google Scholar] [PubMed]
- Lee, K.S.; Yang, C.C. Tracheal length of infants under three months old. Ann. Otol. Rhinol. Laryngol. 2001, 110, 268–270. [Google Scholar] [CrossRef]
- Morgan, G.A.; Steward, D.J. Linear airway dimensions in children: Including those from cleft palate. Can. Anaesth. Soc. J. 1982, 29, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Leader, J.K.; Rogers, R.M.; Fuhrman, C.R.; Sciurba, F.C.; Zheng, B.; Thompson, P.F.; Weissfeld, J.L.; Golla, S.K.; Gur, D. Size and morphology of the trachea before and after lung volume reduction surgery. AJR Am. J. Roentgenol. 2004, 183, 315–321. [Google Scholar] [CrossRef]
- Reed, J.M.; O’Connor, D.M.; Myer, C.M., 3rd. Magnetic resonance imaging determination of tracheal orientation in normal children. Practical implications. Arch. Otolaryngol. Head Neck Surg. 1996, 122, 605–608. [Google Scholar] [CrossRef]
- Hartrey, R.; Kestin, I.G. Movement of oral and nasal tracheal tubes as a result of changes in head and neck position. Anaesthesia 1995, 50, 682–687. [Google Scholar] [CrossRef]
- Jin-Hee, K.; Ro, Y.J.; Seong-Won, M.; Chong-Soo, K.; Seong-Deok, K.; Lee, J.H.; Jae-Hyon, B. Elongation of the trachea during neck extension in children: Implications of the safety of endotracheal tubes. Anesth. Analg. 2005, 101, 974–977. [Google Scholar] [CrossRef]
- Kim, J.T.; Kim, H.J.; Ahn, W.; Kim, H.S.; Bahk, J.H.; Lee, S.C.; Kim, C.S.; Kim, S.D. Head rotation, flexion, and extension alter endotracheal tube position in adults and children. Can. J. Anaesth. 2009, 56, 751–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangar, D.; Sprenker, C.J.; Karlnoski, R.A.; Dodson, R.K.; Brashears, B.H.; Downes, K.L.; Camporesi, E.M. Migration of polyurethane high-volume low-pressure cuffed endotracheal tubes after neck flexion and extension. J. Anesth. 2013, 27, 633–634. [Google Scholar] [CrossRef] [PubMed]
- Herway, S.T.; Benumof, J.L. The tracheal accordion and the position of the endotracheal tube. Anaesth. Intensive Care 2017, 45, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Olufolabi, A.J.; Charlton, G.A.; Spargo, P.M. Effect of head posture on tracheal tube position in children. Anaesthesia 2004, 59, 1069–1072. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, K.; Yokoyama, K. Displacement of the endotracheal tube caused by change of head position in pediatric anesthesia: Evaluation by fiberoptic bronchoscopy. Anesth. Analg. 1996, 82, 251–253. [Google Scholar] [PubMed]
- Yoo, S.Y.; Kim, J.H.; Han, S.H.; Oh, A.Y. A comparative study of endotracheal tube positioning methods in children: Safety from neck movement. Anesth. Analg. 2007, 105, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Trout, S.; Aaron, J.; Zapta-Sirvent, R.L.; Hansbrough, J.F. Influence of head and neck position on endotracheal tube tip position on chest x-ray examination: A potential problem in the infant undergoing intubation. J. Burn Care Rehabil. 1994, 15, 405–407. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamamoto, T.; Schindler, E. Ideal Depth of Endotracheal Intubation at the Vocal Cord Level in Pediatric Patients Considering Racial Differences in Tracheal Length. J. Clin. Med. 2022, 11, 864. https://doi.org/10.3390/jcm11030864
Yamamoto T, Schindler E. Ideal Depth of Endotracheal Intubation at the Vocal Cord Level in Pediatric Patients Considering Racial Differences in Tracheal Length. Journal of Clinical Medicine. 2022; 11(3):864. https://doi.org/10.3390/jcm11030864
Chicago/Turabian StyleYamamoto, Tomohiro, and Ehrenfried Schindler. 2022. "Ideal Depth of Endotracheal Intubation at the Vocal Cord Level in Pediatric Patients Considering Racial Differences in Tracheal Length" Journal of Clinical Medicine 11, no. 3: 864. https://doi.org/10.3390/jcm11030864
APA StyleYamamoto, T., & Schindler, E. (2022). Ideal Depth of Endotracheal Intubation at the Vocal Cord Level in Pediatric Patients Considering Racial Differences in Tracheal Length. Journal of Clinical Medicine, 11(3), 864. https://doi.org/10.3390/jcm11030864