
Cause of Death in Heart Failure Based on Etiology: Long-Term Cohort Study of All-Cause and Cardiovascular Mortality

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Outcomes
2.2. Etiology of HF
2.2.1. Ischemic Heart Disease
2.2.2. Dilated Cardiomyopathy
2.2.3. Hypertensive Heart Disease
2.2.4. Alcoholic Cardiomyopathy
2.2.5. Drug-Induced Cardiomyopathy
2.2.6. Valvular Heart Disease
2.2.7. Hypertrophic Cardiomyopathy
2.2.8. Other Etiologies
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
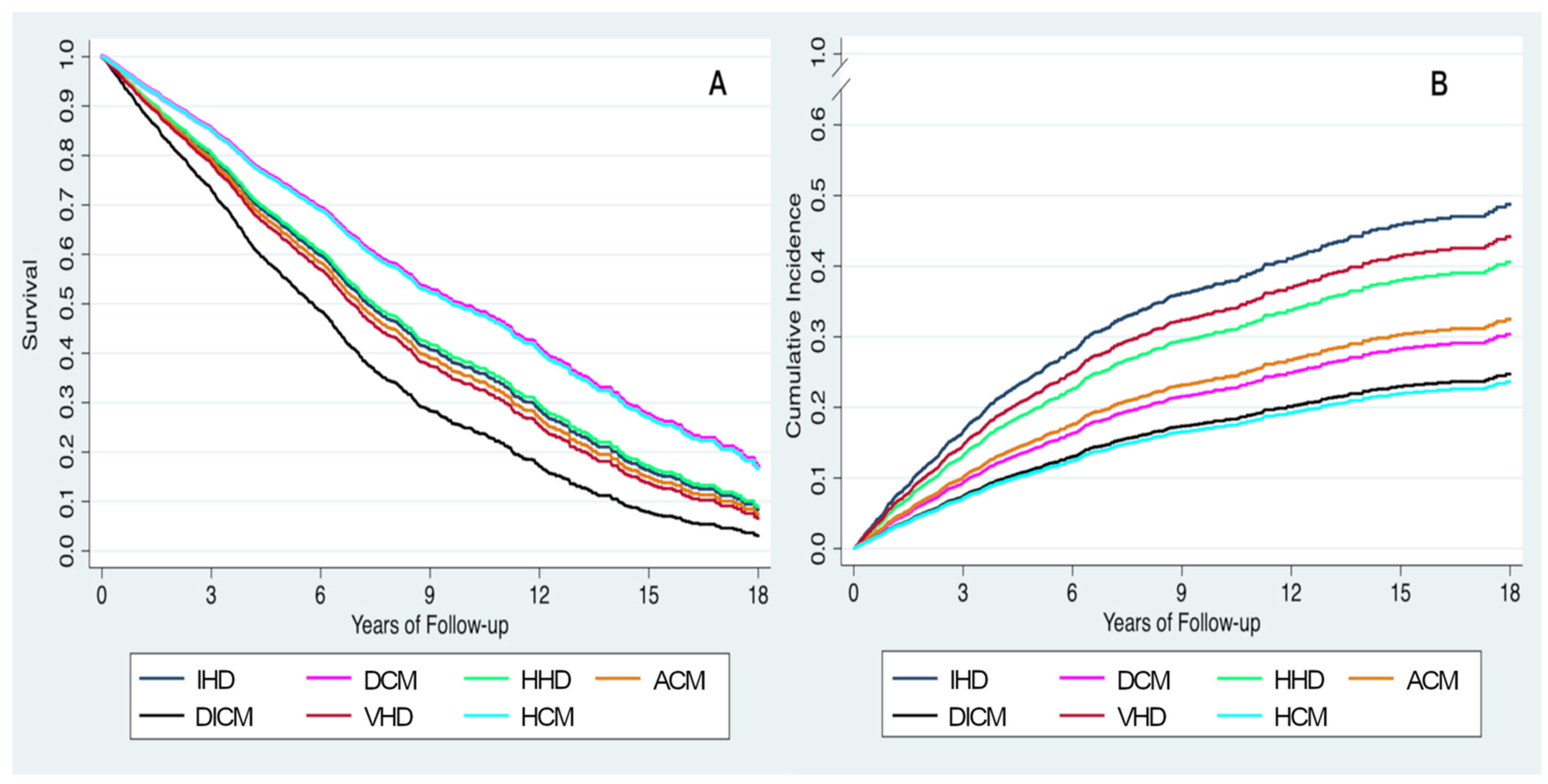
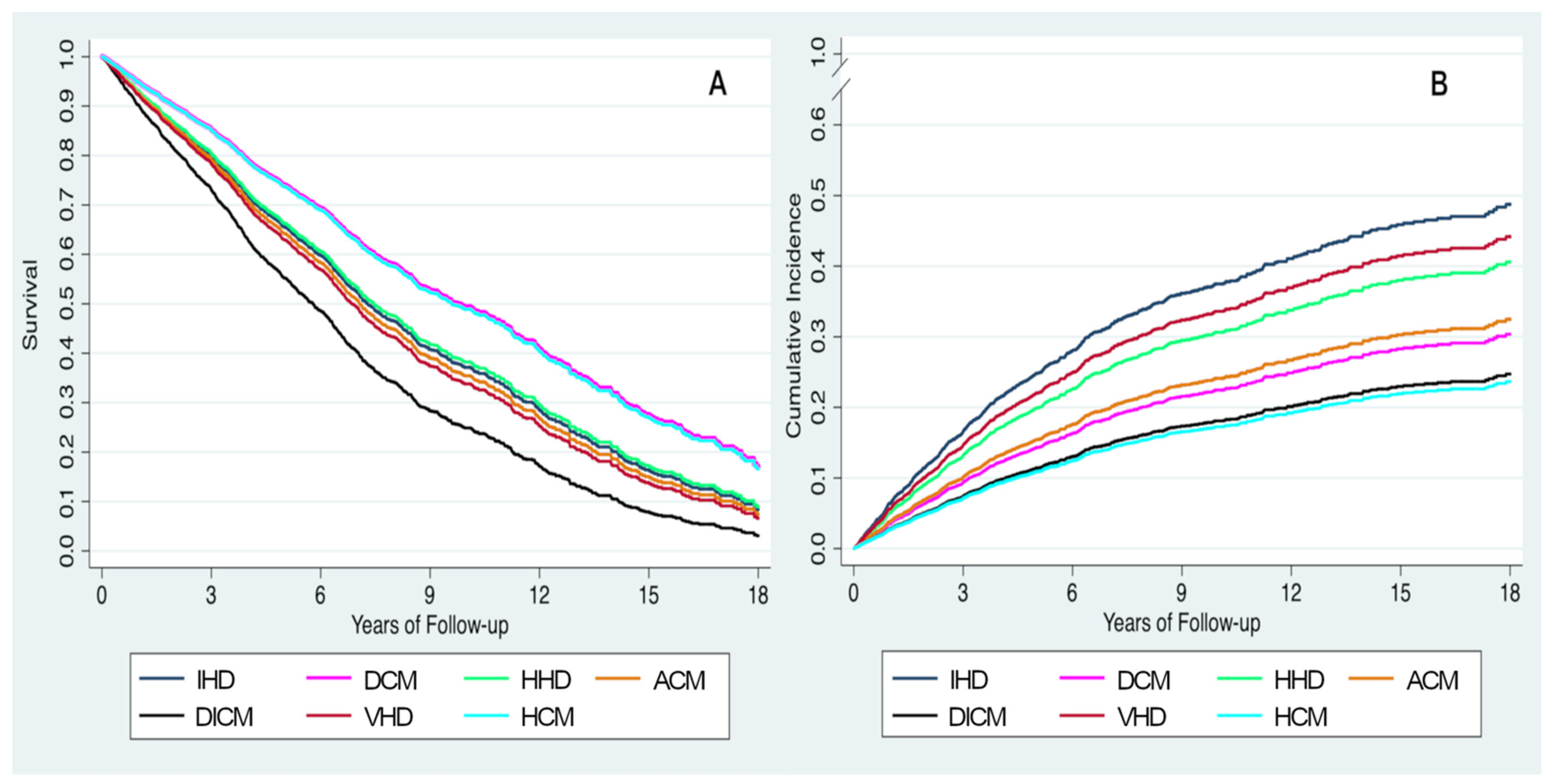
3.2. Association between HF Etiology and Mortality
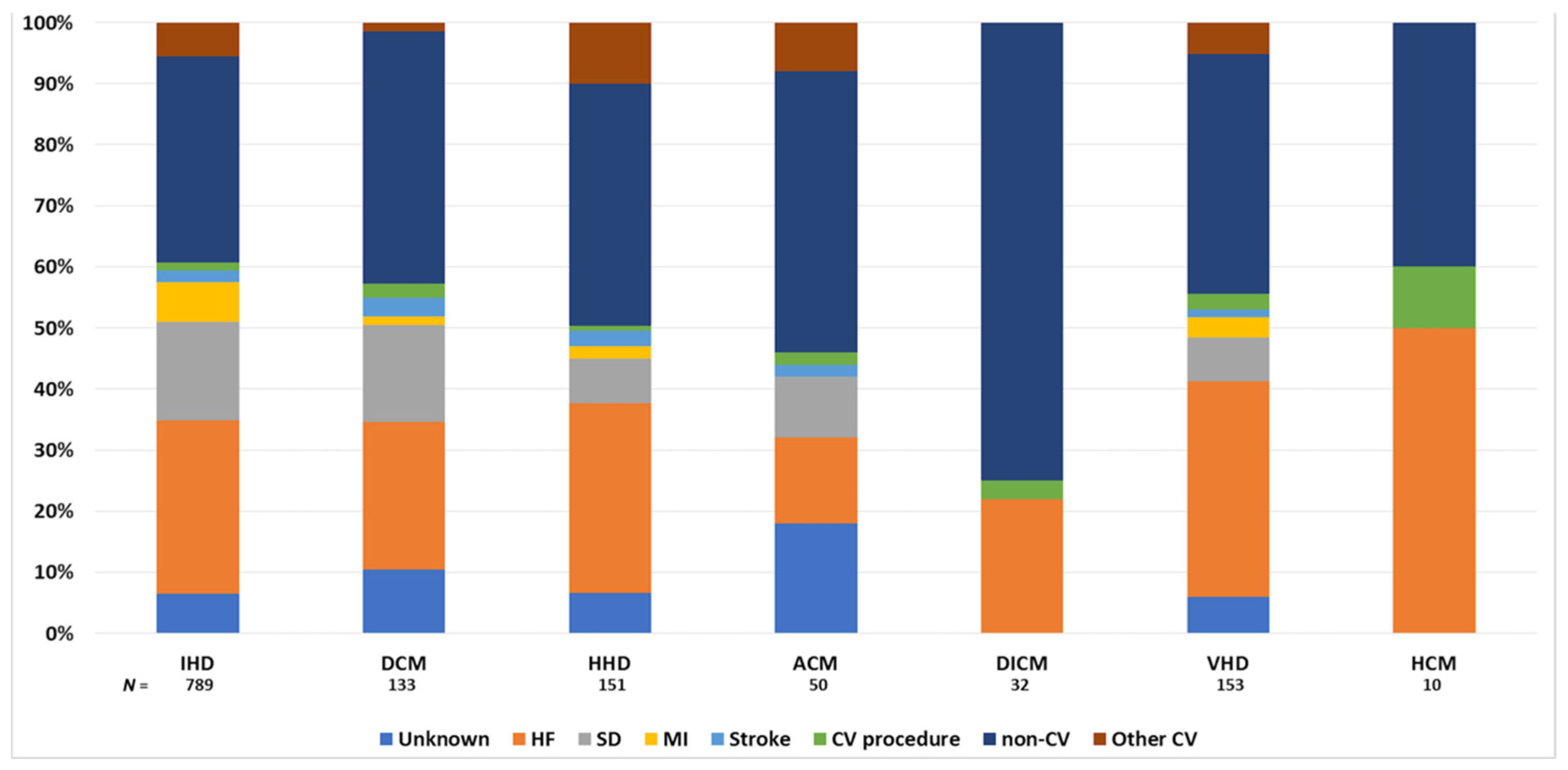
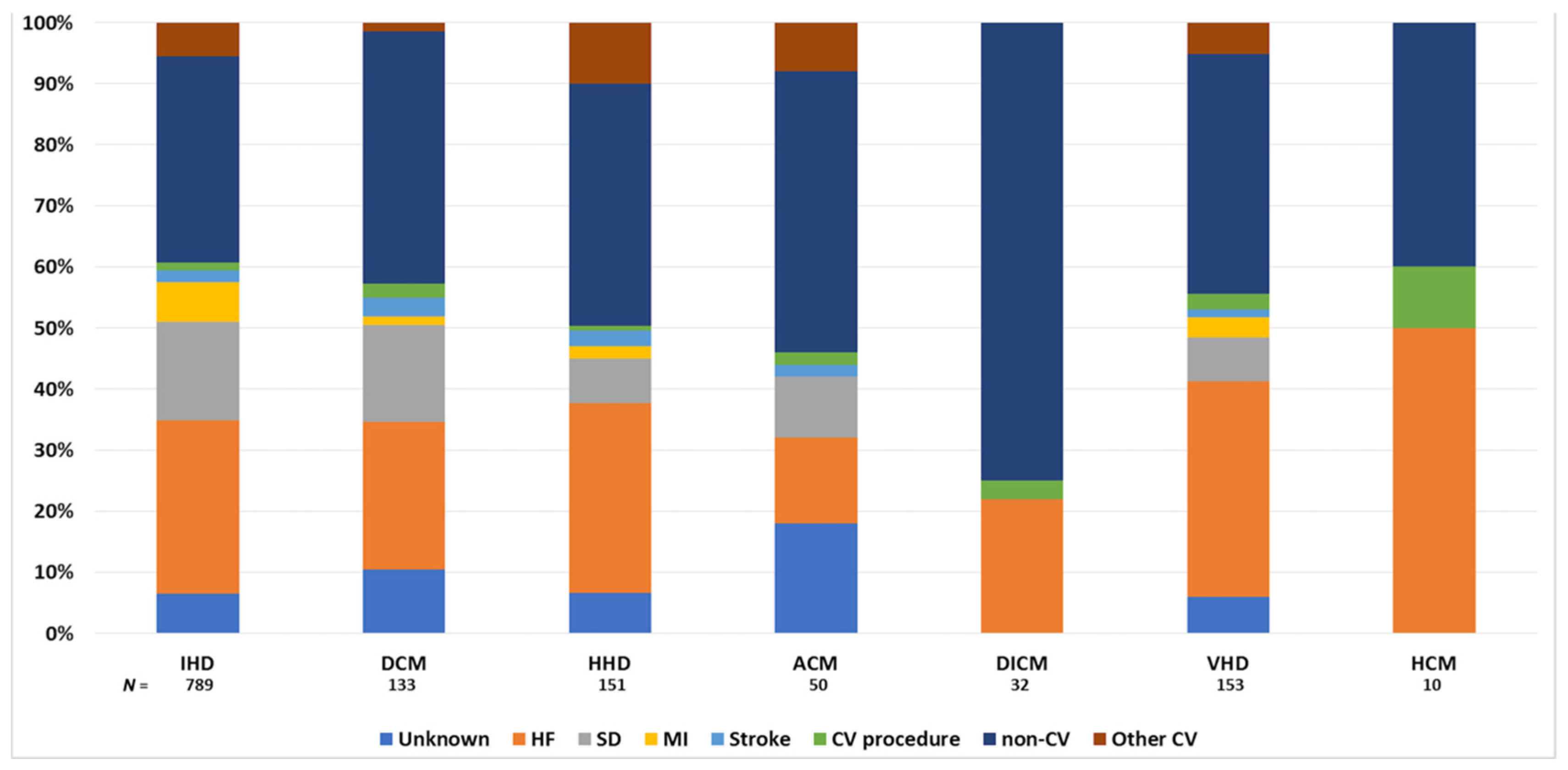
3.3. HF Etiology and Mode of Death
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garg, R.; Yusuf, S. Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity in patients with heart failure. Collaborative group on ACE inhibitor trials. JAMA 1995, 273, 1450–1456. [Google Scholar] [CrossRef] [PubMed]
- Cubbon, R.M.; Gale, C.P.; Kearney, L.C.; Schechter, C.B.; Brooksby, W.P.; Nolan, J.; Fox, K.A.; Rajwani, A.; Baig, W.; Groves, D.; et al. Changing characteristics and mode of death associated with chronic heart failure caused by left ventricular systolic dysfunction: A study across therapeutic eras. Circulation 2011, 4, 396–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spitaleri, G.; Lupón, J.; Domingo, M.; Santiago-Vacas, E.; Codina, P.; Zamora, E.; Cediel, G.; Santesmases, J.; Diez-Quevedo, C.; Troya, M.I.; et al. Mortality trends in an ambulatory multidisciplinary heart failure unit from 2001 to 2018. Sci. Rep. 2021, 11, 732. [Google Scholar] [CrossRef] [PubMed]
- Pocock, S.J.; Ariti, C.A.; McMurray, J.J.; Maggioni, A.; Køber, L.; Squire, I.B.; Swedberg, K.; Dobson, J.; Poppe, K.K.; Whalley, G.A.; et al. Predicting survival in heart failure: A risk score based on 39 372 patients from 30 studies. Eur. Heart J. 2013, 34, 1404–1413. [Google Scholar] [CrossRef]
- Likoff, M.J.; Chandler, S.L.; Kay, H.R. Clinical determinants of mortality in chronic congestive heart failure secondary to idiopathic dilated or to ischemic cardiomyopathy. Am. J. Cardiol. 1987, 59, 634–638. [Google Scholar] [CrossRef]
- Ho, K.K.; Anderson, K.M.; Kannel, W.B.; Grossman, W.; Levy, D. Survival after the onset of congestive heart failure in Framingham Heart Study subjects. Circulation 1993, 88, 107–115. [Google Scholar] [CrossRef] [Green Version]
- Adams, K.F., Jr.; Dunlap, S.H.; Sueta, C.A.; Clarke, S.W.; Patterson, J.H.; Blauwet, M.B.; Jensen, L.R.; Tomasko, L.; Koch, G. Relation between gender, etiology and survival in patients with symptomatic heart failure. J. Am. Coll. Cardiol. 1996, 28, 1781–1788. [Google Scholar] [CrossRef] [Green Version]
- Felker, G.M.; Thompson, R.E.; Hare, J.M.; Hruban, R.H.; Clemetson, D.E.; Howard, D.L.; Baughman, K.L.; Kasper, E.K. Underlying causes and long-term survival in patients with initially unexplained cardiomyopathy. N. Engl. J. Med. 2000, 342, 1077–1084. [Google Scholar] [CrossRef]
- Pecini, R.; Møller, D.V.; Torp-Pedersen, C.; Hassager, C.; Køber, L. Heart failure etiology impacts survival of patients with heart failure. Int. J. Cardiol. 2011, 149, 211–215. [Google Scholar] [CrossRef]
- Zamora, E.; Lupón, J.; Vila, J.; Urrutia, A.; de Antonio, M.; Sanz, H.; Grau, M.; Ara, J.; Bayés-Genís, A. Estimated glomerular filtration rate and prognosis in heart failure: Value of the Modification of Diet in Renal Disease Study-4, chronic kidney disease epidemiology collaboration, and cockroft-gault formulas. J. Am. Coll. Cardiol. 2012, 59, 1709–1715. [Google Scholar] [CrossRef] [Green Version]
- Lupón, J.; Gavidia-Bovadilla, G.; Ferrer, E.; de Antonio, M.; Perera-Lluna, A.; López-Ayerbe, J.; Domingo, M.; Núñez, J.; Zamora, E.; Moliner, P.; et al. Dynamic Trajectories of Left Ventricular Ejection Fraction in Heart Failure. J. Am. Coll. Cardiol. 2018, 72, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Pons, F.; Lupón, J.; Urrutia, A.; González, B.; Crespo, E.; Díez, C.; Cano, L.; Cabanes, R.; Altimir, S.; Coll, R.; et al. Mortality and cause of death in patients with heart failure: Findings at a specialist multidisciplinary heart failure unit. Rev. Esp. Cardiol. 2010, 63, 303–314. [Google Scholar] [CrossRef]
- Seidman, A.; Hudis, C.; Pierri, M.K.; Shak, S.; Paton, V.; Ashby, M.; Murphy, M.; Stewart, S.J.; Keefe, D. Cardiac dysfunction in the trastuzumab clinical trials experience. J. Clin. Oncol. 2002, 20, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Authors/Task Force Members; Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [Green Version]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner-La Rocca, H.P.; Choi, D.J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef] [PubMed]
- van Veldhuisen, D.J.; Ruilope, L.M.; Maisel, A.S.; Damman, K. Biomarkers of renal injury and function: Diagnostic, prognostic and therapeutic implications in heart failure. Eur. Heart J. 2016, 37, 2577–2585. [Google Scholar] [CrossRef] [Green Version]
- Chioncel, O.; Lainscak, M.; Seferovic, P.M.; Anker, S.D.; Crespo-Leiro, M.G.; Harjola, V.P.; Parissis, J.; Laroche, C.; Piepoli, M.F.; Fonseca, C.; et al. Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: An analysis of the ESC Heart Failure Long-Term Registry. Eur. J. Heart Fail. 2017, 19, 1574–1585. [Google Scholar] [CrossRef]
- Nadruz, W., Jr.; West, E.; Sengeløv, M.; Grove, G.L.; Santos, M.; Groarke, J.D.; Forman, D.E.; Claggett, B.; Skali, H.; Nohria, A.; et al. Cardiovascular phenotype and prognosis of patients with heart failure induced by cancer therapy. Heart 2019, 105, 34–41. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Muñoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2017, 19, 9–42. [Google Scholar] [CrossRef] [PubMed]
- Mirijello, A.; Tarli, C.; Vassallo, G.A.; Sestito, L.; Antonelli, M.; d’Angelo, C.; Ferrulli, A.; De Cosmo, S.; Gasbarrini, A.; Addolorato, G. Alcoholic cardiomyopathy: What is known and what is not known. Eur. J. Intern. Med. 2017, 43, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Xi, B.; Veeranki, S.P.; Zhao, M.; Ma, C.; Yan, Y.; Mi, J. Relationship of Alcohol Consumption to All-Cause, Cardiovascular, and Cancer-Related Mortality in U.S. Adults. J. Am. Coll. Cardiol. 2017, 70, 913–922. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J. Clinical Course and Management of Hypertrophic Cardiomyopathy. N. Engl. J. Med. 2018, 379, 1977. [Google Scholar] [CrossRef]
- Maron, B.J.; Rowin, E.J.; Casey, S.A.; Garberich, R.F.; Maron, M.S. What Do Patients With Hypertrophic Cardiomyopathy Die from? Am. J. Cardiol. 2016, 117, 434–435. [Google Scholar] [CrossRef] [Green Version]
- Guzzo-Merello, G.; Segovia, J.; Dominguez, F.; Cobo-Marcos, M.; Gomez-Bueno, M.; Avellana, P.; Millan, I.; Alonso-Pulpon, L.; Garcia-Pavia, P. Natural history and prognostic factors in alcoholic cardiomyopathy. JACC Heart Fail. 2015, 3, 78–86. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Total Cohort (n = 2387) | IHD (n = 1222) | DCM (n = 415) | HHD (n = 231) | ACM (n = 120) | DICM (n = 73) | VHD (n = 237) | HCM (n = 89) | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| Age, years | 67 ± 13 | 68 ± 11 | 62 ± 14 | 71 ± 13 | 57 ± 10 | 59 ± 12 | 71 ± 11 | 58 ± 15 | <0.001 |
| Male | 1702 (71.3) | 969 (79.3) | 300 (72.3) | 119 (51.5) | 113 (94.2) | 18 (24.7) | 117 (49.4) | 66 (74.2) | <0.001 |
| White | 2309 (96.7) | 1187 (97.1) | 392 (94.5) | 226 (97.8) | 117 (97.5) | 71 (97.3) | 23 3(98.3) | 83 (93.3) | 0.03 |
| HF duration, months | 8 (2–48) | 7 (1–42) | 6 (2–36) | 11 (2–48) | 5 (2–36) | 2 (1–14) | 24 (4–42) | 24 (4–118) | <0.001 |
| NYHA class III/IV | 659 (27.6) | 345 (28.2) | 82 (19.8) | 84 (36.4) | 15 (12.5) | 21 (28.8) | 99 (41.8) | 13 (14.6) | <0.001 |
| LVEF, % | 35.4 ± 14.2 | 32.59 ± 10.4 | 30.2 ± 10.7 | 44.4 ± 17.0 | 26.7 ± 10.1 | 33.9 ± 12.6 | 44.6 ± 16.0 | 64.9 ± 11.2 | <0.001 |
| Diabetes | 1040 (43.6) | 652 (53.4) | 140 (33.7) | 105 (45.5) | 26 (21.7) | 19 (26.0) | 83 (35.0) | 15 (16.9) | <0.001 |
| Hypertension | 1533 (64.2) | 821 (67.2) | 215 (51.8) | 225 (97.4) | 51 (42.5) | 25 (34.2) | 156 (65.8) | 40 (44.9) | <0.001 |
| COPD | 408 (17.1) | 218 (17.8) | 70 (16.9) | 41 (17.7) | 30 (25.0) | 2 (2.7) | 43 (18.1) | 4 (4.5) | <0.001 |
| PVD | 356 (14.9) | 255 (20.9) | 39 (9.4) | 29 (12.6) | 11 (9.2) | 1 (1.4) | 19 (8.0) | 2 (2.2) | <0.001 |
| Anaemia 1 | 1072 (45.0) | 657 (53.9) | 104 (25.1) | 113 (48.9) | 30 (25.0) | 25 (34.2) | 129 (54.4) | 14 (15.9) | <0.001 |
| Renal insufficiency 2 | 1051 (44.0) | 587 (48.0) | 138 (33.3) | 144 (62.3) | 21 (17.5) | 26 (35.6) | 121 (51.1) | 14 (15.7) | <0.001 |
| Atrial fibrillation or flutter | 518 (21.7) | 173 (14.2) | 83 (20.0) | 82 (35.5) | 28 (23.3) | 6 (8.2) | 130 (54.9) | 16 (18.0) | <0.001 |
| BMI, kg/m2 (n = 2350) | 27 (24–30) | 27 (24–30) | 27 (24–30) | 29 (36–34) | 26 (23–30) | 26 (23–30) | 26 (23–30) | 27 (25–30) | <0.001 |
| NT-proBNP, ng/L (n = 1712) | 1703 (730–4061) | 2193 (967–4978) | 1118 (517–2470) | 1772 (785–4117) | 1075 (502–2799) | 1409 (544–3491) | 2129 (912–4460) | 863 (307–1739) | <0.001 |
| Treatment (during follow-up) | |||||||||
| ACEI/ARB/ARNI | 2052 (86.0) | 1070 (87.6) | 393 (94.7) | 180 (77.9) | 116 (96.7) | 69 (94.5) | 182 (76.8) | 42 (47.2) | <0.001 |
| Beta-blocker | 2137 (89.5) | 1136 (93.0) | 380 (91.6) | 184 (79.7) | 113 (94.2) | 68 (93.2) | 182 (76.8) | 74 (83.1) | <0.001 |
| MRA | 1581 (66.2) | 808 (66.1) | 316 (76.1) | 133 (57.6) | 92 (76.7) | 49 (67.1) | 164 (69.2) | 19 (21.3) | <0.001 |
| Loop diuretic | 2154 (90.2) | 1122 (91.8) | 365 (88.0) | 224 (97.0) | 116 (96.7) | 58 (79.5) | 227 (95.8) | 42 (47.2) | <0.001 |
| Digoxin | 889 (37.2) | 398 (32.6) | 162 (39.0) | 96 (41.6) | 68 (56.7) | 22 (30.1) | 137 (57.8) | 6 (6.7) | <0.001 |
| Ivabradine | 524 (22.0) | 271 (22.2) | 130 (31.3) | 32 (13.9) | 35 (29.2) | 32 (43.8) | 21 (8.9) | 3 (3.4) | <0.001 |
| CRT | 267 (11.2) | 126 (10.3) | 79 (19.0) | 17 (7.4) | 11 (9.2) | 6 (8.2) | 26 (11.0) | 2 (2.2) | <0.001 |
| ICD | 369 (15.5) | 237 (19.4) | 71 (17.1) | 9 (3.9) | 14 (11.7) | 4 (5.5) | 19 (8.0) | 15 (16.9) | <0.001 |
| Unadjusted Analysis | Adjusted Analysis * | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All-Cause Death | Cardiovascular Death † | All-Cause Death | Cardiovascular Death † | |||||||||
| HR | 95%CI | p-Value | HR | 95%CI | p-Value | HR | 95%CI | p-value | HR | 95%CI | p-Value | |
| IHD | 1 | 1 | 1 | 1 | ||||||||
| DCM | 0.48 | 0.40–0.57 | <0.001 | 0.40 | 0.31–0.53 | <0.001 | 0.68 | 0.56–0.83 | <0.001 | 0.54 | 0.42–0.70 | <0.001 |
| HHD | 1.03 | 0.87–1.23 | 0.72 | 0.86 | 0.68–1–08 | 0.21 | 0.96 | 0.80–1.16 | 0.68 | 0.78 | 0.61–1.00 | 0.05 |
| ACM | 0.49 | 0.37–0.65 | <0.001 | 0.33 | 0.21–0.52 | <0.001 | 0.93 | 0.67–1.28 | 0.65 | 0.59 | 0.37–0.94 | 0.03 |
| DICM | 0.73 | 0.51–1.04 | 0.08 | 0.27 | 0.14–0.52 | <0.001 | 1.47 | 1.02–2.11 | 0.04 | 0.42 | 0.22–0.83 | 0.01 |
| VHD | 1.20 | 1.01–1.42 | 0.04 | 0.97 | 0.76–1.23 | 0.79 | 1.08 | 0.89–1.30 | 0.44 | 0.87 | 0.68–1.12 | 0.29 |
| HCM | 0.27 | 0.14–0.50 | <0.001 | 0.26 | 0.12–0.57 | <0.001 | 0.75 | 0.40–1.41 | 0.37 | 0.40 | 0.18–0.90 | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spitaleri, G.; Zamora, E.; Cediel, G.; Codina, P.; Santiago-Vacas, E.; Domingo, M.; Lupón, J.; Santesmases, J.; Diez-Quevedo, C.; Troya, M.I.; et al. Cause of Death in Heart Failure Based on Etiology: Long-Term Cohort Study of All-Cause and Cardiovascular Mortality. J. Clin. Med. 2022, 11, 784. https://doi.org/10.3390/jcm11030784
Spitaleri G, Zamora E, Cediel G, Codina P, Santiago-Vacas E, Domingo M, Lupón J, Santesmases J, Diez-Quevedo C, Troya MI, et al. Cause of Death in Heart Failure Based on Etiology: Long-Term Cohort Study of All-Cause and Cardiovascular Mortality. Journal of Clinical Medicine. 2022; 11(3):784. https://doi.org/10.3390/jcm11030784
Chicago/Turabian StyleSpitaleri, Giosafat, Elisabet Zamora, German Cediel, Pau Codina, Evelyn Santiago-Vacas, Mar Domingo, Josep Lupón, Javier Santesmases, Crisanto Diez-Quevedo, Maria Isabel Troya, and et al. 2022. "Cause of Death in Heart Failure Based on Etiology: Long-Term Cohort Study of All-Cause and Cardiovascular Mortality" Journal of Clinical Medicine 11, no. 3: 784. https://doi.org/10.3390/jcm11030784
APA StyleSpitaleri, G., Zamora, E., Cediel, G., Codina, P., Santiago-Vacas, E., Domingo, M., Lupón, J., Santesmases, J., Diez-Quevedo, C., Troya, M. I., Boldo, M., Altimir, S., Alonso, N., González, B., & Bayes-Genis, A. (2022). Cause of Death in Heart Failure Based on Etiology: Long-Term Cohort Study of All-Cause and Cardiovascular Mortality. Journal of Clinical Medicine, 11(3), 784. https://doi.org/10.3390/jcm11030784