
Long-Term Follow-Up of Fractional CO2 Laser Therapy for Genitourinary Syndrome of Menopause in Breast Cancer Survivors

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Eligibility
2.2. Procedures
2.3. Measures
3. Results
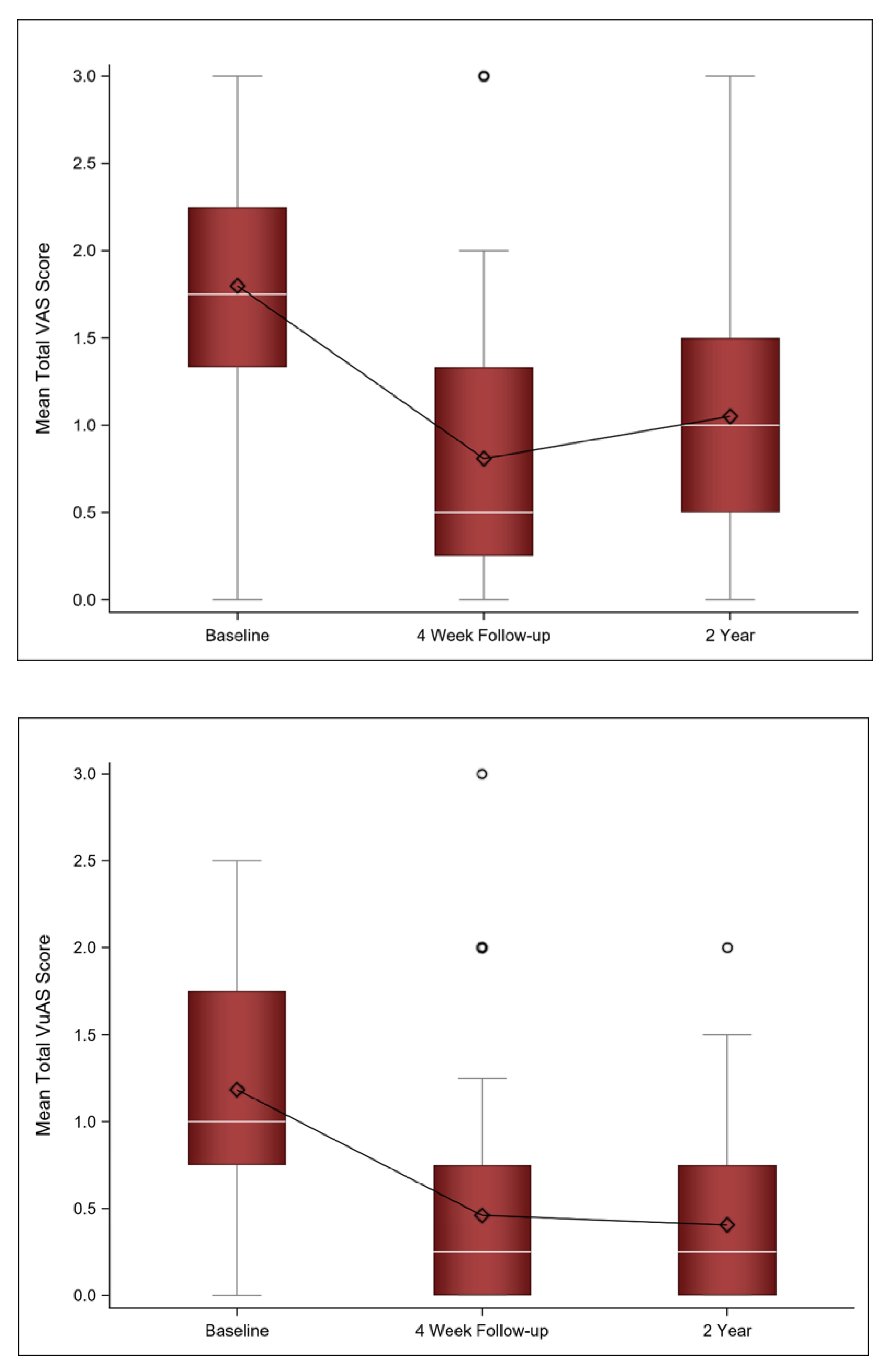
3.1. VAS/VuAS
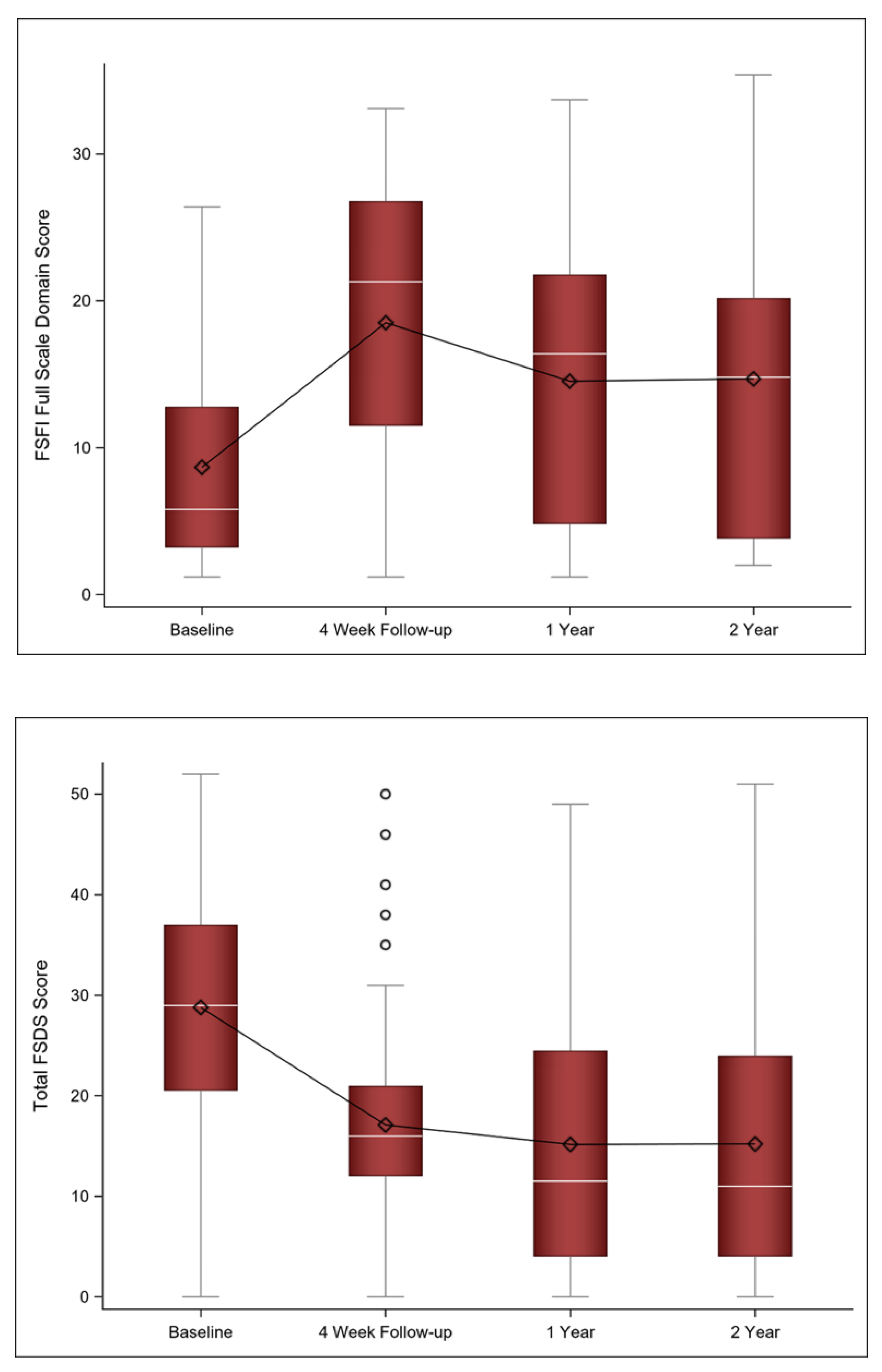
3.2. Sexual Function
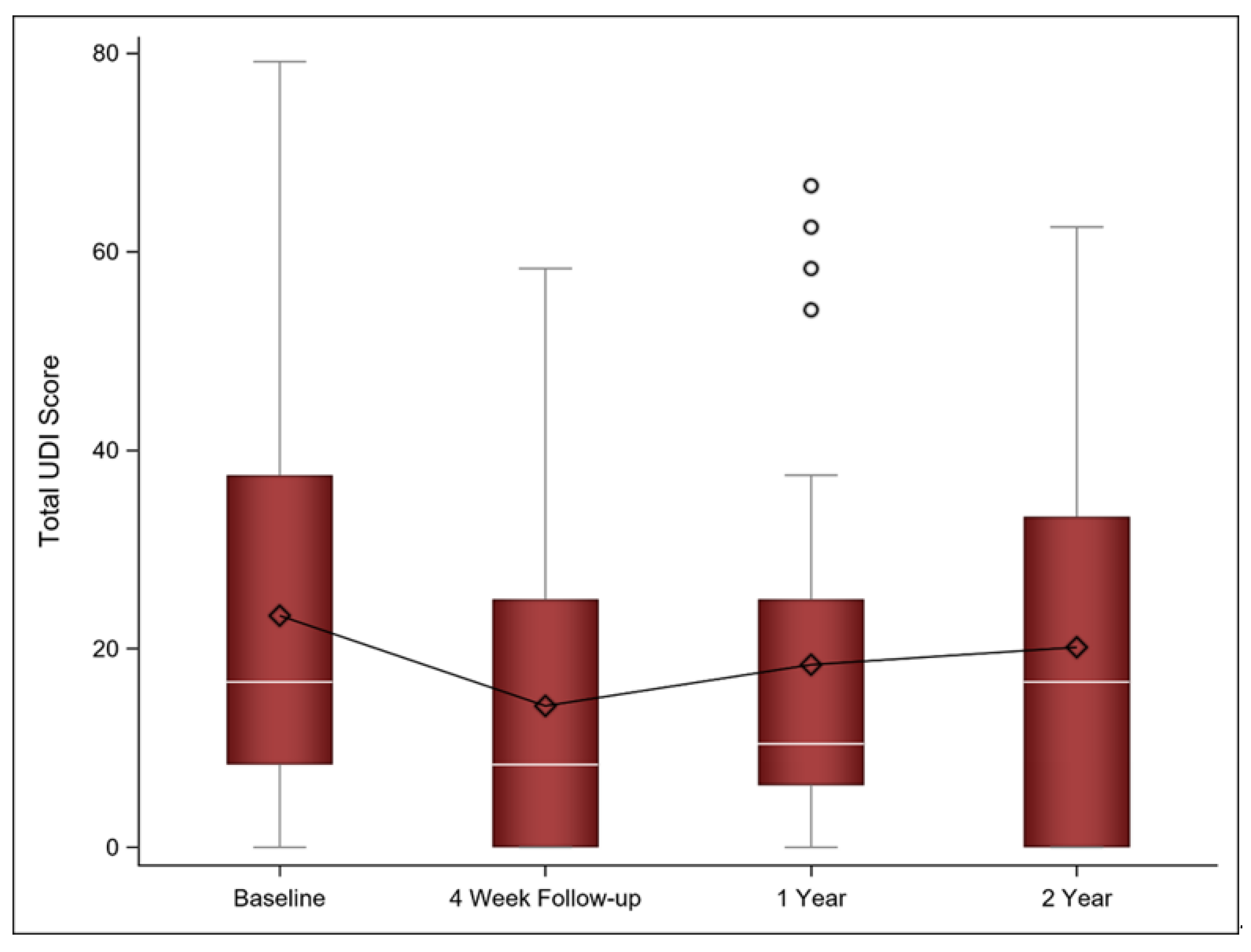
3.3. Urinary Symptoms
3.4. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Falk, S.J.; Bober, S. Vaginal health during breast cancer treatment. Curr. Oncol. Rep. 2016, 18, 32. [Google Scholar] [CrossRef] [PubMed]
- Faubion, S.S.; Sood, R.; Kapoor, E. Genitourinary syndrome of menopause: Management strategies for the clinician. Mayo Clin. Proc. 2017, 92, 1842–1849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, N.A.; Bachmann, G.A. The genitourinary syndrome of menopause. Menopause 2021, 28, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Melisko, M.E.; Goldman, M.E.; Hwang, J.; De Luca, A.; Fang, S.; Esserman, L.J.; Chien, A.J.; Park, J.W.; Rugo, H.S. Vaginal testosterone cream vs estradiol vaginal ring for vaginal dryness or decreased libido in women receiving aromatase inhibitors for early-stage breast cancer. JAMA Oncol. 2017, 3, 313–319. [Google Scholar] [CrossRef]
- Schover, L.R.; Baum, G.P.; Fuson, L.A.; Brewster, A.; Melhem-Bertrandt, A. sexual problems during the first 2 years of adjuvant treatment with aromatase inhibitors. J. Sex. Med. 2014, 11, 3102–3111. [Google Scholar] [CrossRef] [Green Version]
- Faubion, S.S.; Larkin, L.C.; Stuenkel, C.A.; Bachmann, G.A.; Chism, L.A.; Kagan, R.; Kaunitz, A.M.; Krychman, M.L.; Parish, S.J.; Partridge, A.H.; et al. Management of genitourinary syndrome of menopause in women with or at high risk for breast cancer: Consensus recommendations from The North American Menopause Society and The International Society for the Study of Women’s Sexual Health. Menopause 2018, 25, 596–608. [Google Scholar] [CrossRef]
- Perino, A.; Calligaro, A.; Forlani, F.; Tiberio, C.; Cucinella, G.; Svelato, A.; Saitta, S.; Calagna, G. Vulvo-vaginal atrophy: A new treatment modality using thermo-ablative fractional CO2 laser. Maturitas 2015, 80, 296–301. [Google Scholar] [CrossRef]
- Sokol, E.R.; Karram, M.M. An assessment of the safety and efficacy of a fractional CO2 laser system for the treatment of vulvovaginal atrophy. Menopause 2016, 23, 1102–1107. [Google Scholar] [CrossRef]
- Pitsouni, E.; Grigoriadis, T.; Tsiveleka, A.; Zacharakis, D.; Salvatore, S.; Athanasiou, S. Microablative fractional CO2 -laser therapy and the genitourinary syndrome of menopause: An observational study. Maturitas 2016, 94, 131–136. [Google Scholar] [CrossRef]
- Salvatore, S.; Nappi, R.E.; Zerbinati, N.; Calligaro, A.; Ferrero, S.; Origoni, M.; Candiani, M.; Maggiore, U.L.R. A 12-week treatment with fractional CO2 laser for vulvovaginal atrophy: A pilot study. Climacteric 2014, 17, 363–369. [Google Scholar] [CrossRef]
- Athanasiou, S.; Pitsouni, E.; Grigoriadis, T.; Zacharakis, D.; Falagas, M.E.; Salvatore, S.; Protopapas, A.; Loutradis, D. Microablative fractional CO2 laser for the genitourinary syndrome of menopause: Up to 12-month results. Menopause 2019, 26, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Behnia-Willison, F.; Sarraf, S.; Miller, J.; Mohamadi, B.; Care, A.; Lam, A.; Willison, N.; Behnia, L.; Salvatore, S. Safety and long-term efficacy of fractional CO2 laser treatment in women suffering from genitourinary syndrome of menopause. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 213, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Paraiso, M.F.R.; Ferrando, C.A.; Sokol, E.R.; Rardin, C.R.; Matthews, C.A.; Karram, M.M.; Iglesia, C.B. A randomized clinical trial comparing vaginal laser therapy to vaginal estrogen therapy in women with genitourinary syndrome of menopause: The VeLVET Trial. Menopause 2020, 27, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Dutra, P.F.S.P.; Heinke, T.; Pinho, S.C.; Focchi, G.R.A.; Tso, F.K.; de Almeida, B.C.; Silva, I.; Speck, N.M.G. Comparison of topical fractional CO2 laser and vaginal estrogen for the treatment of genitourinary syndrome in postmenopausal women. Menopause 2021, 28, 756–763. [Google Scholar] [CrossRef]
- Cruz, V.L.; Steiner, M.L.; Pompei, L.M.; Strufaldi, R.; Fonseca, F.L.A.; Santiago, L.H.S.; Wajsfeld, T.; Fernandes, C.E. Randomized, double-blind, placebo-controlled clinical trial for evaluating the efficacy of fractional CO2 laser compared with topical estriol in the treatment of vaginal atrophy in postmenopausal women. Menopause 2018, 25, 21–28. [Google Scholar] [CrossRef]
- Li, J.; Li, H.; Zhou, Y.; Xie, M.; Miao, Y.; Wang, L.; Zhao, Y.; Ying, T.; Hu, Y.; Chen, Y.; et al. The Fractional CO2 laser for the treatment of genitourinary syndrome of menopause: A prospective multicenter cohort study. Lasers Surg. Med. 2020, 53, 647–653. [Google Scholar] [CrossRef]
- Stefano, S.; Stavros, A.; Massimo, C. The use of pulsed CO2 lasers for the treatment of vulvovaginal atrophy. Curr. Opin. Obstet. Gynecol. 2015, 27, 504–508. [Google Scholar] [CrossRef]
- Sokol, E.R.; Karram, M.M. Use of a novel fractional CO2 laser for the treatment of genitourinary syndrome of menopause: 1-year outcomes. Menopause 2017, 24, 810–814. [Google Scholar] [CrossRef]
- Salvatore, S.; Pitsouni, E.; Grigoriadis, T.; Zacharakis, D.; Pantaleo, G.; Candiani, M.; Athanasiou, S. CO2 laser and the genitourinary syndrome of menopause: A randomized sham-controlled trial. Climacteric J. Internat. Menopause Soc. 2021, 24, 187–193. [Google Scholar] [CrossRef]
- Ruanphoo, P.; Bunyavejchevin, S. Treatment for vaginal atrophy using microablative fractional CO2 laser: A randomized double-blinded sham-controlled trial. Menopause 2020, 27, 858–863. [Google Scholar] [CrossRef]
- Gittens, P.; Mullen, G. The effects of fractional microablative CO2 laser therapy on sexual function in postmenopausal women and women with a history of breast cancer treated with endocrine therapy. J. Cosmet. Laser Ther. 2019, 21, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Pagano, T.; De Rosa, P.; Vallone, R.; Schettini, F.; Arpino, G.; De Placido, S.; Nazzaro, G.; Locci, M.; De Placido, G. Fractional microablative CO2 laser for vulvovaginal atrophy in women treated with chemotherapy and/or hormonal therapy for breast cancer: A retrospective study. Menopause 2016, 23, 1108–1113. [Google Scholar] [CrossRef] [PubMed]
- Pagano, T.; De Rosa, P.; Vallone, R.; Schettini, F.; Arpino, G.; Giuliano, M.; Lauria, R.; De Santo, I.; Conforti, A.; Gallo, A.; et al. Fractional microablative CO2 laser in breast cancer survivors affected by iatrogenic vulvovaginal atrophy after failure of nonestrogenic local treatments: A retrospective study. Menopause 2017, 25, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Pearson, A.; Booker, A.; Tio, M.; Marx, G. Vaginal CO2 laser for the treatment of vulvovaginal atrophy in women with breast cancer: LAAVA pilot study. Breast Cancer Res. Treat. 2019, 178, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Quick, A.M.; Zvinovski, F.; Hudson, C.; Hundley, A.; Evans, C.; Suresh, A.; Stephens, J.A.; Arthur, E.; Ramaswamy, B.; Reinbolt, R.E.; et al. Fractional CO2 laser therapy for genitourinary syndrome of menopause for breast cancer survivors. Support. Care Cancer 2020, 28, 3669–3677. [Google Scholar] [CrossRef] [PubMed]
- Quick, A.M.; Zvinovski, F.; Hudson, C.; Hundley, A.; Evans, C.; Stephens, J.A.; Arthur, E.; Ramaswamy, B.; Reinbolt, R.E.; Noonan, A.M.; et al. Patient-reported sexual function of breast cancer survivors with genitourinary syndrome of menopause after fractional CO2 laser therapy. Menopause 2021, 28, 642–649. [Google Scholar] [CrossRef]
- Pieralli, A.; Fallani, M.G.; Becorpi, A.; Bianchi, C.; Corioni, S.; Longinotti, M.; Tredici, Z.; Guaschino, S. Fractional CO2 laser for vulvovaginal atrophy (VVA) dyspareunia relief in breast cancer survivors. Arch. Gynecol. Obstet. 2016, 294, 841–846. [Google Scholar] [CrossRef]
- Veron, L.; Wehrer, D.; Annerose-Zéphir, G.; Suciu, V.; Delaloge, S.; Pistilli, B.; Chaltiel, D.; Pautier, P. Effects of local laser treatment on vulvovaginal atrophy among women with breast cancer: A prospective study with long-term follow-up. Breast Cancer Res. Treat. 2021, 1–9. [Google Scholar] [CrossRef]
- Carter, J.; Stabile, C.; Seidel, B.; Baser, R.E.; Goldfarb, S.; Goldfrank, D.J. Vaginal and sexual health treatment strategies within a female sexual medicine program for cancer patients and survivors. J. Cancer Surviv. Res. Pract. 2017, 11, 274–283. [Google Scholar] [CrossRef] [Green Version]
- Eaton, A.A.; Baser, R.E.; Seidel, B.; Stabile, C.; Canty, J.P.; Goldfrank, D.J.; Carter, J. Validation of clinical tools for vaginal and vulvar symptom assessment in cancer patients and survivors. J. Sex. Med. 2017, 14, 144–151. [Google Scholar] [CrossRef] [Green Version]
- Bartula, I.; Sherman, K.A. The female sexual functioning index (FSFI): Evaluation of acceptability, reliability, and validity in women with breast cancer. Support. Care Cancer 2015, 23, 2633–2641. [Google Scholar] [CrossRef] [PubMed]
- Rosen, R.; Brown, C.; Heiman, J.; Leiblum, S.; Meston, C.; Shabsigh, R.; Ferguson, D.; D’Agostino, R., Jr. The female sexual function index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J. Sex. Marital Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef] [PubMed]
- DeRogatis, L.; Clayton, A.; Lewis-D’Agostino, D.; Wunderlich, G.; Fu, Y. Validation of the female sexual distress scale-revised for assessing distress in women with hypoactive sexual desire disorder. J. Sex. Med. 2008, 5, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R.; Rosen, R.; Leiblum, S.; Burnett, A.; Heiman, J. The female sexual distress scale (FSDS): Initial validation of a standardized scale for assessment of sexually related personal distress in women. J. Sex Marital Ther. 2002, 28, 317–330. [Google Scholar] [CrossRef]
- Uebersax, J.S.; Wyman, J.F.; Shumaker, S.A.; McClish, D.K.; Fantl, J.A. Short forms to assess life quality and symptom distress for urinary incontinence in women: The incontinence impact questionnaire and the urogenital distress inventory. Continence Program for Women Research Group. Neurourol. Urodyn. 1995, 14, 131–139. [Google Scholar] [CrossRef]
- Raggio, G.A.; Butryn, M.L.; Arigo, D.; Mikorski, R.; Palmer, S.C. Prevalence and correlates of sexual morbidity in long-term breast cancer survivors. Psychol. Health 2014, 29, 632–650. [Google Scholar] [CrossRef]
- Oberguggenberger, A.; Martini, C.; Huber, N.; Fallowfield, L.; Hubalek, M.; Daniaux, M.; Sperner-Unterweger, B.; Holzner, B.; Sztankay, M.; Gamper, E.; et al. Self-reported sexual health: Breast cancer survivors compared to women from the general population—An observational study. BMC Cancer 2017, 17, 599. [Google Scholar] [CrossRef]
- Hershman, D.L.; Shao, T.; Kushi, L.H.; Buono, D.; Tsai, W.Y.; Fehrenbacher, L.; Kwan, M.; Gomez, S.L.; Neugut, A.I. Early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer. Breast Cancer Res. Treat. 2011, 126, 529–537. [Google Scholar] [CrossRef] [Green Version]
- Farrell, R. ACOG Committee Opinion No. 659: The use of vaginal estrogen in women with a history of estrogen-dependent breast cancer. Obstet. Gynecol. 2016, 127, e93–e96. [Google Scholar] [CrossRef]
- Hirschberg, A.L.; Bitzer, J.; Cano, A.; Ceausu, I.; Chedraui, P.; Durmusoglu, F.; Erkkola, R.; Goulis, D.G.; Kiesel, L.; Lopes, P.; et al. Topical estrogens and non-hormonal preparations for postmenopausal vulvovaginal atrophy: An EMAS clinical guide. Maturitas 2021, 148, 55–61. [Google Scholar] [CrossRef]
- NAMS Position Statement. The 2020 genitourinary syndrome of menopause position statement of The North American Menopause Society. Menopause 2020, 27, 976–992. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.; André, F.; Barrios, C.; Bergh, J.; Bhattacharyya, G.; Biganzoli, L.; et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.L.; Jamy, O.; Mullins, J.; Usman, R.M.; Hare, F.; Valasareddy, P.; Chaudhry, A.; Ryder, J.; Smith, J.R.; Miller, E.; et al. Usefulness of patient-reported outcomes to assess the effectiveness of topical hormonal therapy for gynecologic symptoms symptoms after antihormonal treatment for breast cancer. Bayl. Univ. Med Cent. Proc. 2020, 33, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Pitsouni, E.; Grigoriadis, T.; Falagas, M.E.; Salvatore, S.; Athanasiou, S. Laser therapy for the genitourinary syndrome of menopause. A systematic review and meta-analysis. Maturitas 2017, 103, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Filippini, M.; Luvero, D.; Salvatore, S.; Pieralli, A.; Montera, R.; Plotti, F.; Candiani, M.; Angioli, R. Efficacy of fractional CO2 laser treatment in postmenopausal women with genitourinary syndrome: A multicenter study. Menopause 2020, 27, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Gambacciani, M.; Levancini, M. Vaginal erbium laser as second-generation thermotherapy for the genitourinary syndrome of menopause: A pilot study in breast cancer survivors. Menopause 2017, 24, 316–319. [Google Scholar] [CrossRef] [PubMed]
- Mothes, A.R.; Runnebaum, M.; Runnebaum, I.B. Ablative dual-phase Erbium:YAG laser treatment of atrophy-related vaginal symptoms in post-menopausal breast cancer survivors omitting hormonal treatment. J. Cancer Res. Clin. Oncol. 2018, 144, 955–960. [Google Scholar] [CrossRef]
- Vicariotto, F.; Raichi, M. Technological evolution in the radiofrequency treatment of vaginal laxity and menopausal vulvo-vaginal atrophy and other genitourinary symptoms: First experiences with a novel dynamic quadripolar device. Minerva Ginecol. 2016, 68, 225–236. [Google Scholar]
- Cruff, J.; Khandwala, S. A double-blind randomized sham-controlled trial to evaluate the efficacy of fractional carbon dioxide laser therapy on genitourinary syndrome of menopause. J. Sex. Med. 2021, 18, 761–769. [Google Scholar] [CrossRef]
- Li, F.; Picard-Fortin, V.; Maheux-Lacroix, S.; Deans, R.; Nesbitt-Hawes, E.; McCormack, L.; Abbott, P.J. The efficacy of vaginal laser and other energy-based treatments on genital symptoms in postmenopausal women: A systematic review and meta-analysis. J. Minim. Invasive Gynecol. 2021, 28, 668–683. [Google Scholar] [CrossRef]
- Quick, A.M.; Dockter, T.; Le-Rademacher, J.; Salani, R.; Hudson, C.; Hundley, A.; Terstriep, S.; Streicher, L.; Faubion, S.; Loprinzi, C.L.; et al. Pilot study of fractional CO2 laser therapy for genitourinary syndrome of menopause in gynecologic cancer survivors. Maturitas 2021, 144, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, S.; Nappi, R.E.; Casiraghi, A.; Ruffolo, A.F.; Degliuomini, R.; Parma, M.; Maggiore, U.L.R.; Athanasiou, S.; Candiani, M. Microablative fractional CO2 laser for vulvovaginal atrophy in women with a history of breast cancer: A pilot study at 4-week follow-up. Clin. Breast Cancer 2021, 21, e539–e546. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Initial Participants with 4 Week Follow-Up (n = 64) | Participants with 1 Year Follow-Up (n = 39) | Participants with 2 Year Follow-Up (n = 33) | |
|---|---|---|---|
| Age (on study) | |||
| Mean (SD) | 57.4 (9.5) | 57.7 (10.50) | 59.3 (10.8) |
| Stage | |||
| I | 32 (50.0%) | 19 (48.7%) | 15 (45.5%) |
| II | 21 (32.8%) | 13 (33.3%) | 10 (30.3%) |
| III | 7 (10.9%) | 4 (10.3%) | 5 (15.2%) |
| IV | 1 (1.6%) b | 1 (2.6%) | 0 (0%) |
| Histology | |||
| Adenocarcinoma | 51 (76.7%) | 32 (82.1%) | 27 (81.8%) |
| Other | 13 (20.3%) | 7 (18.0%) | 6 (18.2%) |
| ER status | |||
| Negative | 5 (7.8%) | 0 (0%) | 1 (3.0%) |
| Positive | 58 (90.6%) | 38 (97.4%) | 31 (93.9%) |
| Unknown | 1 (1.6%) | 1 (2.6%) | 1 (3.0%) |
| PR status | |||
| Negative | 15 (23.4%) | 6 (15.4%) | 7 (21.2%) |
| Positive | 47 (73.4%) | 31 (79.5%) | 25 (75.8%) |
| Unknown | 2 (3.1%) | 2 (5.1%) | 1 (3.0%) |
| HER2 Neu status | |||
| Negative | 50 (78.1%) | 28 (71.8%) | 26 (78.8%) |
| Positive | 11 (17.2%) | 9 (23.1%) | 4 (12.1%) |
| Unknown | 3 (4.7%) | 2 (5.1%) | 3 (9.1%) |
| ER−/PR− | 5 (7.8%) | 0 (0%) | 1 (3.0%) |
| ER+/PR+ | 47 (73.4%) | 31 (79.5%) | 25 (75.8%) |
| ER+/PR− | 10 (15.6%) | 6 (15.4%) | 6 (18.2%) |
| Chemotherapy | |||
| Yes | 36 (56.3%) | 20 (51.3%) | 16 (48.5%) |
| No | 27 (42.2%) | 18 (46.2%) | 16 (48.5%) |
| Unknown | 1 (1.6%) | 1 (2.6%) | 1 (3.0%) |
| Endocrine therapy use | |||
| Yes | 59 (92.2%) | 37 (94.9%) | 32 (97.0%) |
| No | 4 (6.3%) | 1 (2.6%) | 0 (0%) |
| Unknown | 1 (1.6%) | 1 (2.6%) | 1 (3.0%) |
| Type of endocrine therapy | |||
| Tamoxifen | 13 (20.3%) | 9 (23.1%) | 7 (21.2%) |
| AI | 44 (68.8%) | 26 (66.7%) | 23 (69.7%) |
| Tamoxifen and ovarian suppression | 2 (3.1%) | 2 (5.1%) | 2 (6.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quick, A.M.; Hundley, A.; Evans, C.; Stephens, J.A.; Ramaswamy, B.; Reinbolt, R.E.; Noonan, A.M.; Van Deusen, J.B.; Wesolowski, R.; Stover, D.G.; et al. Long-Term Follow-Up of Fractional CO2 Laser Therapy for Genitourinary Syndrome of Menopause in Breast Cancer Survivors. J. Clin. Med. 2022, 11, 774. https://doi.org/10.3390/jcm11030774
Quick AM, Hundley A, Evans C, Stephens JA, Ramaswamy B, Reinbolt RE, Noonan AM, Van Deusen JB, Wesolowski R, Stover DG, et al. Long-Term Follow-Up of Fractional CO2 Laser Therapy for Genitourinary Syndrome of Menopause in Breast Cancer Survivors. Journal of Clinical Medicine. 2022; 11(3):774. https://doi.org/10.3390/jcm11030774
Chicago/Turabian StyleQuick, Allison M., Andrew Hundley, Cynthia Evans, Julie A. Stephens, Bhuvaneswari Ramaswamy, Raquel E. Reinbolt, Anne M. Noonan, Jeffrey Bryan Van Deusen, Robert Wesolowski, Daniel G. Stover, and et al. 2022. "Long-Term Follow-Up of Fractional CO2 Laser Therapy for Genitourinary Syndrome of Menopause in Breast Cancer Survivors" Journal of Clinical Medicine 11, no. 3: 774. https://doi.org/10.3390/jcm11030774
APA StyleQuick, A. M., Hundley, A., Evans, C., Stephens, J. A., Ramaswamy, B., Reinbolt, R. E., Noonan, A. M., Van Deusen, J. B., Wesolowski, R., Stover, D. G., Williams, N. O., Sardesai, S. D., Faubion, S. S., Loprinzi, C. L., & Lustberg, M. B. (2022). Long-Term Follow-Up of Fractional CO2 Laser Therapy for Genitourinary Syndrome of Menopause in Breast Cancer Survivors. Journal of Clinical Medicine, 11(3), 774. https://doi.org/10.3390/jcm11030774