
Hyaluronic Acid/Collagenase Ointment in the Treatment of Chronic Hard-to-Heal Wounds: An Observational and Retrospective Study




Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Assessment Methods
2.3. Statistical Analysis
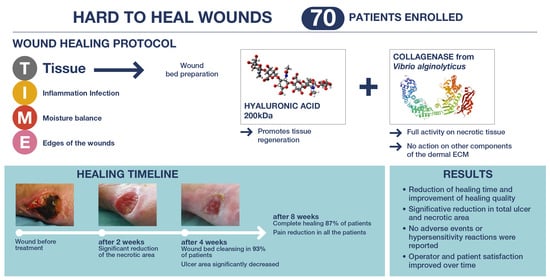
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| COGA | clinician’s global assessment of the wound |
| CW | chronic wound |
| ECM | extracellular matrix |
| HA | hyaluronic acid |
| PTGA | patient satisfaction regarding wound outcomes |
| VAS | visual analogic scale |
References
- Gilmore, M.A. Phases of wound healing. Dimens. Oncol. Nurs. 1991, 5, 32–34. [Google Scholar]
- Han, G.; Ceilley, R. Chronic Wound Healing: A review of current management and treatments. Adv. Ther. 2017, 34, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Demidova-Rice, T.N.; Hamblin, M.R.; Herman, I.M. Acute and impaired wound healing: Pathophysiology and current methods for drug delivery, part 1: Normal and chronic wounds: Biology, causes, and approaches to care. Adv. Skin Wound Care 2012, 25, 304–314. [Google Scholar] [CrossRef]
- Pawar, K.B.; Desai, S.; Bhonde, R.R.; Bhole, R.P.; Deshmukh, A.A. Wound with diabetes: Present Scenario and Future. Curr Diabetes Rev. 2021, 17, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.; Stratman, S.; Kirsner, R.S. Lower extremity ulcers. Med. Clin. N. Am. 2021, 105, 663–679. [Google Scholar] [CrossRef]
- Alam, W.; Hasson, J.; Reed, M. Clinical approach to chronic wound management in older adults. J. Am. Geriatr. Soc. 2021, 69, 2327–2334. [Google Scholar] [CrossRef] [PubMed]
- East, J.M.; Fray, D.A.; Hall, D.E.; Longmore, C.A. Chronic neuropathic ulcer is not the most common antecedent of lower limb infection or amputation among diabetics admitted to a regional hospital in Jamaica: Results from a prospective cohort study. BMC Surg. 2015, 21, 104. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; De Angelis, B.; Pea, F.; Scalise, A.; Stefani, S.; Tasinato, R.; Zanetti, O.; Dalla Paola, L. Challenges in the management of chronic wound infections. J. Glob. Antimicrob. Resist. 2021, 26, 140–147. [Google Scholar] [CrossRef]
- Martinez Garcia, R.M.; Fuentes Chacon, R.M.; Lorenzo Mora, A.M.; Ortega Anta, R.M. Nutrition in the prevention and healing of chronic wounds. Importance in improving the diabetic foot. Nutr. Hosp. 2021, 38, 60–63. [Google Scholar] [CrossRef]
- Wilkinson, H.N.; Hardman, M.J. Wound healing: Cellular mechanisms and pathological outcomes. Open Biol. 2020, 10, 200223. [Google Scholar] [CrossRef]
- Goldberg, S.R.; Diegelmann, R.F. What Makes Wounds Chronic. Surg. Clin. N. Am. 2020, 100, 681–693. [Google Scholar] [CrossRef]
- Frykberg, R.G.; Banks, J. Challenges in the Treatment of Chronic Wounds. Adv. Wound Care 2015, 4, 560–582. [Google Scholar] [CrossRef]
- Nussbaum, S.R.; Carter, M.J.; Fife, C.E.; DaVanzo, J.; Haught, R.; Nusgart, M.; Cartwright, D. An Economic Evaluation of the impact, cost, and medicare policy implications of chronic nonhealing wounds. Value Health 2018, 21, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Sen, C.K.; Roy, S. Socioeconomic approach to wound care: A new patient-centered paradigm. Adv. Wound Care 2019, 8, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Panuncialman, J.; Falanga, V. The science of wound bed preparation. Surg. Clin. N. Am. 2009, 89, 611–626. [Google Scholar] [CrossRef]
- Falanga, V.; Saap, L.J.; Ozonoff, A. Wound bed score and its correlation with healing of chronic wounds. Dermatol. Ther. 2006, 19, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Falanga, V.; Brem, H.; Ennis, W.J.; Wolcott, R.; Gould, L.J.; Ayello, E.A. Maintenance debridement in the treatment of difficult-to-heal chronic wounds. Recommendations of an expert panel. Ostomy Wound Manag. 2008, 2–13, quiz 14–15. [Google Scholar] [PubMed]
- Schultz, G.; Sibbald, R.G.; Falanga, V.; Ayello, E.A.; Dowsett, C.; Harding, K.; Romanelli, M.; Stacey, M.C.; Teot, L.; Vanscheidt, W. Wound bed preparation: A systematic approach to wound management. Wound Repair Regen. 2003, 11 (Suppl. S1), S1–S28. [Google Scholar] [CrossRef]
- Ayello, E.A.; Cuddigan, J.E. Debridement: Controlling the necrotic/cellular burden. Adv. Skin Wound Care 2004, 17, 66–75. [Google Scholar] [CrossRef]
- Sen, C.K.; Roy, S.; Mathew-Steiner, S.; Gordillo, G.M. Biofil management in wound care. Plast. Reconstr. Surg. 2021, 148, 275e–288e. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, F.; Marchesini, A.; Campodonico, A.; Neuendorf, A.D.; Pangrazi, P.P.; Riccio, M. A multistep iter for functional reconstruction in mangled upper limb: A retrospective analysis of integrated surgical and medical approach. Medicina 2020, 56, 398. [Google Scholar] [CrossRef] [PubMed]
- Moog, P.; Jensch, M.; Betzl, J.; Bauer, A.T.; Cerny, M.K.; Schmauss, D.; Kukrek, H.; Erne, H.; Machens, H.G.; Megerle, K. Bacterial bioburden of wounds: Influence of debridement and negative-pressure wound therapy (NPWT). J. Wound Care 2021, 30, 604–611. [Google Scholar] [CrossRef]
- Kravitz, S.R.; McGuire, J.; Zinszer, K. Management of skin ulcers: Understanding the mechanism and selection of enzymatic debriding agents. Adv. Skin Wound Care 2008, 21, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Falanga, V. Classifications for wound bed preparation and stimulation of chronic wounds. Wound Repair Regen. 2000, 8, 347–352. [Google Scholar] [PubMed]
- Shah, D.; Mital, K. The role of trypsin: Chymotrypsin in tissue repair. Adv. Ther. 2018, 35, 31–42. [Google Scholar] [CrossRef]
- Forsling, E. Comparison of saline and streptokinase-streptodornase in the treatment of leg ulcers. Eur. J. Clin. Pharm. 1988, 33, 637–638. [Google Scholar] [CrossRef]
- Karlsson, C.; Andersson, M.L.; Collin, M.; Schmidtchen, A.; Bjorck, L.; Frick, I.M. SulfA—A novel subtilisin-like serine proteinase of Finegoldia magna. Microbiology 2007, 153, 4208–4218. [Google Scholar] [CrossRef]
- Pavan, R.; Jain, S.; Shraddha; Kumar, A. Properties and therapeutic application of bromelain: A review. Biotechnol. Res. Int. 2012, 2012, 976203. [Google Scholar] [CrossRef]
- Ramundo, J.; Gray, M. Enzymatic wound debridement. J. Wound Ostomy Cont. Nurs. 2008, 35, 273–280. [Google Scholar] [CrossRef]
- Wright, J.B.; Shi, L. Accuxyme (R) papain-urea debriding ointment: A historical review. Wounds 2003, 15, 2S–12S. [Google Scholar]
- Marazzi, M.; Stefani, A.; Chiaratti, A.; Ordanini, M.N.; Falcone, L.; Rapisarda, V. Effect of enzymatic debridement with collagenase on acute and chronic hard-to-heal wounds. J. Wound Care 2006, 15, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Cortivo, R.; Abatangelo, A. Bionect Start: The biological synergy for the evolution of enzymatic debridement. J. Wound Technol. 2011, 13, 24–27. [Google Scholar]
- Onesti, M.G.; Fioramonti, P.; Fino, P.; Sorvillo, V.; Carella, S.; Scuderi, N. Effect of enzymatic debridement with two different collagenases versus mechanical debridement on chronic hard-to.-heal wounds. Int. Wound J. 2016, 13, 1111–1115. [Google Scholar] [CrossRef] [PubMed]
- Mast, B.A.; Diegelmann, R.F.; Krummel, T.M.; Cohen, I.K. Hyaluronic acid modulates proliferation, collagen and protein synthesis of cultured fetal fibroblasts. Matrix 1993, 13, 441–446. [Google Scholar] [CrossRef]
- Croce, M.A.; Dyne, K.; Boraldi, F.; Quaglino, D., Jr.; Cetta, G.; Tiozzo, R.; Pasquali Ronchetti, I. Hyaluronan affects protein and collagen synthesis by in vitro human skin fibroblasts. Tissue Cell 2001, 33, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Falanga, V. Measurement in wound healing. Int. J. Low. Extrem. Wounds 2008, 7, 9–11. [Google Scholar] [CrossRef]
- Gravante, G.; Sorge, R.; Giordan, N.; Georgescu, S.R.; Morariu, S.H.; Stoicescu, I.; Clatici, V. Multicenter clinical trial on the performance and tolerability of the Hyaluronic acid-collagenase ointment for the treatment of chronic venous ulcers: A preliminary pilot study. Eur. Rev. Med. Pharm. Sci. 2013, 17, 2721–2727. [Google Scholar]
- Gupta, S.; Sagar, S.; Maheshwari, G.; Kisaka, T.; Tripathi, S. Chronic wounds: Magnitude, socioeconomic burden and consequences. Wounds Asia 2021, 4, 8–14. [Google Scholar]
- Madhok, B.M.; Vowden, K.; Vowden, P. New techniques for wound debridement. Int. Wound J. 2013, 10, 247–251. [Google Scholar] [CrossRef]
- Sinclair, R.D.; Ryan, T.J. Proteolytic enzymes in wound healing: The role of enzymatic debridement. Australas. J. Derm. 1994, 35, 35–41. [Google Scholar] [CrossRef]
- McCallon, S.K.; Weir, D.; Lantis, J.C., 2nd. Optimizing wound bed preparation with collagenase enzymatic debridement. J. Am. Coll. Clin. Wound Spec. 2015, 6, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Di Pasquale, R.; Vaccaro, S.; Caputo, M.; Cuppari, C.; Caruso, S.; Catania, A.; Messina, L. Collagenase-assisted wound bed preparation: An in vitro comparison between Vibrio alginolyticus and Clostridium histolyticum collagenases on substrate specifity. Int. Wound J. 2019, 16, 1013–1023. [Google Scholar] [PubMed]
- Ghosh, K.; Ren, X.D.; Shu, X.Z.; Prestwich, G.D.; Clark, R.A.F. Fibronectin functional domains coupled to hyaluronan stimulate adult human dermal fibroblast responses critical for wound healing. Tissue Eng. 2006, 12, 601–613. [Google Scholar] [CrossRef] [PubMed]
- Onesti, M.G.; Fioramonti, P.; Carella, S.; Fino, P.; Sorvillo, V.; Scuderi, N. A new association between hyaluronic acid and collagenase in wound repair: An open study. Eur. Rev. Med. Pharm. Sci. 2013, 17, 210–216. [Google Scholar]
- Scalise, A.; Campitiello, F.; Della Corte, A.; Longobardi, P.; Di Salvo, M.; Tartaglione, C.; Santin, C.; Giordan, N.; Guarnera, G. Enzymatic debridement: Is HA-collagenase the right synergy? Randomized double-blind controlled clinical trial in venous leg ulcers. Eur. Rev. Med. Pharm. Sci. 2017, 21, 1421–1431. [Google Scholar]
- Patry, J.; Blanchette, V. Enzymatic debridement with collagenase in wounds and ulcers: A systematic review and meta-analysis. Int. Wound J. 2017, 14, 1055–1065. [Google Scholar] [CrossRef] [PubMed]
- Foschi, D.; Castoldi, L.; Radaelli, E.; Abelli, P.; Calderini, G.; Rastrelli, A.; Mariscotti, C.; Marazzi, M.; Trabucchi, E. Hyaluronic acid prevents oxygen free-radical damage to granulation tissue: A study in rats. Int. J. Tissue React. 1990, 12, 333–339. [Google Scholar]
- Riccio, M.; Marchesini, A.; Senesi, L.; Skrami, E.; Gesuita, R.; De Francesco, F. Managing pathologic scars by injecting auto-cross-linked hyaluronic acid. A preliminary prospective clinical study. Aesthetic Plast. Surg. 2019, 43, 480–489. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bionect Start | |
|---|---|
| Patients | 70 |
| Sex | |
| Male | 45 (65%) |
| Female | 25 (35%) |
| Age | |
| Average | 59.2 |
| SD | 12.76 |
| Range | 32–85 |
| Smokers | |
| Yes | 40 (57%) |
| No | 30 (43%) |
| BMI | |
| Average | 32.56 |
| Median | 31.7 |
| SD | 8.276 |
| Range | 19.9–81.6 |
| Etiologies | |
| Diabetes | 20 (28%) |
| Post-traumatic ulcers | 35 (50%) |
| Burns | 10 (14%) |
| Pressure ulcers | 5 (7%) |
| Scores of 0 | Scores of 1 | Scores of 2 | |
|---|---|---|---|
| Black Eschar | >25% of wound surface area | 0–75% | >75% of wound surface area |
| Eczema/Dermatitis | Severe | Moderate | None/mild |
| Depth/granulation | Severely depressed or raised when compared to periwound skin | Moderate | Flushed or almost even |
| Scarring | Severe | Moderate | None/mild |
| Color of wound bed | None | 50–75% | >75% |
| Oedema/Swelling | Severe | Moderate | None/mild |
| Resurfacing epithelium | None | 25–75% | >75% |
| Exudate amount | Severe | Moderate | None/mild |
| Time of Visit | ||||||
|---|---|---|---|---|---|---|
| Pre-Treatment (V0) | 2 Weeks (V1) | 4 Weeks (V2) | 2 Months (V3) | 1 Year (V4) | ||
| Scale of debridement | 1 | 0 | 0 | 61 (87%) | 62 (89%) | 70 (100%) |
| 2 | 0 | 0 | 0 | 5 (0.7%) | ||
| 3 | 0 | 9 (13%) | 7 (10%) | 3 (0.4%) | ||
| 4 | 0 | 33 (47%) | 1 (0.1%) | |||
| 5 | 70 (100%) | 28 (40%) | 1 (0.1%) | |||
| Total area (cm2) | 60 (3–576) | 43 (2–360) | 15 (0–100) | 4 (0–50) | 0 | |
| Necrotic area (cm2) | 60 (3–576) | 29 (2–210) | 3 (0–60) | 2 (0–30) | 0 | |
| Percentage of necrotic area (%) | 100 | 74 (33–100) | 7 (0–87) | 38 (0–71) | 0 | |
| Time of Visit | |||||
|---|---|---|---|---|---|
| WBS Score | Pre-Treatment (V0) | 2 Weeks (V1) | 4 Weeks (V2) | 2 Months (V3) | |
| black eschar | 0 | 46 (66%) | 0 (0%) | 0 (0%) | 0 (0%) |
| 1 | 24 (34%) | 39 (56%) | 39 (56%) | 0 (0%) | |
| 2 | 0 (0%) | 31 (44%) | 31 (44%) | 70 (100%) | |
| eczema/dermatitis | 0 | 18 (26%) | 0 (0%) | 0 (0%) | 0 (0%) |
| 1 | 52 (74%) | 26 (37%) | 0 (0%) | 0 (0%) | |
| 2 | 0 (0%) | 44 (63%) | 70 (100%) | 70 (100%) | |
| depth scarring | 0 | 39 (56%) | 0 (0%) | 0 (0%) | 0 (0%) |
| 1 | 31 (44%) | 37 (53%) | 0 (0%) | 0 (0%) | |
| 2 | 0 (0%) | 33 (47%) | 70 (100%) | 70 (100%) | |
| color of WB | 0 | 60 (86%) | 31 (44%) | 0 (0%) | 0 (0%) |
| 1 | 10 (14%) | 38 (54%) | 24 (34%) | 0 (0%) | |
| 2 | 0 (0%) | 1 (1%) | 46 (66%) | 70 (100%) | |
| oedema | 0 | 17 (24%) | 3 (4%) | 0 (0%) | 0 (0%) |
| 1 | 30 (43%) | 16 (23%) | 3 (4%) | 0 (0%) | |
| 2 | 23 (33%) | 51 (73%) | 67 (96%) | 70 (100%) | |
| resurfacing epithelium | 0 | 27 (39%) | 0 (0%) | 0 (0%) | 0 (0%) |
| 1 | 43 (61%) | 26 (37%) | 0 (0%) | 0 (0%) | |
| 2 | 0 (0%) | 44 (63%) | 70 (100%) | 70 (100%) | |
| exudate amount | 0 | 70 (100%) | 0 (0%) | 0 (0%) | 0 (0%) |
| 1 | 0 (0%) | 70 (100%) | 0 (0%) | 0 (0%) | |
| 2 | 0 (0%) | 0 (0%) | 70 (100%) | 70 (100%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Francesco, F.; De Francesco, M.; Riccio, M. Hyaluronic Acid/Collagenase Ointment in the Treatment of Chronic Hard-to-Heal Wounds: An Observational and Retrospective Study. J. Clin. Med. 2022, 11, 537. https://doi.org/10.3390/jcm11030537
De Francesco F, De Francesco M, Riccio M. Hyaluronic Acid/Collagenase Ointment in the Treatment of Chronic Hard-to-Heal Wounds: An Observational and Retrospective Study. Journal of Clinical Medicine. 2022; 11(3):537. https://doi.org/10.3390/jcm11030537
Chicago/Turabian StyleDe Francesco, Francesco, Marialuisa De Francesco, and Michele Riccio. 2022. "Hyaluronic Acid/Collagenase Ointment in the Treatment of Chronic Hard-to-Heal Wounds: An Observational and Retrospective Study" Journal of Clinical Medicine 11, no. 3: 537. https://doi.org/10.3390/jcm11030537
APA StyleDe Francesco, F., De Francesco, M., & Riccio, M. (2022). Hyaluronic Acid/Collagenase Ointment in the Treatment of Chronic Hard-to-Heal Wounds: An Observational and Retrospective Study. Journal of Clinical Medicine, 11(3), 537. https://doi.org/10.3390/jcm11030537