
Therapeutic Aquatic Exercise in Pregnancy: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
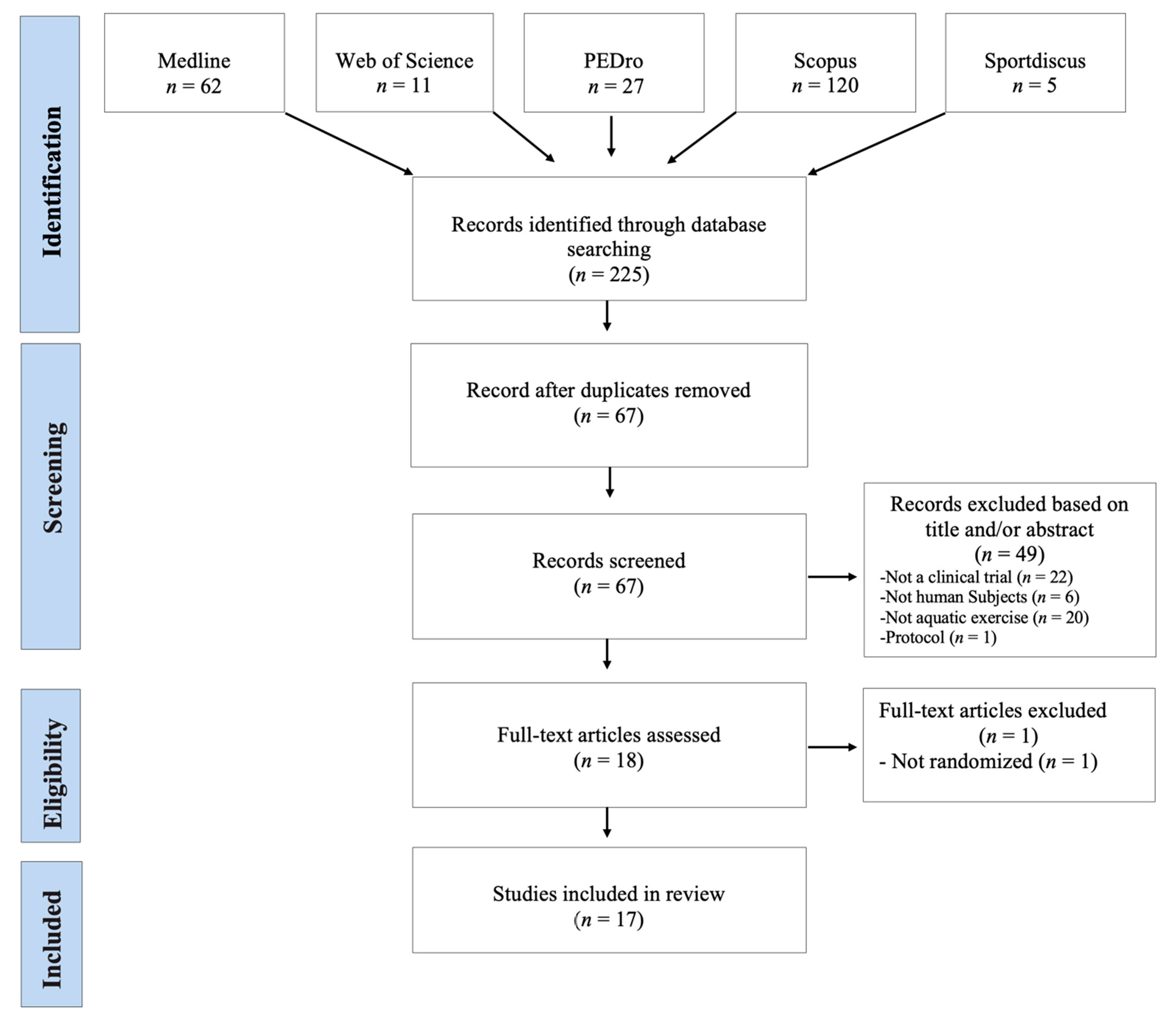
2.1. Search Strategy and Screening Procedures
2.2. Inclusion/Exclusion Criteria
2.3. Selection Process
2.4. Meta-Analysis
2.5. Quality Assessment
3. Results
3.1. Description of Studies Include in Review
3.2. Quality Assessment
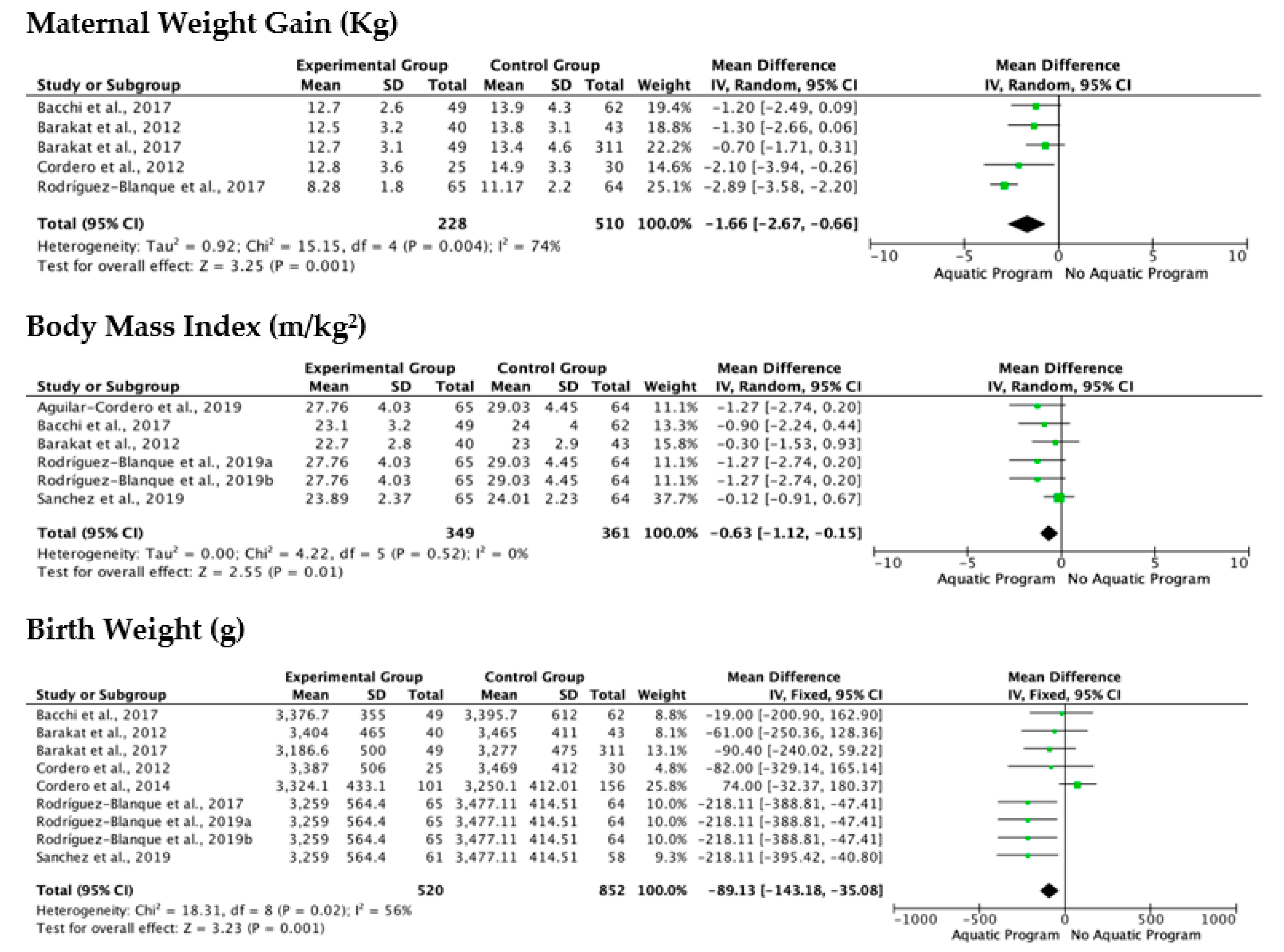
3.3. Meta-Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Dios, M.I.; Díaz, P. Cambios Anatomofisiológicos en la Mujer Gestante. Manual básico de Obstetricia y Ginecología; Instituto Nacional de Gestión Sanitaria: Madrid, Spain, 2017; pp. 72–95. [Google Scholar]
- Balan, P.; Chong, Y.S.; Umashankar, S.; Swarup, S.; Loke, W.M.; Lopez, V.; He, H.G.; Seneviratne, C.J. Keystone Species in Pregnancy Gingivitis: A Snapshot of Oral Microbiome during Pregnancy and Postpartum Period. Front. Microbiol. 2018, 9, 2360. [Google Scholar] [CrossRef] [PubMed]
- Dodds, L.; Fell, D.B.; Joseph, K.S.; Allen, V.M.; Butler, B. Outcomes of Pregnancies Complicated by Hyperemesis Gravidarum. Obstet. Gynecol. 2006, 107, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Cullen, G.; O’Donoghue, D. Constipation and pregnancy. Best Pract. Res. Clin. Gastroenterol. 2007, 21, 807–818. [Google Scholar] [CrossRef]
- Seok, L.D.; Won, K.J.; Lae, L.K.; Gwan, K.B. Prevalence and predictors of gastroesophageal reflux disease in pregnant women and its effects on quality of life and pregnancy outcomes. J. Gynecol. Res. Obstet. 2021, 7, 008–011. [Google Scholar] [CrossRef]
- Suryanarayana, R.; Chandrappa, M.; Santhuram, A.N.; Prathima, S.; Sheela, S.R. Prospective study on prevalence of anemia of pregnant women and its outcome: A community based study. J. Fam. Med. Prim. Care 2017, 6, 739–743. [Google Scholar] [CrossRef] [PubMed]
- Bhandiwad, A.; Desai, N.; Kondareddy, T. Maternal outcomes of rheumatic heart disease in pregnancy. Int. J. Reprod. Contracept. Obstet. Gynecol. 2017, 6, 802. [Google Scholar] [CrossRef]
- Ramlakhan, K.P.; Johnson, M.R.; Roos-Hesselink, J.W. Pregnancy and cardiovascular disease. Nat. Rev. Cardiol. 2020, 17, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Castellón, N.M.; Ruíz, P.S.; Ordóñez, E.F. Problemas de salud durante el embarazo derivados de los riesgos de la actividad laboral. Rev. Enferm. Trab. 2017, 7, 117–122. [Google Scholar]
- Melzer, K.; Schutz, Y.; Boulvain, M.; Kayser, B. Physical Activity and Pregnancy. Sports Med. 2010, 40, 493–507. [Google Scholar] [CrossRef] [PubMed]
- Perales, M.; Santos-Lozano, A.; Ruiz, J.R.; Lucia, A.; Barakat, R. Benefits of aerobic or resistance training during pregnancy on maternal health and perinatal outcomes: A systematic review. Early Hum. Dev. 2016, 94, 43–48. [Google Scholar] [CrossRef]
- Thompson, E.L.; Vamos, C.A.; Daley, E.M. Physical activity during pregnancy and the role of theory in promoting positive behavior change: A systematic review. J. Sport Health Sci. 2017, 6, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Hernández-García, R.; Rodríguez-Díaz, L.; Molina-Torres, G.; Torres-Luque, G. Efectos de un programa de actividad física con el método pilates sobre la funcionalidad de mujeres embarazadas. Estudio piloto. Revista Iberoamericana Ciencias Actividad Física Deporte 2018, 7, 40–52. [Google Scholar] [CrossRef]
- Matsuzaki, M.; Kusaka, M.; Sugimoto, T.; Shiraishi, M.; Kobayashi, R.; Watanabe, S.; Haruna, M. The Effects of a Yoga Exercise and Nutritional Guidance Program on Pregnancy Outcomes among Healthy Pregnant Japanese Women: A Study Protocol for a Randomized Controlled Trial. J. Altern. Complement. Med. 2018, 24, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Kagawa, K.; Hori, N.; Akezaki, Y.; Mori, K.; Nomura, T. Preliminary validation of an exercise program suitable for pregnant women with abnormal glucose metabolism: Inhibitory effects of Tai Chi Yuttari-exercise on plasma glucose elevation. J. Phys. Ther. Sci. 2016, 28, 3411–3415. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Cordero, M.J.; Sánchez-García, J.C.; Blanque, R.R.; López, A.M.S.; Mur-Villar, N. Moderate Physical Activity in an Aquatic Environment During Pregnancy (SWEP Study) and Its Influence in Preventing Postpartum Depression. J. Am. Psychiatr. Nurses Assoc. 2019, 25, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Bacchi, M.; Rodríguez, Y.C.; Puente, M.P.; Mas, C.L.; Carballo, R. Efecto sobre la frecuencia cardiaca del ejercicio en tierra/agua en embarazadas en el tercer trimestre de gestación: Un estudio comparativo. Calid. Vida Salud 2011, 4, 59–67. [Google Scholar]
- Bacchi, M.; Mottola, M.F.; Perales, M.; Refoyo, I.; Barakat, R. Aquatic Activities during Pregnancy Prevent Excessive Maternal Weight Gain and Preserve Birth Weight: A Randomized Clinical Trial. Am. J. Health Promot. 2018, 32, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; Cordero, Y.; Coteron, J.; Luaces, M.; Montejo, R. Exercise during pregnancy improves maternal glucose screen at 24–28 weeks: A randomised controlled trial. Br. J. Sports Med. 2012, 46, 656–661. [Google Scholar] [CrossRef]
- Barakat, R.; Perales, M.; Cordero, Y.; Bacchi, M.; Mottola, M.F. Influence of Land or Water Exercise in Pregnancy on Outcomes. Med. Sci. Sports Exerc. 2017, 49, 1397–1403. [Google Scholar] [CrossRef] [PubMed]
- Cordero, Y.; Pelaez, M.; De Miguel, M.; Perales, M.; Barakat, R. ¿Puede el ejercicio físico moderado durante el embarazo actuar como un factor de prevención de la diabetes gestacional? Int. J. Sport Sci. 2012, 8, 3–19. [Google Scholar]
- Cordero, Y.; Mottola, M.F.; Vargas, J.; Blanco, M.; Barakat, R. Exercise Is Associated with a Reduction in Gestational Diabetes Mellitus. Med. Sci. Sports Exerc. 2015, 47, 1328–1333. [Google Scholar] [CrossRef]
- Granath, A.B.; Hellgren, M.S.; Gunnarsson, R.K. Water Aerobics Reduces Sick Leave due to Low Back Pain during Pregnancy. J. Obstet. Gynecol. Neonatal Nurs. 2006, 35, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Blanque, R.; Sánchez-García, J.C.; Sánchez-López, A.M.; Mur-Villar, N.; Fernández-Castillo, R.; Cordero, M.J.A. Influencia del ejercicio físico durante el embarazo sobre el peso del recién nacido: Un ensayo clínico aleatorizado. Nutrición Hospitalaria 2017, 34, 834–840. [Google Scholar] [CrossRef]
- Rodriguez-Blanque, R.; Sánchez-García, J.; Sánchez-López, A.; Mur-Villar, N.; Aguilar-Cordero, M. The influence of physical activity in water on sleep quality in pregnant women: A randomised trial. Women Birth 2018, 31, e51–e58. [Google Scholar] [CrossRef]
- Rodríguez-Blanque, R.; Garcia, J.C.S.; López, A.M.S.; Expósito-Ruiz, M.; Aguilar-Cordero, M.J. Randomized Clinical Trial of an Aquatic Physical Exercise Program during Pregnancy. J. Obstet. Gynecol. Neonatal Nurs. 2019, 48, 321–331. [Google Scholar] [CrossRef]
- Rodríguez-Blanque, R.; Garcia, J.C.S.; López, A.M.S.; Aguilar-Cordero, M.J. Physical activity during pregnancy and its influence on delivery time: A randomized clinical trial. PeerJ 2019, 7, e6370. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-García, J.C.; Aguilar-Cordero, M.J.; Menor-Rodríguez, M.J.; Paucar-Sánchez, A.; Rodríguez Blanque, R. Influencia del ejercicio físico en la evolución del peso gestacional y posparto. Ensayo clínico aleatorizado. Nutr. Hosp. 2019, 36, 1–8. [Google Scholar] [CrossRef]
- Sillero-Quintana, M.; Conde-Pascual, E.; Gomez-Carmona, P.M.; Fernandez-Cuevas, I.; García-Pastor, T. Effect of yoga and swimming on body temperature of pregnant women. Thermol. Int. 2012, 22, 108. [Google Scholar]
- Smith, S.A.; Michel, Y. A Pilot Study on the Effects of Aquatic Exercises on Discomforts of Pregnancy. J. Obstet. Gynecol. Neonatal Nurs. 2006, 35, 315–323. [Google Scholar] [CrossRef]
- Vallim, A.L.; Osis, M.J.; Cecatti, J.G.; Baciuk, E.P.; Silveira, C.; Cavalcante, S.R. Water exercises and quality of life during pregnancy. Reprod. Health 2011, 8, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Lara, J.M.; Ruiz-Frutos, C.; Rodríguez-Díaz, L.; Ramírez-Rodrigo, J.; Villaverde-Gutiérrez, C.; Torres-Luque, G. Effect of a physical activity programme in the aquatic environment on haemodynamic constants in pregnant women. Enfermería Clínica 2018, 28, 316–325. [Google Scholar] [CrossRef]
- Wolford, S. Viewpoints on aquatic fitness for pregnancy and postpartum. AKWA 1999, 1, 6–7. [Google Scholar]
- Katz, V.L. Exercise in Water during Pregnancy. Clin. Obstet. Gynecol. 2003, 46, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, A.P.; de Vet, H.C.; de Bie, R.A.; Kessels, A.G.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi List: A Criteria List for Quality Assessment of Randomized Clinical Trials for Conducting Systematic Reviews Developed by Delphi Consensus. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Reference | Purpose | Participants | Mean Age ± SD (Median/Range) | Gestational Age (Weeks) | Type of Intervention (E/C) | Intervention (Wk/f/min) | Adherence | Findings | Measurement Tools |
|---|---|---|---|---|---|---|---|---|---|
| Aguilar-Cordero et al. [17] | Determine if physical activity in pregnancy relieves PPP. | EG = 65 CG = 64 | EG = 34.52 ± 4.50 CG = 33.67 ± 5.37 | 20th–37th | EG = Aerobic and resistance activities-SWEP (water) CG = Routine prenatal care | EG = 17/3/60 CG = NR | EG = 92.82% CG = 91.4% | Less at risk of Depression (EPDS) in EG. Overweight and obesity are closely associated with PPD. | Perception of effort (Borg scale) BMI (Formula QUETELET) Depression postpartum (Edinburgh Postnatal Depression Scale-EPDS-) |
| Bacchi et al. [18] | Evaluate and compare maternal HR in water and land exercises with the same intensity | EG = 15 CG = 15 | NR | 3rd TRIMESTRE (27th–38th–42nd) | EG = Calisthenics exercise (water) CG = Calisthenics exercise (land) | EG = 1/1/25 CG = 1/1/25 | EG = 100% CG = 100% | Calisthenics exercise (land) produce higher FC elevations (110.86 ± 6.10) than calisthenics exercise (water) (105.40 ± 6.10), but not significant differences. | Perception of effort (Borg scale) Heart rate monitor (Polar F6); |
| Bacchi et al. [19] | Study the effect of a program of aquatic activities on pregnancy on maternal weight and birth weight | EG = 49 CG = 62 | EG = 30.4 ± 4.0 CG = 31.0 ± 5.0 | 10 to 12th/38 to 39th | EG = Aerobic and resistance activities (water) CG = Routine prenatal care | EG = 26–29/3/55–60 CG = NR | EG = 70% CG = 88.57% | Higher percentage of women with excessive maternal weight gain in the CG (45.2%; n = 28) than in the EG (24.5%). Aerobic and resistance activities (Water) increase maternal weight and preserves birth weight. | Perception of effort (Borg scale) BMI (Formula QUETELET) |
| Barakat et al. [20] | Analyze glucose tolerance through aquatic exercises for pregnant women | EG = 40 CG = 43 | EG = 32 ± 4 CG = 31 ± 3 | 24th–28th | EG = Aerobic activities (land + water) CG = Routine prenatal care | EG = 32–33/2 + 1/35–45 CG = NR | EG = 80% CG = 86% | The glucose values corresponding to the EG (103.80 ± 20.40 mg/dL) were better (significant differences; p = 0.001) than those of the CG (126.9 ± 29.5 mg/dL). No differences in maternal weight and cases of gestational diabetes. Exercise during pregnancy improves the level of tolerance to maternal glucose. | Heart rate monitor (Accurex Plus, Sark Products, Waltham, MA, USA); Polar Electro OY (Polar, Kempele, Finland) Perception of effort (Borg scale) Blood glucose level (blood test) |
| Barakat et al. [21] | Compare terrestrial or aquatic exercises during pregnancy in maternal and neonatal outcomes. | EG1 = 107 EG2 = 49 EG3 = 101 CG = 311 | EG1 = 31.5 ± 3.8 EG2 = 30.9 ± 4.0 EG3 = 32.0 ± 3.5 EC = 31.9 ± 4.5 | 9th–11th | EG1 = aerobic activities (land) EG2 = aerobic + resistance activities (water) EG3 = aerobic activities (land) + resistance activities (water) CG = Routine prenatal care | EG1 = 30/3/55–60 EG2 = 30/3/55–60 EG3 = 30/2 + 1/55–60 CG = NR | EG1 = 79.68% EG2 = 79.28% EG3 = 75.14% CG = NR | Exercise on land is more effective in preventing excessive maternal weight gain (p = 0.001). Combined programs or aquatic programs seem more effective in preventing gestational diabetes (p = 0.03). Both are safe for the baby. | Evaluate knowledge, attitudes and reasoning (questionnaire ad hoc) Height (stature meter) Weight (weight scale) |
| Cordero et al. [22] | Evaluate the effectiveness of a moderate exercise program during pregnancy on maternal weight, glucose and gestational diabetes. | EG = 25 CG = 30 | EG = 34.1 ± 4.7 CG = 31.6 ± 2.0 | 6th–10th/38th–39th | EG = aerobic activities (land) + resistance activities (water) CG: Routine prenatal care | EG = 28/2 + 1/50 CG = NR | EG = 62.50%; CG = 75.00% | The exercise program performed during pregnancy reduced maternal weight gain (p = 0.03), values of the maternal glucose screen test (p = 0.002) and appears to prevent gestational diabetes. | Perception of effort (Borg scale) Heart rate monitor (Accurex Plus, Polar Electro OY). Blood glucose level (blood test) |
| Cordero et al. [23] | Assess the effectiveness of a maternal exercise program (land/aquatic activities) in preventing gestational diabetes mellitus. | EG = 100 CG = 146 | EG = 33.6 ± 4.1 CG = 32.9 ± 4.5 | 10th–12th | EG = aerobic activities (land) + resistance activities (water) CG = Routine prenatal care | EG = 26–30/2 + 1/50–60 CG = NR | EG = 81.96% GC = 66.36% | The prevalence of GDM was reduced in the EG group (EG, 1%, n = 1, vs. CG, 8.8%, n = 13 (p = 0.009)). Exercise on land and in water reduced the incidence of DMG is associated with a decreased gestational weight gain and conserved glucose tolerance | Perception of effort (Borg scale) Heart rate monitor (Accurex Plus, Polar Electro OY) Blood glucose level (blood test) BMI (Formula QUETELET) |
| Granath et al. [24] | Evaluate and compare low back or pelvic and pain due to illness in pregnant women through terrestrial and aquatic exercises | EG = 132 CG = 134 | EG = 29.10 ± 4.50 CG = 29.10 ± 4.50 | 11th–12th | EG = Aerobic activities (water) CG = Aerobic activities (land) | EG = 28–29/1/60 CG = 28–29/1/60 | EG = 68.75% CG = 67.68% | Aerobic activities (Water) decreased low back pain related to pregnancy (p = 0.04) and sick leave (p = 0.03) more than a physical exercise program on land. Water exercises are recommended for pregnant women. | Pregnancy-related pelvic girdle pain (PLBP) Pregnancy-related low back pain (PPP) |
| Rodríguez-Blanque et al. [25] | Analyze the influence of a physical activity program in the aquatic environment on the newborn weight | EG = 65 CG = 64 | EG = 34.52 ± 4.50 CG = 33.67 ± 5.37 | 20th–37th | EG = Aerobic and resistance activities-SWEP—(water) CG = Routine prenatal care | EG = 17/3/60 CG = NR | EG = 91.42%; CG = 92.85% | The aerobic and resistance activities-SWEP—(Water) doesn’t present birth risks premature and gestation time is not altered. The SWEP has achieved a significant decrease in the weight of the newborn and a lower weight gain during pregnancy. | BMI (Formula QUETELET) Perception of effort (Borg scale) Heart Rate Monitor (Quirumed OXYM2000, London, UK) |
| Rodríguez-Blanque et al. [26] | Determine if there is an association between physical activity in the aquatic environment and sleep quality in pregnant women. | EG = 65 CG = 64 | EG = 32.12 ± 4.43 CG = 30.58 ± 4.75 | 20th–37th | EG = Aerobic and resistance activities-SWEP—(water) CG = Routine prenatal care | EG = 17/3/60 CG = NR | EG = 91.42%; CG = 92.85% | The SWEP methodology improves sleep quality, both subjectively and in terms of latency, duration and efficiency. | Evaluate BMI (Formula QUETELET) Perception of Effort (Borg scale) Heart Rate Monitor (Quirumed OXYM2000, London, UK) Evaluate self-perception (Pittsburgh Sleep Quality Index PSQI) |
| Rodríguez-Blanque et al. [27] | Determine the effect of a water exercise program on the rate of perineum intact after delivery. | EG = 65 CG = 64 | EG = 32.12 ± 4.43 CG = 30.58 ± 4.75 | 20th–37th | EG = Aerobic and resistance activities-SWEP—(water) CG = Routine prenatal care | EG = 17/3/60 CG = NR | EG = 92.82%; CG = 91.40% | The women who followed the SWEP methodology were significantly more likely to have intact perinea after childbirth. | Physical activity level (Global Physical Activity Questionnaire, GPAQ) Perception of effort (Borg scale) |
| Rodríguez-Blanque et al. [28] | Determine the duration of labor in pregnant women who completed a program of moderate physical exercise in water and subsequently presented eutocic birth. | EG = 65 CG = 64 | EG = 32.12 ± 4.43 CG = 30.58 ± 4.75 | 20th–37th | EG = Aerobic and resistance activities-SWEP—(Water) CG = Routine Prenatal Care | EG = 17/3/60 CG = NR | EG = 92.82%; CG = 91.40% | Women who exercised in water during pregnancy have a shorter duration of labor than those who did not. The difference was especially marked with respect to the duration of the first and second stages of labor (p < 0.001). | Perception of effort (Borg scale) Heart rate monitor (Quirumed OXYM2000) Total duration (minutes) of labor (Ad hoc questionnaire) |
| Sánchez García et al. [29] | Analyze the evolution of weight, gestational and postpartum, in pregnant women who perform an aquatic program. | EG = 65 CG = 64 | EG = 32.12 ± 4.43 CG = 30.58 ± 4.75 | 20th–37th | EG = Aerobic and resistance activities-SWEP—(water) CG = Routine prenatal care | EG = 17/3/60 CG: NR | EG = 93.84%; CG = 90.60% | The SWEP methodology during pregnancy helps to control gestational weight gain and weight recovery before pregnancy. | Body weight (calibrated scale) Height (calibrated metal rod) BMI (Formula QUETELET) Physical activity level (Global Physical Activity Questionnaire, GPAQ) Perception of effort (Borg scale) |
| Sillero et al. [30] | Analyze the effect of two physical activities on skin temperature in women 31 weeks pregnant. | EG = 14 CG = 14 | EG = NR CG = NR | 31st | EG = Swimming; CG = Yoga | EG = NR CG = NR | EG = 100%; CG = 100% | Significant reduction in skin temperature of pregnant mothers after aquatic activity, in the areas of the mother and belly, in case of an inadequate water temperature. Tsk values are not dangerous for the fetus. | Thermograms (T335FLIR infrared camera) |
| Smith and Michel. [31] | Evaluate the impact of a water exercise program on the perception of body image, participation in health behaviors, participation in health promotion, level of physical discomfort and mobility. | EG = 20 CG = 20 | EG = 25.10 ± 4.90 CG = 24.80 ± 5.60 | 19th | EG = Calisthenics exercise (water); CG = Normal activity of daily living | EG = 6/3/60 CG = NR | EG = 100%; CG = 100% | Water exercise can improve physical functioning, decrease maternal discomfort, improvement of the maternal body and improve health behaviors. | Body image (Prenancy Body shape Questionnaire, PBSQ) Effects of aquatic exercise (Pender’s Health Promotion Lifestyle Profile (HPLP)). Mobility (timed get up and go test) Physical discomfort (Smith’s Prenancy Discomfort Intensity Index (SPDII)) |
| Vallim et al. [32] | Analyze the quality of life (QOL) in sedentary pregnant women through aerobic physical exercises in water | EG = 31 CG = 35 | EG = 26 CG = 24 | 28th–36th | EG = Aerobic activities (Water) CG = Routine prenatal care | EG = 28–36/3/50 CG: NR | EG = 64.52% CG = 65.72% | The majority had eight or more years of schooling: 52% (EG) and 83% (CG), this difference being statistically significant (p = 0.0065). | Quality of life (Questionnaire WHOQOL-BREF) |
| Vázquez-Lara et al. [33] | Examine the effect of physical activity in the aquatic environment on hemodynamic constants in pregnant women. | EG = 18 EC = 28 | EG = 31.0 ± 4.6 CG = 29.5 ± 6.1 | 25th–27th | EG = Calisthenics exercise AEPPW (water) CG = Routine prenatal care | EG: 6/2/45 CG: NR | EG = 90% CG = 100% | An aquatic exercise programme for pregnant women (AEPPW), contributes to the hydrosaline balance, preventing the excessive increase in the usual plasma volume (p < 0.010), increasing the secretion of sodium (0.050) and reducing the arterial pressures (p < 0.050) | Blood pressure monitor (Riester, Jungingen, Germany), Calculate plasma volume (Dill y Costill’s) Blood and urine test Heart rate monitor (Polar F4, Kempele Finland)) |
| Reference | Eligibility Criteria * | Random Allocation | Concealed Allocation | Groups Similar at Baseline | Blind Participant | Blind Therapist | Blind Assessor | Follow-Up | Intention to Treat Analysis | Between-Group Comparisons | Point Measure and Variability | PEDro Score Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aguilar-Cordero et al. [17] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
| Bacchi et al. [18] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
| Bacchi et al. [19] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 |
| Barakat et al. [20] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 6 |
| Barakat et al. [21] | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 5 |
| Cordero et al. [22] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 4 |
| Cordero et al. [23] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 7 |
| Granath et al. [24] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 4 |
| Rodríguez-Blanque et al. [25] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
| Rodríguez-Blanque., et al. [26] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
| Rodríguez-Blanque et al. [27] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
| Rodríguez-Blanque et al. [28] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
| Sánchez García et al. [29] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 6 |
| Sillero et al. [30] | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 3 |
| Smith and Michel [31] | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 3 |
| Vallim et al. [32] | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 3 |
| Vázquez-Lara et al. [33] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cancela-Carral, J.M.; Blanco, B.; López-Rodríguez, A. Therapeutic Aquatic Exercise in Pregnancy: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 501. https://doi.org/10.3390/jcm11030501
Cancela-Carral JM, Blanco B, López-Rodríguez A. Therapeutic Aquatic Exercise in Pregnancy: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022; 11(3):501. https://doi.org/10.3390/jcm11030501
Chicago/Turabian StyleCancela-Carral, José Maria, Benigna Blanco, and Adriana López-Rodríguez. 2022. "Therapeutic Aquatic Exercise in Pregnancy: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 11, no. 3: 501. https://doi.org/10.3390/jcm11030501
APA StyleCancela-Carral, J. M., Blanco, B., & López-Rodríguez, A. (2022). Therapeutic Aquatic Exercise in Pregnancy: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 11(3), 501. https://doi.org/10.3390/jcm11030501