
Unraveling Pathophysiology of Takotsubo Syndrome: The Emerging Role of the Oxidative Stress’s Systemic Status
 ,
,  ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
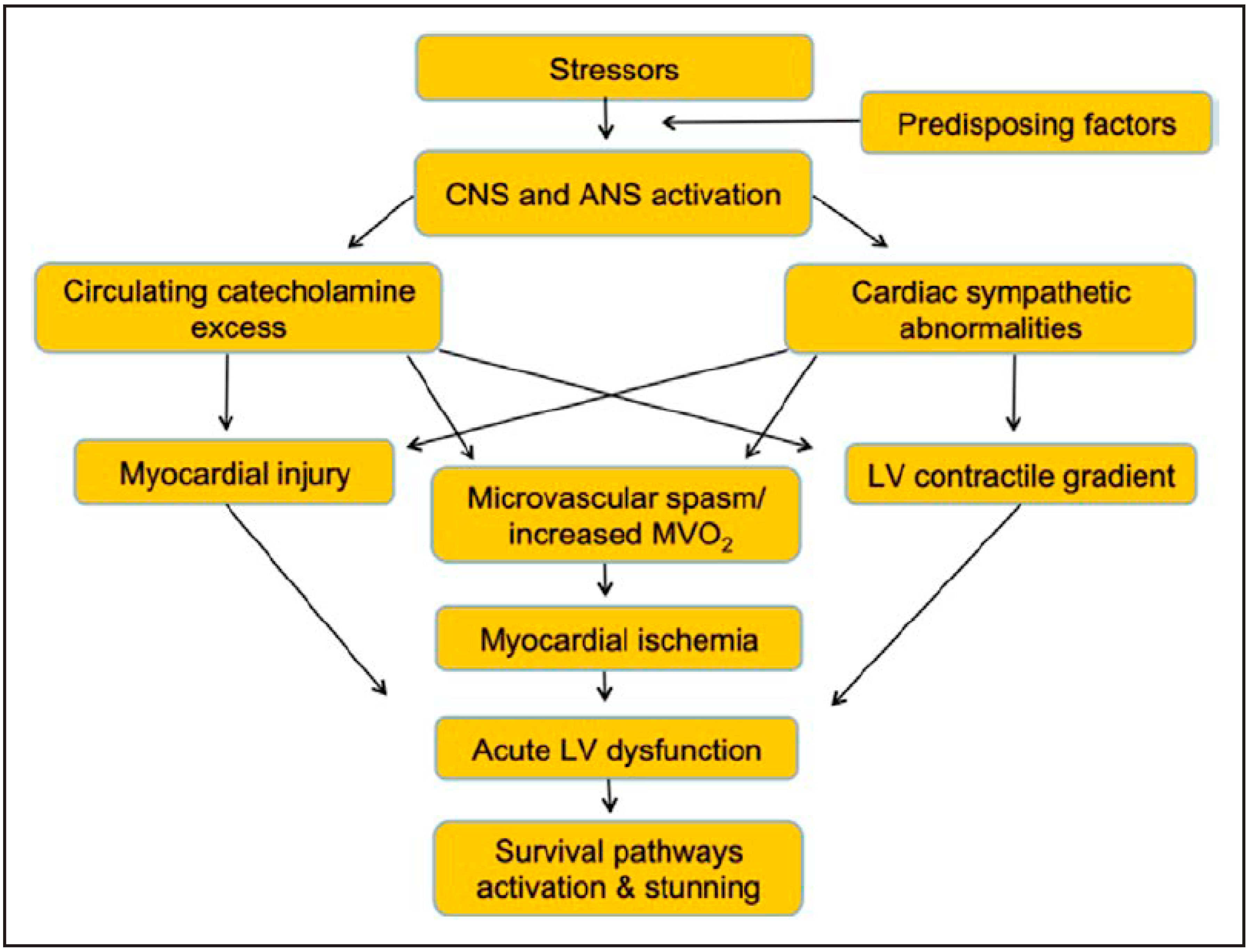
2. Established Mechanisms Underlying TTS
3. Novel Pathophysiologic Determinants of TTS
3.1. Inflammation
3.2. Genetics
3.3. Oxidative Status
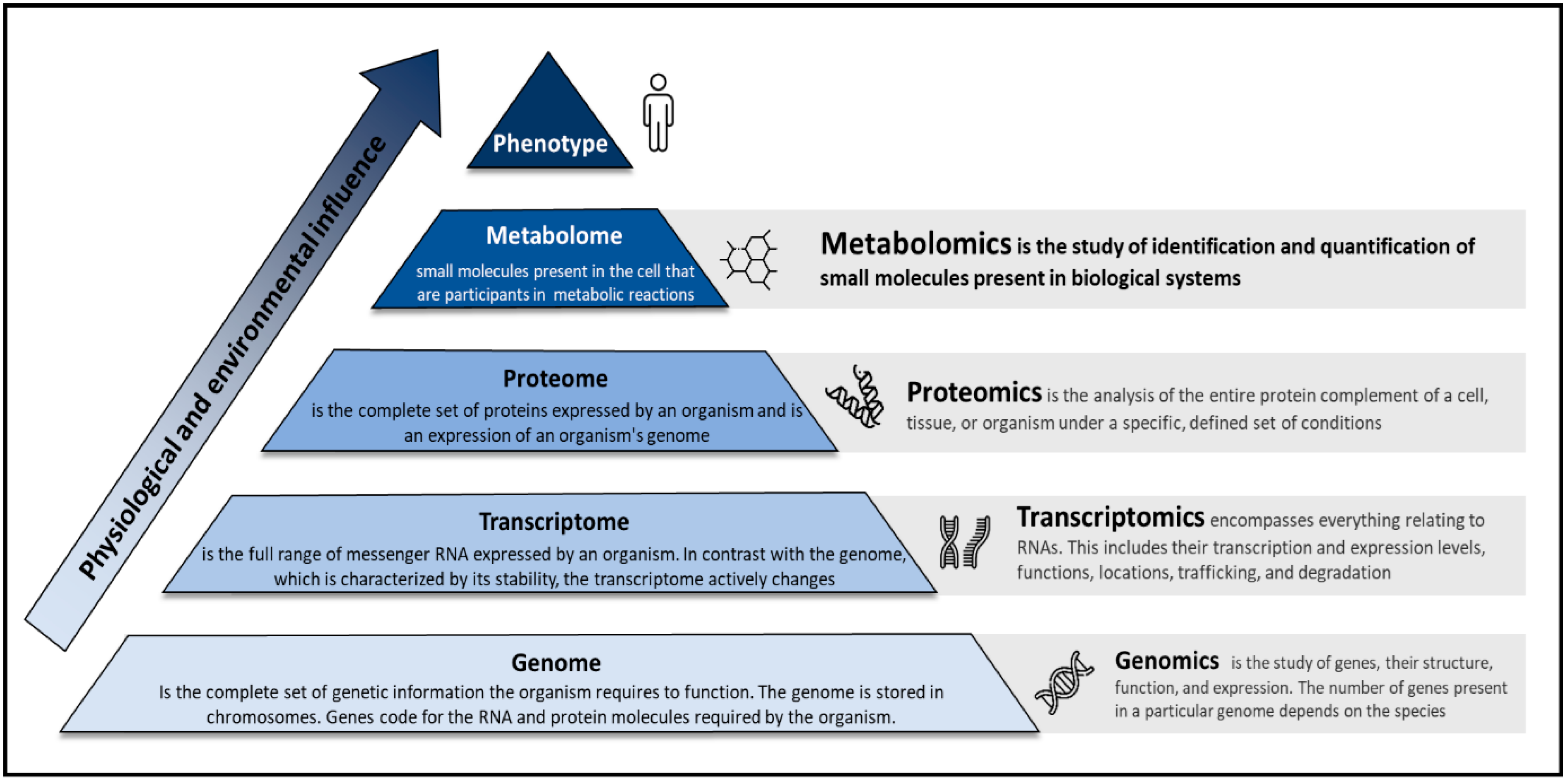
4. Metabolomics
5. The Contribution of Metabolomics in the Context of TTS
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Pelliccia, F.; Kaski, J.C.; Crea, F.; Camici, P.G. Pathophysiology of Takotsubo Syndrome. Circulation 2017, 135, 2426–2441. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, F.; Greco, C.; Vitale, C.; Rosano, G.; Gaudio, C.; Kaski, J.C. Takotsubo syndrome (stress cardiomyopathy): An intriguing clinical condition in search of its identity. Am. J. Med. 2014, 127, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, F.; Parodi, G.; Greco, C.; Antoniucci, D.; Brenner, R.; Bossone, E.; Cacciotti, L.; Capucci, A.; Citro, R.; Delmas, C.; et al. Comorbidities frequency in takotsubo syndrome: An international collaborative systematic review including 1109 patients. Am. J. Med. 2015, 128, 654.e11–654.e19. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Carson, K.; Shah, R.; Sawhney, G.; Singh, B.; Parsaik, A.; Gilutz, H.; Usmani, Z.; Horowitz, J. Meta-Analysis of Clinical Correlates of Acute Mortality in Takotsubo Cardiomyopathy. Am. J. Cardiol. 2014, 113, 1420–1428. [Google Scholar] [CrossRef]
- Pelliccia, F.; Sinagra, G.; Elliott, P.; Parodi, G.; Basso, C.; Camici, P.G. Takotsubo is not a cardiomyopathy. Int. J. Cardiol. 2018, 254, 250–253. [Google Scholar] [CrossRef]
- Ghadri, J.-R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part I): Clinical Characteristics, Diagnostic Criteria, and Pathophysiology. Eur. Heart J. 2018, 39, 2032–2046. [Google Scholar] [CrossRef]
- Ghadri, J.-R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International Expert Consensus Document on Takotsubo Syndrome (Part II): Diagnostic Workup, Outcome, and Management. Eur. Heart J. 2018, 39, 2047–2062. [Google Scholar] [CrossRef]
- Roncella, A.; Pristipino, C.; Cianfrocca, C.; Scorza, S.; Pasceri, V.; Pelliccia, F.; Denollet, J.; Pedersen, S.S.; Speciale, G. One-year results of the randomized, controlled, short-term psychotherapy in acute myocardial infarction (STEP-IN-AMI) trial. Int. J. Cardiol. 2013, 170, 132–139. [Google Scholar] [CrossRef]
- Pelliccia, F.; Pasceri, V.; Limongelli, G.; Autore, C.; Basso, C.; Corrado, D.; Imazio, M.; Rapezzi, C.; Sinagra, G.; Mercuro, G. Long-term outcome of nonobstructive versus obstructive hypertrophic cardiomyopathy: A systematic review and meta-analysis. Int. J. Cardiol. 2017, 243, 379–384. [Google Scholar] [CrossRef]
- Angelini, P. Transient left ventricular apical ballooning: A unifying pathophysiologic theory at the edge of Prinzmetal angina. Catheter. Cardiovasc. Interv. 2008, 71, 342–352. [Google Scholar] [CrossRef]
- Angelini, P. Midventricular variant of transient apical ballooning: A likely demonstration of its pathophysiologic mechanism. Mayo Clin. Proc. 2009, 84, 92–93. [Google Scholar] [CrossRef] [PubMed]
- Marazzi, G.; Wajngarten, M.; Vitale, C.; Patrizi, R.; Pelliccia, F.; Gebara, O.; Pierri, H.; Ramires, J.A.F.; Volterrani, M.; Fini, M.; et al. Effect of free fatty acid inhibition on silent and symptomatic myocardial ischemia in diabetic patients with coronary artery disease. Int. J. Cardiol. 2007, 120, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Aimo, A.; Pelliccia, F.; Panichella, G.; Vergaro, G.; Barison, A.; Passino, C.; Emdin, M.; Camici, P.G. Indications of beta-adrenoceptor blockers in Takotsubo syndrome and theoretical reasons to prefer agents with vasodilating activity. Int. J. Cardiol. 2021, 333, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, F.; Trani, C.; Biondi-Zoccai, G.G.; Nazzaro, M.; Berni, A.; Patti, G.; Patrizi, R.; Pironi, B.; Mazzarotto, P.; Gioffrè, G.; et al. Comparison of the Feasibility and Effectiveness of Transradial Coronary Angiography Via Right Versus Left Radial Artery Approaches (from the PREVAIL Study). Am. J. Cardiol. 2012, 110, 771–775. [Google Scholar] [CrossRef]
- Pelliccia, F.; Pasceri, V.; Marazzi, G.; Rosano, G.; Greco, C.; Gaudio, C. A pilot randomized study of ranolazine for reduction of myocardial damage during elective percutaneous coronary intervention. Am. Heart J. 2012, 163, 1019–1023. [Google Scholar] [CrossRef]
- Templin, C.; Ghadri, J.R.; Diekmann, J.; Napp, L.C.; Bataiosu, D.R.; Jaguszewski, M.; Cammann, V.L.; Sarcon, A.; Geyer, V.; Neumann, C.A.; et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. N. Engl. J. Med. 2015, 373, 929–938. [Google Scholar] [CrossRef]
- Marazzi, G.; Campolongo, G.; Pelliccia, F.; Calabrò, P.; Cacciotti, L.; Vitale, C.; Massaro, R.; Volterrani, M.; Rosano, G. Usefulness of Low-Dose Statin Plus Ezetimibe and/or Nutraceuticals in Patients with Coronary Artery Disease Intolerant to High-Dose Statin Treatment. Am. J. Cardiol. 2018, 123, 233–238. [Google Scholar] [CrossRef]
- Pelliccia, F.; Patti, G.; Rosano, G.; Greco, C.; Gaudio, C. Efficacy and safety of eplerenone in the management of mild to moderate arterial hypertension: Systematic review and meta-analysis. Int. J. Cardiol. 2014, 177, 219–228. [Google Scholar] [CrossRef]
- Dias, A.; Gil, I.J.N.; Santoro, F.; Madias, J.E.; Pelliccia, F.; Brunetti, N.D.; Salmoirago-Blotcher, E.; Sharkey, S.W.; Eitel, I.; Akashi, Y.J.; et al. Takotsubo syndrome: State-of-the-art review by an expert panel—Part 1. Cardiovasc. Revascularization Med. 2018, 20, 70–79. [Google Scholar] [CrossRef]
- Dias, A.; Gil, I.J.N.; Santoro, F.; Madias, J.E.; Pelliccia, F.; Brunetti, N.D.; Salmoirago-Blotcher, E.; Sharkey, S.W.; Eitel, I.; Akashi, Y.J.; et al. Takotsubo syndrome: State-of-the-art review by an expert panel—Part 2. Cardiovasc. Revascularization Med. 2018, 20, 153–166. [Google Scholar] [CrossRef]
- Crossman, A.R.; Neary, D. Neuroanatomy, 2nd ed.; Churchill Livingston: London, UK, 2000. [Google Scholar]
- Janig, W. The Integrative Action of the Autonomic Nervous System; Cambridge University Press: Cambridge, UK, 2006. [Google Scholar]
- Angelini, P.; Uribe, C.; Tobis, J.M. Pathophysiology of Takotsubo Cardiomyopathy: Reopened Debate. Tex. Heart Inst. J. 2021, 48, e207490. [Google Scholar] [CrossRef] [PubMed]
- Crea, F.; Camici, P.G.; Merz, C.N.B. Coronary microvascular dysfunction: An update. Eur. Heart J. 2013, 35, 1101–1111. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, F.; Kaski, J.C.; Camici, P.G. Takotsubo syndrome’s pathophysiology: Still a mystery? Eur. Heart J. 2019, 40, 1989. [Google Scholar] [CrossRef] [PubMed]
- Scally, C.; Abbas, H.; Ahearn, T.; Srinivasan, J.; Mezincescu, A.; Rudd, A.; Spath, N.; Yucel-Finn, A.; Yuecel, R.; Oldroyd, K.; et al. Myocardial and Systemic Inflammation in Acute Stress-Induced (Takotsubo) Cardiomyopathy. Circulation 2019, 139, 1581–1592. [Google Scholar] [CrossRef]
- Pelliccia, F.; Morgantini, A.; Rosati, R. Takotsubo Syndrome: From Bench to Bedside and Bedside to Bench. J. Clin. Med. 2022, 11, 4704. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, F.; Camici, P.G. Unrevealing Takotsubo Syndrome: Appraising what has emerged from the International Journal of Cardiology contributions in 2019. Int J Cardiol. 2020, 302, 131–133. [Google Scholar] [CrossRef] [PubMed]
- Y-Hassan, S. Myocarditis and takotsubo syndrome: Are they mutually exclusive? Int. J. Cardiol. 2014, 177, 149–151. [Google Scholar] [CrossRef]
- Y-Hassan, S. Myocarditis is an essential feature rather than an exclusion criterion for takotsubo syndrome: Case report. Int. J. Cardiol. 2015, 187, 304–306. [Google Scholar] [CrossRef]
- Limongelli, G.; Masarone, D.; Maddaloni, V.; Rubino, M.; Fratta, F.; Cirillo, A.; Ludovica, S.B.; Pacileo, R.; Fusco, A.; Coppola, G.R.; et al. Genetics of Takotsubo Syndrome. Heart Fail. Clin. 2016, 12, 499–506. [Google Scholar] [CrossRef]
- Spinelli, L.; Trimarco, V.; Di Marino, S.; Marino, M.; Iaccarino, G.; Trimarco, B. L41Q polymorphism of the G protein coupled receptor kinase 5 is associated with left ventricular apical ballooning syndrome. Eur. J. Heart Fail. 2009, 12, 13–16. [Google Scholar] [CrossRef]
- Figtree, G.A.; Bagnall, R.D.; Abdulla, I.; Buchholz, S.; Galougahi, K.K.; Yan, W.; Tan, T.; Neil, C.; Horowitz, J.D.; Semsarian, C.; et al. No association of G-protein-coupled receptor kinase 5 or beta-adrenergic receptor polymorphisms with Takotsubo cardiomyopathy in a large Australian cohort. Eur. J. Heart Fail. 2013, 15, 730–733. [Google Scholar] [CrossRef] [PubMed]
- Mattsson, E.; Saliba-Gustafsson, P.; Ehrenborg, E.; Tornvall, P. Lack of genetic susceptibility in takotsubo cardiomyopathy: A case-control study. BMC Med. Genet. 2018, 19, 39. [Google Scholar] [CrossRef] [PubMed]
- Nef, H.M.; Möllmann, H.; Troidl, C.; Kostin, S.; Voss, S.; Hilpert, P.; Behrens, C.B.; Rolf, A.; Rixe, J.; Weber, M.; et al. Abnormalities in intracellular Ca2+ regulation contribute to the pathomechanism of Tako-Tsubo cardiomyopathy. Eur. Heart J. 2009, 30, 2155–2164. [Google Scholar] [CrossRef] [PubMed]
- Kołodzińska, A.; Czarzasta, K.; Szczepankiewicz, B.; Główczyńska, R.; Fojt, A.; Ilczuk, T.; Budnik, M.; Krasuski, K.; Folta, M.; Cudnoch-Jędrzejewska, A.; et al. Toll-like receptor expression and apoptosis morphological patterns in female rat hearts with takotsubo syndrome induced by isoprenaline. Life Sci. 2018, 199, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Ueyama, T.; Yamamoto, Y.; Ueda, K.; Kawabe, T.; Hano, T.; Ito, T.; Tsuruo, Y.; Ichinose, M.; Yoshida, K.-I. Cardiac and vascular gene profiles in an animal model of takotsubo cardiomyopathy. Heart Vessel. 2011, 26, 321–337. [Google Scholar] [CrossRef]
- Redfors, B.; Shao, Y.; Ali, A.; Omerovic, E. Are ischemic stunning, conditioning, and ‘takotsubo’ different sides to the same coin? Int J. Cardiol. 2014, 172, 490–491. [Google Scholar] [CrossRef]
- Pelliccia, F.; Pasceri, V.; Niccoli, G.; Tanzilli, G.; Speciale, G.; Gaudio, C.; Crea, F.; Camici, P.G. Predictors of Mortality in Myocardial Infarction and Nonobstructed Coronary Arteries: A Systematic Review and Meta-Regression. Am. J. Med. 2020, 133, 73–83.e4. [Google Scholar] [CrossRef]
- Eitel, I.; Moeller, C.; Munz, M.; Stiermaier, T.; Meitinger, T.; Thiele, H.; Erdmann, J. Genome-wide association study in takotsubo syndrome—Preliminary results and future directions. Int. J. Cardiol. 2017, 236, 335–339. [Google Scholar] [CrossRef]
- Golbidi, S.; Li, H.; Laher, I. Oxidative Stress: A Unifying Mechanism for Cell Damage Induced by Noise, (Water-Pipe) Smoking, and Emotional Stress—Therapeutic Strategies Targeting Redox Imbalance. Antioxid. Redox Signal. 2018, 28, 741–759. [Google Scholar] [CrossRef]
- Black, C.N.; Bot, M.; Révész, D.; Scheffer, P.G.; Penninx, B. The association between three major physiological stress systems and oxidative DNA and lipid damage. Psychoneuroendocrinology 2017, 80, 56–66. [Google Scholar] [CrossRef]
- Odnoshivkina, U.G.; Sytchev, V.I.; Nurullin, L.F.; Giniatullin, A.R.; Zefirov, A.L.; Petrov, A.M. β2-adrenoceptor agonist-evoked reactive oxygen species generation in mouse atria: Implication in delayed inotropic effect. Eur. J. Pharmacol. 2015, 765, 140–153. [Google Scholar] [CrossRef] [PubMed]
- Tanzilli, G.; Truscelli, G.; Arrivi, A.; Carnevale, R.; Placanica, A.; Viceconte, N.; Raparelli, V.; Mele, R.; Cammisotto, V.; Nocella, C.; et al. Glutathione infusion before primary percutaneous coronary intervention: A randomised controlled pilot study. BMJ Open 2019, 9, e025884. [Google Scholar] [CrossRef] [PubMed]
- Marazzi, G.; Pelliccia, F.; Campolongo, G.; Quattrino, S.; Cacciotti, L.; Volterrani, M.; Gaudio, C.; Rosano, G. Usefulness of Nutraceuticals (Armolipid Plus) Versus Ezetimibe and Combination in Statin-Intolerant Patients with Dyslipidemia with Coronary Heart Disease. Am. J. Cardiol. 2015, 116, 1798–1801. [Google Scholar] [CrossRef] [PubMed]
- Oliver, S.G.; Winson, M.K.; Kell, D.B.; Baganz, F. Systematic functional analysis of the yeast genome. Trends Biotechnol. 1998, 16, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Van Der Greef, J.; Van Wietmarschen, H.; Van Ommen, B.; Verheij, E. Looking back into the future: 30 years of metabolomics at TNO. Mass Spectrom. Rev. 2013, 32, 399–415. [Google Scholar] [CrossRef] [PubMed]
- Limongelli, G.; Adorisio, R.; Baggio, C.; Bauce, B.; Biagini, E.; Castelletti, S.; Favilli, S.; Imazio, M.; Lioncino, M.; Merlo, M.; et al. Diagnosis and Management of Rare Cardiomyopathies in Adult and Paediatric Patients. A Position Paper of the Italian Society of Cardiology (SIC) and Italian Society of Paediatric Cardiology (SICP). Int. J. Cardiol. 2022, 357, 55–71. [Google Scholar] [CrossRef]
- Wishart, D.S.; Guo, A.; Oler, E.; Wang, F.; Anjum, A.; Peters, H.; Dizon, R.; Sayeeda, Z.; Tian, S.; Lee, B.L.; et al. HMDB 5.0: The Human Metabolome Database for 2022. Nucleic Acids Res. 2022, 50, D622–D631. [Google Scholar] [CrossRef]
- Jones, O.A.H. Illuminating the dark metabolome to advance the molecular characterisation of biological systems. Metabolomics 2018, 14, 101. [Google Scholar] [CrossRef]
- Botstein, D.; Risch, N. Discovering genotypes underlying human phenotypes: Past successes for mendelian disease, future approaches for complex disease. Nat. Genet. 2003, 33, 228–237. [Google Scholar] [CrossRef]
- E Stranger, B.; A Stahl, E.; Raj, T. Progress and Promise of Genome-Wide Association Studies for Human Complex Trait Genetics. Genetics 2011, 187, 367–383. [Google Scholar] [CrossRef]
- Rattray, N.J.W.; DeZiel, N.C.; Wallach, J.D.; Khan, S.A.; Vasiliou, V.; Ioannidis, J.P.A.; Johnson, C.H. Beyond genomics: Understanding exposotypes through metabolomics. Hum. Genom. 2018, 12, 4. [Google Scholar] [CrossRef] [PubMed]
- Rappaport, S.M.; Barupal, D.; Wishart, D.S.; Vineis, P.; Scalbert, A. The Blood Exposome and Its Role in Discovering Causes of Disease. Environ. Health Perspect. 2014, 122, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Mokdad, A.H.; Marks, J.S.; Stroup, D.F.; Gerberding, J.L. Actual Causes of Death in the United States, 2000. JAMA 2004, 291, 1238–1245. [Google Scholar] [CrossRef]
- Scalbert, A.; Brennan, L.; Manach, C.; Andres-Lacueva, C.; O Dragsted, L.; Draper, J.; Rappaport, S.M.; van der Hooft, J.J.; Wishart, D.S. The food metabolome: A window over dietary exposure. Am. J. Clin. Nutr. 2014, 99, 1286–1308. [Google Scholar] [CrossRef] [PubMed]
- Wild, C.P.; Scalbert, A.; Herceg, Z. Measuring the exposome: A powerful basis for evaluating environmental exposures and cancer risk. Environ. Mol. Mutagen. 2013, 54, 480–499. [Google Scholar] [CrossRef]
- Di Marino, S.; Viceconte, G.N.; Lembo, A.; Summa, V.; Tanzilli, G.; Raparelli, V.; Truscelli, G.; Mangieri, E.; Gaudio, C.; Cicero, D.O. Early metabolic response to acute myocardial ischaemia in patients undergoing elective coronary angioplasty. Open Heart 2018, 5, e000709. [Google Scholar] [CrossRef]
- Godsman, N.; Kohlhaas, M.; Nickel, A.; Cheyne, L.; Mingarelli, M.; Schweiger, L.; Hepburn, C.; Munts, C.; Welch, A.; Delibegovic, M.; et al. Metabolic alterations in a rat model of takotsubo syndrome. Cardiovasc. Res. 2021, 118, 1932–1946. [Google Scholar] [CrossRef]
- Nuñez-Gil, I.; Andrés, M.; Benito, B.; Bernardo, E.; Vedia, O.; Ferreira-Gonzalez, I.; Barba, I. Serum Metabolomic Analysis Suggests Impairment of Myocardial Energy Production in Takotsubo Syndrome. Metabolites 2021, 11, 439. [Google Scholar] [CrossRef]
- Karnati, S.; Guntas, G.; Rajendran, R.; Shityakov, S.; Höring, M.; Liebisch, G.; Kosanovic, D.; Ergün, S.; Nagai, M.; Förster, C.Y. Quantitative Lipidomic Analysis of Takotsubo Syndrome Patients’ Serum. Front. Cardiovasc. Med. 2022, 9, 797154. [Google Scholar] [CrossRef]
- Zeng, C.; Wen, B.; Hou, G.; Lei, L.; Mei, Z.; Jia, X.; Chen, X.; Zhu, W.; Li, J.; Kuang, Y.; et al. Lipidomics profiling reveals the role of glycerophospholipid metabolism in psoriasis. Gigascience 2017, 6, 1–11. [Google Scholar] [CrossRef]
- Wilson, H.M.; Cheyne, L.; Brown, P.A.; Kerr, K.; Hannah, A.; Srinivasan, J.; Duniak, N.; Horgan, G.; Dawson, D.K. Characterization of the Myocardial Inflammatory Response in Acute Stress-Induced (Takotsubo) Cardiomyopathy. JACC Basic Transl. Sci. 2018, 3, 766–778. [Google Scholar] [CrossRef] [PubMed]
- Weber, C.; Noels, H. Atherosclerosis: Current pathogenesis and therapeutic options. Nat. Med. 2011, 17, 1410–1422. [Google Scholar] [CrossRef] [PubMed]
- Ittner, C.; Burek, M.; Störk, S.; Nagai, M.; Förster, C.Y. Increased Catecholamine Levels and Inflammatory Mediators Alter Barrier Properties of Brain Microvascular Endothelial Cells in vitro. Front. Cardiovasc. Med. 2020, 7, 73. [Google Scholar] [CrossRef] [PubMed]
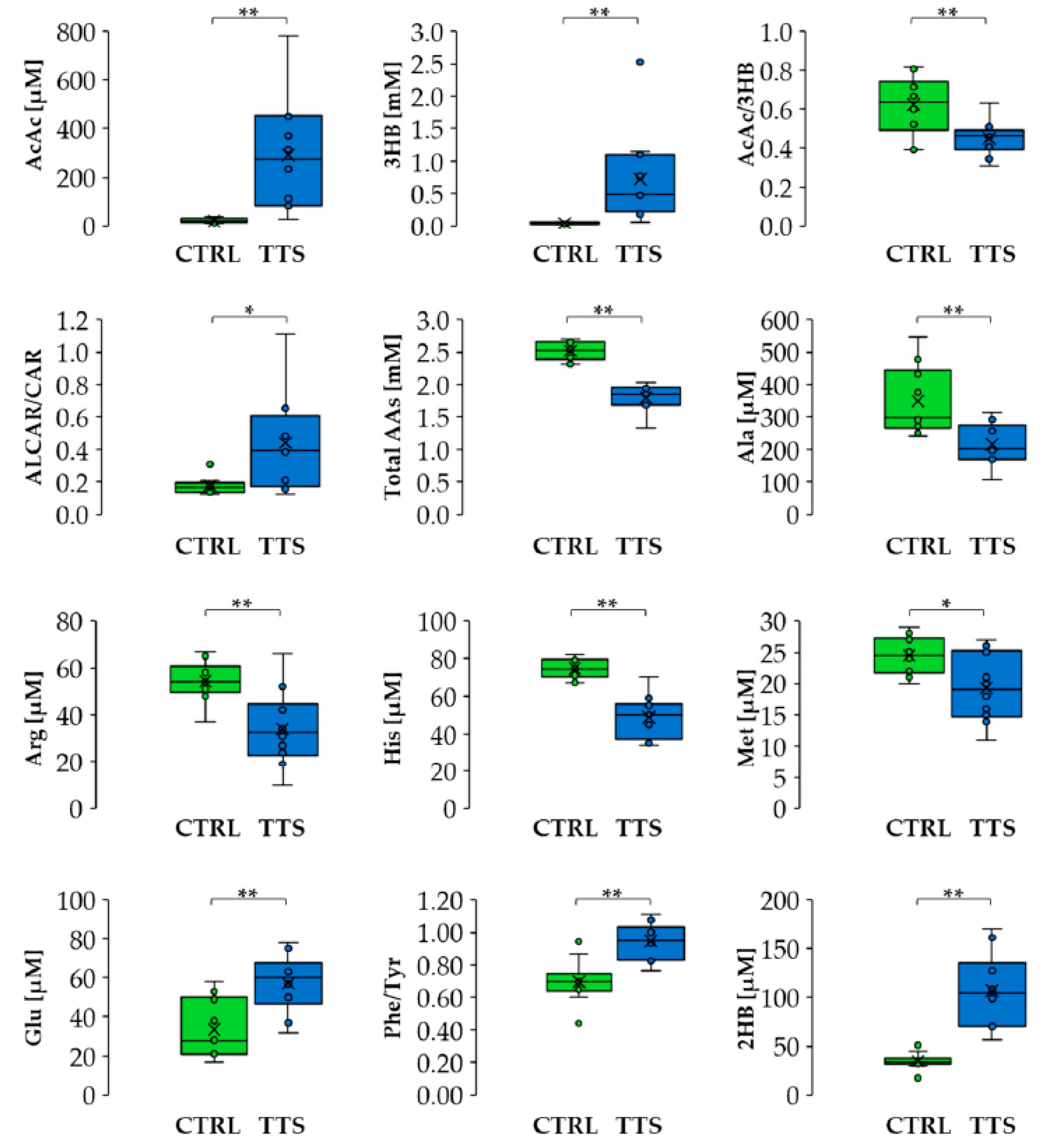
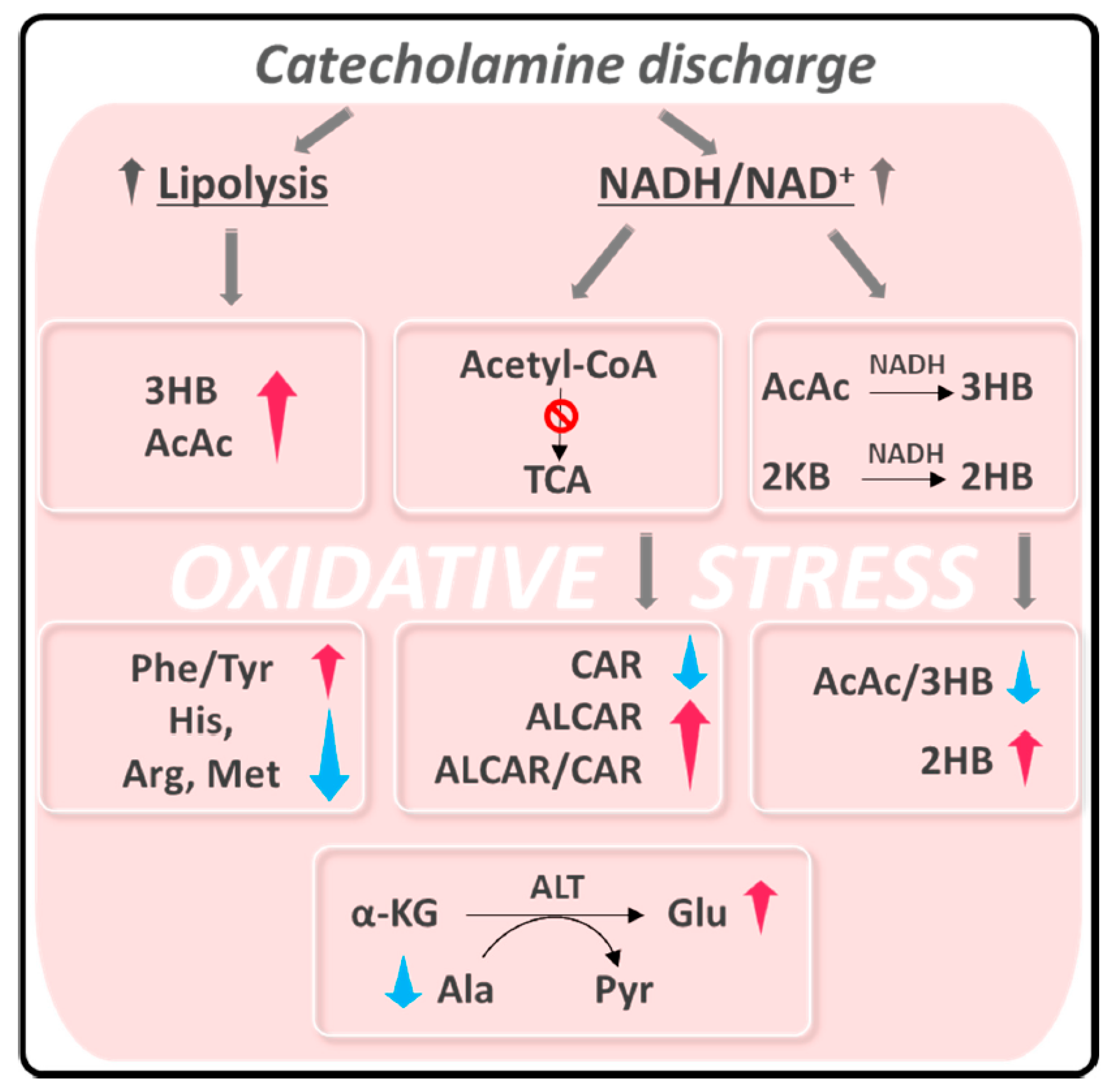
- Vanni, D.; Viceconte, N.; Petrella, G.; Biccirè, F.G.; Pelliccia, F.; Tanzilli, G.; Cicero, D.O. A Pilot Study on the 1H-NMR Serum Metabolic Profile of Takotsubo Patients Reveals Systemic Response to Oxidative Stress. Antioxidants 2021, 10, 1982. [Google Scholar] [CrossRef] [PubMed]
- Hakuno, D.; Hamba, Y.; Toya, T.; Adachi, T. Plasma Amino Acid Profiling Identifies Specific Amino Acid Associations with Cardiovascular Function in Patients with Systolic Heart Failure. PLoS ONE 2015, 10, e0117325. [Google Scholar] [CrossRef]
- Ong, G.J.; Nguyen, T.H.; Kucia, A.; Liu, S.-F.; Surikow, S.Y.; Girolamo, O.; Chong, C.-R.; Chirkov, Y.Y.; Schenck-Gustafsson, K.; Frenneaux, M.P.; et al. Takotsubo Syndrome: Finally Emerging From the Shadows? Heart Lung Circ. 2020, 30, 36–44. [Google Scholar] [CrossRef]
- Siegrist, J.; Sies, H. Disturbed Redox Homeostasis in Oxidative Distress. Circ. Res. 2017, 121, 103–105. [Google Scholar] [CrossRef]
- Morel, O.; Sauer, F.; Imperiale, A.; Cimarelli, S.; Blondet, C.; Jesel, L.; Trinh, A.; De Poli, F.; Ohlmann, P.; Constantinesco, A.; et al. Importance of Inflammation and Neurohumoral Activation in Takotsubo Cardiomyopathy. J. Card. Fail. 2009, 15, 206–213. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viceconte, N.; Petrella, G.; Pelliccia, F.; Tanzilli, G.; Cicero, D.O. Unraveling Pathophysiology of Takotsubo Syndrome: The Emerging Role of the Oxidative Stress’s Systemic Status. J. Clin. Med. 2022, 11, 7515. https://doi.org/10.3390/jcm11247515
Viceconte N, Petrella G, Pelliccia F, Tanzilli G, Cicero DO. Unraveling Pathophysiology of Takotsubo Syndrome: The Emerging Role of the Oxidative Stress’s Systemic Status. Journal of Clinical Medicine. 2022; 11(24):7515. https://doi.org/10.3390/jcm11247515
Chicago/Turabian StyleViceconte, Nicola, Greta Petrella, Francesco Pelliccia, Gaetano Tanzilli, and Daniel Oscar Cicero. 2022. "Unraveling Pathophysiology of Takotsubo Syndrome: The Emerging Role of the Oxidative Stress’s Systemic Status" Journal of Clinical Medicine 11, no. 24: 7515. https://doi.org/10.3390/jcm11247515
APA StyleViceconte, N., Petrella, G., Pelliccia, F., Tanzilli, G., & Cicero, D. O. (2022). Unraveling Pathophysiology of Takotsubo Syndrome: The Emerging Role of the Oxidative Stress’s Systemic Status. Journal of Clinical Medicine, 11(24), 7515. https://doi.org/10.3390/jcm11247515