

Implant or Tooth?—A Prospective Clinical Study on Oral Health-Related Quality of Life for Patients with “Unrestorable” Teeth

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Interventions
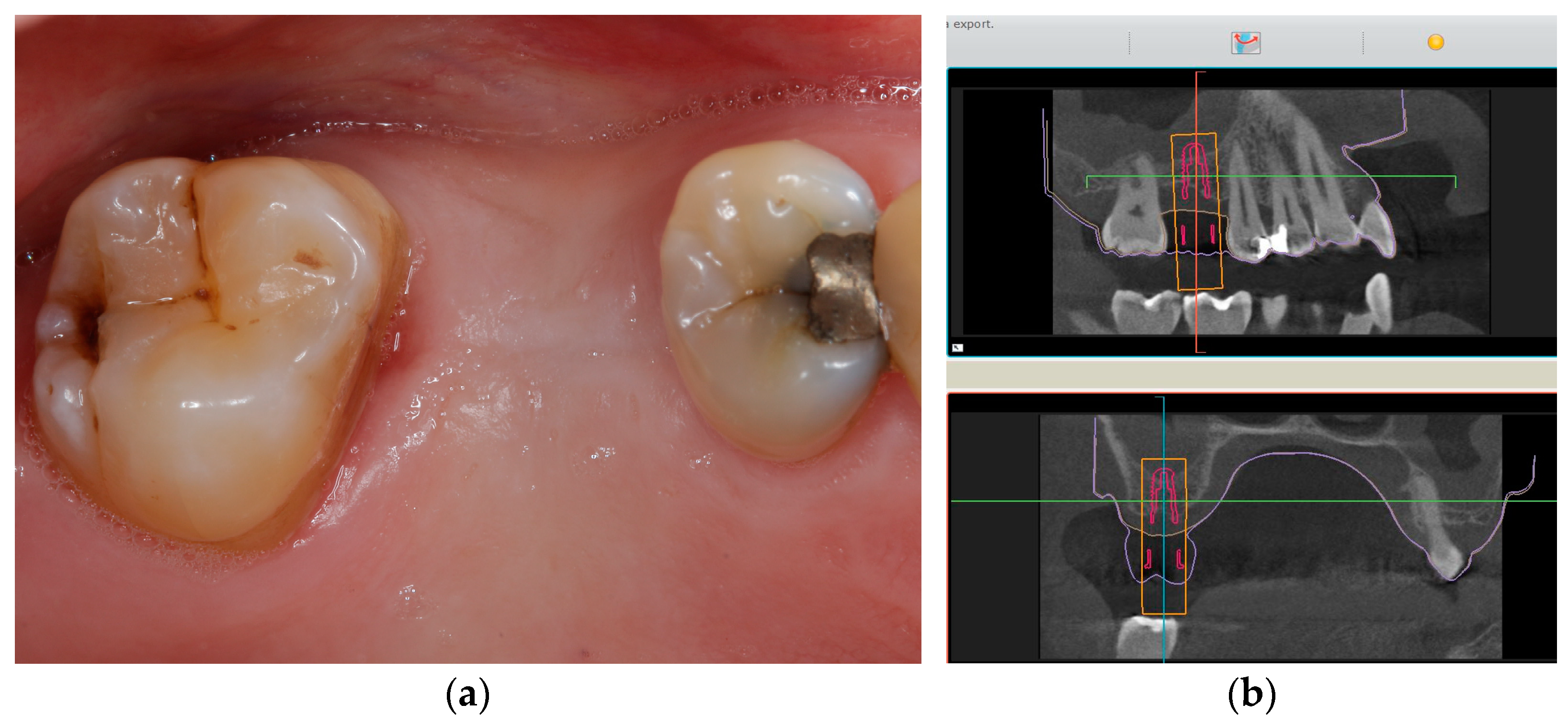
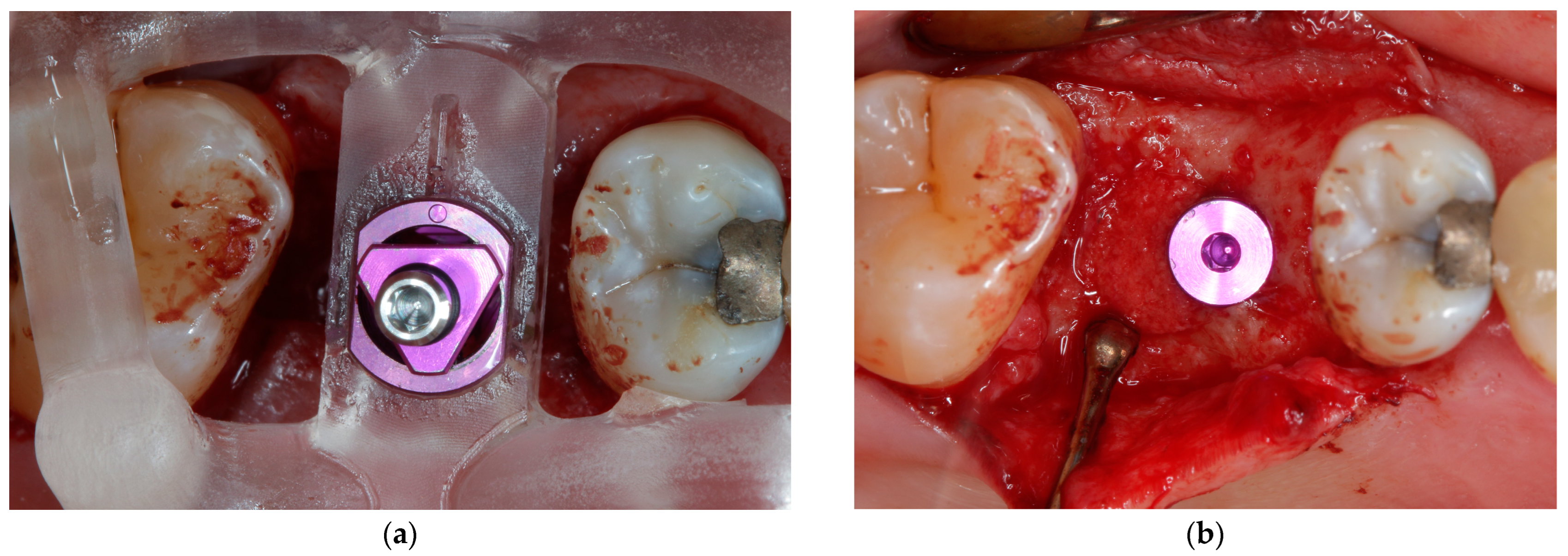
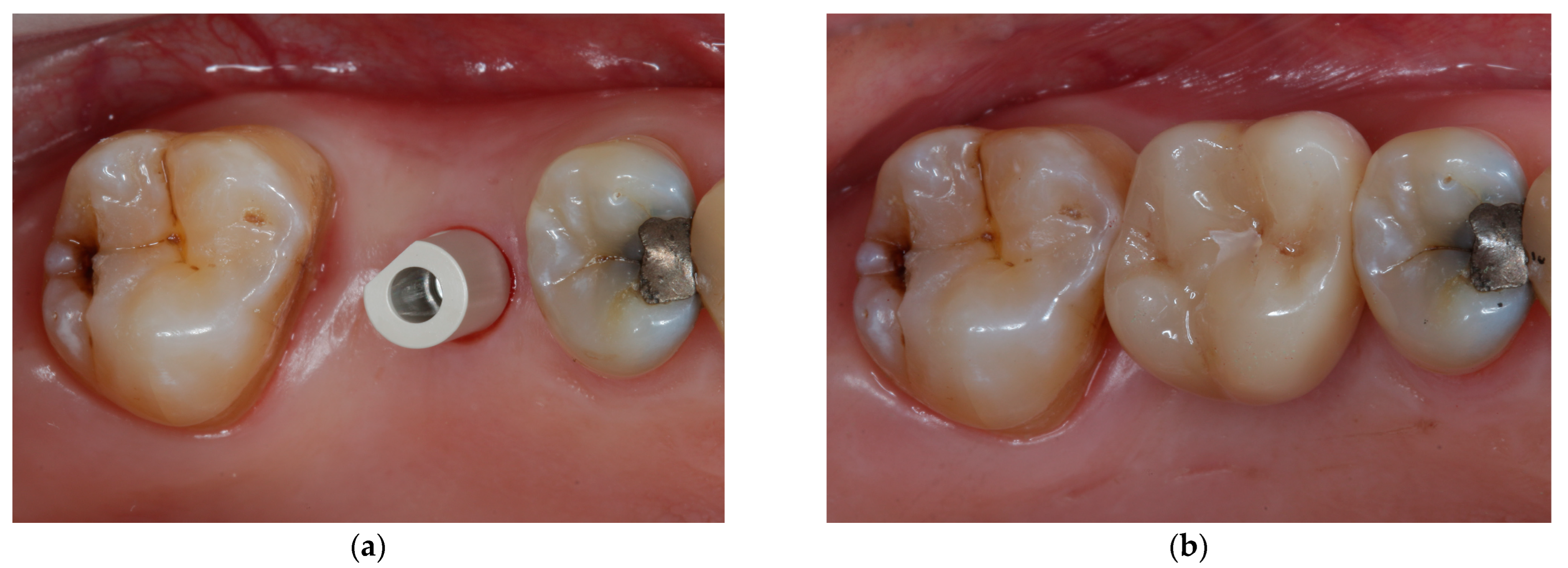
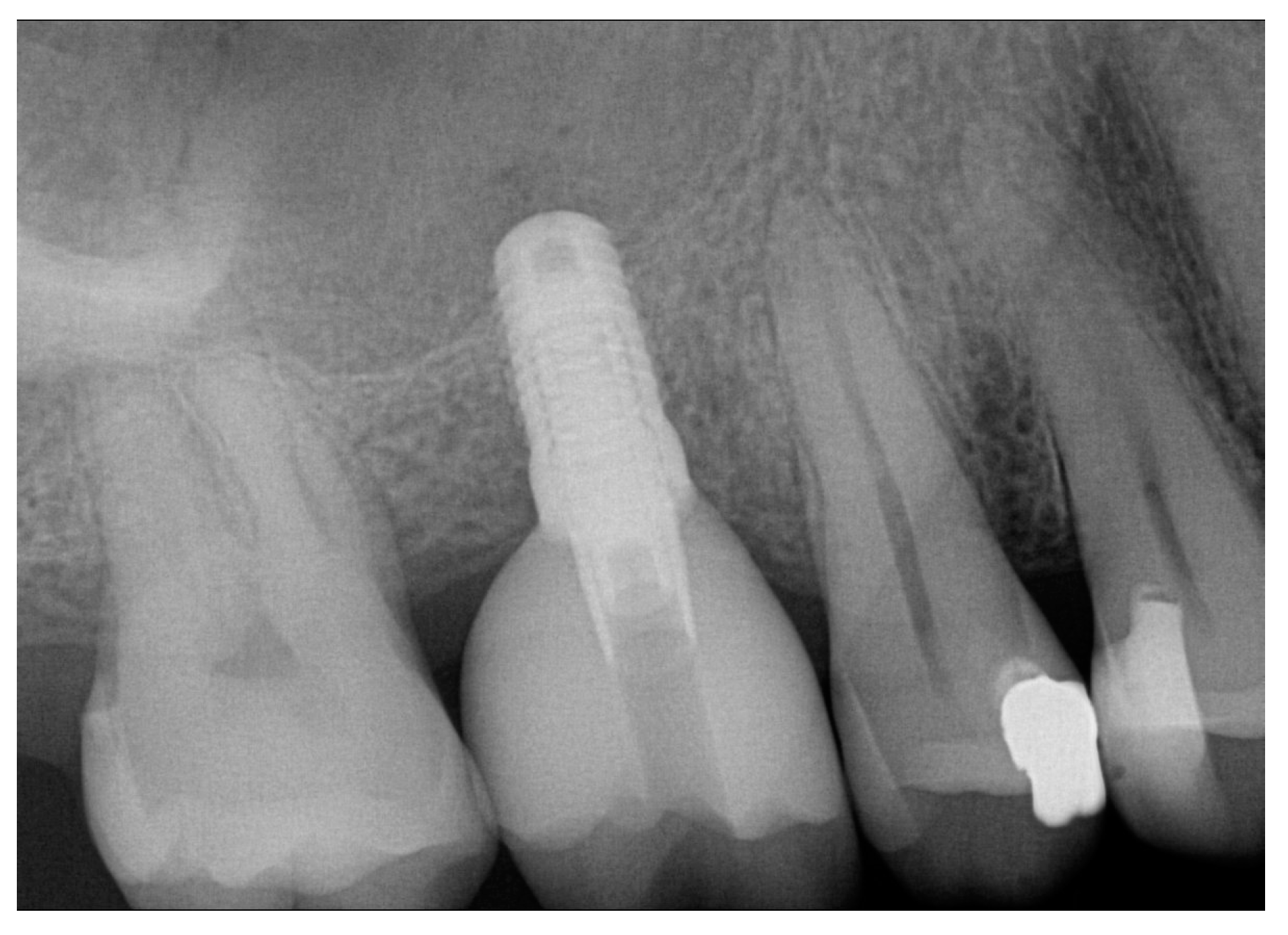
2.2.1. Implant-Supported Single Crown Treatment (ISC)
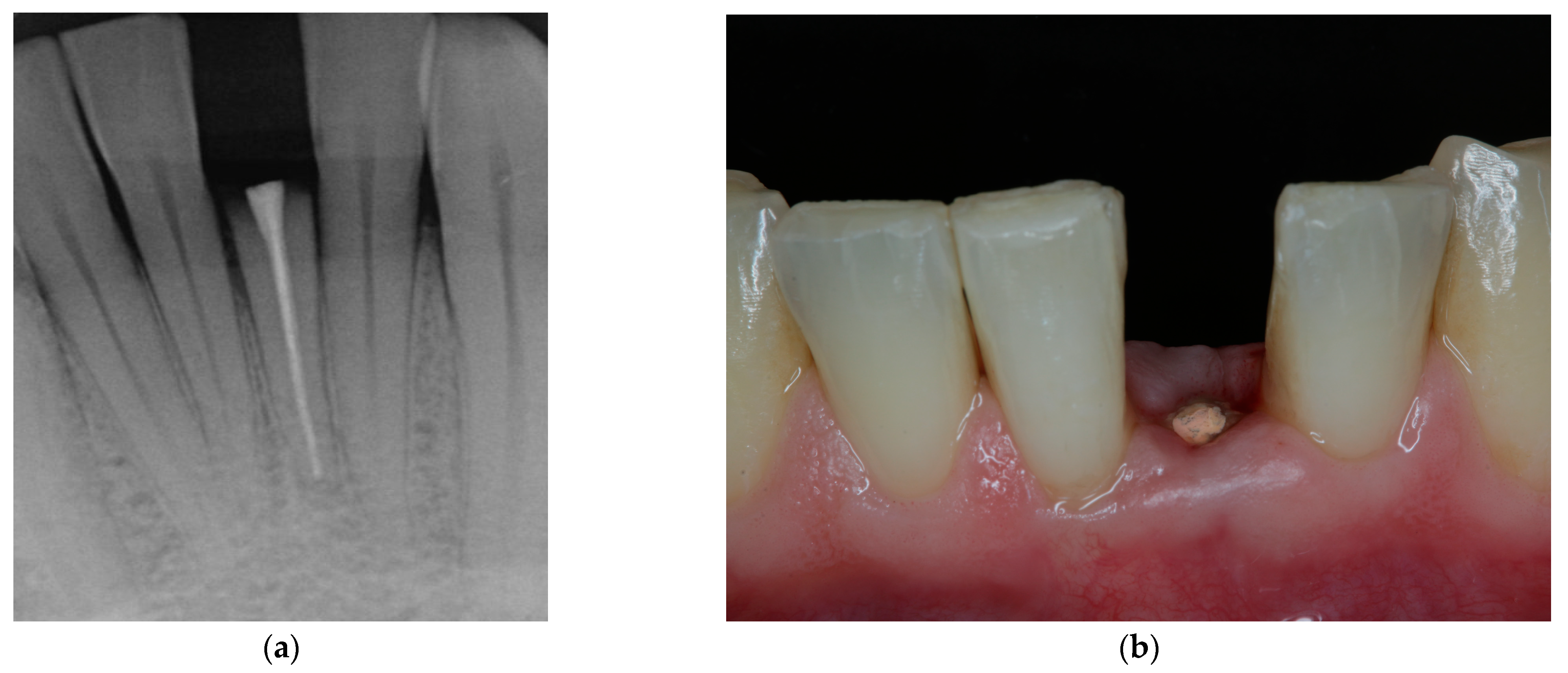
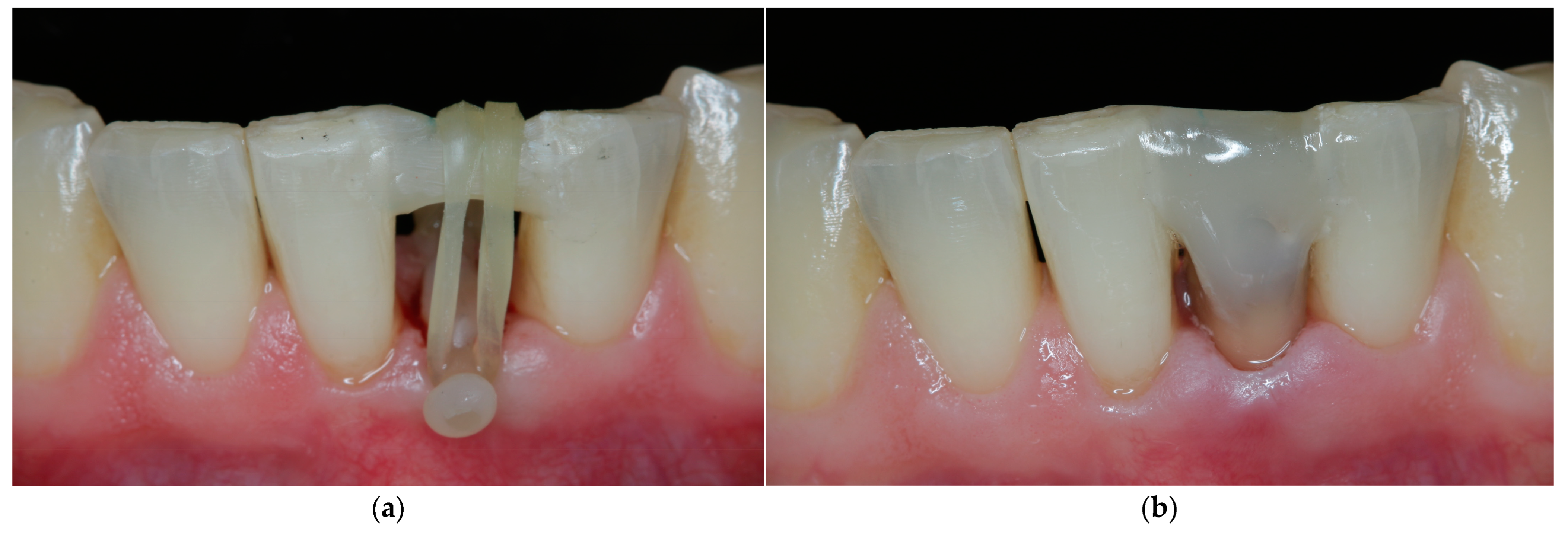
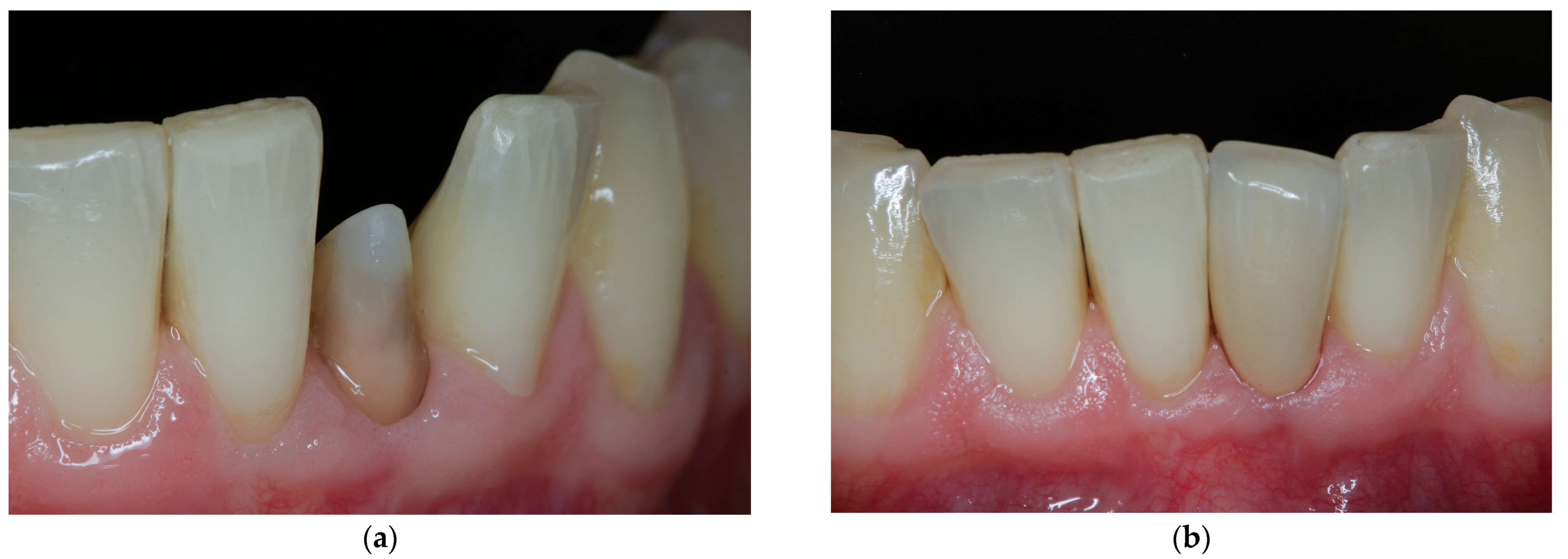
2.2.2. Forced Orthodontic Extrusion Treatment (FOE)
2.3. Assessment of Oral Health-Related Quality of Life (OHRQoL)
3. Results
3.1. Baseline Characteristics
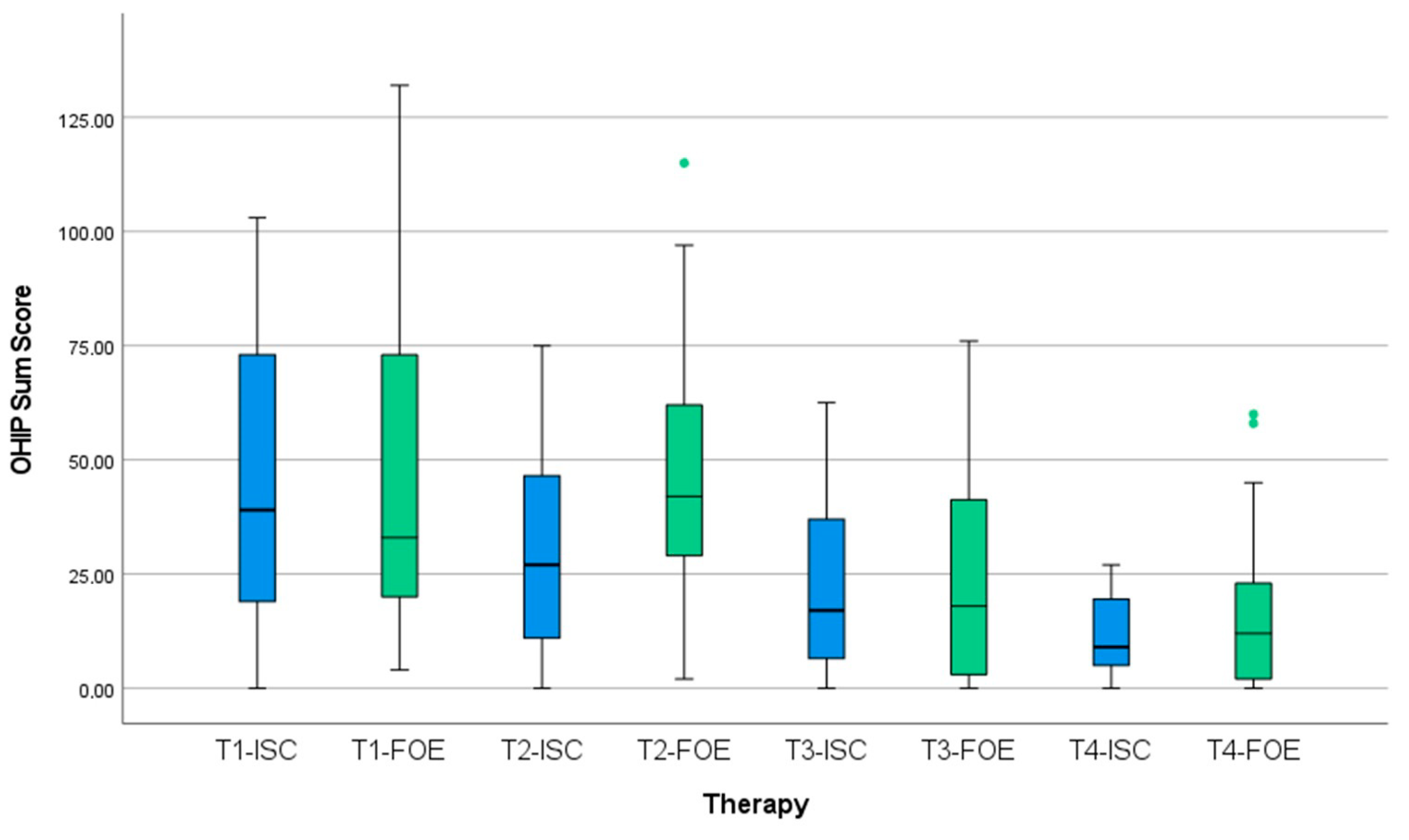
3.2. Oral Health-Related Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schatzle, M.; Land, N.P.; Anerud, A.; Boysen, H.; Burgin, W.; Loe, H. The influence of margins of restorations of the periodontal tissues over 26 years. J. Clin. Periodontol. 2001, 28, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Ingber, J.S.; Rose, L.F.; Coslet, J.G. The “biologic width”—A concept in periodontics and restorative dentistry. Alpha Omegan 1977, 70, 62–65. [Google Scholar] [PubMed]
- Naumann, M.; Schmitter, M.; Frankenberger, R.; Krastl, G. “Ferrule Comes First. Post Is Second!” Fake News and Alternative Facts? A Systematic Review. J. Endod. 2018, 44, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Juloski, J.; Radovic, I.; Goracci, C.; Vulicevic, Z.R.; Ferrari, M. Ferrule effect: A literature review. J. Endod. 2012, 38, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Lanning, S.K.; Waldrop, T.C.; Gunsolley, J.C.; Maynard, J.G. Surgical crown lengthening: Evaluation of the biological width. J. Periodontol. 2003, 74, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Ingber, J.S. Forced eruption: Part II. A method of treating nonrestorable teeth--Periodontal and restorative considerations. J. Periodontol. 1976, 47, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Heithersay, G.S.; Moule, A.J. Anterior subgingival fractures: A review of treatment alternatives. Aust. Dent. J. 1982, 27, 368–376. [Google Scholar] [CrossRef]
- Krastl, G.; Filippi, A.; Zitzmann, N.U.; Walter, C.; Weiger, R. Current aspects of restoring traumatically fractured teeth. Eur. J. Esthet. Dent. 2011, 6, 124–141. [Google Scholar]
- Bach, N.; Baylard, J.F.; Voyer, R. Orthodontic extrusion: Periodontal considerations and applications. J. Can. Dent. Assoc. 2004, 70, 775–780. [Google Scholar]
- Heithersay, G.S. Combined endodontic-orthodontic treatment of transverse root fractures in the region of the alveolar crest. Oral Surg. Oral Med. Oral Pathol. 1973, 36, 404–415. [Google Scholar] [CrossRef]
- Malmgren, O.; Malmgren, B.; Frykholm, A. Rapid orthodontic extrusion of crown root and cervical root fractured teeth. Endod. Dent. Traumatol. 1991, 7, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Bruhnke, M.; Bitter, K.; Beuer, F.; Bose, M.W.H.; Neumeyer, S.; Naumann, M. Tooth preservation of deeply destroyed teeth by forced orthodontic extrusion: A case series. Quintessence Int. 2022, 0, 2–11. [Google Scholar] [CrossRef]
- Torabinejad, M.; Anderson, P.; Bader, J.; Brown, L.J.; Chen, L.H.; Goodacre, C.J.; Kattadiyil, M.T.; Kutsenko, D.; Lozada, J.; Patel, R.; et al. Outcomes of root canal treatment and restoration, implant-supported single crowns, fixed partial dentures, and extraction without replacement: A systematic review. J. Prosthet. Dent. 2007, 98, 285–311. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implant. Res. 2012, 23 (Suppl. 5), 1–21. [Google Scholar] [CrossRef]
- Dawson, A.C.S. The SAC Classification in Implant Dentistry; Quintessence: Berlin, Germany, 2009. [Google Scholar]
- Clementini, M.; Tiravia, L.; De Risi, V.; Vittorini Orgeas, G.; Mannocci, A.; de Sanctis, M. Dimensional changes after immediate implant placement with or without simultaneous regenerative procedures: A systematic review and meta-analysis. J. Clin. Periodontol. 2015, 42, 666–677. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Polyzos, I.P.; Felice, P.; Worthington, H.V. Timing of implant placement after tooth extraction: Immediate, immediate-delayed or delayed implants? A Cochrane systematic review. Eur. J. Oral Implantol. 2010, 3, 189–205. [Google Scholar]
- Esposito, M.; Grusovin, M.G.; Polyzos, I.P.; Felice, P.; Worthington, H.V. Interventions for replacing missing teeth: Dental implants in fresh extraction sockets (immediate, immediate-delayed and delayed implants). Cochrane Database Syst. Rev. 2010, 8, CD005968. [Google Scholar] [CrossRef]
- Chen, S.T.; Buser, D. Clinical and esthetic outcomes of implants placed in postextraction sites. Int. J. Oral Maxillofac. Implant. 2009, 24 (Suppl. 24), 186–217. [Google Scholar]
- Cosyn, J.; Eghbali, A.; Hermans, A.; Vervaeke, S.; De Bruyn, H.; Cleymaet, R. A 5-year prospective study on single immediate implants in the aesthetic zone. J. Clin. Periodontol. 2016, 43, 702–709. [Google Scholar] [CrossRef]
- Turp, J.C.; Heydecke, G.; Krastl, G.; Pontius, O.; Antes, G.; Zitzmann, N.U. Restoring the fractured root-canal-treated maxillary lateral incisor: In search of an evidence-based approach. Quintessence Int. 2007, 38, 179–191. [Google Scholar]
- Pjetursson, B.E.; Heimisdottir, K. Dental implants-are they better than natural teeth? Eur. J. Oral Sci. 2018, 126 (Suppl. 1), 81–87. [Google Scholar] [CrossRef] [PubMed]
- Slade, G.D.; Spencer, A.J. Development and evaluation of the Oral Health Impact Profile. Community Dent. Health 1994, 11, 3–11. [Google Scholar] [PubMed]
- John, M.T.; Omara, M.; Su, N.; List, T.; Sekulic, S.; Haggman-Henrikson, B.; Visscher, C.M.; Bekes, K.; Reissmann, D.R.; Baba, K.; et al. Recommendations for Use and Scoring of Oral Health Impact Profile Versions. J. Evid. Based Dent. Pract. 2022, 22, 101619. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, N.U.; Krastl, G.; Weiger, R.; Kuhl, S.; Sendi, P. Cost-effectiveness of anterior implants versus fixed dental prostheses. J. Dent. Res. 2013, 92, 183S–188S. [Google Scholar] [CrossRef]
- Carvalho, C.V.; Bauer, F.P.; Romito, G.A.; Pannuti, C.M.; De Micheli, G. Orthodontic extrusion with or without circumferential supracrestal fiberotomy and root planing. Int. J. Periodontics Restor. Dent. 2006, 26, 87–93. [Google Scholar]
- John, M.T.; Feuerstahler, L.; Waller, N.; Baba, K.; Larsson, P.; Celebic, A.; Kende, D.; Rener-Sitar, K.; Reissmann, D.R. Confirmatory factor analysis of the Oral Health Impact Profile. J. Oral Rehabil. 2014, 41, 644–652. [Google Scholar] [CrossRef]
- Sanz, E.; Azabal, M.; Arias, A. Quality of life and satisfaction of patients two years after endodontic and dental implant treatments performed by experienced practitioners. J. Dent. 2022, 125, 104280. [Google Scholar] [CrossRef]
- John, M.T.; Reissmann, D.R.; Feuerstahler, L.; Waller, N.; Baba, K.; Larsson, P.; Celebic, A.; Szabo, G.; Rener-Sitar, K. Exploratory factor analysis of the Oral Health Impact Profile. J. Oral Rehabil. 2014, 41, 635–643. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Asgeirsson, A.G.; Zwahlen, M.; Sailer, I. Improvements in implant dentistry over the last decade: Comparison of survival and complication rates in older and newer publications. Int. J. Oral Maxillofac. Implant. 2014, 29, 308–324. [Google Scholar] [CrossRef]
- Bader, H.I. Treatment planning for implants versus root canal therapy: A contemporary dilemma. Implant. Dent. 2002, 11, 217–223. [Google Scholar] [CrossRef]
- Chappuis, V.; Avila-Ortiz, G.; Araujo, M.G.; Monje, A. Medication-related dental implant failure: Systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29 (Suppl. 16), 55–68. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Liu, N.; Xu, X.; Qu, X.; Lu, E. Smoking, radiotherapy, diabetes and osteoporosis as risk factors for dental implant failure: A meta-analysis. PLoS ONE 2013, 8, e71955. [Google Scholar] [CrossRef] [PubMed]
- Beikler, T.; Flemmig, T.F. EAO consensus conference: Economic evaluation of implant-supported prostheses. Clin. Oral Implant. Res. 2015, 26 (Suppl. 11), 57–63. [Google Scholar] [CrossRef] [PubMed]
- Jemt, T.; Ahlberg, G.; Henriksson, K.; Bondevik, O. Changes of anterior clinical crown height in patients provided with single-implant restorations after more than 15 years of follow-up. Int. J. Prosthodont. 2006, 19, 455–461. [Google Scholar] [PubMed]
- Thilander, B.; Odman, J.; Lekholm, U. Orthodontic aspects of the use of oral implants in adolescents: A 10-year follow-up study. Eur. J. Orthod. 2001, 23, 715–731. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient, Tooth and Treatment Characteristics | ||
|---|---|---|
| Forced Orthodontic Extrusion | Implant-Supported Single Crown | |
| No. of patients | 21 | 21 |
| Age (y, mean ±SD 1) | 47 ± 19 | 51 ± 15 |
| Gender | ||
| female (% of group) | 5 (24%) | 11 (52%) |
| male (% of group) | 16 (76%) | 10 (48%) |
| Tooth Location | ||
| Incisor | 7 (33%) | 0 |
| Canine | 3 (14%) | 1 (5%) |
| Premolar | 10 (48%) | 8 (39%) |
| Molar | 1 (5%) | 12 (57%) |
| Jaw Distribution | ||
| Maxilla | 16 (76%) | 11 (52%) |
| Mandible | 5 (24%) | 10 (48%) |
| Assessment | Overall | Treatment Group | p Value | ||||
|---|---|---|---|---|---|---|---|
| Forced Orthodontic Extrusion (FOE) | Implant-Supported Single Crown (ISC) | ||||||
| N | Median (Min/Max) | N | Median (Min/Max) | N | Median (Min/Max) | ||
| T1 | 41 | 39 (0/132) | 21 | 33 (4/132) | 20 | 44 (0/103) | 0.927 |
| T2 | 42 | 36 (0/115) | 21 | 42 (2/115) | 21 | 27 (0/75) | 0.059 |
| T3 | 40 | 18 (0/76) | 20 | 18 (0/76) | 20 | 17 (0/63) | 0.968 |
| T4 | 40 | 11 (0/60) | 20 | 11 (0/60) | 20 | 11 (0/45) | 0.820 |
| Assessment | Overall | Treatment Group | p-Value | |
|---|---|---|---|---|
| Forced Orthodontic Extrusion (FOE) | Implant-Supported Single Crown (ISC) | |||
| Median (Min/Max) | Median (Min/Max) | Median (Min/Max) | ||
| T1 | ||||
| Functional limitations | 8 (0/21) | 8 (0/19) | 9 (0/21) | 0.794 |
| Physical pain | 9 (0/27) | 9 (0/27) | 10 (0/22) | 0.754 |
| Psychological discomfort | 7 (0/20) | 7 (0/20) | 7 (0/18) | 0.990 |
| Physical disability | 4 (0/22) | 5 (0/22) | 3 (0/14) | 0.538 |
| Psychological disability | 5 (0/19) | 5 (0/19) | 6 (0/15) | 0.618 |
| Social disability | 3 (0/13) | 3 (0/13) | 3 (0/9) | 0.808 |
| Handicap | 4 (0/20) | 4 (0/20) | 6 (0/13) | 0.843 |
| T2 | ||||
| Functional limitations | 6 (0/15) | 9 (0/15) | 5 (0/12) | 0.003 |
| Physical pain | 8 (0/22) | 9 (0/22) | 6 (0/14) | 0.054 |
| Psychological discomfort | 5 (0/16) | 5 (0/16) | 5 (0/14) | 0.503 |
| Physical disability | 6 (0/21) | 7 (0/21) | 2 (0/13) | 0.021 |
| Psychological disability | 5 (0/16) | 5 (0/16) | 4 (0/12) | 0.415 |
| Social disability | 2 (0/14) | 2 (0/14) | 0 (0/9) | 0.312 |
| Handicap | 3 (0/12) | 4 (0/12) | 3 (0/10) | 0.436 |
| T3 | ||||
| Functional limitations | 4 (0/16) | 18 (0/76) | 4 (0/13) | 0.620 |
| Physical pain | 5 (0/17) | 5 (0/17) | 5 (0/12) | 0.841 |
| Psychological discomfort | 3 (0/11) | 3 (0/11) | 3 (0/9) | 0.602 |
| Physical disability | 2 (0/15) | 2 (0/14) | 2 (0/15) | 0.841 |
| Psychological disability | 2 (0/10) | 2 (0/10) | 3 (0/9) | 0.820 |
| Social disability | 0 (0/8) | 0 (0/8) | 0 (0/5) | 0.565 |
| Handicap | 2 (0/8) | 1.5 (0/7) | 2 (0/8) | 0.640 |
| T4 | ||||
| Functional limitations | 3 (0/10) | 3 (0/10) | 3 (0/8) | 0.841 |
| Physical pain | 3 (0/17) | 4 (0/17) | 3 (0/15) | 0.820 |
| Psychological discomfort | 1 (0/9) | 1 (0/9) | 1 (0/8) | 0.862 |
| Physical disability | 0 (0/9) | 0 (0/9) | 0 (0/6) | 0.583 |
| Psychological disability | 1 (0/10) | 0 (0/10) | 1 (0/8) | 0.799 |
| Social disability | 0 (0/6) | 0 (0/6) | 0 (0/5) | 0.841 |
| Handicap | 0 (0/8) | 0 (0/8) | 0 (0/7) | 0.620 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bruhnke, M.; Naumann, M.; Beuer, F.; Herklotz, I.; Böse, M.W.H.; Neumeyer, S.; Stein-Lausnitz, M.v. Implant or Tooth?—A Prospective Clinical Study on Oral Health-Related Quality of Life for Patients with “Unrestorable” Teeth. J. Clin. Med. 2022, 11, 7496. https://doi.org/10.3390/jcm11247496
Bruhnke M, Naumann M, Beuer F, Herklotz I, Böse MWH, Neumeyer S, Stein-Lausnitz Mv. Implant or Tooth?—A Prospective Clinical Study on Oral Health-Related Quality of Life for Patients with “Unrestorable” Teeth. Journal of Clinical Medicine. 2022; 11(24):7496. https://doi.org/10.3390/jcm11247496
Chicago/Turabian StyleBruhnke, Maria, Michael Naumann, Florian Beuer, Insa Herklotz, Mats Wernfried Heinrich Böse, Stefan Neumeyer, and Manja von Stein-Lausnitz. 2022. "Implant or Tooth?—A Prospective Clinical Study on Oral Health-Related Quality of Life for Patients with “Unrestorable” Teeth" Journal of Clinical Medicine 11, no. 24: 7496. https://doi.org/10.3390/jcm11247496
APA StyleBruhnke, M., Naumann, M., Beuer, F., Herklotz, I., Böse, M. W. H., Neumeyer, S., & Stein-Lausnitz, M. v. (2022). Implant or Tooth?—A Prospective Clinical Study on Oral Health-Related Quality of Life for Patients with “Unrestorable” Teeth. Journal of Clinical Medicine, 11(24), 7496. https://doi.org/10.3390/jcm11247496