
Pathological Diagnosis of Adult Craniopharyngioma on MR Images: An Automated End-to-End Approach Based on Deep Neural Networks Requiring No Manual Segmentation


Abstract
1. Introduction
2. Materials and Methods
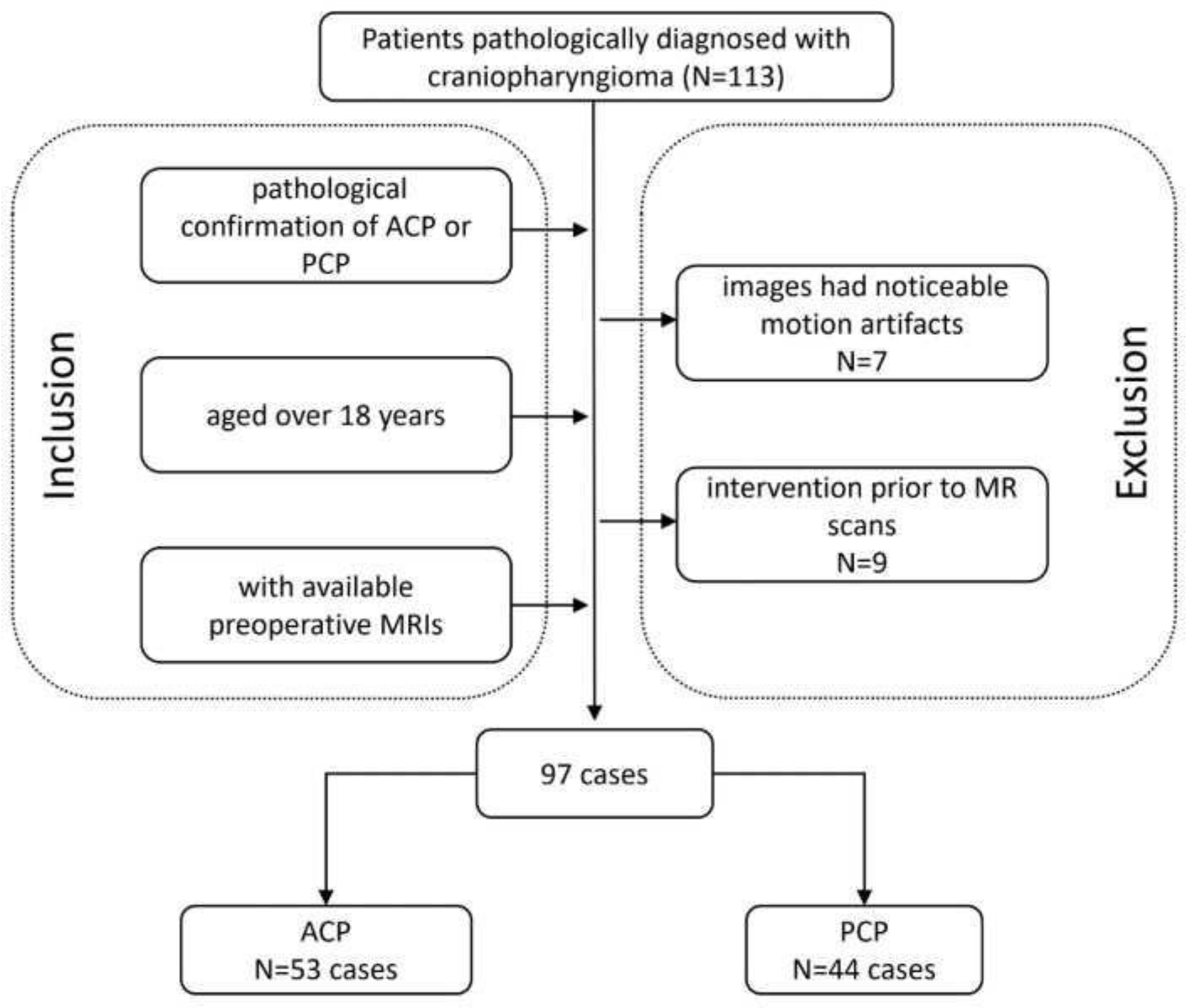
2.1. Patient Enrollment
2.2. MRI Protocol
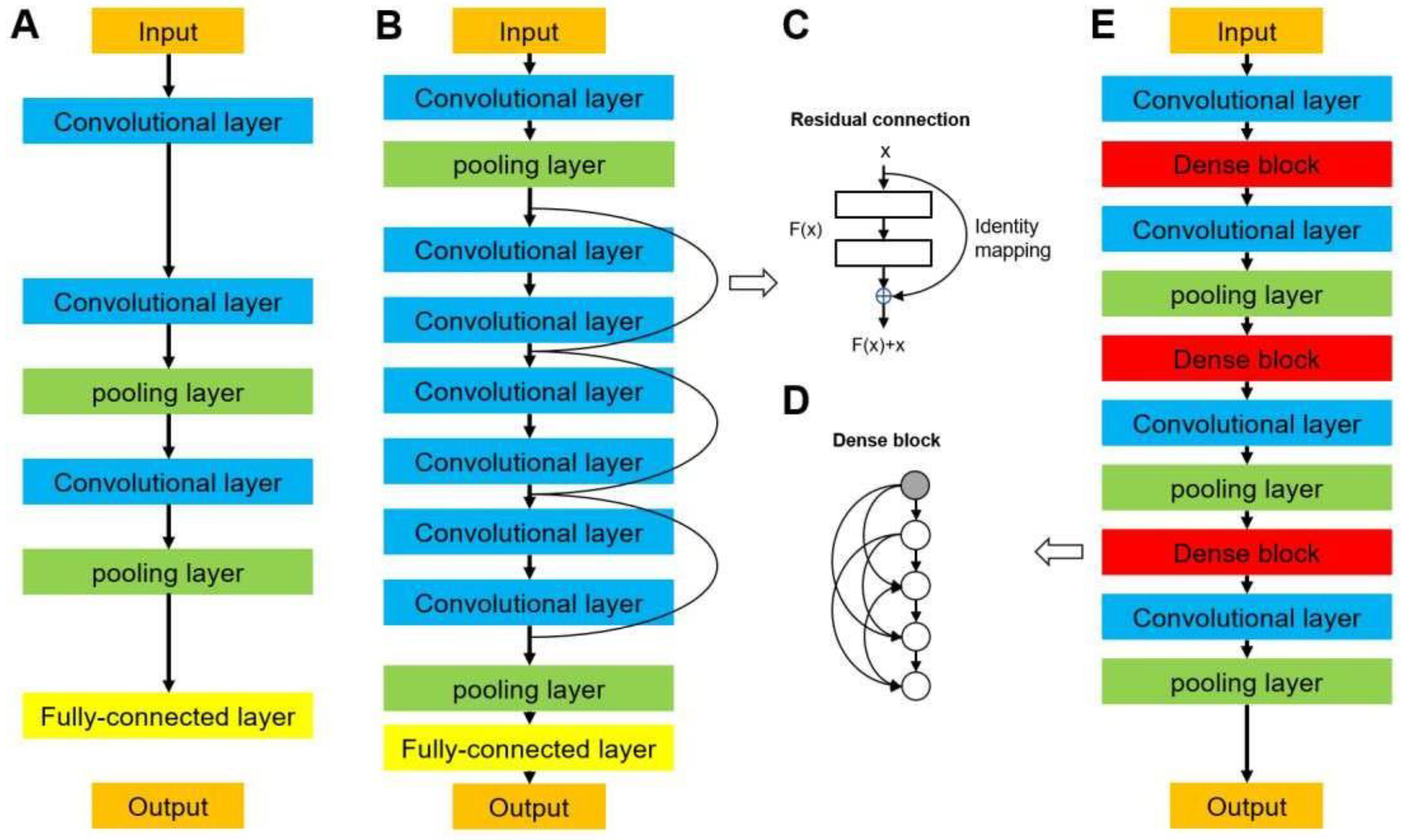
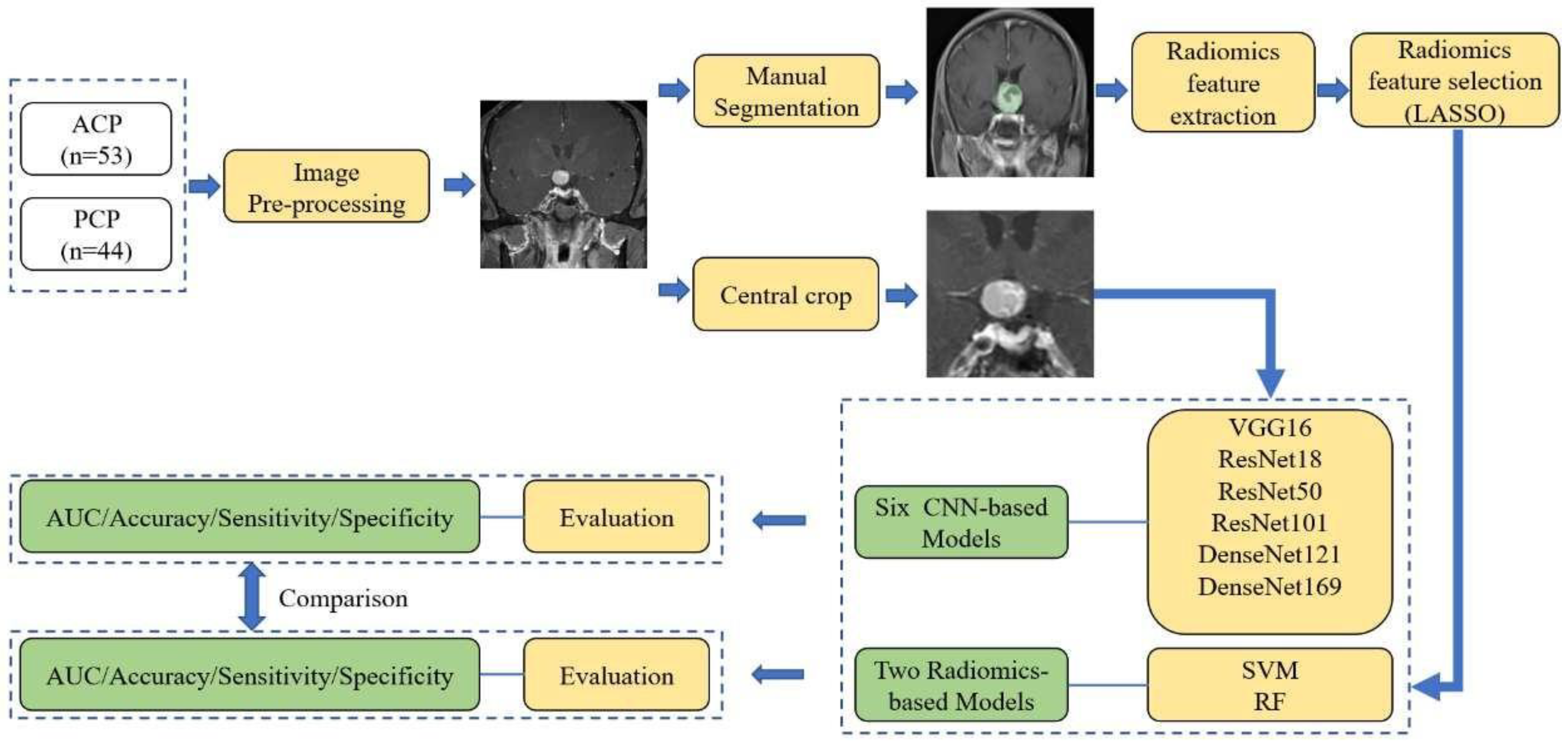
2.3. Image Preprocessing and Deep Neural Network Architecture
2.3.1. VGG Networks
2.3.2. DenseNet Networks
2.4. Deep Learning Model Training and Test
2.5. Radiomics Method
2.6. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Study Population
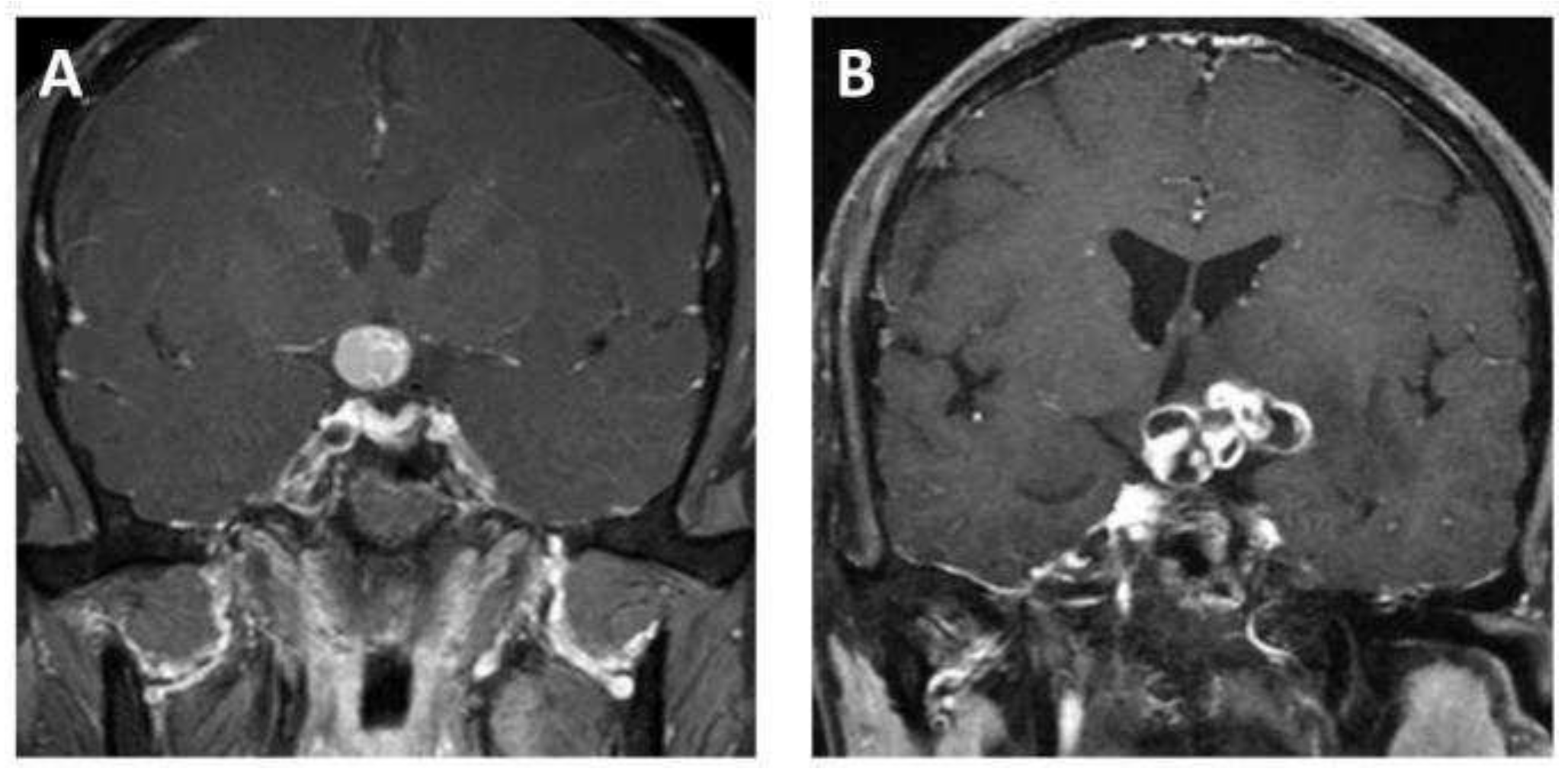
3.2. Radiological Features of Tumors
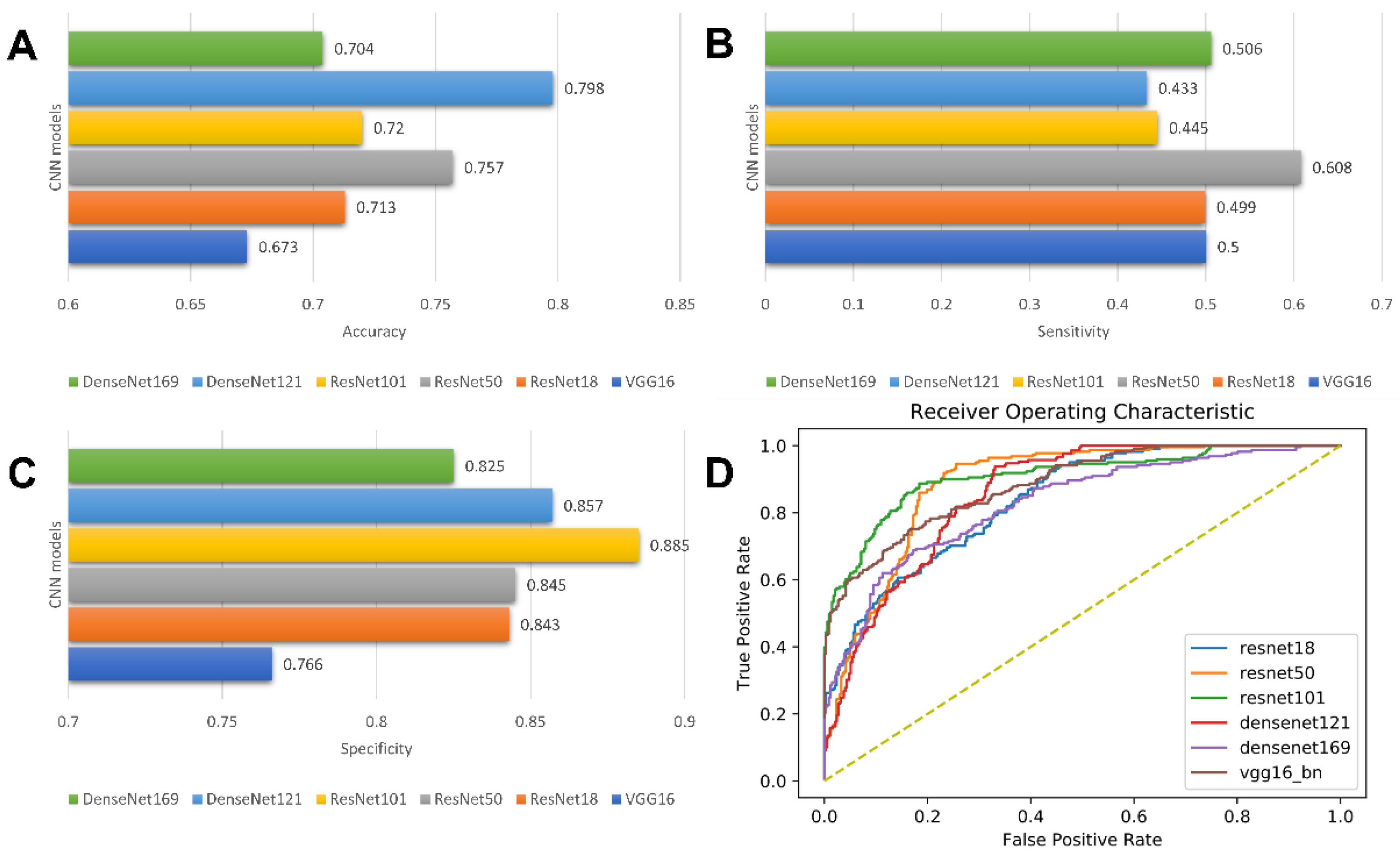
3.3. Prediction Performance of CNNs
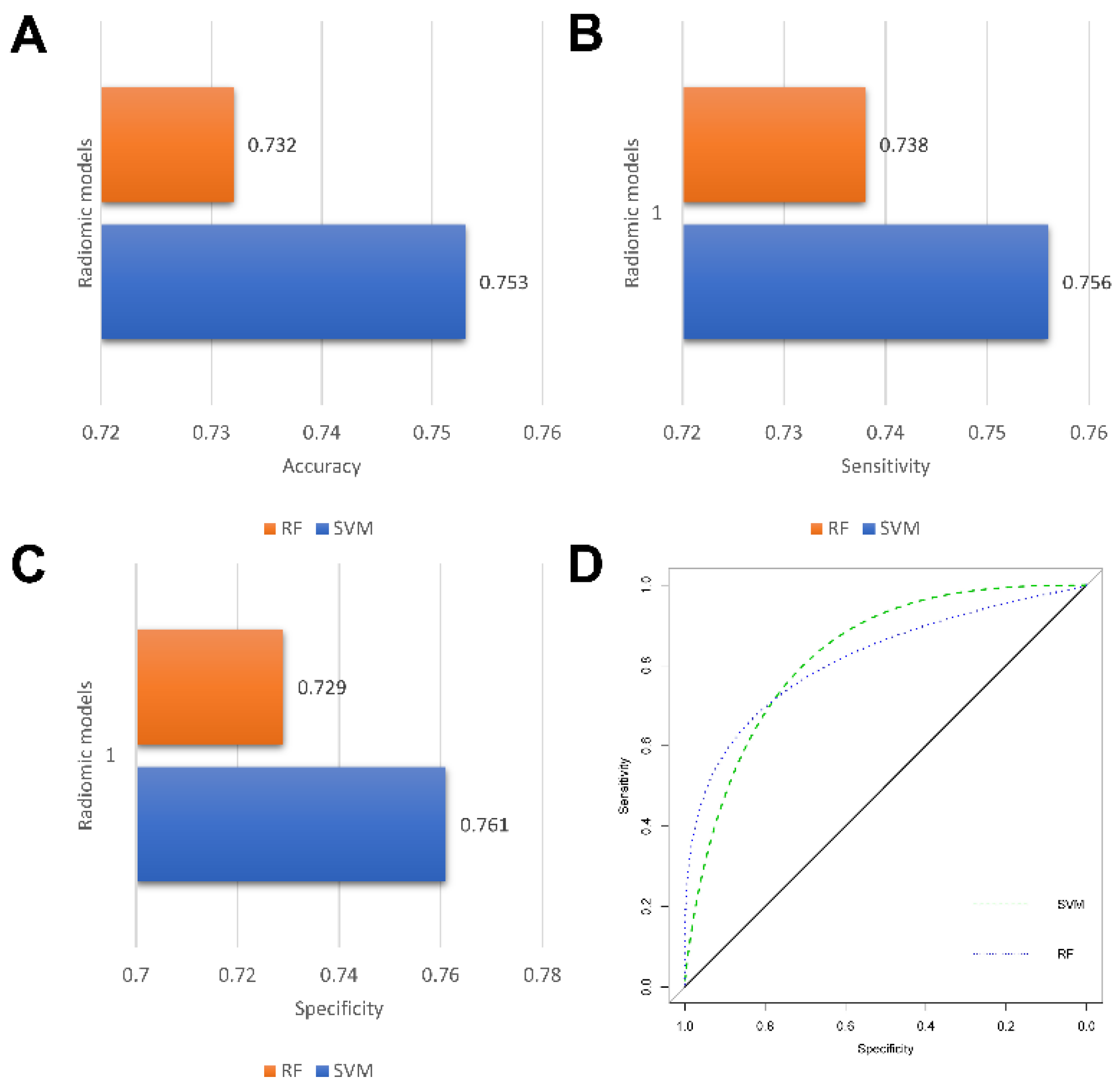
3.4. Predictive Performance of Radiomics Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Müller, H.L.; Merchant, T.E.; Warmuth-Metz, M.; Martinez-Barbera, J.P.; Puget, S. Craniopharyngioma. Nat. Rev. Dis. Primers 2019, 5, 75. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Hamblin, R.; Tsermoulas, G.; Karavitaki, N. Craniopharyngiomas. Presse Med. 2021, 50, 104078. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Gittleman, H.; Liao, P.; Vecchione-Koval, T.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary brain and other central nervous system tumors diagnosed in the United States in 2010-2014. Neuro Oncol. 2017, 19, v1–v88. [Google Scholar] [CrossRef]
- Wu, J.; Wu, X.; Yang, Y.Q.; Ding, H.; Yang, L.; Bao, Y.Y.; Zhou, L.; Yang, C.X.; Hong, T. Association of histological subtype with risk of recurrence in craniopharyngioma patients: A systematic review and meta-analysis. Neurosurg. Rev. 2022, 45, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Lara-Velazquez, M.; Mehkri, Y.; Panther, E.; Hernandez, J.; Rao, D.; Fiester, P.; Makary, R.; Rutenberg, M.; Tavanaiepour, D.; Rahmathulla, G. Current Advances in the Management of Adult Craniopharyngiomas. Curr. Oncol. 2022, 29, 1645–1671. [Google Scholar] [CrossRef]
- Brastianos, P.K.; Taylor-Weiner, A.; Manley, P.E.; Jones, R.T.; Dias-Santagata, D.; Thorner, A.R.; Lawrence, M.S.; Rodriguez, F.J.; Bernardo, L.A.; Schubert, L.; et al. Exome sequencing identifies BRAF mutations in papillary craniopharyngiomas. Nat. Genet. 2014, 46, 161–165. [Google Scholar] [CrossRef]
- Hölsken, A.; Sill, M.; Merkle, J.; Schweizer, L.; Buchfelder, M.; Flitsch, J.; Fahlbusch, R.; Metzler, M.; Kool, M.; Pfister, S.M.; et al. Adamantinomatous and papillary craniopharyngiomas are characterized by distinct epigenomic as well as mutational and transcriptomic profiles. Acta Neuropathol. Commun. 2016, 4, 20. [Google Scholar] [CrossRef]
- Brastianos, P.K.; Santagata, S. ENDOCRINE TUMORS: BRAF V600E mutations in papillary craniopharyngioma. Eur. J. Endocrinol. 2016, 174, R139–R144. [Google Scholar] [CrossRef]
- Roque, A.; Odia, Y. BRAF-V600E mutant papillary craniopharyngioma dramatically responds to combination BRAF and MEK inhibitors. CNS Oncol. 2017, 6, 95–99. [Google Scholar] [CrossRef]
- Himes, B.T.; Ruff, M.W.; Van Gompel, J.J.; Park, S.S.; Galanis, E.; Kaufmann, T.J.; Uhm, J.H. Recurrent papillary craniopharyngioma with BRAF V600E mutation treated with dabrafenib: Case report. J. Neurosurg. 2018, 130, 1299–1303. [Google Scholar] [CrossRef] [PubMed]
- Juratli, T.A.; Jones, P.S.; Wang, N.; Subramanian, M.; Aylwin, S.J.B.; Odia, Y.; Rostami, E.; Gudjonsson, O.; Shaw, B.L.; Cahill, D.P.; et al. Targeted treatment of papillary craniopharyngiomas harboring BRAF V600E mutations. Cancer 2019, 125, 2910–2914. [Google Scholar] [CrossRef] [PubMed]
- Brastianos, P.K.; Shankar, G.M.; Gill, C.M.; Taylor-Weiner, A.; Nayyar, N.; Panka, D.J.; Sullivan, R.J.; Frederick, D.T.; Abedalthagafi, M.; Jones, P.S.; et al. Dramatic Response of BRAF V600E Mutant Papillary Craniopharyngioma to Targeted Therapy. J. Natl. Cancer Inst. 2016, 108, djv310. [Google Scholar] [CrossRef] [PubMed]
- Mori, M.; Takeshima, H.; Kuratsu, J. Expression of interleukin-6 in human craniopharyngiomas: A possible inducer of tumor-associated inflammation. Int. J. Mol. Med. 2004, 14, 505–509. [Google Scholar] [CrossRef]
- Wang, Y.; Deng, J.; Wang, L.; Zhou, T.; Yang, J.; Tian, Z.; Yang, J.; Chen, H.; Tang, X.; Zhao, S.; et al. Expression and clinical significance of PD-L1, B7-H3, B7-H4 and VISTA in craniopharyngioma. J. Immunother. Cancer 2020, 8, e000406. [Google Scholar] [CrossRef]
- Sartoretti-Schefer, S.; Wichmann, W.; Aguzzi, A.; Valavanis, A. MR differentiation of adamantinous and squamous-papillary craniopharyngiomas. AJNR. Am. J. Neuroradiol. 1997, 18, 77–87. [Google Scholar]
- Lee, I.H.; Zan, E.; Bell, W.R.; Burger, P.C.; Sung, H.; Yousem, D.M. Craniopharyngiomas: Radiological Differentiation of Two Types. J. Korean Neurosurg. Soc. 2016, 59, 466–470. [Google Scholar] [CrossRef]
- Bangalore Yogananda, C.G.; Shah, B.R.; Vejdani-Jahromi, M.; Nalawade, S.S.; Murugesan, G.K.; Yu, F.F.; Pinho, M.C.; Wagner, B.C.; Mickey, B.; Patel, T.R.; et al. A novel fully automated MRI-based deep-learning method for classification of IDH mutation status in brain gliomas. Neuro Oncol. 2020, 22, 402–411. [Google Scholar] [CrossRef]
- Ben Naceur, M.; Akil, M.; Saouli, R.; Kachouri, R. Fully automatic brain tumor segmentation with deep learning-based selective attention using overlapping patches and multi-class weighted cross-entropy. Med. Image Anal. 2020, 63, 101692. [Google Scholar] [CrossRef]
- Xue, J.; Wang, B.; Ming, Y.; Liu, X.; Jiang, Z.; Wang, C.; Liu, X.; Chen, L.; Qu, J.; Xu, S.; et al. Deep learning-based detection and segmentation-assisted management of brain metastases. Neuro Oncol. 2020, 22, 505–514. [Google Scholar] [CrossRef]
- Zhang, M.; Young, G.S.; Chen, H.; Li, J.; Qin, L.; McFaline-Figueroa, J.R.; Reardon, D.A.; Cao, X.; Wu, X.; Xu, X. Deep-Learning Detection of Cancer Metastases to the Brain on MRI. J. Magn. Reson. Imaging JMRI 2020, 52, 1227–1236. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Tong, Y.; Shi, Z.; Chen, H.; Yang, Z.; Wang, Y.; Chen, L.; Yu, J. Noninvasive molecular diagnosis of craniopharyngioma with MRI-based radiomics approach. BMC Neurol. 2019, 19, 6. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.S.; Xiao, X.; Li, X.D.; Mo, H.Z.; He, W.L.; Deng, Y.H.; Lu, L.J.; Wu, Y.K.; Liu, H. Machine Learning-Based Multiparametric Magnetic Resonance Imaging Radiomic Model for Discrimination of Pathological Subtypes of Craniopharyngioma. J. Magn. Reson. Imaging JMRI 2021, 54, 1541–1550. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.; Zhao, W.; Yang, J.; Wang, H.; Zhang, H. Integrative Analysis of Biomarkers and Mechanisms in Adamantinomatous Craniopharyngioma. Front. Genet. 2022, 13, 830793. [Google Scholar] [CrossRef] [PubMed]
- Havaei, M.; Davy, A.; Warde-Farley, D.; Biard, A.; Courville, A.; Bengio, Y.; Pal, C.; Jodoin, P.M.; Larochelle, H. Brain tumor segmentation with Deep Neural Networks. Med. Image Anal. 2017, 35, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.; Pinto, A.; Alves, V.; Silva, C.A. Brain Tumor Segmentation Using Convolutional Neural Networks in MRI Images. IEEE Trans Med Imaging 2016, 35, 1240–1251. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; DePristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J. A guide to deep learning in healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef]
- Sitaula, C.; Hossain, M.B. Attention-based VGG-16 model for COVID-19 chest X-ray image classification. Appl. Intell. 2021, 51, 2850–2863. [Google Scholar] [CrossRef]
- Yoon, H.; Lee, J.; Oh, J.E.; Kim, H.R.; Lee, S.; Chang, H.J.; Sohn, D.K. Tumor Identification in Colorectal Histology Images Using a Convolutional Neural Network. J. Digit. Imaging 2019, 32, 131–140. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A.J. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Zhou, J.; Zhang, Y.; Chang, K.T.; Lee, K.E.; Wang, O.; Li, J.; Lin, Y.; Pan, Z.; Chang, P.; Chow, D.; et al. Diagnosis of Benign and Malignant Breast Lesions on DCE-MRI by Using Radiomics and Deep Learning With Consideration of Peritumor Tissue. J. Magn. Reson. Imaging JMRI 2020, 51, 798–809. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.C.; Lai, J.; Huang, J.Y.; Cho, C.F.; Lee, P.H.; Lu, M.H.; Yeh, C.C.; Yu, J.; Lin, W.C. Predicting microvascular invasion in hepatocellular carcinoma: A deep learning model validated across hospitals. Cancer Imaging 2021, 21, 56. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Tao, Z.; Bingqiang, H.; Huiling, L.; Zaoli, Y.; Hongbin, S. NSCR-Based DenseNet for Lung Tumor Recognition Using Chest CT Image. BioMed Res. Int. 2020, 2020, 6636321. [Google Scholar] [CrossRef]
- Thakur, M.; Kuresan, H.; Dhanalakshmi, S.; Lai, K.W.; Wu, X. Soft Attention Based DenseNet Model for Parkinson’s Disease Classification Using SPECT Images. Front. Aging Neurosci. 2022, 14, 908143. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.C.; Pieper, S.; Aerts, H. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Xie, N.; Fan, X.; Chen, D.; Chen, J.; Yu, H.; He, M.; Liu, H.; Yin, X.; Li, B.; Wang, H. Peritumoral and Intratumoral Texture Features Based on Multiparametric MRI and Multiple Machine Learning Methods to Preoperatively Evaluate the Pathological Outcomes of Pancreatic Cancer. J. Magn. Reson. Imaging JMRI, 2022; in press. [Google Scholar] [CrossRef]
- Joo, L.; Park, J.E.; Park, S.Y.; Nam, S.J.; Kim, Y.H.; Kim, J.H.; Kim, H.S. Extensive peritumoral edema and brain-to-tumor interface MRI features enable prediction of brain invasion in meningioma: Development and validation. Neuro Oncol. 2021, 23, 324–333. [Google Scholar] [CrossRef]
- Ma, G.; Kang, J.; Qiao, N.; Zhang, B.; Chen, X.; Li, G.; Gao, Z.; Gui, S. Non-Invasive Radiomics Approach Predict Invasiveness of Adamantinomatous Craniopharyngioma Before Surgery. Front. Oncol. 2020, 10, 599888. [Google Scholar] [CrossRef]
- Ngiam, K.Y.; Khor, I.W. Big data and machine learning algorithms for health-care delivery. Lancet Oncol. 2019, 20, e262–e273. [Google Scholar] [CrossRef] [PubMed]
- Apps, J.R.; Carreno, G.; Gonzalez-Meljem, J.M.; Haston, S.; Guiho, R.; Cooper, J.E.; Manshaei, S.; Jani, N.; Hölsken, A.; Pettorini, B.; et al. Tumour compartment transcriptomics demonstrates the activation of inflammatory and odontogenic programmes in human adamantinomatous craniopharyngioma and identifies the MAPK/ERK pathway as a novel therapeutic target. Acta Neuropathol. 2018, 135, 757–777. [Google Scholar] [CrossRef] [PubMed]
- Haston, S.; Pozzi, S.; Carreno, G.; Manshaei, S.; Panousopoulos, L.; Gonzalez-Meljem, J.M.; Apps, J.R.; Virasami, A.; Thavaraj, S.; Gutteridge, A.; et al. MAPK pathway control of stem cell proliferation and differentiation in the embryonic pituitary provides insights into the pathogenesis of papillary craniopharyngioma. Development 2017, 144, 2141–2152. [Google Scholar] [CrossRef]
- Adamson, T.E.; Wiestler, O.D.; Kleihues, P.; Yaşargil, M.G. Correlation of clinical and pathological features in surgically treated craniopharyngiomas. J. Neurosurg. 1990, 73, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Tavangar, S.M.; Larijani, B.; Mahta, A.; Hosseini, S.M.; Mehrazine, M.; Bandarian, F. Craniopharyngioma: A clinicopathological study of 141 cases. Endocr. Pathol. 2004, 15, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Szeifert, G.T.; Sipos, L.; Horváth, M.; Sarker, M.H.; Major, O.; Salomváry, B.; Czirják, S.; Bálint, K.; Slowik, F.; Kolonics, L.; et al. Pathological characteristics of surgically removed craniopharyngiomas: Analysis of 131 cases. Acta Neurochir. 1993, 124, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Cui, E.; Li, Z.; Ma, C.; Li, Q.; Lei, Y.; Lan, Y.; Yu, J.; Zhou, Z.; Li, R.; Long, W.; et al. Predicting the ISUP grade of clear cell renal cell carcinoma with multiparametric MR and multiphase CT radiomics. Eur. Radiol. 2020, 30, 2912–2921. [Google Scholar] [CrossRef] [PubMed]
- Tang, T.Y.; Li, X.; Zhang, Q.; Guo, C.X.; Zhang, X.Z.; Lao, M.Y.; Shen, Y.N.; Xiao, W.B.; Ying, S.H.; Sun, K.; et al. Development of a Novel Multiparametric MRI Radiomic Nomogram for Preoperative Evaluation of Early Recurrence in Resectable Pancreatic Cancer. J. Magn. Reson. Imaging JMRI 2020, 52, 231–245. [Google Scholar] [CrossRef]
- Zhang, B.; Tian, J.; Dong, D.; Gu, D.; Dong, Y.; Zhang, L.; Lian, Z.; Liu, J.; Luo, X.; Pei, S.; et al. Radiomics Features of Multiparametric MRI as Novel Prognostic Factors in Advanced Nasopharyngeal Carcinoma. Clin. Cancer Res. 2017, 23, 4259–4269. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | ACP (n = 53) | PCP (n = 44) | p Value |
|---|---|---|---|
| Age (y) | 49.6 ± 3.0 | 44.7 ± 2.2 | 0.187 |
| Sex | 0.422 | ||
| Male | 27 | 26 | |
| Female | 26 | 18 | |
| Onset duration (w) | 50.9 ± 9.9 | 39.7 ± 11.0 | 0.453 |
| Symptoms | |||
| Headache | 34 | 32 | 0.367 |
| Visual impairment | 36 | 35 | 0.198 |
| Endocrine dysfunction | 35 | 33 | 0.337 |
| None | 2 | 3 | 0.500 |
| Hypothalamic involvement | 11 | 17 | 0.053 |
| Location | 0.396 | ||
| Intrasellar | 0 | 1 | |
| Suprasellar | 29 | 27 | |
| Combination | 24 | 16 | |
| Tissue structure | 0.154 | ||
| Solid | 7 | 10 | |
| Cystic | 15 | 6 | |
| Mixed | 31 | 28 | |
| Shape | 0.751 | ||
| Regular | 11 | 8 | |
| Irregular | 42 | 36 | |
| Maximum diameter (mm) | 37.91 ± 1.7 (22–78) | 30.02 ± 1.7 (9–66) | 0.015 |
| Method | Model | AUC | Accuracy | Sensitivity | Specificity |
|---|---|---|---|---|---|
| CNN | VGG16 | 0.822 ± 0.054 | 0.673 ± 0.013 | 0.500 ± 0.327 | 0.766 ± 0.189 |
| ResNet18 | 0.791 ± 0.055 | 0.713 ± 0.038 | 0.499 ± 0.203 | 0.843 ± 0.077 | |
| ResNet50 | 0.838 ± 0.062 | 0.757 ± 0.052 | 0.608 ± 0.198 | 0.845 ± 0.034 | |
| ResNet101 | 0.821 ± 0.080 | 0.720 ± 0.079 | 0.445 ± 0.122 | 0.885 ± 0.060 | |
| DenseNet121 | 0.799 ± 0.063 | 0.798 ± 0.051 | 0.433 ± 0.052 | 0.857 ± 0.052 | |
| DenseNet169 | 0.789 ± 0.050 | 0.704 ± 0.049 | 0.506 ± 0.088 | 0.825 ± 0.063 | |
| Radiomics | SVM | 0.763 ± 0.068 | 0.753 ± 0.091 | 0.756 ± 0.058 | 0.761 ± 0.144 |
| RF | 0.769 ± 0.066 | 0.732 ± 0.053 | 0.738 ± 0.044 | 0.729 ± 0.085 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teng, Y.; Ran, X.; Chen, B.; Chen, C.; Xu, J. Pathological Diagnosis of Adult Craniopharyngioma on MR Images: An Automated End-to-End Approach Based on Deep Neural Networks Requiring No Manual Segmentation. J. Clin. Med. 2022, 11, 7481. https://doi.org/10.3390/jcm11247481
Teng Y, Ran X, Chen B, Chen C, Xu J. Pathological Diagnosis of Adult Craniopharyngioma on MR Images: An Automated End-to-End Approach Based on Deep Neural Networks Requiring No Manual Segmentation. Journal of Clinical Medicine. 2022; 11(24):7481. https://doi.org/10.3390/jcm11247481
Chicago/Turabian StyleTeng, Yuen, Xiaoping Ran, Boran Chen, Chaoyue Chen, and Jianguo Xu. 2022. "Pathological Diagnosis of Adult Craniopharyngioma on MR Images: An Automated End-to-End Approach Based on Deep Neural Networks Requiring No Manual Segmentation" Journal of Clinical Medicine 11, no. 24: 7481. https://doi.org/10.3390/jcm11247481
APA StyleTeng, Y., Ran, X., Chen, B., Chen, C., & Xu, J. (2022). Pathological Diagnosis of Adult Craniopharyngioma on MR Images: An Automated End-to-End Approach Based on Deep Neural Networks Requiring No Manual Segmentation. Journal of Clinical Medicine, 11(24), 7481. https://doi.org/10.3390/jcm11247481