


GP IIb/IIIa Receptor Inhibitors in Mechanically Ventilated Patients with Cardiogenic Shock due to Myocardial Infarction in the Era of Potent P2Y12 Receptor Antagonists

Abstract
1. Introduction
2. Materials and Methods
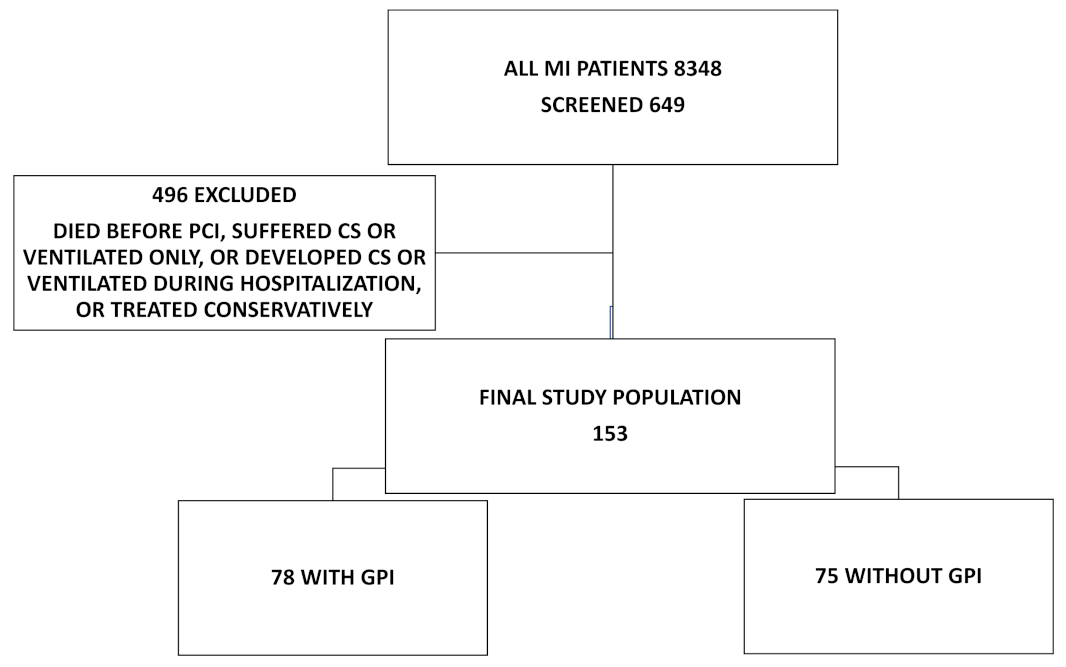
2.1. Patients and Definitions
2.2. Pharmacological Treatment
2.3. Study End Points
2.4. Statistical Methods
3. Results
3.1. Thirty-Day Mortality
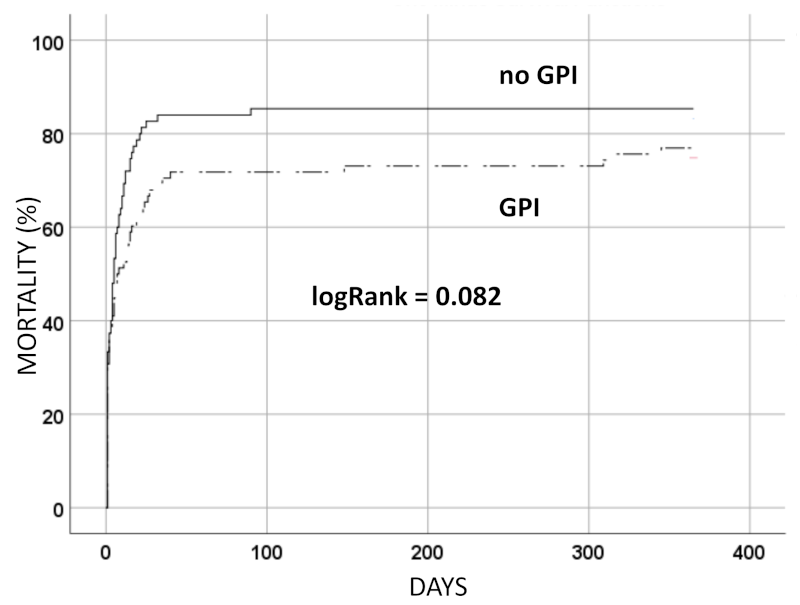
3.2. Mortality after One Year
3.3. TIMI Grade Flow
3.4. Bleeding
3.5. Cerebral Performance Category (CPC) Score
3.6. Complications during Hospitalization
4. Discussion
- (a)
- Patients receiving GPI had significantly better TIMI flow after PCI and more often experienced an improvement of ≥ 1 TIMI grade flow during PCI.
- (b)
- GPI use was not associated with a higher bleeding rate in these patients.
- (c)
- The CPC score was better in patients with GPI.
- (d)
- Patients receiving GPI had similar 30-day and one-year mortality, and GPI were not independently associated with either outcome.
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- Karathanos, A.; Lin, Y.; Dannenberg, L.; Parco, C.; Schulze, V.; Brockmeyer, M.; Jung, C.; Heinen, Y.; Perings, S.; Zeymer, U.; et al. Routine Glycoprotein IIb/IIIa Inhibitor Therapy in ST-Segment Elevation Myocardial Infarction: A Meta-analysis. Can. J. Cardiol. 2019, 11, 1576–1588. [Google Scholar] [CrossRef]
- Droppa, M.; Vaduganathan, M.; Venkateswaran, R.V.; Singh, A.; Szumita, P.M.; Roberts, R.J.; Qamar, A.; Hack, L.; Rath, D.; Gawaz, M.; et al. Cangrelor in cardiogenic shock and after cardiopulmonary resuscitation: A global, multicenter, matched pair analysis with oral P2Y 12 inhibition from the IABP-SHOCK II trial. Resuscitation 2019, 137, 205–212. [Google Scholar] [CrossRef]
- Blanchart, K.; Heudel, T.; Ardouin, P.; Lemaitre, A.; Briet, C.; Bignon, M.; Sabatier, R.; Legallois, D.; Roule, V.; Beygui, F. Glycoprotein IIb/IIIa inhibitors use in the setting of primary percutaneous coronary intervention for ST elevation myocardial infarction in patients pre-treated with newer P2Y12 inhibitors. Clin. Cardiol. 2021, 8, 1080–1088. [Google Scholar] [CrossRef]
- Gorgis, S.; Lemor, A.; Kolski, B.; Lalonde, T.; Kaki, A.; Marso, S.; Senter, S.; Rahman, A.; Gorwara, S.; Nazir, R.; et al. Antiplatelet Therapy in Acute Myocardial Infarction and Cardiogenic Shock: Insights From the National Cardiogenic Shock Initiative. J. Invasive Cardiol. 2022, 34, E156–E163. [Google Scholar]
- Myrda, K.; Gąsior, M.; Dudek, D.; Nawrotek, B.; Niedziela, J.; Wojakowski, W.; Gierlotka, M.; Grygier, M.; Stępińska, J.; Witkowski, A.; et al. One-Year Outcome of Glycoprotein IIb/IIIa Inhibitor Therapy in Patients with Myocardial Infarction-Related Cardiogenic Shock. J. Clin. Med. 2021, 21, 5059. [Google Scholar] [CrossRef]
- Bernat, I.; Abdelaal, E.; Plourde, G.; Bataille, Y.; Cech, J.; Pesek, J.; Koza, J.; Jirous, S.; Machaalany, J.; Déry, J.-P.; et al. Early and late outcomes after primary percutaneous coronary intervention by radial or femoral approach in patients presenting in acute ST-elevation myocardial infarction and cardiogenic shock. Am. Hear. J. 2013, 165, 338–343. [Google Scholar] [CrossRef]
- Kanic, V.; Vollrath, M.; Penko, M.; Markota, A.; Kompara, G.; Kanic, Z. GPI Ib-IIIa Receptor Inhibitors in Acute Coronary Syndrome Patients Presenting with Cardiogenic Shock and/or After Cardiopulmonary Resuscitation. Heart Lung. Circ. 2018, 27, 73–78. [Google Scholar] [CrossRef]
- Mebazaa, A.; Combes, A.; van Diepen, S.; Hollinger, A.; Katz, J.N.; Landoni, G.; Hajjar, L.A.; Lassus, J.; Lebreton, G.; Montalescot, G.; et al. Management of cardiogenic shock complicating myocardial infarction. Intensiv. Care Med. 2018, 44, 760–773. [Google Scholar] [CrossRef]
- Kayaert, P.; Coeman, M.; Demolder, A.; Gevaert, S.; Schaubroeck, H.; Claeys, M.J.; Hanet, C.; Beauloye, C.; Desmet, W.; de Pauw, M.; et al. Mortality in STEMI Patients with Cardiogenic Shock: Results From a Nationwide PCI Registry and Focus on Left Main PCI. J. Invasive Cardiol. 2022, 34, E142–E148. [Google Scholar] [PubMed]
- Valgimigli, M.; Frigoli, E.; Leonardi, S.; Rothenbühler, M.; Gagnor, A.; Calabrò, P.; Garducci, S.; Rubartelli, P.; Briguori, C.; Andò, G.; et al. Bivalirudin or Unfractionated Heparin in Acute Coronary Syndromes. N. Engl. J. Med. 2015, 11, 997–1009. [Google Scholar] [CrossRef] [PubMed]
- Saleiro, C.; Teixeira, R.; De Campos, D.; Lopes, J.; Oliveiros, B.; Costa, M.; Gonçalves, L. Glycoprotein IIb/IIIa inhibitors for cardiogenic shock complicating acute myocardial infarction: A systematic review, meta-analysis, and meta-regression. J. Intensiv. Care 2020, 1, 85. [Google Scholar] [CrossRef] [PubMed]
- De Luca, G.; Navarese, E.; Marino, P. Risk profile and benefits from Gp IIb-IIIa inhibitors among patients with ST-segment elevation myocardial infarction treated with primary angioplasty: A meta-regression analysis of randomized trials. Eur. Heart J. 2009, 22, 2705–2713. [Google Scholar] [CrossRef]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur. Heart J. 2019, 2, 87–165. [Google Scholar] [CrossRef]
- Kanic, V.; Vollrath, M.; Naji, F.H.; Markota, A.; Sinkovic, A. Impact of the New P2Y12 Receptor Inhibitors on Mortality in STElevation Myocardial Infarction Patients with Cardiogenic Shock and/or After Cardiopulmonary Resuscitation Undergoing Percutaneous Coronary Intervention. Cardiovasc. Pharm Open Access 2016, 5, 175. [Google Scholar] [CrossRef]
- Siller-Matula, J.M.; Delle Karth, G. Dual platelet inhibitors in intensive care units. Medizinische Klinik, Intensivmedizin und Notfallmedizin 2014, 109, 429–436. [Google Scholar] [CrossRef]
- Weeks, P.A.; Sieg, A.; Paruthi, C.; Rajapreyar, I. Antiplatelet Therapy Considerations in Ischemic Cardiogenic Shock: Implications of Metabolic Bioactivation. J. Cardiovasc. Pharmacol. Ther. 2015, 4, 370–377. [Google Scholar] [CrossRef]
- Droppa, M.; Borsta, O.; Ratha, D.; Müllera, K.; Gawaza, M.; Bhatt, D.L.; Geisler, T. Impact of Intravenous P2Y12-Receptor Inhibition with Cangrelor in Patients Presenting with Acute Coronary Syndrome and Cardiogenic Shock—A Case Series. Cell. Physiol. Biochem. 2017, 42, 1336–1341. [Google Scholar] [CrossRef]
- White, C.W. Simplicity's virtue scorned. Precision comes to TIMI flow grading and the results are...surprising. Circulation 1996, 93, 853–856. [Google Scholar] [CrossRef]
- Mehran, R.; Rao, S.V.; Bhatt, D.L.; Gibson, C.M.; Caixeta, A.; Eikelboom, J.; Kaul, S.; Wiviott, S.D.; Menon, V.; Nikolsky, E.; et al. Standardized bleeding definitions for cardiovascular clinical trials: A consensus report from the Bleeding Academic Research Consortium. Circulation 2011, 23, 2736–2747. [Google Scholar] [CrossRef] [PubMed]
- Edgren, E.; Hedstrand, U.; Kelsey, S.; Sutton-Tyrrell, K.; Safar, P.; BRCTI Study Group. Assessment of neurological prognosis in comatose survivors of cardiac arrest. Lancet 1994, 343, 1055–1059. [Google Scholar] [CrossRef] [PubMed]
- Parodi, G.; Valenti, R.; Bellandi, B.; Migliorini, A.; Marcucci, R.; Comito, V.; Carrabba, N.; Santini, A.; Gensini, G.F.; Abbate, R.; et al. Comparison of prasugrel and ticagrelor loading doses in ST-segment elevation myocardial infarction patients: RAPID (Rapid Activity of Platelet Inhibitor Drugs) primary PCI study. J. Am. Coll. Cardiol. 2013, 61, 1601–1616. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Tebaldi, M.; Campo, G.; Gambetti, S.; Bristot, L.; Monti, M.; Parrinello, G.; Ferrari, R. Prasugrel Versus Tirofiban Bolus with or without Short Post-Bolus Infusion with or without Concomitant Prasugrel Administration in Patients with Myocardial Infarction Undergoing Coronary Stenting: The FABOLUS PRO (Facilitation through Aggrastat By drOpping or shortening Infusion Line in patients with ST-segment elevation myocardial infarction compared to or on top of PRasugrel given at loading dOse) Trial. JACC Cardiovasc. Interv. 2012, 5, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Tousek, P.; Rokyta, R.; Tesarova, J.; Pudil, R.; Belohlavek, J.; Stasek, J.; Rohac, F.; Widimsky, P. Routine upfront abciximab versus standard periprocedural therapy in patients undergoing primary percutaneous coronary intervention for cardiogenic shock: The PRAGUE-7 Study. An open randomized multicentre study. Acute Card. Care 2011, 13, 116–122. [Google Scholar] [CrossRef] [PubMed]
- De Felice, F.; Tomassini, F.; Fiorilli, R.; Gagnor, A.; Parma, A.; Cerrato, E.; Musto, C.; Nazzaro, M.S.; Varbella, F.; Violini, R. Effect of Abciximab Therapy in Patients Undergoing Coronary Angioplasty for Acute ST-Elevation Myocardial Infarction Complicated by Cardiogenic Shock. Circ. J. 2015, 79, 1568–1574. [Google Scholar] [CrossRef]
- Mehta, R.H.; Ou, F.-S.; Peterson, E.D.; Shaw, R.E.; Hillegass, W.B.; Rumsfeld, J.S.; Roe, M.T. Clinical Significance of Post-Procedural TIMI Flow in Patients with Cardiogenic Shock Undergoing Primary Percutaneous Coronary Intervention. JACC Cardiovasc. Interv. 2009, 2, 56–64. [Google Scholar] [CrossRef]
- Holmes, D.R., Jr.; Kereiakes, D.J.; Garg, S.; Serruys, P.W.; Dehmer, G.J.; Ellis, S.G.; Williams, D.O.; Kimura, T.; Moliterno, D.J. Stent thrombosis. J. Am. Coll. Cardiol. 2010, 56, 1357–1365. [Google Scholar] [CrossRef]
- Muhlestein, J.B. Effect of antiplatelet therapy on inflammatory markers in atherothrombotic patients. Thromb. Haemost. 2010, 103, 71–82. [Google Scholar] [CrossRef]
- Schulman, S.P. Antiplatelet Therapy in Non–ST-Segment Elevation Acute Coronary Syndromes. JAMA 2004, 292, 1875–1882. [Google Scholar] [CrossRef]
- Kanič, V.; Balevski, I.; Granda, S.; Naji, F.H.; Krajnc, I.; Kompara, G. Radial access versus femoral access in myocardial infarction—A single-center experience. Slov. Med. J. 2019, 88, 328–338. [Google Scholar] [CrossRef]
- Hinohara, T.T.; Rao, S.V. Current State of Radial Artery Catheterization in ST-Elevation Myocardial Infarction. Prog. Cardiovasc. Dis. 2015, 58, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Dobies, D.R.; Barber, K.R.; Cohoon, A.L. Analysis of safety outcomes for radial versus femoral access for percutaneous coronary intervention from a large clinical registry. Open Heart 2016, 3, e000397. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Akin, I.; Sandri, M.; Fuernau, G.; De Waha, S.; Meyer-Saraei, R.; Nordbeck, P.; Geisler, T.; Landmesser, U.; Skurk, C.; et al. PCI Strategies in Patients with Acute Myocardial Infarction and Cardiogenic Shock. N. Engl. J. Med. 2017, 377, 2419–2432. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, M.; Wade, S.R.; Henry, T.D. STEMI care 2021: Addressing the knowledge gaps. Am. Heart J. Plus Cardiol. Res. Pract. 2021, 11, 100044. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | NO-GPI N = 75 | GPI N = 78 | POPULATION N = 153 | p |
|---|---|---|---|---|
| Age (years) | 66.0 (12.9) | 65.1 (13.3) | 66.0 (12.9) | 0.66 |
| Women | 28 (37.5) | 25 (32.1) | 53 (34.6) | 0.50 |
| Diabetes | 14 (18.7) | 17 (21.8) | 31 (20.3) | 0.69 |
| Hypertension | 24 (32.0) | 29 (37.2) | 53 (34.6) | 0.61 |
| Hyperlipidemia | 7 (9.3) | 13 (16.7) | 20 (13.1) | 0.23 |
| Smoking | 12 (16.0) | 11 (14.1) | 23 (15.0) | 0.82 |
| Previous MI | 13 (17.3) | 10 (12.8) | 23 (15.0) | 0.50 |
| Previous stroke | 7 (9.3) | 2 (2.6) | 9 (5.9) | 0.094 |
| Previous PCI or CABG | 7 (9.3) | 2 (2.6) | 9 (5.99) | 0.094 |
| Aortic stenosis | 3 (4.0) | 1 (1.3) | 4 (2.6) | 0.36 |
| Known chronic kidney disease | 7 (9.3) | 4 (5.1) | 11 (7.2) | 0.36 |
| STEMI | 63 (84.0) | 73 (92.3) | 136 (88.2) | 0.13 |
| Anterior infarct | 34 (45.3) | 46 (59.0) | 80 (52.3) | 0.11 |
| Cardiopulmonary resuscitation | 50 (66.7) | 58 (74.4) | 108 (70.6) | 0.37 |
| Therapeutic hypothermia | 19 (25.3) | 37 (47.4) | 56 (36.6) | 0.007 |
| Pulmonary edema | 63 (84.0) | 57 (73.1) | 120 (78.4) | 0.12 |
| Hemoglobin (g/L) | 128.2 (19.9) | 130.8 (21.8) | 129.6 (19.9) | 0.055 |
| Systolic pressure (mmHg) | 85.6 (25.8) | 91.5 (23.3) | 88.6 (24.7) | 0.14 |
| Diastolic pressure (mmHg) | 59.4 (16.2) | 62.5 (14.2) | 61.1 15.2) | 0.23 |
| Mean pressure (mmHg) | 70.6 (17.0) | 73.2 (15.7) | 72.0 (16.3) | 0.36 |
| GFR (mL/min/1.73 m2) | 49.4 (30.4, 64.1) | 57.5 (44.4, 71.2) | 53.0 (35.2, 68.9) | 0.031 |
| Radial access | 3 (4.0) | 2 (2.6) | 5 (3.3) | 0.68 |
| PCI LMCA | 13 (17.3) | 15 (19.2) | 28 (18.3) | 0.84 |
| PCI LAD | 28 (37.3) | 49 (62.8) | 77 (50.3) | 0.002 |
| PCI LCX | 11 (14.7) | 22 (28.2) | 33 (21.6) | 0.05 |
| PCI RCA | 12 (16.0) | 18 (23.1) | 30 (19.6) | 0.31 |
| Multivessel PCI | 15 (21.1) | 26 (39.4) | 41 (29.9) | 0.025 |
| Mechanical circulatory support | 16 (21.3) | 19 (24.3) | 35 (20.9) | 0.89 |
| P2Y12 | 39 (52.0) | 45 (57.7) | 84 (54.9) | 0.52 |
| Potent P2Y12 (prasugrel, ticagrelor) | 24 (32.0) | 26 (33.3) | 50 (32.7) | 0.86 |
| Bivalirudin | 3 (4.0) | 2 (2.6) | 5 (3.3) | 0.68 |
| TIMI 0/1 before PCI | 51 (68.0) | 60 (76.9) | 111 (72.5) | 0.28 |
| TIMI 0/1 after PCI | 26 (34.7) | 8 (10.3) | 34 (22.2) | <0.0001 |
| Tn, µg/L | 53.6 (57.2) | 63.1 (60.3) | 58.9 (58.7) | 0.44 |
| EF | 31.5 (5.9) | 31.0 (4.5) | 31.2 (5.2) | 0.59 |
| Bleeding | 31 (41.3) | 33 (42.3) | 64 (41.8) | 1.00 |
| Bleeding in P2Y12 patients | 18 (46.2) | 21 (46.7) | 39 (46.4) | 1.00 |
| Bleeding in potent P2Y12 patients | 9 (37.5) | 8 (30.8) | 17 (34.0) | 0.76 |
| Acute stent thrombosis | 3 (4.0) | 1 (1.3) | 4 (2.6) | 0.36 |
| CABG in the same hospitalization | 6 (8.0) | 2 (2.6) | 8 (5.2) | 0.16 |
| CPC | 2.86 (1.34) | 1.57 (0.98) | 1.89 (1.19) | 0.011 |
| Mortality outcome | ||||
| Death 30-day | 62 (82.7) | 54 (69.2) | 116 (75.8) | 0.06 |
| Death one-year | 64 (85.3) | 60 (76.9) | 124 (81.0) | 0.22 |
| 30-Day Mortality | One-Year Mortality | |||
|---|---|---|---|---|
| OR (95% CI) | p | HR (95% CI) | p | |
| Age | 1.04 (0.99 to 1.08) | 0.087 | 1.01 (0.99 to 1.03) | 0.30 |
| Male sex | 1.55 (0.53 to 4.50) | 0.42 | 0.87 (0.58 to 1.32) | 0.52 |
| Diabetes | 0.82 (0.22 to 3.08) | 0.77 | 0.96 (0.78 to 1.57) | 0.87 |
| Hypertension | 0.59 (0.18 to 1.93) | 0.38 | 1.03 (0.67 to 1.60) | 0.88 |
| Hyperlipidemia | 2.30 (0.48 to 11.34) | 0.29 | 0.99 (0.56 to 1.76) | 0.98 |
| GFR | 1.00 (0.98 to 1.02) | 0.99 | 1.00 (0.99 to 1.01) | 0.99 |
| STEMI | 0.65 (0.10 to 4.28) | 0.66 | 1.04 (0.58 to 1.86) | 0.90 |
| CPR | 1.89 (0.50 to 7.24) | 0.35 | 1.18 (0.72 to 1.92) | 0.51 |
| Therapeutic hypothermia | 0.54 (0.14 to 2.11) | 0.38 | 0.74 (0.45 to 1.22) | 0.23 |
| TIMI 0/1 after PCI | 1.75 (0.42 to 7.25) | 0.44 | 1.11 (0.68 to 1.80) | 0.67 |
| P2Y12 | 0.08 (0.02 to 0.32) | <0.0001 | 0.66 (0.45 to 0.98) | 0.035 |
| GPI | 0.53 (0.19 to 1.46) | 0.22 | 0.92 (0.62 to 1.34) | 0.70 |
| Bleeding | 3.25 (1.17 to 9.05) | 0.024 | 1.15 (0.77 to 1.72) | 0.48 |
| All Patients N = 153 | All Patients Receiving P2Y12 N = 84 | Patients Receiving Potent P2Y12 N = 50 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| No-GPI | GPI | p | No-GPI | GPI | p | No-GPI | GPI | ||
| TIMI flow before PCI | 0.84 (1.15) | 0.62 (0.87) | 0.17 | 0.82 (1.05) | 0.56 (0.84) | 0.20 | 0.71 (1.04) | 0.42 (0.81) | 0.28 |
| TIMI flow after PCI | 1.85 (1.27) | 2.54 (0.85) | <0.0001 | 2.0 (1.26) | 2.64 (0.77) | 0.005 | 1.88 (1.33) | 2.73 (0.60) | 0.005 |
| Improvement of TIMI flow ≥ 1 | 38 (50.7) | 68 (87.2) | <0.0001 | 23 (59.0) | 41 (91.1) | 0.001 | 13 (54.0) | 25 (96.2) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanic, V.; Kompara, G.; Suran, D. GP IIb/IIIa Receptor Inhibitors in Mechanically Ventilated Patients with Cardiogenic Shock due to Myocardial Infarction in the Era of Potent P2Y12 Receptor Antagonists. J. Clin. Med. 2022, 11, 7426. https://doi.org/10.3390/jcm11247426
Kanic V, Kompara G, Suran D. GP IIb/IIIa Receptor Inhibitors in Mechanically Ventilated Patients with Cardiogenic Shock due to Myocardial Infarction in the Era of Potent P2Y12 Receptor Antagonists. Journal of Clinical Medicine. 2022; 11(24):7426. https://doi.org/10.3390/jcm11247426
Chicago/Turabian StyleKanic, Vojko, Gregor Kompara, and David Suran. 2022. "GP IIb/IIIa Receptor Inhibitors in Mechanically Ventilated Patients with Cardiogenic Shock due to Myocardial Infarction in the Era of Potent P2Y12 Receptor Antagonists" Journal of Clinical Medicine 11, no. 24: 7426. https://doi.org/10.3390/jcm11247426
APA StyleKanic, V., Kompara, G., & Suran, D. (2022). GP IIb/IIIa Receptor Inhibitors in Mechanically Ventilated Patients with Cardiogenic Shock due to Myocardial Infarction in the Era of Potent P2Y12 Receptor Antagonists. Journal of Clinical Medicine, 11(24), 7426. https://doi.org/10.3390/jcm11247426