


Impact of Urinary Incontinence on Physical Function and Respiratory Muscle Strength in Incontinent Women: A Comparative Study between Urinary Incontinent and Apparently Healthy Women

 , , , ,
, , , ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Size
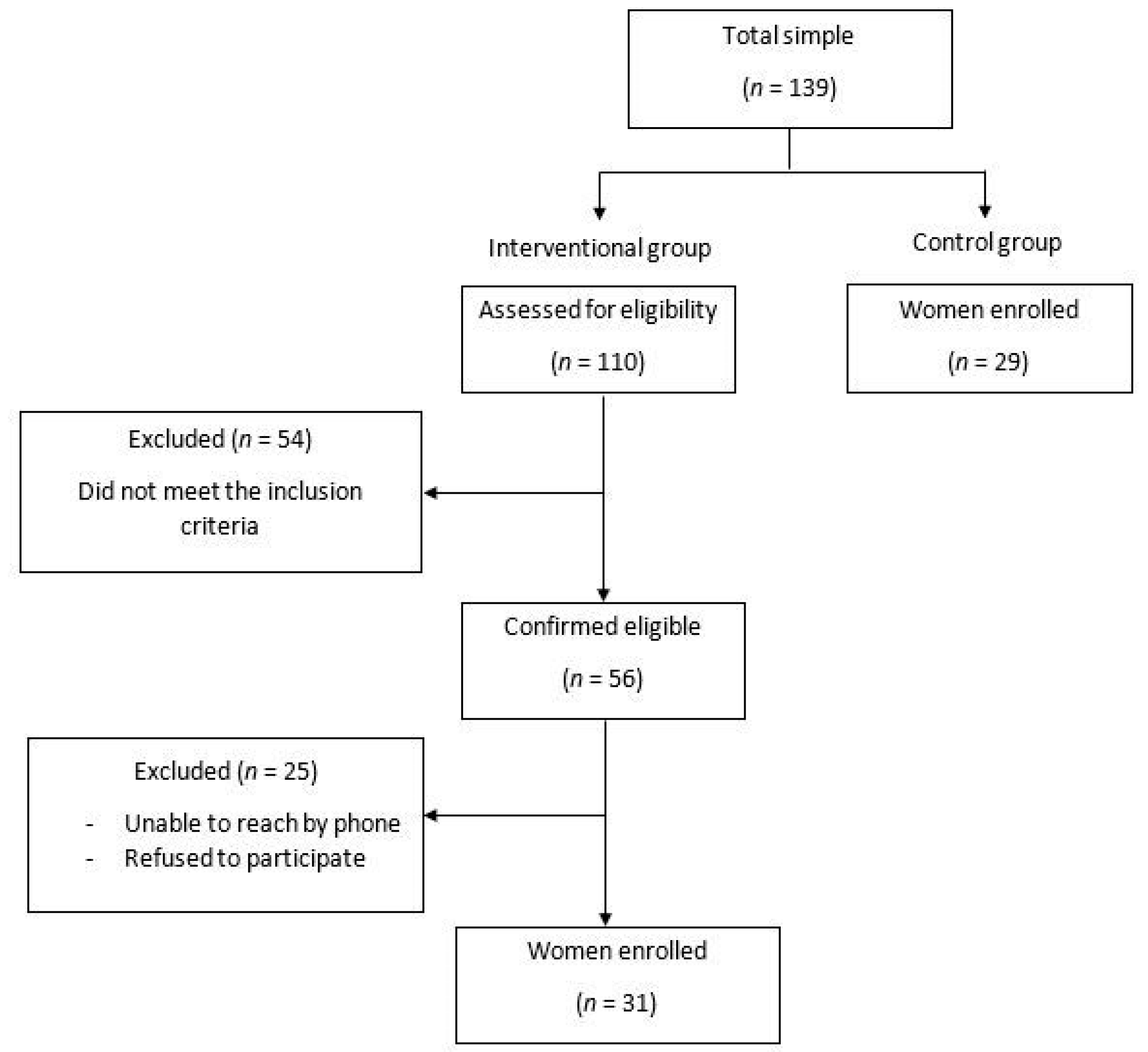
2.3. Participants: Intervention and Control Groups
2.4. Anthropometric Measurements
2.5. Urogenital Distress Inventory-6 (UDI-6)
2.6. Incontinence Impact Questionnaire-7 (IIQ-7)
2.7. The One-Hour Pad Test (Pad Test)
2.8. Respiratory Muscle Strength (RMS)
2.9. Physical Function (PF)
2.10. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Correlation of RMS (MIP and MEP) with SUI (UDI-6, IIQ-7, and Pad Test), PF (TUG, AMS at 60°/s, and AMS at 90°/s), WC, and BMI
3.3. Correlation of SUI (UDI-6, IIQ-7, and Pad Test) with PF (TUG, AMS at 60°/s, and AMS at 90°/s), WC, and BMI
3.4. Correlation of WC and BMI with PF (TUG, AMS at 60°/s, and AMSat 90°/s)
3.5. Associations between PF (TUG, AMS at 60°/s), WC, BMI, Fat Mass, and SUI (UDI-6 and Pad Test) with RMS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haylen, B.T.; de Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K.; et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int. Urogynecology J. 2010, 21, 5–26. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.A.; O’Sullivan, P.B.; Briffa, N.K.; Neumann, P. Altered muscle activation patterns in symptomatic women during pelvic floor muscle contraction and Valsalva manouevre. Neurourol. Urodyn. 2006, 25, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Hwang, U.J.; Lee, M.S.; Jung, S.H.; Ahn, S.H.; Kwon, O.Y. Effect of pelvic floor electrical stimulation on diaphragm excursion and rib cage movement during tidal and forceful breathing and coughing in women with stress urinary incontinence: A randomized controlled trial. Medicine 2021, 100, e24158. [Google Scholar] [CrossRef] [PubMed]
- Sapsford, R. Rehabilitation of pelvic floor muscles utilizing trunk stabilization. Man. Ther. 2004, 9, 3–12. [Google Scholar] [CrossRef]
- Navarro Brazalez, B.; Sanchez Sanchez, B.; Prieto Gomez, V.; De La Villa Polo, P.; McLean, L.; Torres Lacomba, M. Pelvic floor and abdominal muscle responses during hypopressive exercises in women with pelvic floor dysfunction. Neurourol. Urodyn. 2020, 39, 793–803. [Google Scholar] [CrossRef]
- Hodges, P.W.; Gandevia, S.C. Changes in intra-abdominal pressure during postural and respiratory activation of the human diaphragm. J. Appl. Physiol. 2000, 89, 967–976. [Google Scholar] [CrossRef]
- Talasz, H.; Kofler, M.; Kalchschmid, E.; Pretterklieber, M.; Lechleitner, M. Breathing with the pelvic floor? Correlation of pelvic floor muscle function and expiratory flows in healthy young nulliparous women. Int. Urogynecology J. 2010, 21, 475–481. [Google Scholar] [CrossRef]
- Talasz, H.; Kremser, C.; Kofler, M.; Kalchschmid, E.; Lechleitner, M.; Rudisch, A. Phase-locked parallel movement of diaphragm and pelvic floor during breathing and coughing—A dynamic MRI investigation in healthy females. Int. Urogynecology J. 2011, 22, 61–68. [Google Scholar] [CrossRef]
- Neumann, P.; Gill, V. Pelvic Floor and Abdominal Muscle Interaction: EMG Activity and Intra-abdominal Pressure. Int. Urogynecology J. 2002, 13, 125–132. [Google Scholar] [CrossRef]
- Kim, E.Y.; Kim, S.Y.; Oh, D.W. Pelvic floor muscle exercises utilizing trunk stabilization for treating postpartum urinary incontinence: Randomized controlled pilot trial of supervised versus unsupervised training. Clin. Rehabil. 2012, 26, 132–141. [Google Scholar] [CrossRef]
- Sapsford, R.R.; Hodges, P.W.; Richardson, C.A.; Cooper, D.H.; Markwell, S.J.; Jull, G.A. Co-activation of the abdominal and pelvic floor muscles during voluntary exercises. Neurourol. Urodyn. 2001, 20, 31–42. [Google Scholar] [CrossRef]
- Leitner, M.; Moser, H.; Taeymans, J.; Kuhn, A.; Radlinger, L. Pelvic floor muscle displacement during voluntary and involuntary activation in continent and incontinent women: A systematic review. Int. Urogynecology J. 2015, 26, 1587–1598. [Google Scholar] [CrossRef] [PubMed]
- Saunders, S.W.; Rath, D.; Hodges, P.W. Postural and respiratory activation of the trunk muscles changes with mode and speed of locomotion. Gait Posture 2004, 20, 280–290. [Google Scholar] [CrossRef]
- Azevedo, I.G.; Sousa, S.L.D.O.; Viana, E.D.S.R.; Dantas, D.D.S.; Maciel, Á.C.C.; Da Câmara, S.M.A. Relationship between symptomatic pelvic organ prolapse and respiratory muscle strength in middle-aged and older women in Northeast Brazil: A cross-sectional study. Physiother. Theory Pract. 2021, 37, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Zafra, S.; Del Corral, T.; Montero-Gonzalez, N.; de-Gabriel-Hierro, A.; Lopez-de-Uralde-Villanueva, I. Urinary incontinence and impaired physical function are associated with expiratory muscle weakness in patients with multiple sclerosis. Disabil. Rehabil. 2022, 44, 3531–3539. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- WHO. Physical status: The use and interpretation of anthropometry. In Report of a WHO Expert Committee; World Health Organ: Geneva, Switzerland, 1995; Volume 854, pp. 1–452. [Google Scholar]
- Bosy-Westphal, A.; Later, W.; Hitze, B.; Sato, T.; Kossel, E.; Glüer, C.-C.; Heller, M.; Müller, M.J. Accuracy of bioelectrical impedance consumer devices for measurement of body composition in comparison to whole body magnetic resonance imaging and dual X-ray absorptiometry. Obes. Facts 2008, 1, 319–324. [Google Scholar] [CrossRef]
- Mason, C.; Katzmarzyk, P. Variability in Waist Circumference Measurements According to Anatomic Measurement Site. Obesity 2009, 17, 1789–1795. [Google Scholar] [CrossRef]
- Ghroubi, S.; El Fani, N.; Elarem, S.; Alila, S.; Ben Ayed, H.; Borgi, O.; Chmak, J.; Elleuch, M.H. Arabic (Tunisian) translation and validation of the urogenital distress inventory short form (UDI-6) and incontinence impact questionnaire short form (IIQ-7). Arab. J. Urol. 2020, 18, 27–33. [Google Scholar] [CrossRef]
- Castro-Diaz, D.; Robinson, D.; Bosch, R.; Costantini, E.; Cotterill, N.; Espuna-Pons, M.; Kocjancic, E.; Lemos, N.; Tarcan, T.; Yoshida, M. Patient-reported outcome assessment. In Incontinence: Proceedings of the Sixth International Consultation on Incontinence, 6th ed.; Abrams, P., Cardozo, L., Wagg, A., Wein, A., Eds.; Health Publications Limited: Tokyo, Japan, 2017; pp. 541–598. [Google Scholar]
- Shumaker, S.A.; Wyman, J.F.; Uebersax, J.; McClish, D.; Fantl, J.A. Health-related quality of life measures for women with urinary incontinence: The Incontinence Impact Questionnaire and the Urogenital Distress Inventory. Qual. Life Res. 1994, 3, 291–306. [Google Scholar] [CrossRef] [PubMed]
- Skorupska, K.; Grzybowska, M.E.; Kubik-Komar, A.; Rechberger, T.; Miotla, P. Identification of the Urogenital Distress Inventory-6 and the Incontinence Impact Questionnaire-7 cutoff scores in urinary incontinent women. Health Qual. Life Outcomes 2021, 19, 87. [Google Scholar] [CrossRef] [PubMed]
- Uebersax, J.S.; Wyman, J.F.; Shumaker, S.A.; McClish, D.K. Short forms to assess life quality and symptom distress for urinary incontinence in women: The Incontinence Impact Questionnaire and the Urogenital Distress Inventory. Neurourol. Urodyn. 1995, 14, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; van Kerrebroeck, P.; Victor, A.; Wein, A. The standardisation of terminology of lower urinary tract function: Report from the Standardisation Sub-committee of the International Continence Society. Neurourol. Urodyn. 2002, 21, 167–178. [Google Scholar] [CrossRef]
- Laveneziana, P.; Albuquerque, A.; Aliverti, A.; Babb, T.; Barreiro, E.; Dres, M.; Dube, B.P.; Fauroux, B.; Gea, J.; Guenette, J.A.; et al. ERS statement on respiratory muscle testing at rest and during exercise. Eur. Respir. J. 2019, 53, 1801214. [Google Scholar] [CrossRef]
- Dimitriadis, Z.; Kapreli, E.; Konstantinidou, I.; Oldham, J.; Strimpakos, N. Test/retest reliability of maximum mouth pressure measurements with the MicroRPM in healthy volunteers. Respir. Care 2011, 56, 776–782. [Google Scholar] [CrossRef]
- Black, L.F.; Hyatt, R.E. Maximal respiratory pressures: Normal values and relationship to age and sex. Am. Rev. Respir. Dis. 1969, 99, 696–702. [Google Scholar]
- Harik-Khan, R.I.; Wise, R.A.; Fozard, J.L. Determinants of maximal inspiratory pressure. The Baltimore Longitudinal Study of Aging. Am. J. Respir. Crit. Care Med. 1998, 158, 1459–1464. [Google Scholar] [CrossRef]
- American Thoracic Society/European Respiratory Society. ATS/ERS Statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 2002, 166, 518–624. [Google Scholar] [CrossRef]
- Kammoun, R.; Ben Saad, H. From deficiency to handicap in the respiratory field: Lung function tests (LFT) norms and quality of life (QOL) questionnaires validated for the Tunisian population. La Tunis. Med. 2020, 98, 378–395. [Google Scholar]
- Evans, J.A.; Whitelaw, W.A. The assessment of maximal respiratory mouth pressures in adults. Respir. Care 2009, 54, 1348–1359. [Google Scholar] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Grabiner, M.D.; Jeziorowski, J.J. Isokinetic trunk extension and flexion strength-endurance relationships. Clin. Biomech. 1991, 6, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Leardini, A.; Biagi, F.; Merlo, A.; Belvedere, C.; Benedetti, M.G. Multi-segment trunk kinematics during locomotion and elementary exercises. Clin. Biomech. 2011, 26, 562–571. [Google Scholar] [CrossRef]
- Garcia-Vaquero, M.P.; Barbado, D.; Juan-Recio, C.; Lopez-Valenciano, A.; Vera-Garcia, F.J. Isokinetic trunk flexion-extension protocol to assess trunk muscle strength and endurance: Reliability, learning effect, and sex differences. J. Sport Health Sci. 2020, 9, 692–701. [Google Scholar] [CrossRef]
- Karatas, G.K.; Gogus, F.; Meray, J. Reliability of isokinetic trunk muscle strength measurement. Am. J. Phys. Med. Rehabil. 2002, 81, 79–85. [Google Scholar] [CrossRef]
- Karatas, M.; Cetin, N.; Bayramoglu, M.; Dilek, A. Trunk muscle strength in relation to balance and functional disability in unihemispheric stroke patients. Am. J. Phys. Med. Rehabil. 2004, 83, 81–87. [Google Scholar] [CrossRef]
- Sole, G.; Hamrén, J.; Milosavljevic, S.; Nicholson, H.; Sullivan, S.J. Test-retest reliability of isokinetic knee extension and flexion. Arch. Phys. Med. Rehabil. 2007, 88, 626–631. [Google Scholar] [CrossRef]
- Madsen, O.R. Trunk extensor and flexor strength measured by the Cybex 6000 dynamometer. Assessment of short-term and long-term reproducibility of several strength variables. Spine 1996, 21, 2770–2776. [Google Scholar] [CrossRef]
- Hopkins, W.G. Linear models and effect magnitudes for research, clinical and practical applications. Sportscience 2010, 14, 49–59. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Taylor and Francis: Hoboken, NJ, USA, 2013; pp. 23–26. [Google Scholar] [CrossRef]
- Szczygiel, E.; Blaut, J.; Zielonka-Pycka, K.; Tomaszewski, K.; Golec, J.; Czechowska, D.; Maslon, A.; Golec, E. The Impact of Deep Muscle Training on the Quality of Posture and Breathing. J. Mot. Behav. 2018, 50, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, F.; Lee, A.H.; Binns, C.W.; Nishimura, K.; Taniguchi, H. Association of impaired respiratory function with urinary incontinence. Respirology 2009, 14, 753–756. [Google Scholar] [CrossRef] [PubMed]
- Gacci, M.; Sebastianelli, A.; Salvi, M.; De Nunzio, C.; Tubaro, A.; Gravas, S.; Moncada, I.; Serni, S.; Maggi, M.; Vignozzi, L. The impact of central obesity on storage luts and urinary incontinence after prostatic surgery. Curr. Urol. Rep. 2016, 17, 61. [Google Scholar] [CrossRef] [PubMed]
- Nygaard, C.; Schreiner, L.; Morsch, T.; Saadi, R.; Figueiredo, M.; Padoin, A. Urinary Incontinence and Quality of Life in Female Patients with Obesity. Rev. Bras. Ginecol. Obs. RBGO Gynecol. Obstet. 2018, 40, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Townsend, M.K.; Danforth, K.N.; Rosner, B.; Curhan, G.C.; Resnick, N.M.; Grodstein, F. Body Mass Index, Weight Gain, and Incident Urinary Incontinence in Middle-Aged Women. Obstet. Gynecol. 2007, 110, 346–353. [Google Scholar] [CrossRef]
- Lamerton, T.J.; Torquati, L.; Brown, W.J. Overweight and obesity as major, modifiable risk factors for urinary incontinence in young to mid-aged women: A systematic review and meta-analysis. Obes. Rev. 2018, 19, 1735–1745. [Google Scholar] [CrossRef]
- Richter, H.E.; Creasman, J.M.; Myers, D.L.; Wheeler, T.L.; Burgio, K.L.; Subak, L.L. Urodynamic characterization of obese women with urinary incontinence undergoing a weight loss program: The Program to Reduce Incontinence by Diet and Exercise (PRIDE) trial. Int. Urogynecology J. Pelvic. Floor Dysfunct. 2008, 19, 1653–1658. [Google Scholar] [CrossRef]
- Dos Santos, K.M.; Da Roza, T.; Mochizuki, L.; Arbieto, E.R.M.; Tonon da Luz, S.C. Assessment of abdominal and pelvic floor muscle function among continent and incontinent athletes. Int. Urogynecology J. 2019, 30, 693–699. [Google Scholar] [CrossRef]
- Hung, H.-C.; Hsiao, S.-M.; Chih, S.-Y.; Lin, H.-H.; Tsauo, J.-Y. An alternative intervention for urinary incontinence: Retraining diaphragmatic, deep abdominal and pelvic floor muscle coordinated function. Man. Ther. 2010, 15, 273–279. [Google Scholar] [CrossRef]
- Madill, S.J.; McLean, L. Relationship between abdominal and pelvic floor muscle activation and intravaginal pressure during pelvic floor muscle contractions in healthy continent women. Neurourol. Urodyn. 2006, 25, 722–730. [Google Scholar] [CrossRef]
- Van Gerwen, M.; Schellevis, F.; Lagro-Janssen, T. Comorbidities associated with urinary incontinence: A case-control study from the Second Dutch National Survey of General Practice. J. Am. Board Fam. Med. 2007, 20, 608–610. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Ha, M. Effect of pelvic floor muscle exercises on pulmonary function. J. Phys. Ther. Sci. 2015, 27, 3233–3235. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Hwang, B.; Kim, Y. The impact of the pelvic floor muscles on dynamic ventilation maneuvers. J. Phys. Ther. Sci. 2015, 27, 3155–3157. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kucukkaya, B.; Kahyaoglu Sut, H. Effectiveness of pelvic floor muscle and abdominal training in women with stress urinary incontinence. Psychol. Health Med. 2021, 26, 779–786. [Google Scholar] [CrossRef]
- Chiu, A.F.; Huang, M.H.; Hsu, M.H.; Liu, J.L.; Chiu, J.F. Association of urinary incontinence with impaired functional status among older people living in a long-term care setting. Geriatr. Gerontol. Int. 2015, 15, 296–301. [Google Scholar] [CrossRef]
- Müller, R.; Ertelt, T.; Blickhan, R. Low back pain affects trunk as well as lower limb movements during walking and running. J. Biomech. 2015, 48, 1009–1014. [Google Scholar] [CrossRef]
- Smith, M.D.; Coppieters, M.W.; Hodges, P.W. Is balance different in women with and without stress urinary incontinence? Neurourol. Urodyn. Off. J. Int. Cont. Soc. 2008, 27, 71–78. [Google Scholar] [CrossRef]
- Chen, C.-H.; Huang, M.-H.; Chen, T.-W.; Weng, M.-C.; Lee, C.-L.; Wang, G.-J. Relationship between ankle position and pelvic floor muscle activity in female stress urinary incontinence. Urology 2005, 66, 288–292. [Google Scholar] [CrossRef]
- Triki, L.; Ben Saad, H. The impacts of parity on spirometric parameters: A systematic review. Expert Rev. Respir. Med. 2021, 15, 1169–1185. [Google Scholar] [CrossRef]
- Ben Saad, H.; Tfifha, M.; Harrabi, I.; Tabka, Z.; Guenard, H.; Hayot, M.; Zbidi, A. [Factors influencing pulmonary function in Tunisian women aged 45 years and more]. Rev. Mal. Respir. 2006, 23, 324–338. [Google Scholar] [CrossRef]
- Lemos, A.; Souza, A.I.; Andrade, A.D.; Figueiroa, J.N.; Cabral-Filho, J.E. Respiratory muscle strength: Comparison between primigravidae and nulligravidae. J. Bras. Pneumol. 2011, 37, 193–199. [Google Scholar] [CrossRef] [PubMed][Green Version]


{kind=link}
| Incontinence Group (n = 31) | Control Group (n = 29) | p-Value | Effect Size | |
|---|---|---|---|---|
| Age (years), mean (SD) | 53.2 (7.3) | 51.2 (6.1) | 0.25 a | 0.15 z |
| Body height (m), mean (SD) | 1.6 (0.1) | 1.6 (0.06) | 0.09 a | 0 z |
| Body weight (kg), median (IQR) | 72.6 (67.1 to 80.7) | 69.2 (64.to 72.6) | 0.01 b | 0.30 z |
| Fat mass (kg), mean (SD) | 28.1 (3.2) | 25.2 (4.9) | 0.005 | 0.35z |
| Body mass index (kg/m2), median (IQR) | 27.4 (25.8 to 30.4) | 24.8 (24.01 to 26.3) | <0.001 b | 0.50 z |
| Waist circumference (cm), median (IQR) | 93 (90 to 100) | 84.0 (81 to 89.5) | 0.001 b | 0.67 Q |
| Urinary incontinence | ||||
| UDI-6, median (IQR) | 42 (37.5 to 54) | 4.2 (0 to 8.3) | 0.001 b | 0.86 X |
| IIQ-7, median (IQR) | 41.6 (29.2 to 50) | 0.0(0 to 4.2) | <0.001 b | 0.87 X |
| Pad test, median (IQR) | 13.0 (8 to 21) | 0.2 (0.09 to 0.6) | <0.001 b | 0.85 X |
| Physical function | ||||
| TUG (s), median (IQR) | 8.9 (7.6 to 9.7) | 6.8 (6.4 to 7.1)) | <0.001 b | 0.72 X |
| AMS at 60°/s (N.m), median (IQR) | 102.0 (72 to 113) | 120.0(110.5 to 128)) | <0.001 b | 0.62 z |
| AMS at 90°/s (N.m) median (IQR) | 90.0 (60 to 102) | 106.0 (97.5 to 117) | <0.001 b | 0.50 z |
| RMS (cmH2O) | ||||
| MIP, mean (SD) | 67.2 (5.5) | 80.1 (4.8) | <0.001 a | 0.78 X |
| MEP, median (IQR) | 79.0 (73 to 86) | 89.0 (81.5 to 92.5) | <0.001 b | 0.50 z |
| RMS (% predicted value) | ||||
| MIP, median (IQR) | 87.5 (81.9 to 96.5) | 103.4 (96.8 to 104.8) | <0.001 b | 0.73 X |
| MEP, mean (SD) | 93.6 (9.4) | 101.1 (5.9) | 0.001 a | 0.43 z |
| RMS | Incontinence group | Predicted value | p-value | |
| MIP vs. MIPref, mean (SD) | 67.2 (5.5) | 75.5 (4.5) | <0.001 c | 0.63 z |
| MEP vs. MEPref, median (IQR) | 79 (73 to 86) | 83.7 (80 to 89.7) | 0.001 d | 0.31 z |
| RMS | SUI | WC | BMI | PF | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MIP | MEP | UDI-6 | IIQ-7 | Pad Test | Functional Mobility (TUG) | AMS at 60°/s | AMS at 90°/s | |||||
| RMS | MIP | - | 0.51 **b | −0.28 | −0.36 *a | −0.09 | −0.27 | −0.13 | −0.32 | 0.38 *a | 0.29 | |
| MEP | 0.51 **b | - | −0.64 **b | −0.61 **b | −0.45 *a | −0.35 *a | −0.28 | −0.65 **b | 0.69 **b | 0.62 *b | ||
| SUI | UDI-6 | −0.28 | −0.64 **b | - | 0.78 **c | 0.80 **c | 0.62 **b | 0.52 **b | 0.73 **c | −0.68 **b | −0.53 **b | |
| IIQ-7 | −0.36 *a | −0.61 **b | 0.78 **c | - | 0.74 **c | 0.47 **a | 0.29 | 0.74 **c | −0.73 **c | −0.58 **b | ||
| Pad test | −0.09 | −0.45 *a | 0.80 **c | 0.74 **c | - | 0.57 **b | 0.30 | 0.67 **b | −0.63 **b | −0.46 **a | ||
| WC | −0.27 | −0.35 *a | 0.62 **b | 0.47 **a | 0.57 **b | - | 0.74 **c | 0.55 **b | −0.42 *a | −0.26 | ||
| BMI | −0.13 | −0.28 | 0.52 **b | 0.29 | 0.30 | 0.74 **c | 0.40 * a | −0.17 | 0.004 | |||
| PF | Functional mobility (TUG) | −0.32 | −0.65 **b | 0.73 **c | 0.74 **c | 0.67 **b | −0.55 **b | 0.40 *a | - | −0.80 **c | −0.72 **c | |
| AMS at 60°/s | 0.38 *a | 0.69 **b | −0.68 **b | −0.73 **c | −0.63 **b | −0.42 *a | −017 | −0.80 **c | - | 0.88 **c | ||
| AMS at 90°/s | 0.29 | 0.62 *b | −0.53 **b | −0.58 **b | −0.46 **a | −0.26 | 0.004 | −0.72 **c | 0.88 **c | - | ||
| Variables | Unstandardized B | 95% CI | p-Value | |
|---|---|---|---|---|
| MEP | Fat mass | 0.463 | 0.038–0.889 | 0.034 a |
| BMI | −1.135 | −2.212–−0.057 | 0.04 a | |
| WC | 0.277 | −0.166–0.720 | 0.209 a | |
| Pad test | 0.161 | −0.368–0.664 | 0.559 a | |
| UDI-6 | −0.354 | −0.691–−0.016 | 0.041 a | |
| TUG | −0.153 | −2.903–2.597 | 0.909 a | |
| AMS at 60°/s | 0.161 | 0.007–0.315 | 0.041 a | |
| MIP | Fat mass | 0.414 | −0.023–0.850 | 0.062 a |
| BMI | −0.834 | −1.938–0.271 | 0.132 a | |
| WC | 0.015 | −0.439–0.469 | 0.946 a | |
| Pad test | 0.362 | −0.167–0.891 | 0.170 a | |
| UDI-6 | −0.222 | −0.568–0.124 | 0.197 a | |
| TUG | 0.309 | −2.510–3.128 | 0.823 a | |
| AMS at 60°/s | 0.106 | −0.052–0.263 | 0.180 a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abidi, S.; Ghram, A.; Ghroubi, S.; Ahmaidi, S.; Elleuch, M.H.; Girard, O.; Papasavvas, T.; Laukkanen, J.; Ben Saad, H.; Knechtle, B.; et al. Impact of Urinary Incontinence on Physical Function and Respiratory Muscle Strength in Incontinent Women: A Comparative Study between Urinary Incontinent and Apparently Healthy Women. J. Clin. Med. 2022, 11, 7344. https://doi.org/10.3390/jcm11247344
Abidi S, Ghram A, Ghroubi S, Ahmaidi S, Elleuch MH, Girard O, Papasavvas T, Laukkanen J, Ben Saad H, Knechtle B, et al. Impact of Urinary Incontinence on Physical Function and Respiratory Muscle Strength in Incontinent Women: A Comparative Study between Urinary Incontinent and Apparently Healthy Women. Journal of Clinical Medicine. 2022; 11(24):7344. https://doi.org/10.3390/jcm11247344
Chicago/Turabian StyleAbidi, Sirine, Amine Ghram, Sameh Ghroubi, Said Ahmaidi, Mohamed Habib Elleuch, Olivier Girard, Theodoros Papasavvas, Jari Laukkanen, Helmi Ben Saad, Beat Knechtle, and et al. 2022. "Impact of Urinary Incontinence on Physical Function and Respiratory Muscle Strength in Incontinent Women: A Comparative Study between Urinary Incontinent and Apparently Healthy Women" Journal of Clinical Medicine 11, no. 24: 7344. https://doi.org/10.3390/jcm11247344
APA StyleAbidi, S., Ghram, A., Ghroubi, S., Ahmaidi, S., Elleuch, M. H., Girard, O., Papasavvas, T., Laukkanen, J., Ben Saad, H., Knechtle, B., Weiss, K., & Chlif, M. (2022). Impact of Urinary Incontinence on Physical Function and Respiratory Muscle Strength in Incontinent Women: A Comparative Study between Urinary Incontinent and Apparently Healthy Women. Journal of Clinical Medicine, 11(24), 7344. https://doi.org/10.3390/jcm11247344