
Fractional Flow Reserve versus Angiography–Guided Management of Coronary Artery Disease: A Meta–Analysis of Contemporary Randomised Controlled Trials
 , , , and
, , , and
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
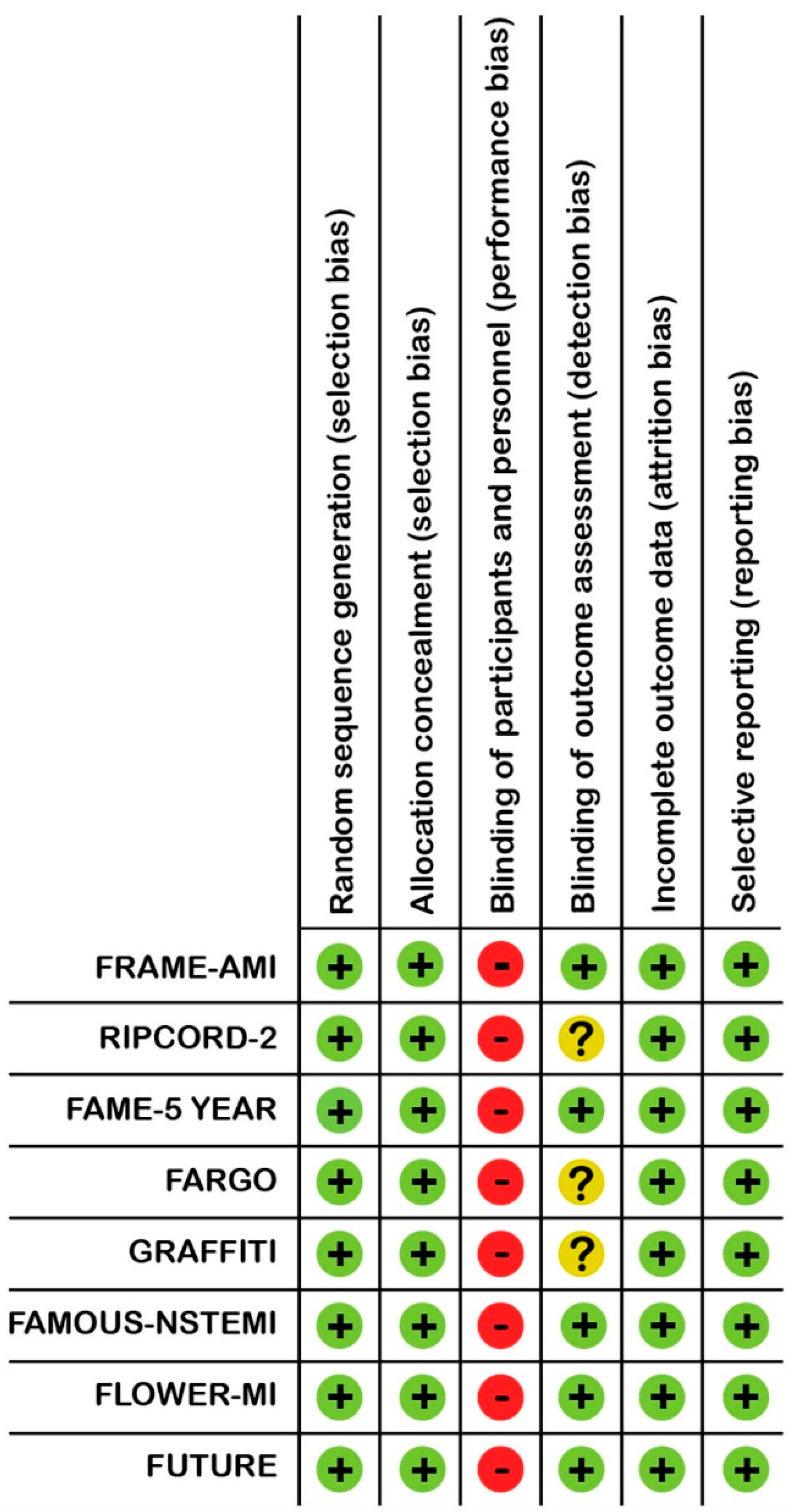
2.4. Quality Assessment
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Included RCTs
3.2. Baseline Characteristics of the Population
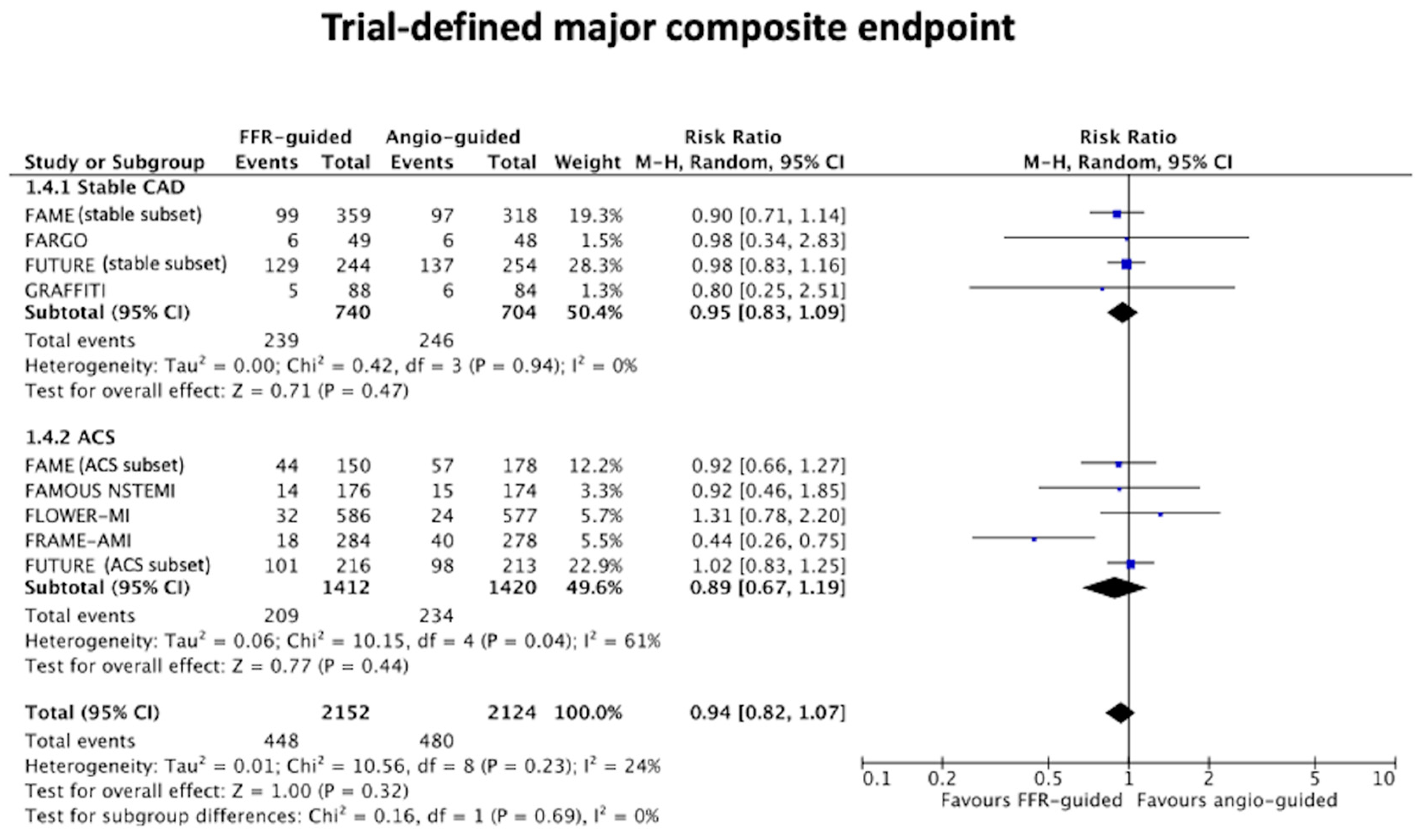
3.3. Clinical Endpoints
3.4. Revascularisation and Stent Implanted per Allocated Strategy
4. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e4–e17. [Google Scholar] [CrossRef]
- van Nunen, L.X.; Zimmermann, F.M.; Tonino, P.A.L.; Barbato, E.; Baumbach, A.; Engstrøm, T.; Klauss, V.; A MacCarthy, P.; Manoharan, G.; Oldroyd, K.G.; et al. Fractional flow reserve versus angiography for guidance of PCI in patients with multivessel coronary artery disease (FAME): 5-year follow-up of a randomised controlled trial. Lancet 2015, 386, 1853–1860. [Google Scholar] [CrossRef]
- Hahn, J.Y. FFR vs. Angiography-guided PCI in AMI with multivessel disease—FRAME-AMI trial. In Proceedings of the European Society of Cardiology Conference, Barcelona, Spain, 27–31 August 2022. [Google Scholar]
- Stables, R.H.; Mullen, L.J.; Elguindy, M.; Nicholas, Z.; Aboul-Enien, Y.H.; Kemp, I.; O’Kane, P.; Hobson, A.; Johnson, T.W.; Khan, S.Q.; et al. Routine Pressure Wire Assessment Versus Conventional Angiography in the Management of Patients with Coronary Artery Disease: The RIPCORD 2 Trial. Circulation 2022, 146, 687–698. [Google Scholar] [CrossRef]
- Thuesen, A.L.; Riber, L.; Veien, K.T.; Christiansen, E.H.; Jensen, S.E.; Modrau, I.S.; Andreasen, J.J.; Junker, A.; Mortensen, P.E.; Jensen, L.O. Fractional Flow Reserve Versus Angiographically-Guided Coronary Artery Bypass Grafting. J. Am. Coll. Cardiol. 2018, 72, 2732–2743. [Google Scholar] [CrossRef]
- Toth, G.G.; De Bruyne, B.; Kala, P.; Ribichini, F.L.; Casselman, F.; Ramos, R.; Piroth, Z.; Fournier, S.; Piccoli, A.; Van Mieghem, C.; et al. Graft patency after FFR-guided versus angiography-guided coronary artery bypass grafting: The GRAFFITI trial. EuroIntervention 2019, 15, e999–e1005. [Google Scholar] [CrossRef]
- Puymirat, E.; Cayla, G.; Simon, T.; Steg, P.G.; Montalescot, G.; Durand-Zaleski, I.; le Bras, A.; Gallet, R.; Khalife, K.; Morelle, J.-F.; et al. Multivessel PCI Guided by FFR or Angiography for Myocardial Infarction. N. Engl. J. Med. 2021, 385, 297–308. [Google Scholar] [CrossRef]
- Rioufol, G.; Dérimay, F.; Roubille, F.; Perret, T.; Motreff, P.; Angoulvant, D.; Cottin, Y.; Meunier, L.; Cetran, L.; Cayla, G.; et al. Fractional Flow Reserve to Guide Treatment of Patients with Multivessel Coronary Artery Disease. J. Am. Coll. Cardiol. 2021, 78, 1875–1885. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Layland, J.; Oldroyd, K.G.; Curzen, N.; Sood, A.; Balachandran, K.; Das, R.; Junejo, S.; Ahmed, N.; Lee, M.M.; Shaukat, A.; et al. Fractional flow reserve vs. angiography in guiding management to optimize outcomes in non-ST-segment elevation myocardial infarction: The British Heart Foundation FAMOUS-NSTEMI randomized trial. Eur. Heart J. 2014, 36, 100–111. [Google Scholar] [CrossRef]
- Elbadawi, A.; Sedhom, R.; Dang, A.T.; Gad, M.M.; Rahman, F.; Brilakis, E.S.; Elgendy, I.Y.; Jneid, H. Fractional flow reserve versus angiography alone in guiding myocardial revascularisation: A systematic review and meta-analysis of randomised trials. Heart 2022, 108, 1699–1706. [Google Scholar] [CrossRef]
- Prasad, R.M.; Baloch, Z.Q.; Gumbita, R. Updated meta-analysis comparing FFR-guided and angiographic-guided intervention in patients with multivessel coronary artery disease. Int. J. Heart Vasc. Syst. 2022, 2, 6–10. [Google Scholar]
- Quintella, E.F.; Ferreira, E.; Azevedo, V.M.P.; Araujo, D.V.; Sant’anna, F.M.; Amorim, B.; De Albuquerque, D.C. Clinical Outcomes and Cost-Effectiveness Analysis of FFR Compared with Angiography in Multivessel Disease Patient. Arq. Bras. Cardiol. 2018, 112, 40–47. [Google Scholar] [CrossRef]
- Park, S.H.; Jeon, K.-H.; Lee, J.M.; Nam, C.-W.; Doh, J.-H.; Lee, B.-K.; Rha, S.-W.; Yoo, K.-D.; Jung, K.T.; Cho, Y.-S.; et al. Long-Term Clinical Outcomes of Fractional Flow Reserve–Guided Versus Routine Drug-Eluting Stent Implantation in Patients with Intermediate Coronary Stenosis: Five-Year Clinical Outcomes of DEFER-DES Trial. Circ. Cardiovasc. Interv. 2015, 8, e002442. [Google Scholar] [CrossRef]
- Chen, S.-L.; Ye, F.; Zhang, J.-J.; Xu, T.; Tian, N.-L.; Liu, Z.-Z.; Lin, S.; Shan, S.-J.; Ge, Z.; You, W.; et al. Randomized Comparison of FFR-Guided and Angiography-Guided Provisional Stenting of True Coronary Bifurcation Lesions: The DKCRUSH-VI Trial (Double Kissing Crush Versus Provisional Stenting Technique for Treatment of Coronary Bifurcation Lesions VI). JACC Cardiovasc. Interv. 2015, 8, 536–546. [Google Scholar] [CrossRef]
- Matthews, C.J.; Naylor, K.; Blaxill, J.M.; Greenwood, J.P.; Mozid, A.M.; Rossington, J.A.; Veerasamy, M.; Wheatcroft, S.B.; Bulluck, H. Meta-Analysis Comparing Clinical Outcomes of Fractional-Flow-Reserve- and Angiography-Guided Multivessel Percutaneous Coronary Intervention. Am. J. Cardiol. 2022, 184, 160–162. [Google Scholar] [CrossRef]
- Tonino, P.A.L.; De Bruyne, B.; Pijls, N.H.J.; Siebert, U.; Ikeno, F.; van’t Veer, M.; Klauss, V.; Manoharan, G.; Engstrøm, T.; Oldroyd, K.G.; et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N. Engl. J. Med. 2009, 360, 213–224. [Google Scholar] [CrossRef]
- White, C.W.; Wright, C.B.; Doty, D.B.; Hiratza, L.F.; Eastham, C.L.; Harrison, D.G.; Marcus, M.L. Does Visual Interpretation of the Coronary Arteriogram Predict the Physiologic Importance of a Coronary Stenosis? N. Engl. J. Med. 1984, 310, 819–824. [Google Scholar] [CrossRef]
- Curzen, N.; Rana, O.; Nicholas, Z.; Golledge, P.; Zaman, A.; Oldroyd, K.; Hanratty, C.; Banning, A.; Wheatcroft, S.; Hobson, A.; et al. Does Routine Pressure Wire Assessment Influence Management Strategy at Coronary Angiography for Diagnosis of Chest Pain? Circ. Cardiovasc. Interv. 2014, 7, 248–255. [Google Scholar] [CrossRef]
- Shaw, L.J.; Berman, D.S.; Maron, D.J.; Mancini, G.B.J.; Hayes, S.W.; Hartigan, P.M.; Weintraub, W.S.; O’Rourke, R.A.; Dada, M.; Spertus, J.A.; et al. Optimal Medical Therapy with or Without Percutaneous Coronary Intervention to Reduce Ischemic Burden: Results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation 2008, 117, 1283–1291. [Google Scholar] [CrossRef]
- Pijls, N.H.; A van Son, J.; Kirkeeide, R.L.; De Bruyne, B.; Gould, K.L. Experimental basis of determining maximum coronary, myocardial, and collateral blood flow by pressure measurements for assessing functional stenosis severity before and after percutaneous transluminal coronary angioplasty. Circulation 1993, 87, 1354–1367. [Google Scholar] [CrossRef]
- Stone, G.W.; Maehara, A.; Lansky, A.J.; de Bruyne, B.; Cristea, E.; Mintz, G.S.; Mehran, R.; McPherson, J.; Farhat, N.; Marso, S.P.; et al. A Prospective Natural-History Study of Coronary Atherosclerosis. N. Engl. J. Med. 2011, 364, 226–235. [Google Scholar] [CrossRef]
- Kedhi, E.; Berta, B.; Roleder, T.; Hermanides, R.S.; Fabris, E.; Ijsselmuiden, A.J.J.; Kauer, F.; Alfonso, F.; von Birgelen, C.; Escaned, J.; et al. Thin-cap fibroatheroma predicts clinical events in diabetic patients with normal fractional flow reserve: The COMBINE OCT–FFR trial. Eur. Heart J. 2021, 42, 4671–4679. [Google Scholar] [CrossRef]
- Smith, C.T.; Marcucci, M.; Nolan, S.J.; Iorio, A.; Sudell, M.; Riley, R.; Rovers, M.M.; Williamson, P.R. Individual participant data meta-analyses compared with meta-analyses based on aggregate data. Cochrane Database Syst. Rev. 2016, 2016, MR000007. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year Published | Enrolment Centres | Participants and Presentation | Primary Endpoint | Follow-Up (Years) | Loss to Follow- Up, n (%) | Findings |
|---|---|---|---|---|---|---|---|
| FRAME-AMI [3] (NCT02715518) | 2022 | 14 sites in Korea | 562 patients (STEMI/ NSTEMI) | MACE defined as the composite of death, MI, or unplanned revascularisation | 3.5 | 0.4 | Lower composite rates of death, MI, or unplanned revascularisation with FFR-guidance vs. angiography-guidance (7.4% vs. 19.7%, hazard ratio: 0.43 [95% CI: 0.25, 0.75] p = 0.003) |
| RIPCORD-2 [4] (NCT02892903) | 2022 | 17 sites in United Kingdom | 1100 patients (stable angina/ NSTEMI) | Total hospital cost and quality of life | 1 | 0.3 | No difference in median hospital costs or quality of life for FFR-guidance vs. angiography-guidance. No difference in the composite of death, stroke, MI, or unplanned revascularisation for FFR-guidance vs. angiography-guidance (9.5% vs. 8.7%, p = 0.064). |
| FAME 5 year [2] (NCT00267774) | 2015 | 20 sites in the United States and Europe | 1005 patients (stable/unstable Angina) | MACE defined as the composite of death, MI, or unplanned revascularisation | 5 | 7.5 | At 5 years, no difference in the composite of death, MI, or unplanned revascularisation with FFR -guidance vs. angiography-guidance (28% vs. 31%, relative risk: 0.91 [95% CI: 0.75, 1.10] p = 0.31). At 2 years, MACE was lower with FFR-guidance vs. angiography-guidance. Number of stents implanted per patient was lower with FFR-guidance vs. angiography-guidance (mean 1.9 ± 1.3 vs. 2.7 ± 1.2, p< 0.0001). |
| FARGO [5] (NCT02477371) | 2018 | 3 sites in Denmark | 100 patients (stable angina/ NSTEMI) | Graft failure in the percentage of all grafts | 0.5 | 0.0 (for MACE) 25.0 (for angiogram follow-up at 6 months) | No difference in graft failure rates with FFR guidance vs. angiography-guidance (16% vs. 12%, p = 0.97). No difference in the composite of death, nonprocedural MI, unplanned revascularisation and stroke with FFR-guidance vs. angiography-guidance (12% vs. 12%, p = 0.97). |
| GRAFFITI [6] (NCT01810224) | 2019 | 6 sites in Europe | 172 patients (stable angina/ NSTEMI) | Graft occlusion | 1 | 1.7 (for MACE) 35.5 (for Coronary imaging follow- up at 6 months) | No difference in graft failure rates with FFR- guidance vs. angiography-guidance (19% vs. 20%, p = 0.885). No difference in the composite of death, MI, unplanned revascularisation and stroke with FFR-guidance vs. angiography-guidance (3.7% vs. 7.1%, hazard ratio: 1.28 [95% CI: 0.39, 4.16], p = 0.687). |
| FAMOUS- NSTEMI [12] (NCT01764334) | 2014 | 6 sites in the United Kingdom | 350 patients (NSTEMI) | Proportion of patients allocated to medical management | 1 | 0.0 | Higher proportion of patients initially treated by medical therapy with FFR-guidance vs. angiography guidance (22.7% vs. 13.2%, p = 0.022). No difference in the composite of cardiovascular death, MI, or unplanned hospitalisation for heart failure (8.0% vs. 8.6%, risk difference −0.7% [95% CI: −6.7, 5.3%] p = 0.89). |
| FLOWER-MI [7] (NCT02943954) | 2021 | 41 sites in France | 1163 patients (STEMI) | MACE defined as the composite of death, MI, and unplanned hospitalisation leading to urgent revascularisation | 1 | 0.4 | At 5 years, no difference in the composite of death, MI and urgent revascularisation with FFR- guidance vs. angiography-guidance (5.5% vs. 4.2%, hazard ratio: 1.32 [95% CI: 0.78, 2.23] p = 0.31). |
| FUTURE [8] (NCT01881555) | 2021 | 31 sites in France | 927 patients (stable angina/ ACS/atypical chest pain/ silent ischaemia) | Composite of death, MI, stroke or unplanned revascularisation | 1 | 0.1 | No difference in the composite of death, MI, stroke or unplanned revascularisation with FFR-guidance vs. angiography-guidance (14.6% vs. 14.4%, hazard ratio: 0.97 [95% CI: 0.69, 1.36], p = 0.85). |
| Study | Strategy | Age, Years (Mean ± SD, or Median [IQR]) | Male (%) | Diabetes Mellitus (%) | Smoker (%) | ACS Presentation (%) | Treatment with CABG (%) | Procedure Time for PCI, Mins (Mean ± SD, or Median IQR]) | FFR Cut-Off | Angiogram Visual Stenosis Threshold for PCI (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| FRAME-AMI [3] (NCT02715518) | Angio (n = 278) | 62.7 ± 11.5 | 84.2 | 30.9 | 37.8 | 100.0 | 0 | Not reported | NA | >50 |
| FFR (n = 284) | 63.9 ± 11.4 | 84.5 | 34.2 | 32.0 | 100.0 | 0 | Not reported | ≤0.8 | NA | |
| RIPCORD-2 [4] (NCT02892903) | Angio (n = 552) | 64.3 ± 10.2 | 77.2 | 17.6 | 65.0 | 53.1 | 9.2 | 42.4 ± 27.0 | NA | ≥30 |
| FFR (n = 548) | 64.3 ± 10.0 | 73.5 | 20.6 | 58.5 | 50.4 | 11.9 | 69.0 ± 27.0 | ≤0.8 | NA | |
| FAME 5 year [2] (NCT00267774) | Angio (n = 496) | 63.9 ± 10.0 | 74.0 | 25.0 | 30.0 | 31.3 | 0 | 70.0 ± 44 | NA | >50 |
| FFR (n = 509) | 64.5 ± 10.4 | 75.0 | 22.0 | 25.0 | 25.1 | 0 | 71.0 ± 43 | ≤0.8 | NA | |
| FARGO [5] (NCT02477371) | Angio (n = 48) | 65.3 ± 8.8 | 89.0 | 23.0 | 17.0 | 14.0 | 100.0 | NA | NA | ≥50 |
| FFR (n = 49) | 66.4 ± 6.4 | 88.0 | 22.0 | 27.0 | 31.0 | 100.0 | NA | ≤0.8 | NA | |
| GRAFFITI [6] (NCT01810224) | Angio (n = 84) | 67 (63, 72) | 79.00 | 40.0 | 42.0 | 11.0 (for entire population) | 100.0 | NA | NA | ≥30 |
| FFR (n = 88) | 67 (62, 72) | 83.0 | 35.0 | 53.0 | 100.0 | NA | ≤0.8 | NA | ||
| FAMOUS- NSTEMI [2] (NCT01764334) | Angio (n = 174) | 61.6 ± 11.1 | 73.0 | 14.9 | 40.8 | 100 | 6.9 | 70.5 ± 33.5 | NA | ≥30 |
| FFR (n = 176) | 62.3 ± 11.0 | 75.6 | 14.8 | 40.9 | 100 | 6.2 | 66.5 ± 23.4 | ≤0.8 | NA | |
| FLOWER-MI [7] (NCT02943954) | Angio (n = 577) | 61.9 ± 11.4 | 81.1 | 14.2 | 36.4 | 100 | 0 | 32.0 (20.0, 24.0) | NA | ≥50 |
| FFR (n = 586) | 62.5 ± 11.0 | 85.0 | 18.3 | 40.1 | 100 | 0 | 31.0 (21, 45) | ≤0.8 | NA | |
| FUTURE [8] (NCT01881555) | Angio (n = 467) | 66.0 ± 11.0 | 82.0 | 32.0 | 26.0 | 46.0 | 12.0 | Not reported | NA | ≥50 |
| FFR (n = 460) | 65.0 ± 10.0 | 85.0 | 31.0 | 24.0 | 47.0 | 12.0 | Not reported | ≤0.8 | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maznyczka, A.M.; Matthews, C.J.; Blaxill, J.M.; Greenwood, J.P.; Mozid, A.M.; Rossington, J.A.; Veerasamy, M.; Wheatcroft, S.B.; Curzen, N.; Bulluck, H. Fractional Flow Reserve versus Angiography–Guided Management of Coronary Artery Disease: A Meta–Analysis of Contemporary Randomised Controlled Trials. J. Clin. Med. 2022, 11, 7092. https://doi.org/10.3390/jcm11237092
Maznyczka AM, Matthews CJ, Blaxill JM, Greenwood JP, Mozid AM, Rossington JA, Veerasamy M, Wheatcroft SB, Curzen N, Bulluck H. Fractional Flow Reserve versus Angiography–Guided Management of Coronary Artery Disease: A Meta–Analysis of Contemporary Randomised Controlled Trials. Journal of Clinical Medicine. 2022; 11(23):7092. https://doi.org/10.3390/jcm11237092
Chicago/Turabian StyleMaznyczka, Annette M., Connor J. Matthews, Jonathan M. Blaxill, John P. Greenwood, Abdul M. Mozid, Jennifer A. Rossington, Murugapathy Veerasamy, Stephen B. Wheatcroft, Nick Curzen, and Heerajnarain Bulluck. 2022. "Fractional Flow Reserve versus Angiography–Guided Management of Coronary Artery Disease: A Meta–Analysis of Contemporary Randomised Controlled Trials" Journal of Clinical Medicine 11, no. 23: 7092. https://doi.org/10.3390/jcm11237092
APA StyleMaznyczka, A. M., Matthews, C. J., Blaxill, J. M., Greenwood, J. P., Mozid, A. M., Rossington, J. A., Veerasamy, M., Wheatcroft, S. B., Curzen, N., & Bulluck, H. (2022). Fractional Flow Reserve versus Angiography–Guided Management of Coronary Artery Disease: A Meta–Analysis of Contemporary Randomised Controlled Trials. Journal of Clinical Medicine, 11(23), 7092. https://doi.org/10.3390/jcm11237092