
Prognostic Factors and a Model for Occult Breast Cancer: A Population-Based Cohort Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Variable Retrieval and Definition
2.3. Statistical Analyses
3. Results
3.1. Patients’ Characteristics
3.2. Risk Factors for LN Metastasis
3.3. Prognostic Impact of PLNR on BCSS
3.4. Survival and Prognosis
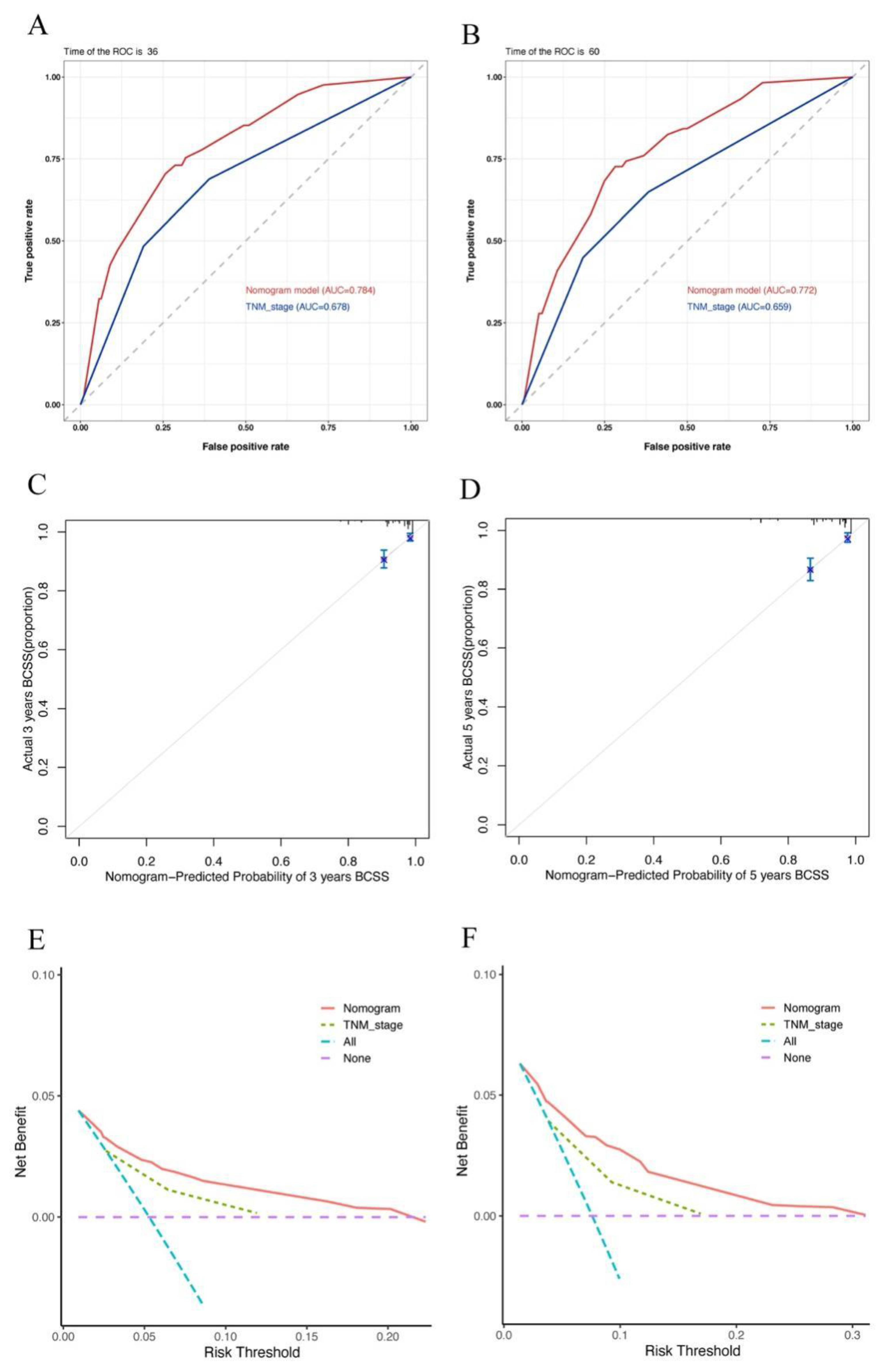
3.5. Nomogram Construction and Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sohn, G.; Son, B.H.; Lee, S.J.; Kang, E.Y.; Jung, S.H.; Cho, S.H.; Baek, S.; Lee, Y.R.; Kim, H.J.; Ko, B.S.; et al. Treatment and survival of patients with occult breast cancer with axillary lymph node metastasis: A nationwide retrospective study. J. Surg. Oncol. 2014, 110, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Walker, G.V.; Smith, G.L.; Perkins, G.H.; Oh, J.L.; Woodward, W.; Yu, T.K.; Hunt, K.K.; Hoffman, K.; Strom, E.A.; Buchholz, T.A. Population-based analysis of occult primary breast cancer with axillary lymph node metastasis. Cancer 2010, 116, 4000–4006. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.; Nemoto, T.; Rosner, D.; Dao, T.L.; Pickren, J.W. Axillary lymph node metastasis from an occult breast cancer. Cancer 1981, 47, 2923–2927. [Google Scholar] [CrossRef]
- Galimberti, V.; Bassani, G.; Monti, S.; Simsek, S.; Villa, G.; Renne, G.; Luini, A. Clinical experience with axillary presentation breast cancer. Breast Cancer Res. Treat 2004, 88, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Pavlidis, N.; Pentheroudakis, G. Cancer of unknown primary site. Lancet 2012, 379, 1428–1435. [Google Scholar] [CrossRef]
- Lee, M.S.; Sanoff, H.K. Cancer of unknown primary. BMJ 2020, 371, m4050. [Google Scholar] [CrossRef]
- Terada, M.; Miyashita, M.; Kumamaru, H.; Miyata, H.; Tamura, K.; Yoshida, M.; Ogo, E.; Nagahashi, M.; Asaga, S.; Kojima, Y.; et al. Surgical treatment trends and identification of primary breast tumors after surgery in occult breast cancer: A study based on the Japanese National Clinical Database-Breast Cancer Registry. Breast Cancer 2022, 29, 698–708. [Google Scholar] [CrossRef]
- He, M.; Tang, L.C.; Yu, K.D.; Cao, A.Y.; Shen, Z.Z.; Shao, Z.M.; Di, G.-H. Treatment outcomes and unfavorable prognostic factors in patients with occult breast cancer. Eur. J. Surg. Oncol. (EJSO) 2012, 38, 1022–1028. [Google Scholar] [CrossRef]
- Chen, K.; Zhang, J.; Beeraka, N.M.; Sinelnikov, M.Y.; Zhang, X.; Cao, Y.; Lu, P. Robot-Assisted Minimally Invasive Breast Surgery: Recent Evidence with Comparative Clinical Outcomes. J. Clin. Med. 2022, 11, 1827. [Google Scholar] [CrossRef]
- Chen, K.; Beeraka, N.M.; Zhang, J.; Reshetov, I.V.; Nikolenko, V.N.; Sinelnikov, M.Y.; Mikhaleva, L.M. Efficacy of da Vinci robot-assisted lymph node surgery than conventional axillary lymph node dissection in breast cancer-A comparative study. Int. J. Med. Robot 2021, 17, e2307. [Google Scholar] [CrossRef]
- Vlastos, G.; Jean, M.E.; Mirza, A.N.; Mirza, N.Q.; Kuerer, H.M.; Ames, F.C.; Hunt, K.K.; Ross, M.I.; Buchholz, T.A.; Buzdar, A.U.; et al. Feasibility of breast preservation in the treatment of occult primary carcinoma presenting with axillary metastases. Ann. Surg. Oncol. 2001, 8, 425–431. [Google Scholar] [CrossRef]
- Qian, K.; Sun, W.; Guo, K.; Zheng, X.; Sun, T.; Chen, L.; Xiang, J.; Li, D.; Wu, Y.; Ji, Q.; et al. The number and ratio of positive lymph nodes are independent prognostic factors for patients with major salivary gland cancer: Results from the surveillance, epidemiology, and End Results dataset. Eur. J. Surg. Oncol. (EJSO) 2019, 45, 1025–1032. [Google Scholar] [CrossRef]
- Foroudi, F.; Tiver, K.W. Occult breast carcinoma presenting as axillary metastases. Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 143–147. [Google Scholar] [CrossRef]
- Singletary, S.E.; Allred, C.; Ashley, P.; Bassett, L.W.; Berry, D.; Bland, K.I.; Borgen, P.I.; Clark, G.; Edge, S.B.; Hayes, D.F.; et al. Revision of the American Joint Committee on Cancer staging system for breast cancer. J. Clin. Oncol. 2002, 20, 3628–3636. [Google Scholar] [CrossRef]
- Wang, Z.; Chong, W.; Zhang, H.; Liu, X.; Zhao, Y.; Guo, Z.; Fu, L.; Ma, Y.; Gu, F. Breast Cancer Patients With Positive Apical or Infraclavicular/Ipsilateral Supraclavicular Lymph Nodes Should Be Excluded in the Application of the Lymph Node Ratio System. Front. Cell Dev. Biol. 2022, 10, 784920. [Google Scholar] [CrossRef]
- Solak, M.; Turkoz, F.P.; Keskin, O.; Aksoy, S.; Babacan, T.; Sarici, F.; Kertmen, N.; Sever, A.R.; Altundag, K. The lymph node ratio as an independent prognostic factor for non-metastatic node-positive breast cancer recurrence and mortality. J. Buon. 2015, 20, 737–745. [Google Scholar]
- Cho, D.H.; Bae, S.Y.; You, J.Y.; Kim, H.K.; Chang, Y.W.; Choi, Y.J.; Woo, S.U.; Son, G.S.; Lee, J.B.; Bae, J.W.; et al. Lymph node ratio as an alternative to pN staging for predicting prognosis after neoadjuvant chemotherapy in breast cancer. Kaohsiung J. Med. Sci. 2018, 34, 341–347. [Google Scholar] [CrossRef]
- Ataseven, B.; Kümmel, S.; Weikel, W.; Heitz, F.; Holtschmidt, J.; Lorenz-Salehi, F.; Kümmel, A.; Traut, A.; Blohmer, J.; Harter, P.; et al. Additional prognostic value of lymph node ratio over pN staging in different breast cancer subtypes based on the results of 1656 patients. Arch. Gynecol. Obstet. 2015, 291, 1153–1166. [Google Scholar] [CrossRef]
- Woodward, W.A.; Vinh-Hung, V.; Ueno, N.T.; Cheng, Y.C.; Royce, M.; Tai, P.; Vlastos, G.; Wallace, A.M.; Hortobagyi, G.N.; Nieto, Y. Prognostic value of nodal ratios in node-positive breast cancer. J. Clin. Oncol. 2006, 24, 2910–2916. [Google Scholar] [CrossRef]
- Schneider, D.F.; Chen, H.; Sippel, R.S. Impact of lymph node ratio on survival in papillary thyroid cancer. Ann. Surg. Oncol. 2013, 20, 1906–1911. [Google Scholar] [CrossRef]
- Wen, J.; Yang, Y.; Liu, P.; Ye, F.; Tang, H.; Huang, X.; Zhong, S.; Xie, X. Development and validation of a nomogram for predicting survival on the base of modified lymph node ratio in breast cancer patients. Breast 2017, 33, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Johnson, H.M.; Irish, W.; Vohra, N.A.; Wong, J.H. The effect of local therapy on breast cancer-specific mortality of women with occult breast cancer and advanced nodal disease (N2/N3): A population analysis. Breast Cancer Res. Treat 2019, 177, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.P.; Allison, D.C.; Wainstock, J.; Miller, K.D.; Dooley, W.C.; Friedman, N.; Baker, R.R. Impact of axillary lymph node dissection on the therapy of breast cancer patients. J. Clin. Oncol. 1993, 11, 1536–1544. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Li, Y.; Wu, J.; Tian, H.; Liu, H.; Fang, Y.; Li, Y.; Yu, F. Nomograms for prediction of overall and cancer-specific survival in young breast cancer. Breast Cancer Res. Treat 2020, 184, 597–613. [Google Scholar] [CrossRef]
- Liu, D.; Chen, Y.; Deng, M.; Xie, G.; Wang, J.; Zhang, L.; Liu, Q.; Yuan, P.; Feng, X. Lymph node ratio and breast cancer prognosis: A meta-analysis. Breast Cancer 2014, 21, 1–9. [Google Scholar] [CrossRef]
- Yang, J.; Long, Q.; Li, H.; Lv, Q.; Tan, Q.; Yang, X. The value of positive lymph nodes ratio combined with negative lymph node count in prediction of breast cancer survival. J. Thorac. Dis. 2017, 9, 1531–1537. [Google Scholar] [CrossRef]
- Vinh-Hung, V.; Verkooijen, H.M.; Fioretta, G.; Neyroud-Caspar, I.; Rapiti, E.; Vlastos, G.; Deglise, C.; Usel, M.; Lutz, J.-M.; Bouchardy, C. Lymph node ratio as an alternative to pN staging in node-positive breast cancer. J. Clin. Oncol. 2009, 27, 1062–1068. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 843) N (%) | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|---|
| HR (95%CI) | p | HR (95%CI) | p | ||
| Age at Diagnosis | |||||
| <60 | 426 (50.5) | 1 | |||
| ≥60 | 417 (49.5) | 1.014 (0.626–1.645) | 0.954 | ||
| ER status | |||||
| Negative | 286 (33.9) | 1 | 1 | ||
| Positive | 476 (56.5) | 0.398 (0.233–0.681) | 0.001 | 0.394 (0.23–0.676) | 0.001 |
| Unknown | 81 (9.6) | 1.039 (0.513–2.104) | 0.915 | 1.116 (0.544–2.288) | 0.764 |
| PR status | |||||
| Negative | 410 (48.6) | 1 | 0.047 | ||
| Positive | 334 (39.6) | 0.483 (0.271–0.861) | 0.014 | ||
| Unknown | 99 (11.7) | 0.873 (0.424–1.796) | 0.711 | ||
| HER-2 status | |||||
| Negative | 266 (31.6) | 1 | |||
| Positive | 102 (12.1) | 0.809 (0.299–2.194) | 0.678 | ||
| Unknown | 475 (56.3) | 0.854 (0.474–1.537) | 0.598 | ||
| Grade | |||||
| I–II | 48 (5.7) | 1 | |||
| III–IV | 163 (19.3) | 1.972 (0.586–6.641) | 0.273 | ||
| Unknown | 632 (75.0) | 1.169 (0.363–3.77) | 0.793 | ||
| pN | |||||
| N1 | 504 (59.8) | 1 | 1 | ||
| N2 | 165 (19.6) | 2.505 (1.298–4.834) | 0.006 | 2.584 (1.334–5.005) | 0.005 |
| N3 | 174 (20.6) | 4.765 (2.706–8.392) | <0.001 | 5.374 (3.02–9.565) | <0.001 |
| Number of regional LNs examined | |||||
| <6 | 218 (25.9) | 1 | 1 | ||
| ≥6, <10 | 97 (11.5) | 0.574 (0.232–1.415) | 0.228 | 0.629 (0.249–1.594) | 0.329 |
| ≥10 | 528 (62.6) | 0.648 (0.383–1.096) | 0.105 | 0.448 (0.256–0.785) | 0.005 |
| Breast surgery | |||||
| Mastectomy | 322 (38.2) | 1 | |||
| Breast-conserving surgery | 92 (10.9) | 1.047 (0.614–1.783) | 0.867 | ||
| No | 429 (50.9) | 1.512 (0.719–3.178) | 0.275 | ||
| Radiotherapy | |||||
| Yes | 455 (54.0) | 1 | |||
| No | 388 (46.0) | 1.241 (0.766–2.011) | 0.381 | ||
| Chemotherapy | |||||
| Yes | 636 (75.4) | 1 | |||
| No | 207 (24.6) | 0.989 (0.556–1.759) | 0.970 | ||
| Characteristic | N1 (n = 504) (%) | N2 (n = 165) (%) | N3 (n = 174) (%) | χ2 | p |
|---|---|---|---|---|---|
| Age at diagnosis | 0.358 | 0.836 | |||
| <60 | 254 (50.4) | 81 (49.1) | 91 (52.3) | ||
| ≥60 | 250 (49.6) | 84 (50.9) | 83 (47.7) | ||
| ER status | 6.257 | 0.181 | |||
| Negative | 157 (31.2) | 62 (37.6) | 67 (38.5) | ||
| Positive | 291 (57.7) | 90 (54.5) | 95 (54.6) | ||
| Unknown | 56 (11.1) | 13 (7.9) | 12 (6.9) | ||
| PR status | 8.147 | 0.086 | |||
| Negative | 231 (45.8) | 84 (50.9) | 95 (54.6) | ||
| Positive | 203 (40.3) | 64 (38.8) | 67 (38.5) | ||
| Unknown | 70 (13.9) | 17 (10.3) | 12 (6.9) | ||
| HER-2 status | 5.257 | 0.262 | |||
| Negative | 163 (32.3) | 56 (33.9) | 47 (27.0) | ||
| Positive | 53 (10.5) | 21 (12.7) | 28 (16.1) | ||
| Unknown | 288 (57.1) | 88 (53.3) | 99 (56.9) | ||
| Grade | 9.909 | 0.042 | |||
| I–II | 30 (6.0) | 12 (7.3) | 6 (3.4) | ||
| III–IV | 82 (16.3) | 38 (23.0) | 43 (24.7) | ||
| Unknown | 392 (77.8) | 115 (69.7) | 125 (71.8) | ||
| Number of regional LNs examined | 70.243 | <0.001 | |||
| 1–5 | 172 (34.1) | 15 (9.1) | 31 (17.8) | ||
| 6–9 | 63 (12.5) | 29 (17.6) | 5 (2.9) | ||
| ≥10 | 269 (53.4) | 121 (73.3) | 138 (79.3) | ||
| Breast surgery | 4.508 | 0.342 | |||
| Mastectomy | 187 (37.1) | 72 (43.6) | 63 (36.2) | ||
| BCS | 58 (11.5) | 19 (11.5) | 15 (8.6) | ||
| No | 259 (51.4) | 74 (44.8) | 96 (55.2) | ||
| Radiotherapy | 17.914 | <0.001 | |||
| Yes | 242 (48.0) | 104 (63.0) | 109 (62.6) | ||
| No | 262 (52.0) | 61 (37.0) | 65 (37.4) | ||
| Chemotherapy | 7.191 | 0.027 | |||
| Yes | 364 (72.2) | 134 (81.2) | 138 (79.3) | ||
| No | 140 (27.8) | 31 (18.8) | 36 (20.7) |
| Characteristics | Total (n = 843) N (%) | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | ||
| Age at diagnosis | |||||
| <60 | 426 (50.5) | 1 | |||
| ≥60 | 417 (49.5) | 1.014 (0.626–1.645) | 0.954 | ||
| ER status | |||||
| Negative | 286 (33.9) | 1 | 1 | ||
| Positive | 476 (56.5) | 0.398 (0.233–0.681) | 0.001 | 0.399 (0.233–0.684) | 0.001 |
| Unknown | 81 (9.6) | 1.039 (0.513–2.104) | 0.915 | 1.123 (0.551–2.287) | 0.750 |
| PR status | |||||
| Negative | 410 (48.6) | 1 | |||
| Positive | 334 (39.6) | 0.483 (0.271–0.861) | 0.014 | ||
| Unknown | 99 (11.7) | 0.873 (0.424–1.796) | 0.711 | ||
| HER-2 status | |||||
| Negative | 266 (31.6) | 1 | 0.847 | ||
| Positive | 102 (12.1) | 0.809 (0.299-2.194) | 0.678 | ||
| Unknown | 475 (56.3) | 0.854 (0.474–1.537) | 0.598 | ||
| Grade | |||||
| I–II | 48 (5.7) | 1 | |||
| III–IV | 163 (19.3) | 1.972 (0.586–6.641) | 0.273 | ||
| Unknown | 632 (75.0) | 1.169 (0.363–3.77) | 0.793 | ||
| pN | |||||
| N1 | 504 (59.8) | 1 | 1 | ||
| N2 | 165 (19.6) | 2.505 (1.298–4.834) | 0.006 | 2.104 (1.083–4.09) | 0.028 |
| N3 | 174 (20.6) | 4.765 (2.706–8.392) | <0.001 | 2.662 (1.438–4.929) | 0.002 |
| Number of regional LNs examined | |||||
| <6 | 218 (25.9) | 1 | |||
| ≥6, <10 | 97 (11.5) | 0.574 (0.232–1.415) | 0.228 | ||
| ≥10 | 528 (62.6) | 0.648 (0.383–1.096) | 0.105 | ||
| PLNR | |||||
| <0.50 | 502 (59.5) | 1 | 1 | ||
| ≥0.50 | 341 (40.5) | 5.07 (2.887–8.905) | <0.001 | 3.584 (1.943–6.614) | <0.001 |
| Breast surgery | |||||
| Mastectomy | 322 (38.2) | 1 | |||
| Breast-conserving surgery | 92 (10.9) | 1.047 (0.614–1.783) | 0.867 | ||
| No | 429 (50.9) | 1.512 (0.719–3.178) | 0.275 | ||
| Radiotherapy | |||||
| Yes | 455 (54.0) | 1 | |||
| No | 388 (46.0) | 1.241 (0.766–2.011) | 0.381 | ||
| Chemotherapy | |||||
| Yes | 636 (75.4) | 1 | |||
| No | 207 (24.6) | 0.989 (0.556–1.759) | 0.970 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, D.; Zhai, J.; Li, L.; Wu, Y.; Ma, F.; Xu, B. Prognostic Factors and a Model for Occult Breast Cancer: A Population-Based Cohort Study. J. Clin. Med. 2022, 11, 6804. https://doi.org/10.3390/jcm11226804
Zhang D, Zhai J, Li L, Wu Y, Ma F, Xu B. Prognostic Factors and a Model for Occult Breast Cancer: A Population-Based Cohort Study. Journal of Clinical Medicine. 2022; 11(22):6804. https://doi.org/10.3390/jcm11226804
Chicago/Turabian StyleZhang, Di, Jingtong Zhai, Lixi Li, Yun Wu, Fei Ma, and Binghe Xu. 2022. "Prognostic Factors and a Model for Occult Breast Cancer: A Population-Based Cohort Study" Journal of Clinical Medicine 11, no. 22: 6804. https://doi.org/10.3390/jcm11226804
APA StyleZhang, D., Zhai, J., Li, L., Wu, Y., Ma, F., & Xu, B. (2022). Prognostic Factors and a Model for Occult Breast Cancer: A Population-Based Cohort Study. Journal of Clinical Medicine, 11(22), 6804. https://doi.org/10.3390/jcm11226804