
Combination of Interleukin-6, C-Reactive Protein and Procalcitonin Values as Predictive Index of Sepsis in Course of Fever Episode in Adult Haematological Patients: Observational and Statistical Study


 , ,
, ,
Abstract

1. Introduction
2. Materials and Methods
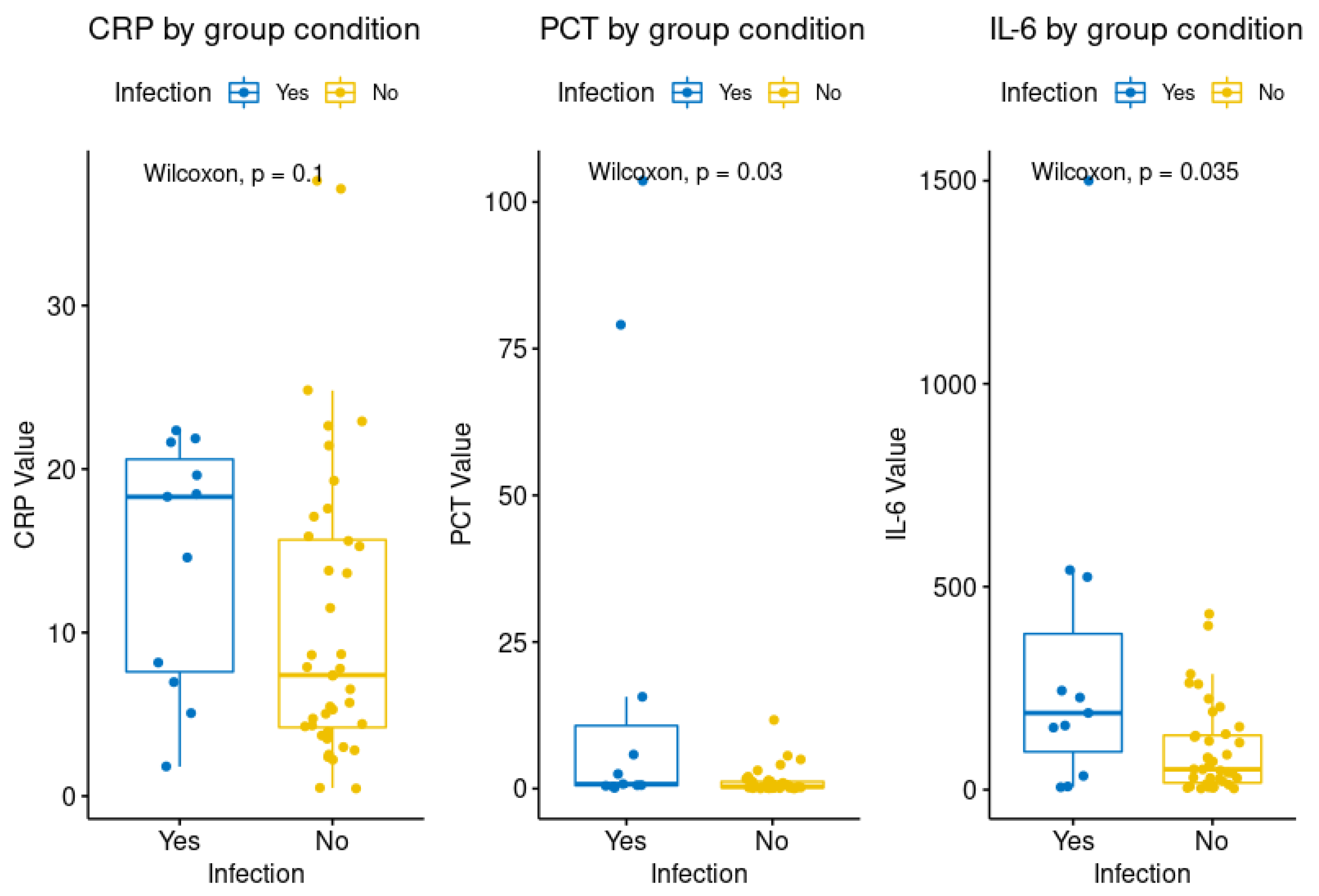
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Massaro, K.; Costa, S.F. Role of Biomarkers as Predictors of Infection and Death in Neutropenic Febrile Patients after Hematopoietic Stem Cell Transplantation. Mediterr. J. Hematol. Infect. Dis. 2015, 7, e2015059. [Google Scholar] [CrossRef]
- Pierrakos, C.; Vincent, J.L. Sepsis biomarkers: A review. Crit. Care 2010, 14, R15. [Google Scholar] [CrossRef]
- Wu, C.W.; Wu, J.Y.; Chen, C.K.; Huang, S.L.; Hsu, S.C.; Lee, M.T.G.; Chang, S.-S.; Lee, C.C. Does procalcitonin, C-reactive protein, or interleukin-6 test have a role in the diagnosis of severe infection in patients with febrile neutropenia? A systematic review and meta-analysis. Support. Care Cancer 2015, 23, 2863–2872. [Google Scholar] [CrossRef]
- Signorelli, J.; Zimmer, A.; Liewer, S.; Shostrom, V.K.; Freifeld, A. Incidence of Febrile Neutropenia in Autologous Hematopoietic Stem Cell Transplant (HSCT) Recipients on levofloxacin prophylaxis. Transpl. Infect. Dis. 2020, 22, e13225. [Google Scholar] [CrossRef]
- Nesher, L.; Rolston, K.V. The current spectrum of infection in cancer patients with chemotherapy related neutropenia. Infection 2014, 42, 5–13. [Google Scholar] [CrossRef]
- Klastersky, J.; De Naurois, J.; Rolston, K.; Rapoport, B.; Maschmeyer, G.; Aapro, M.; Herrstedt, J. Management of febrile neutropaenia: ESMO Clinical Practice Guidelines. Ann. Oncol. 2016, 27 (Suppl. S5), v111–v118. [Google Scholar] [CrossRef]
- Guarana, M.; Nucci, M.; Nouér, S.A. Shock and Early Death in Hematologic Patients with Febrile Neutropenia. Antimicrob. Agents Chemother. 2019, 63, e01250-19. [Google Scholar] [CrossRef]
- Kollu, V.; Mott, S.L.; Khan, R.; Farooq, U.; Jethava, Y.; Dilek, I.; Tricot, G. C-Reactive Protein Monitoring Predicts Neutropenic Fever Following Autologous Hematopoietic Stem Cell Transplantation for Multiple Myeloma. Cureus 2018, 10, e2945. [Google Scholar] [CrossRef]
- Owattanapanich, W.; Suphadirekkul, K.; Kunacheewa, C.; Ungprasert, P.; Prayongratana, K. Risk of febrile neutropenia among patients with multiple myeloma or lymphoma who undergo inpatient versus outpatient autologous stem cell transplantation: A systematic review and meta-analysis. BMC Cancer 2018, 18, 1126. [Google Scholar] [CrossRef]
- Alali, M.; David, M.Z.; Ham, S.A.; Danziger-Isakov, L.; Pisano, J. Febrile Neutropenia Syndromes in Children: Risk Factors and Outcomes of Primary, Prolonged, and Recurrent Fever. J. Pediatr. Hematol. Oncol. 2021, 43, e962–e971. [Google Scholar] [CrossRef]
- Ahmad, S.; Tejuja, A.; Newman, K.D.; Zarychanski, R.; Seely, A.J. Clinical review: A review and analysis of heart rate variability and the diagnosis and prognosis of infection. Crit. Care 2009, 13, 232. [Google Scholar] [CrossRef]
- Bravi, A.; Green, G.; Longtin, A.; Seely, A.J. Monitoring and identification of sepsis development through a composite measure of heart rate variability. PLoS ONE 2012, 7, e45666. [Google Scholar] [CrossRef]
- Papaioannou, V.E.; Dragoumanis, C.; Theodorou, V.; Gargaretas, C.; Pneumatikos, I. Relation of heart rate variability to serum levels of C-reactive protein, interleukin 6, and 10 in patients with sepsis and septic shock. J. Crit. Care 2009, 24, e1–e625. [Google Scholar] [CrossRef]
- Garrard, C.S.; Kontoyannis, D.A.; Piepoli, M. Spectral analysis of heart rate variability in the sepsis syndrome. Clin. Auton. Res. 1993, 3, 5–13. [Google Scholar] [CrossRef]
- Chen, W.L.; Kuo, C.D. Characteristics of heart rate variability can predict impending septic shock in emergency department patients with sepsis. Acad. Emerg. Med. 2007, 14, 392–397. [Google Scholar] [CrossRef]
- Buchan, C.A.; Li, H.O.Y.; Herry, C.L.; Scales, N.; MacPherson, P.; Faller, E.; Bredeson, C.; Huebsch, L.; Hodgins, M.; Seely, A.J.E. Early Warning of Infection in Patients Undergoing Hematopoietic Stem Cell Transplantation Using Heart Rate Variability and Serum Biomarkers. Transplant. Cell. Ther. 2022, 28, 166.e1–166.e8. [Google Scholar] [CrossRef]
- Bruserud, Ø.; Aarstad, H.H.; Tvedt, T.H.A. Combined C-Reactive Protein and Novel Inflammatory Parameters as a Predictor in Cancer-What Can We Learn from the Hematological Experience? Cancers 2020, 12, 1966. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, K.; Ni, J.; Zhang, H.; Yin, L.; Zhang, Y.; Shi, H.; Zhang, T.; Zhou, N.; Mao, W.; et al. Combination of C-Reactive Protein and Neutrophil-to-Lymphocyte Ratio as a Novel Prognostic Index in Patients With Bladder Cancer After Radical Cystectomy. Front. Oncol. 2021, 11, 762470. [Google Scholar] [CrossRef]
- Fink-Neuboeck, N.; Lindemann, J.; Bajric, S.; Maier, A.; Riedl, R.; Weinberg, A.M.; Smolle-Jeuttner, F.M. Clinical impact of interleukin-6 as a predictive biomarker in the early diagnosis of postoperative systemic inflammatory response syndrome after major thoracic surgery: A prospective clinical trial. Surgery 2016, 160, 443–453. [Google Scholar] [CrossRef]
- Sarafidis, K.; Soubasi-Griva, V.; Piretzi, K.; Thomaidou, A.; Agakidou, E.; Taparkou, A.; Diamanti, E.; Drossou-Agakidou, V. Diagnostic utility of elevated serum soluble triggering receptor expressed on myeloid cells (sTREM)-1 in infected neonates. Intensive Care Med. 2010, 36, 864–868. [Google Scholar] [CrossRef]
- Gibot, S.; Bene, M.C.; Noel, R.; Massin, F.; Guy, J.; Cravoisy, A.; Barraud, D.; De Carvalho Bittencourt, M.; Quenot, J.P.; Bollaert, P.E.; et al. Combination biomarkers to diagnose sepsis in the critically ill patient. Am. J. Respir. Crit. Care Med. 2012, 186, 65–71. [Google Scholar] [CrossRef]
- Yang, Y.; Xie, J.; Guo, F.; Longhini, F.; Gao, Z.; Huang, Y.; Qiu, H. Combination of C-reactive protein, procalcitonin and sepsis-related organ failure score for the diagnosis of sepsis in critical patients. Ann. Intensive Care 2016, 6, 51. [Google Scholar] [CrossRef]
- R Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- R Studio Team. Integrated Development Environment for R; RStudio, PBC: Boston, MA, USA, 2021; Available online: http://www.rstudio.com/ (accessed on 1 September 2021).
- Sing, T.; Sander, O.; Beerenwinkel, N.; Lengauer, T. ROCR: Visualizing classifier performance in R. Bioinformatics 2005, 21, 7881. [Google Scholar] [CrossRef]
- Wei, R.; Wang, J. multiROC: Calculating and Visualizing ROC and PR Curves across Multi-Class Classifications. 2018. Available online: https://github.com/WandeRum/multiROC (accessed on 1 September 2021).
- Wilke, C.O. Ggridges: Ridgeline Plots in ‘ggplot2’; R Package Version 0.5.3; 2021. Available online: https://CRAN.R-project.org/package=ggridges (accessed on 1 September 2021).
- Nordmann, E.; McAleer, P.; Toivo, W.; Paterson, H.; DeBruine, L. Data visualisation using R, for researchers who don’t use R. Adv. Methods Pract. Psychol. Sci. 2022, 5, 25152459221074654. [Google Scholar]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Stoma, I.; Karpov, I.; Uss, A.; Krivenko, S.; Iskrov, I.; Milanovich, N.; Vlasenkova, S.; Lendina, I.; Belyavskaya, K.; Cherniak, V. Combination of sepsis biomarkers may indicate an invasive fungal infection in haematological patients. Biomarkers 2019, 24, 401–406. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biomarker | Group | N | Mean | Median | SD | Q1 | Q3 |
|---|---|---|---|---|---|---|---|
| CRP (ng/mL) | Total | 51 | 11.44 | 7.90 | 8.94 | 4.35 | 17.95 |
| Sepsis | 11 | 14.45 | 18.30 | 7.55 | 7.60 | 20.60 | |
| No sepsis | 40 | 10.62 | 7.40 | 9.19 | 4.20 | 15.68 | |
| PCT (mg/mL) | Total | 51 | 5.05 | 0.50 | 18.01 | 0.20 | 1.44 |
| Sepsis | 11 | 19.05 | 0.79 | 36.45 | 0.53 | 10.73 | |
| No sepsis | 40 | 1.21 | 0.37 | 2.15 | 0.16 | 1.22 | |
| IL−6 (pg/mL) | Total | 51 | 146.35 | 69.40 | 235.25 | 19.40 | 190.50 |
| Sepsis | 11 | 325.81 | 189.00 | 0.04 | 93.45 | 384.00 | |
| No sepsis | 40 | 97.00 | 50.20 | 109.72 | 16.98 | 134.00 |
| Biomarker | AUC | Cut-Off | Sensitivity | Specificity |
|---|---|---|---|---|
| PCT | 0.72 | 0.59 | 60% | 73% |
| CRP | 0.66 | 14.6 | 64% | 70% |
| IL−6 | 0.71 | 153 | 73% | 77% |
| CIndex | 0.79 | 1.72 | 73% | 77% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carcò, D.; Castorina, P.; Guardo, P.; Iachelli, V.; Pace, T.; Scirè, P.; Stanco, R.; Markovic, U.; Milone, G.A.; Galbo, F.; et al. Combination of Interleukin-6, C-Reactive Protein and Procalcitonin Values as Predictive Index of Sepsis in Course of Fever Episode in Adult Haematological Patients: Observational and Statistical Study. J. Clin. Med. 2022, 11, 6800. https://doi.org/10.3390/jcm11226800
Carcò D, Castorina P, Guardo P, Iachelli V, Pace T, Scirè P, Stanco R, Markovic U, Milone GA, Galbo F, et al. Combination of Interleukin-6, C-Reactive Protein and Procalcitonin Values as Predictive Index of Sepsis in Course of Fever Episode in Adult Haematological Patients: Observational and Statistical Study. Journal of Clinical Medicine. 2022; 11(22):6800. https://doi.org/10.3390/jcm11226800
Chicago/Turabian StyleCarcò, Daniela, Paolo Castorina, Paola Guardo, Valeria Iachelli, Tecla Pace, Paola Scirè, Rosaria Stanco, Uros Markovic, Giulio Antonio Milone, Federica Galbo, and et al. 2022. "Combination of Interleukin-6, C-Reactive Protein and Procalcitonin Values as Predictive Index of Sepsis in Course of Fever Episode in Adult Haematological Patients: Observational and Statistical Study" Journal of Clinical Medicine 11, no. 22: 6800. https://doi.org/10.3390/jcm11226800
APA StyleCarcò, D., Castorina, P., Guardo, P., Iachelli, V., Pace, T., Scirè, P., Stanco, R., Markovic, U., Milone, G. A., Galbo, F., Moschetti, G., & Martorana, E. (2022). Combination of Interleukin-6, C-Reactive Protein and Procalcitonin Values as Predictive Index of Sepsis in Course of Fever Episode in Adult Haematological Patients: Observational and Statistical Study. Journal of Clinical Medicine, 11(22), 6800. https://doi.org/10.3390/jcm11226800