

Significance of the Lung Immune Prognostic Index for Assessment of the Reliability of the Clinical Treatment Outcome for Advanced Non-Small-Cell Lung Cancer in Patients with COVID-19 Infection

 ,
,
Abstract
1. Introduction
2. Materials and Methods
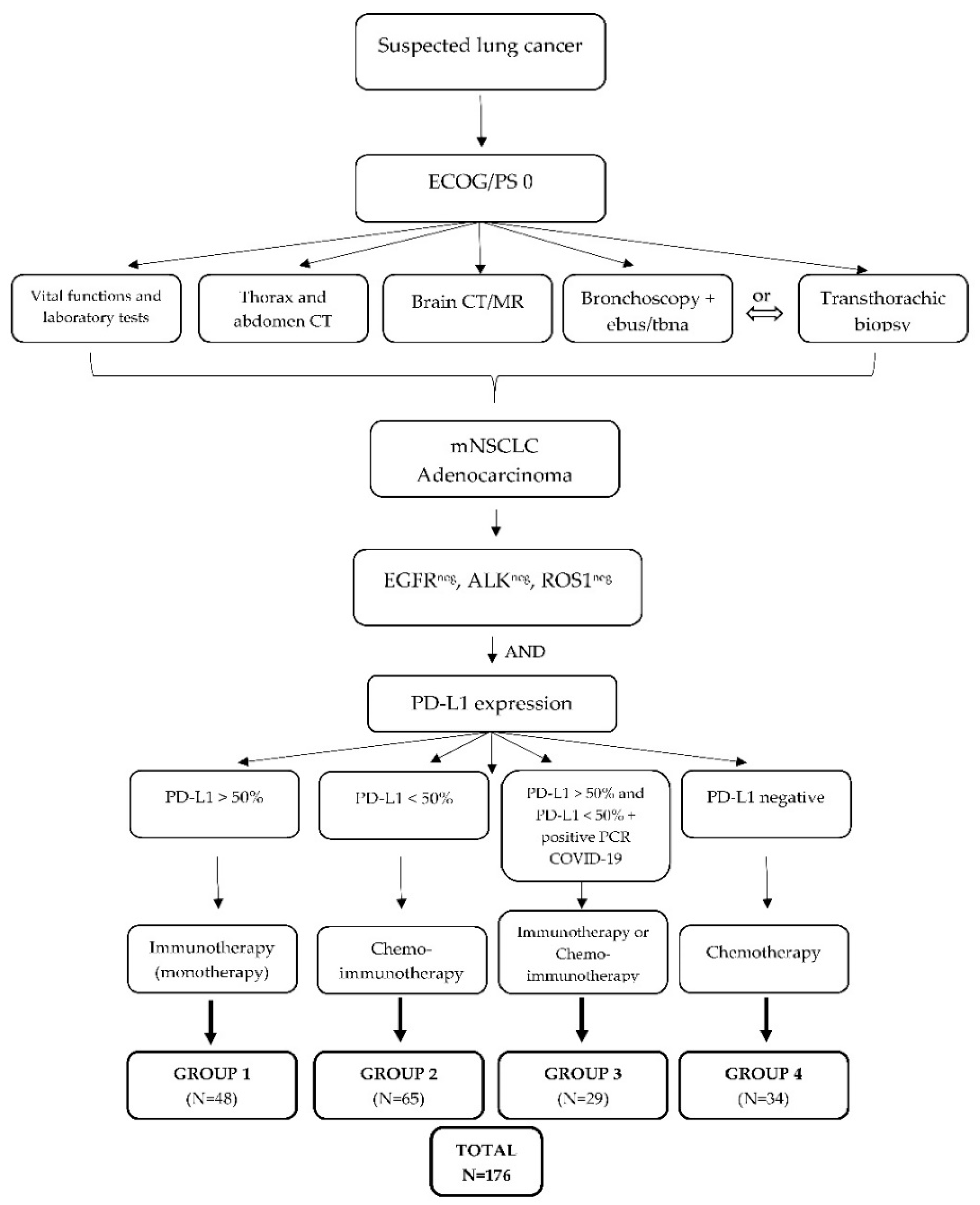
2.1. Patients
2.2. Methods
2.3. Statistical Analysis
3. Results
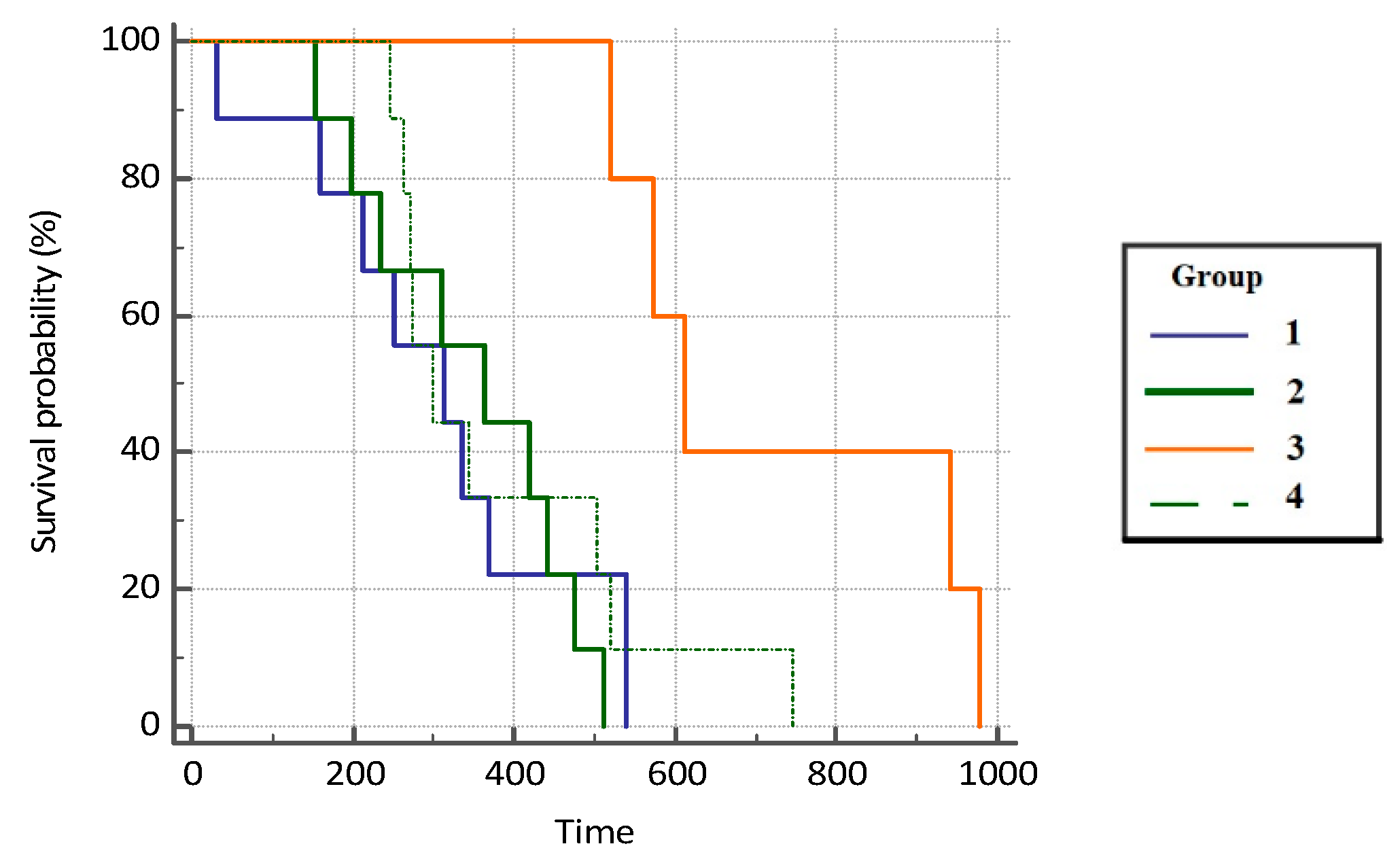
3.1. Overall Survival of Patients
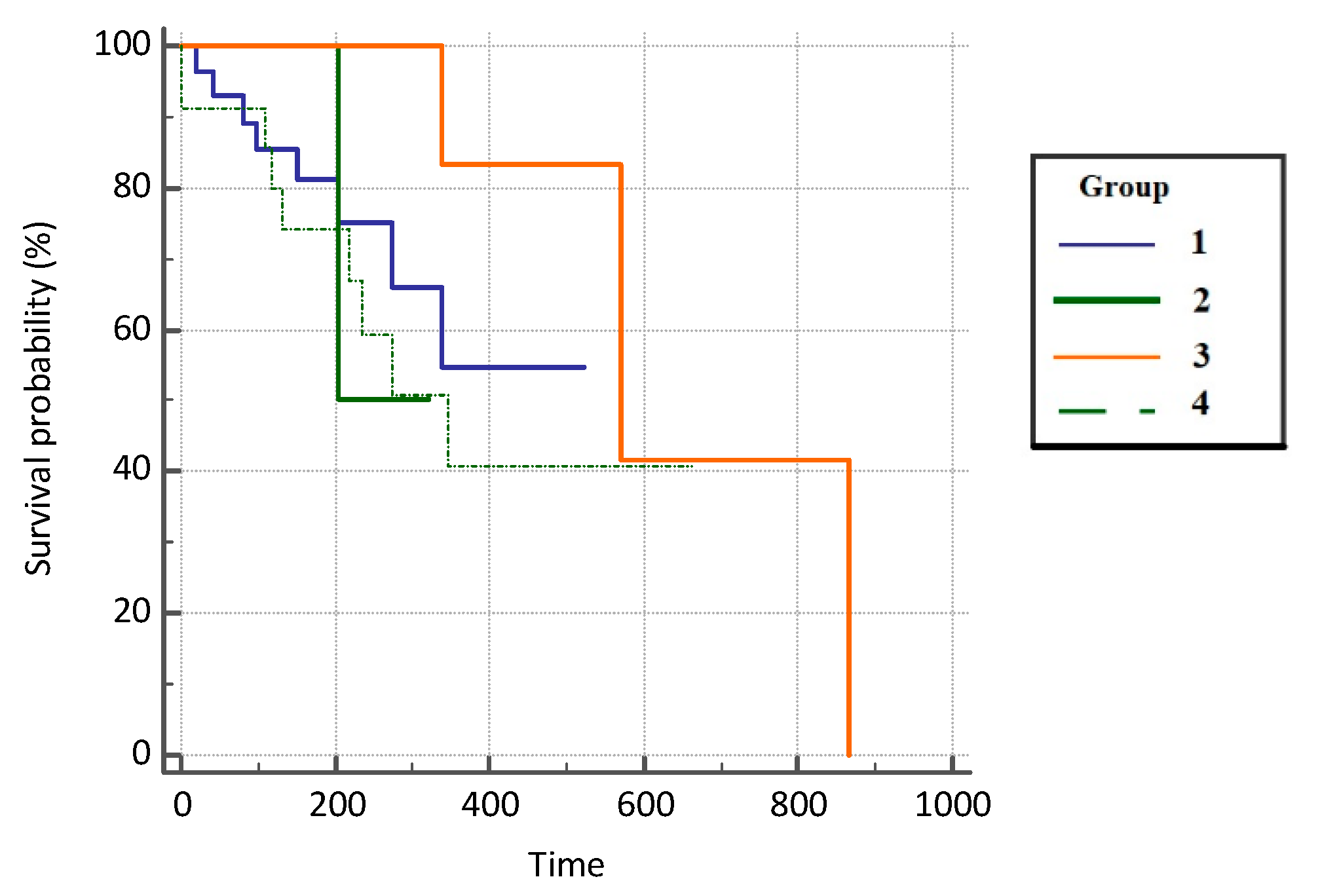
3.2. Progression-Free Survival (PFS) of Patients
3.3. Disease Control Rate (DCR)
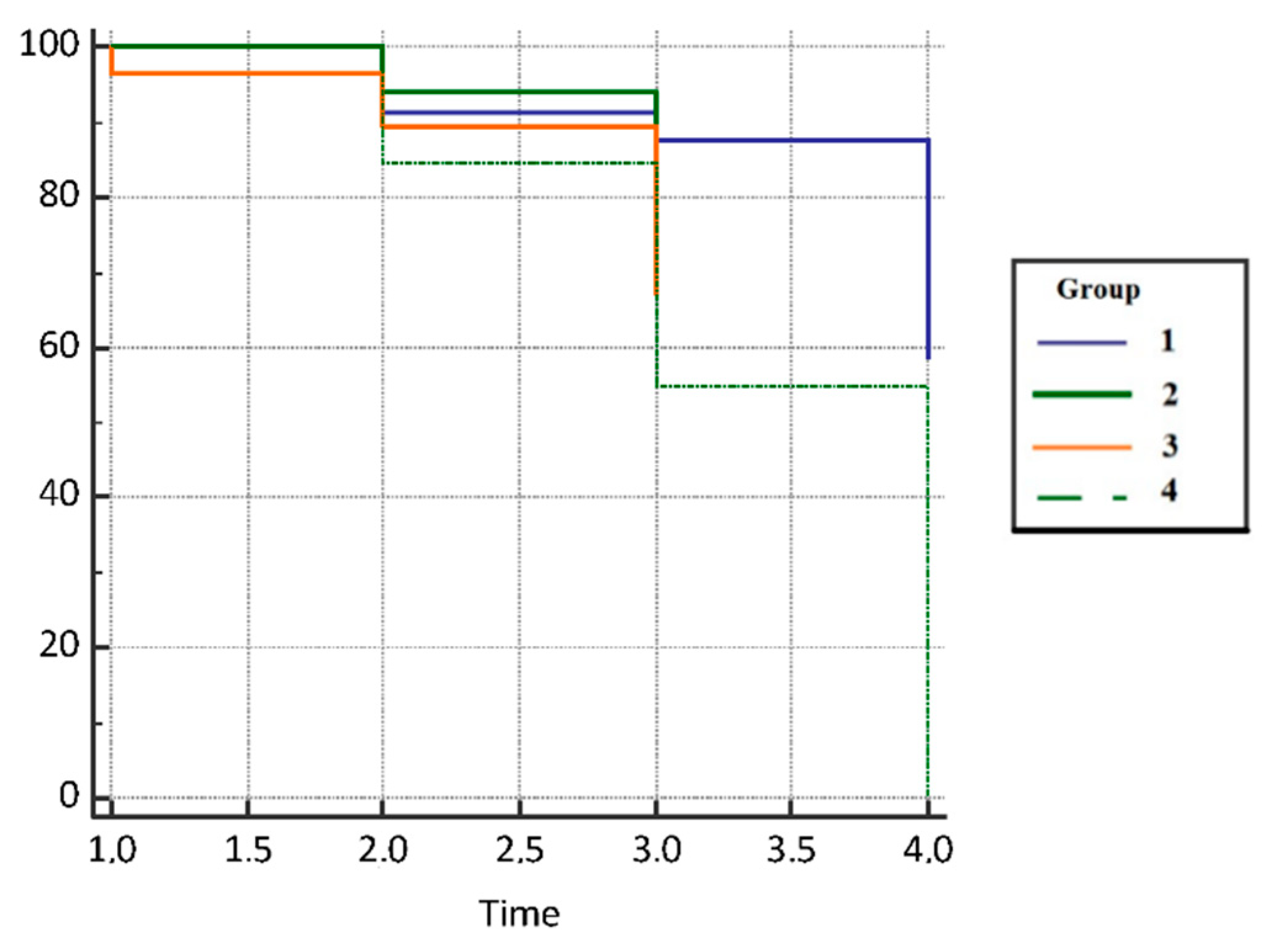
3.4. Lung Immune Prognostic Index (LIPI)
3.5. Clinical Relevance and Predictivity of the Lung Immune Prognostic Index
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ralston, S.H.; Penman, I.D. Davidson’s Principles and Practice of Medicine, 23rd ed.; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Pavelić, J.; Križanac, S.; Kapitanović, S.; Pavelić, L.; Samaržija, M.; Pavičić, F.; Spaventi, S.; Jakopović, M.; Herceg-Ivanovi, Z.; Pavelić, K. The Consequences of Insulin-Like Growth Factors/Receptors Dysfunction in Lung Cancer. Am. J. Respir. Cell Mol. Biol. 2005, 32, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Osmani, L.; Askin, F.; Gabrielson, E.; Li, Q.K. Current WHO guidelines and the critical role of immunohistochemical markers in the subclassification of non-small cell lung carcinoma (NSCLC): Moving from targeted therapy to immunotherapy. Semin Cancer Biol. 2018, 52 Pt 1, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Cordero, R.; Devine, W.P. Targeted Therapy and Checkpoint Immunotherapy in Lung Cancer. Surg Pathol Clin. 2020, 13, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Duma, N.; Santana-Davila, R.; Molina, J.R. Non-Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin. Proc. 2019, 94, 1623–1640. [Google Scholar] [CrossRef] [PubMed]
- Copeman, P.W.; Cowell, T.K.; Dallas, N.L. Lung cancer and smoking. Lancet 1964, 18, 1374–1375. [Google Scholar]
- Edinburg Lung Cancer Group. Patients presenting with lung cancer in south east Scotland. Thorax 1987, 42, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Textbook Promlom. The role of the family doctor in improving health and preventing disease. In Smoking and Lung Diseases; Krpina, K., Ed.; MEF Zagreb: Zagreb, Croatia, 2021. [Google Scholar]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. Non-Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2022, 209, 497–530. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network, NCCN. Guidelines for Non Small Cell Lung Cancer; NCCN: Plymouth Meeting, PA, USA, 2022. [Google Scholar]
- European Society for Medical Oncology, ESMO. Guidelines for Non Small Cell Lung Cancer; ESMO: Lugano, Switzerland, 2020. [Google Scholar]
- Chen, D.S.; Mellman, I. Oncology Meets Immunology: The Cancer-Immunity Cycle. Immunity 2013, 39, 1–10. [Google Scholar] [CrossRef]
- Carbone, D.P.; Gandara, D.R.; Antonia, S.J.; Zielinski, C.; Paz-Ares, L. Non–Small-Cell Lung Cancer: Role of the Immune System and Potential for Immunotherapy. J. Thorac. Oncol. 2015, 10, 974–984. [Google Scholar] [CrossRef]
- Doroshow, D.B.; Sanmamed, M.F.; Hastings, K.; Politi, K.; Rimm, D.L.; Chen, L.; Melero, I.; Schalper, K.A.; Herbst, R.S. Immunotherapy in Non–Small Cell Lung Cancer: Facts and Hopes. Clin. Cancer Res. 2019, 25, 4592–4602. [Google Scholar] [CrossRef]
- Pawelczyk, K.; Piotrowska, A.; Ciesielska, U.; Jablonska, K.; Glatzel-Plucinska, N.; Grzegrzołka, J.; Podhorska-Okolow, M.; Dziegiel, P.; Nowinska, K. Role of PD-L1 expression in non-small cell lung cancer and their prognostic significance according to clinicopathological factors and diagnostic markers. Int. J. Mol. Sci. 2019, 20, 824. [Google Scholar] [CrossRef]
- Mazzaschi, G.; Minari, R.; Zecca, A.; Cavazzoni, A.; Ferri, V.; Mori, C.; Squadrilli, A.; Bordi, P.; Buti, S.; Bersanelli, M.; et al. Soluble PD-L1 and Circulating CD8+PD-1+ and NK Cells Enclose a Prognostic and Predictive Immune Effector Score in Immunotherapy Treated NSCLC patients. Lung Cancer 2020, 148, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Mielgo-Rubio, X.; Uribelarrea, E.A.; Cortés, L.Q.; Moyano, M.S. Immunotherapy in non-small cell lung cancer: Update and new insights. J. Clin. Transl. Res. 2021, 7, 1–21. [Google Scholar] [PubMed]
- Mezquita, L.; Auclin, E.; Ferrara, R.; Charrier, M.; Remon, J.; Planchard, D.; Ponce, S.; Ares, L.P.; Leroy, L.; Audigier-Valette, C.; et al. Association of the Lung Immune Prognostic Index With Immune Checkpoint Inhibitor Outcomes in Patients With Advanced Non–Small Cell Lung Cancer. JAMA Oncol. 2018, 4, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Bañobre, J.; Areses-Manrique, M.C.; Mosquera-Martínez, J.; Cortegoso, A.; Afonso-Afonso, F.J.; de Dios-Álvarez, N.; Fernández-Núñez, N.; Azpitarte-Raposeiras, C.; Amenedo, M.; Santomé, L.; et al. Evaluation of the lung immune prognostic index in advanced non-small cell lung cancer patients under nivolumab monotherapy. Transl. Lung Cancer Res. 2019, 8, 1078–1085. [Google Scholar] [CrossRef] [PubMed]
- Sorich, M.J.; Rowland, A.; Karapetis, C.S.; Hopkins, A.M. Evaluation of the Lung Immune Prognostic Index for Prediction of Survival and Response in Patients Treated With Atezolizumab for NSCLC: Pooled Analysis of Clinical Trials. J. Thorac. Oncol. 2019, 14, 1440–1446. [Google Scholar] [CrossRef]
- Lim, S.M.; Hong, M.H.; Kim, H.R. Immunotherapy for Non-small Cell Lung Cancer: Current Landscape and Future Perspectives. Immune Netw. 2020, 20, e10. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Giovanetti, M.; Benvenuto, D.; Angeletti, S.; Ciccozzi, M. The first two cases of 2019-nCoV in Italy: Where they come from? J. Med. Virol. 2020, 92, 518–521. [Google Scholar] [CrossRef]
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef]
- Lawlor, R.T.; Mattiolo, P.; Mafficini, A.; Hong, S.-M.; Piredda, M.L.; Taormina, S.V.; Malleo, G.; Marchegiani, G.; Pea, A.; Salvia, R.; et al. Tumor Mutational Burden as a Potential Biomarker for Immunotherapy in Pancreatic Cancer: Systematic Review and Still-Open Questions. Cancers 2021, 13, 3119. [Google Scholar] [CrossRef]
- Huang, L.; Han, H.; Zhou, L.; Chen, X.; Xu, Q.; Xie, J.; Zhan, P.; Chen, S.; Lv, T.; Song, Y. Evaluation of the Lung Immune Prognostic Index in Non-Small Cell Lung Cancer Patients Treated With Systemic Therapy: A Retrospective Study and Meta-Analysis. Front. Oncol. 2021, 11, 670230. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Franco, A.; Hodgson, C.; Raja, H.; Carter, M.; Lindsay, C.; Hughes, S.; Cove-Smith, L.; Taylor, P.; Summers, Y.; Blackhall, F.; et al. Real-World Data on Pembrolizumab for Pretreated Non-Small-Cell Lung Cancer: Clinical Outcome and Relevance of the Lung Immune Prognostic Index. Target. Oncol. 2022, 17, 453–465. [Google Scholar] [CrossRef] [PubMed]
- Minami, S.; Ihara, S.; Komuta, K. Pretreatment Lung Immune Prognostic Index Is a Prognostic Marker of Chemotherapy and Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitor. World J. Oncol. 2019, 10, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.P.; Boyer, M.; Lee, J.H.; Kao, S.C. COVID-19: The use of immunotherapy in metastatic lung cancer. Immunotherapy 2020, 12, 545–548. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Group 1 N = 48 N (%) | Group 2 N = 65 N (%) | Group 3 N = 29 N (%) | Group 4 N = 34 N (%) | Total N = 176 N (%) |
|---|---|---|---|---|---|
| Sex (M/F) | 31 (65) 17 (35) | 45 (69) 20 (31) | 15 (52) 14 (48) | 26 (76) 8 (24) | 117 (66) 59 (34) |
| Age at diagnosis (median years, range) | 62.5 (29–76) | 63 (34–78) | 65 (42–91) | 64.5 (47–77) | 63 (29–91) |
| CRP (median, 95% CI) | 9 (3.85–13.9) | 9.8 (5.38–17.18) | 149 (112–205) | 7.9 (0.4–45.47) | 10.3 (7.64–14.09) |
| Days from diagnosis to progression (median, 95% CI) | 435 (344–559) | 320 (260–343) | 696 (634–983) | 200 (0–376) | 338 (294–365) |
| dNLR (N/%) | 28 (37) | 32 (42) | 6 (8) | 10 (13) | 76 (43) |
| Immunotherapy PD-L1 | 48 (27) | 65 (37) | 29 (16) | 34 (19) | 176 (100) |
| 0 | 0 | 0 | 0 | 34 (100) | 34 (19) |
| 1 | 48 (100) | 0 | 9 (31) | 0 | 57 (32) |
| 2 | 0 | 65 (100) | 20 (69) | 0 | 85 (48) |
| LIPI | 48 (27) | 65 (37) | 29 (16) | 34 (19) | 176 (100) |
| 0 | 12 (25) | 27 (42) | 17 (59) | 22 (65) | 78 (44) |
| 1 | 29 (60) | 32 (49) | 12 (41) | 8 (24) | 81 (46) |
| 2 | 7 (15) | 6 (9) | 0 | 4 (11) | 17 (10) |
| LDH (IU/L) | 48 (29) | 65 (39) | 29 (17) | 25 (15) | 167 (95) |
| Median days (95% CI) | 198 (170–221) | 177 (162–187) | 168 (150–213) | 209 (177–232) | 182 (174–192) |
| Overall survival (OS) | 9 (30) | 1 (3) | 2 (6) | 20 (63) | 32 (18) |
| Median days (95% CI) | 312 (167–515) | 437 | 749 | 253 (0–349) | 285 (160–370) |
| Progression-free survival | 28 (45) | 2 (3) | 9 (14) | 23 (37) | 62 (35) |
| Median days (95% CI) | 198 (155–264) | 262 | 353 (200–866) | 151 (38–268) | 209 (178–260) |
| Time from diagnosis to first cycle (days) | 47 (64) | 2 (3) | 10 (14) | 14 (19) | 73 (41) |
| Median days (95% CI) | 218 (139–346) | 31 | 515 (26–420) | 45 (37–69) | 133 (76–208) |
| Time from first to last cycle (days) | 47 (50) | 1 (1) | 16 (17) | 30 (32) | 94 (53) |
| Median days (95% CI) | 269 (208–335) | 511 | 536 (321–607) | 163 (116–265) | 268 (213–330) |
| Total number of doses | 48 (27) | 65 (37) | 29 (16) | 34 (19) | 176 (100) |
| Median of doses (95% CI) | 10 (8–14) | 4 (4–5) | 21 (13–24) | 45 (38–69) | 6 (6–8) |
| Groups | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Group 1 | - | 0.7279 (0.08275–6.4034) | 0.2901 (0.08725–0.9646) | 0.6680 (0.2497–1.7869) |
| Group 2 | 1.3737 (0.1562–12.0842) | - | 0.3985 (0.04337–3.6617) | 0.9176 (0.1115–7.5540) |
| Group 3 | 3.4470 (1.0367–11.4608) | 2.5092 (0.2731–23.0548) | - | 2.3025 (0.7844–6.7584) |
| Group 4 | 1.4971 (0.5596–4.0049) | 1.0898 (0.1324–8.9715) | 0.4343 (0.1480–1.2748) | - |
| Groups | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Group 1 | - | 1.5692 (0.1247–19.7430) | 0.5215 (0.1801–1.5107) | 1.4285 (0.5068–4.0264) |
| Group 2 | 0.6373 (0.05065–8.0180) | - | 0.3324 (0.02548–4.3360) | 0.9103 (0.07056–11.7444) |
| Group 3 | 1.9174 (0.6620–5.5540) | 3.0088 (0.2306–39.2531) | - | 2.7390 (0.8920–8.4108) |
| Group 4 | 0.7000 (0.2484–1.9732) | 1.0985 (0.08515–14.1720) | 0.3651 (0.1189–1.1211) | - |
| Disease Control Rate | N (%) | ||||
|---|---|---|---|---|---|
| Group | 1 (CR) | 2 (PR) | 3 (SD) | 4 (PD) | |
| Group 1 | 00.0% RT | 2143.7% RT | 1531.2% RT | 1225.0% RT | 48 (27.3%) |
| 0.0% CT | 25.6% CT | 19.2% CT | 92.3% CT | ||
| 0.0% GT | 11.9% GT | 8.5% GT | 6.8% GT | ||
| Group 2 | 00.0% RT | 3046.2% RT | 3553.8% RT | 00.0% RT | 65 (36.9%) |
| 0.0% CT | 36.6% CT | 44.9% CT | 0.0% CT | ||
| 0.0% GT | 17.0% GT | 19.9% GT | 0.0% GT | ||
| Group 3 | 13.4% RT | 1965.5% RT | 931.0% RT | 00.0% RT | 29 (16.5%) |
| 33.3% CT | 23.2% CT | 11.5% CT | 0.0% CT | ||
| 0.6% GT | 10.8% GT | 5.1% GT | 0.0% GT | ||
| Group 4 | 25.9% RT | 1235.3% RT | 1955.9% RT | 12.9% RT | 34 (19.3%) |
| 66.7% CT | 14.6% CT | 24.4% CT | 7.7% CT | ||
| 1.1% GT | 6.8% GT | 10.8% GT | 0.6% GT | ||
| TOTAL | 3 | 82 | 78 | 13 | 176 |
| −1.7% | −46.6% | −44.3% | −7.4% | ||
| Groups | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Group 1 | - | 1.09 (0.50–2.39) | 1.88 (0.61–5.80) | 2.80 (1.11–7.05) |
| Group 2 | 0.91 (0.42–1.99) | - | 1.72 (0.55–5.37) | 2.56 (1.00–6.55) |
| Group 3 | 0.53 (0.17–1.65) | 0.58 (0.19–1.82) | - | 1.49 (0.43–5.17) |
| Group 4 | 0.36 (0.14–0.90) | 0.39 (0.15–0.99) | 0.67 (0.19–2.33) | - |
| Lung Immune Prognostic Index (LIPI) | Group 1 | Group 2 | Group 3 | Group 4 | Total |
|---|---|---|---|---|---|
| N (%) | |||||
| Group 0 (good) | 12 (25%) | 27 (42%) | 17 (59%) | 22 (65%) | 78 (44%) |
| Group 1 (intermediate) | 29 (60%) | 32 (49%) | 12 (41%) | 8 (24%) | 81 (46%) |
| Group 2 (poor) | 7 (15%) | 6 (9%) | 0 | 4 (11%) | 17 (10%) |
| Total | 48 (27%) | 65 (37%) | 29 (16%) | 34 (19%) | 176 (100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krpina, K.; Mavrinac, M.; Samarzija, M.; Tolic, E.; Darapi, D.; Baticic, L. Significance of the Lung Immune Prognostic Index for Assessment of the Reliability of the Clinical Treatment Outcome for Advanced Non-Small-Cell Lung Cancer in Patients with COVID-19 Infection. J. Clin. Med. 2022, 11, 6695. https://doi.org/10.3390/jcm11226695
Krpina K, Mavrinac M, Samarzija M, Tolic E, Darapi D, Baticic L. Significance of the Lung Immune Prognostic Index for Assessment of the Reliability of the Clinical Treatment Outcome for Advanced Non-Small-Cell Lung Cancer in Patients with COVID-19 Infection. Journal of Clinical Medicine. 2022; 11(22):6695. https://doi.org/10.3390/jcm11226695
Chicago/Turabian StyleKrpina, Kristina, Martina Mavrinac, Miroslav Samarzija, Ena Tolic, Dora Darapi, and Lara Baticic. 2022. "Significance of the Lung Immune Prognostic Index for Assessment of the Reliability of the Clinical Treatment Outcome for Advanced Non-Small-Cell Lung Cancer in Patients with COVID-19 Infection" Journal of Clinical Medicine 11, no. 22: 6695. https://doi.org/10.3390/jcm11226695
APA StyleKrpina, K., Mavrinac, M., Samarzija, M., Tolic, E., Darapi, D., & Baticic, L. (2022). Significance of the Lung Immune Prognostic Index for Assessment of the Reliability of the Clinical Treatment Outcome for Advanced Non-Small-Cell Lung Cancer in Patients with COVID-19 Infection. Journal of Clinical Medicine, 11(22), 6695. https://doi.org/10.3390/jcm11226695